Re: Ms. no. ???? (Revision)
Association between Atopic Diseases and Attention-deficit /
Hyperactivity Disorder in Childhood in A Large Population-Based
Case-Control Study
JENG-DAU TSAI, MD1,2, SHIH-NI CHANG, MS3,4, CHIH-HSIN MOU, MS3,4,
FUNG-CHANG SUNG,PhD, MPH3,4, KO-HUANG LUE, MD, PhD1,2
1Institute of Medicine, 2Department of Pediatrics, Chung Shan Medical University and
Hospital, Taichung, Taiwan
3Department of Public Health, 4Management Office for Health Data, China Medical
University and Hospital, Taichung, Taiwan
Running title: Atopic disease and ADHD in childhood
Key words: atopic disease, ADHD, childhood, case-control study
Drs Ko-Huang Lue and Fung-Chang Sung contributed equally to this work Address for reprints:
Ko-Huang Lue, MD, PhD, Department of Pediatrics, Chung Shan Medical University Hospital,
#110, Section 1, Jianguo North Road, Taichung 402, Taiwan e-mail: [email protected]
Telephone: (+886)-4-2473-9595 ext. 34112 Fax: (+886)-4-2471-0934
Fung-Chang Sung, PhD, MPH, Department of Public Health, China Medical University, 91 Hsueh-Shih Road, Taichung 404, Taiwan Taiwan;
e-mail: [email protected]
Telephone: (+886)-4-2205-2121 ext. 7520
Words count: 247 in Abstract, 2078 in text, 3 Tables 1 Figure and 26 references.
PURPOSE Both atopic diseases and attention-deficit/hyperactivity disorders (ADHD) are common pediatric disorders that may lead to mental and physical complications. This population-based case-control design is to correlate the risk of ADHD with allergic diseases among pediatric population.
METHODS Using a national insurance claim dataset in Taiwan, 4692 children with ADHD from 2002 to 2009 were identified, and 18768 randomly selected controls frequency matched for gender, age and index date were also enrolled. Odds ratios (OR) of ADHD were calculated for the association with allergic rhinitis, allergic conjunctivitis, atopic dermatitis and asthma.
RESULTS The children with ADHD were predominantly male (77.9%), and 70.1% were 7-12 years old. Logistic regression analysis estimated ORs showed ADHD risk was higher for those living in urban areas. Patients with ADHD had a higher rate of atopic diseases than controls, particularly allergic rhinitis (46.3% vs. 32.3%), and allergic conjunctivitis (33.7% vs. 23.1%). The corresponding ORs were 1.81 (95% confidence interval (CI) = 1.69-1.93) and 1.69 (95% CI = 1.58-1.81), respectively. With a lower prevalence, children with atopic dermatitis and asthma were also at higher risk of ADHD, with ORs of 1.80 (95% CI = 1.58-2.05) and 1.48 (1.24-1.78). The risk of ADHD increased with urbanization, numbers of allergic disease and aging.
CONCLUSION: Most of the children with ADHD had a strong association with atopic diseases, especially allergic rhinitis. The risk also increased with urbanization and age. Awareness of these comorbidities may help clinicians provide better comprehensive management and reduce the burden of disease.
Atopic diseases (AD) are common chronic conditions in pediatric clinics. They usually manifest as recurring, non-infectious, inflammatory conditions, and cause a large economic burden despite the development of prevention therapies and
medication (1-4). It is evident that environmental factors play a role in the
development, and the prevalence of allergic diseases depends on complex interactions between genetic and environmental factors (5). Numerous complications can lead to significant problems both physically and mentally in childhood, and subsequent substantial behavioral disorders can lead to psychosocial impairment (6).
Epidemiology studies have documented that attention-deficit/hyperactivity disorder (ADHD) is a common neurobehavioral disorder in pediatric populations, and estimated a prevalence rate of 5% in school-aged children, with 3 to 4-fold higher rate in males than females (7). The characteristics are recognized by behavioral symptoms of inattention, impulsivity, and hyperactivity (8). Variable environmental influences are known to raise the risk of ADHD development. The etiologies are multi-factorial, and interactions between genetic and environmental factors have been suggested to cause this disorder (9).
Both AD and ADHD are hereditary diseases involving gene-environment interactions. Previous research has shown epidemiological correlation and substantial pathophysiological relationship between AD and ADHD in childhood (10-12).
Children with AD may exhibit hyperactivity and impulsive behavior that may be thought to be secondary to the illness (13). AD and ADHD are frequent and highly impairing childhood conditions imposing a substantial financial burden on social services. The purpose of this study was to examine the relationship between AD and ADHD using a population-based case-control study, with the hypothesis that AD may be a potential cause or exacerbating factor of ADHD symptoms.
METHODS Data source
National Health Research Institutes (NHRI), Department of Health, Taiwan, for this study. This database includes claims data from 1996 to 2009 for one million people covered in the Taiwan National Health Insurance (TNHI) program. There were no significant differences in the distributions of gender and age between the LHID and all beneficiaries. The TNHI system was launched in March 1995, with 23.03 million (99.2%) of the population and 91% medical institutions of Taiwan insured by the end of 2009 (http://www.doh.gov.tw). Information on the basic patient demographics, and medical care received including outpatient and inpatient claims, dental care, childbirth, physical therapy, preventive care, home care, and rehabilitation are available. The NHRI provide eighteen National Health Insurance Research Databases (NHIRDs) to Taiwan scientists for research. We were able to link the LHID to the other datasets using scrambled patient identification numbers to secure the privacy of individual. The present study was thus exempted from ethical review. The International Classification of Diseases, 9th Revision, Clinical Modification
(ICD-9-CM) was used to identify diagnoses of diseases in the claims data due to government policy.
Study sample
from 2002 to 2009 with the date of diagnosis as the index date. The diagnosis of ADHD was based on at least two outpatient department visits with the diagnosis of ADHD in the primary coding field. Diagnostic criteria of ADHD based on the Diagnostic and Statistical Manual of Mental Disorders, Fourth Edition (DSM-IV), and assessment of ADHD or AD were made by clinical physicians in charge at medical institutions. Four control children were randomly selected for each ADHD case, matched for age, gender, index-year and index-month (in total, 18,768 controls). None of the controls had a history of ADHD. Information on ADHD, atopic diseases and urbanization level of where the study subjects resided were also extracted for this study. The urbanization of Taiwan is divided into 7 levels according to the NHRI, with level 1 being the most urbanized area and level 7 the lowest. In this study, we combined urbanization levels 5-7 into level 5 because of the small number of cases in these levels. The atopic diseases included allergic conjunctivitis (ICD-9-CM: 372.05, 372.10 and 372.14), allergic rhinitis (ICD-9-CM 477), asthma (ICD-9-CM 493.00-493.12), and atopic dermatitis (ICD-9-CM 691.8), identified before the index date and during at least three medical visits with diagnosis appeared in either primary or secondary coding fields. For protection of privacy, the identities of patients, physicians and institutions were scrambled in accordance with the Personal Electronic Data Protection Law.
Statistical analysis
The Chi-square test was used to assess differences of categorical variables between the ADHD and non-ADHD groups. Unconditional logistic regression was used to estimate the odds ratios (ORs) and 95% confidence intervals (95% CI) for the association between atopic diseases and ADHD, controlling for urbanization. We further estimated the risk of ADHD associated with the number of atopic diseases by sex controlling for age (<7, 7-12 and 12-18 years) and urbanization, and by age controlling for sex and urbanization. All statistical analyses were performed using SAS software version 9.1 (SAS Institute Inc., Carey, NC), and the significance level was set at 0.05 in two-tailed tests.
RESULTS
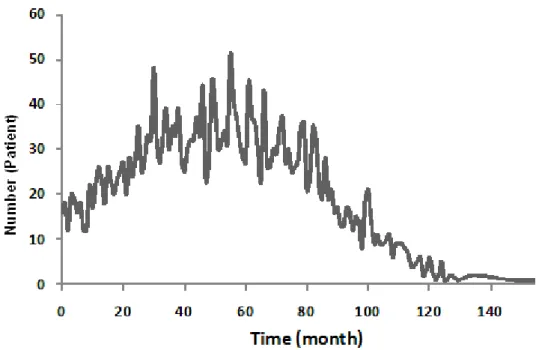
Table 1 shows a comparison of the gender, age, urbanization and atopic diseases between the ADHD and non-ADHD groups. There were no significant differences in demographics between the two groups. The study consisted of 4,692 children with ADHD and 18,768 matched controls (males: 77.9%), with a mean age of 8.91 years (SD = 3.02 years), and 70.1% of the subjects were 7- 12 years of age. Most of the children lived in urban areas (66.4%). The ORs of those with ADHD were reduced in less urbanized areas. As a result, the risk for ADHD is significantly associated with AD, particular allergic rhinitis (46.3% vs. 32.3%) and allergic conjunctivitis (33.7% vs. 23.1%). The risk of ADHD increased for children with allergic rhinitis (OR = 1.81, 95% CI = 1.69-1.93), atopic dermatitis (OR = 1.80, 95% CI = 1.58-2.05), allergic conjunctivitis (OR = 1.69, 95% CI = 1.58-1.81), and asthma (OR = 1.48, 95% CI = 1.24-1.78) in the univariate logistic regression analysis. Most of the children had an allergic disease diagnosed 20 to 80 months before the diagnosis of ADHD (Fig. 1).
When the association between AD and ADHD was evaluated by gender, the adjusted risk for both genders was significantly related to allergic rhinitis, allergic conjunctivitis and atopic dermatitis. The ORs increased with the number of allergic diseases, to 3.87 (95% CI = 2.57-5.83) for girls and 2.58 (95% CI = 2.10-3.15) for boys in those with three atopic diseases (Table 2) in multivariable logistic regression.
In age-stratified analysis, there was a significant trend between ADHD and age (Table 3). The results suggested a strong association between allergic rhinitis and atopic dermatitis and ADHD in each age group. Significant associations were found in allergic conjunctivitis in those aged 7- 18 years (Table 3). The adjusted ORs increased to 2.63 (95% CI = 1.03-6.74), 2.85 (95% CI = 2.33-3.5) and 2.75 (95% CI = 1.78-4.23) in each age group of those with three or more allergic diseases.
DISUSSION
case-control database. The large representative sample of the nationwide database and case-control design suggest high validity and extended availability enable us to eliminate various possible coding biases. This results display strong and independent associations between ADHD and AD, adding substantial evidence of the reported relationship. (14-16). The correlation were independent from various factors that are known to have impact on the presence of ADHD, here also demonstrated the
association correlated with the numbers of AD even though the severity of the disorders are not available from the LHID database.
The etiologies of both AD and ADHD are multi-factorial and heterogeneous, which contributes to their development (9). The immunopathological hypothesis is that inflammatory cytokines provoked by allergic reactions activate neuroimmune mechanisms; subsequently leading to such neurobehavioral disorders, including ADHD (20). Eventually, ADHD was hypothesized as side effects of allergic reactions engendering cholinergic/ adrenergic activity imbalance in the neurological system (19). Neuroimmunology research suggests dopamine transporters, abundantly expressed on human T-cell, are causally implicated in ADHD and being targets for drug like methylphenidate (25). As a conclusion, ADHD is hypothesized an allergic disorder based on a comparison of mechanisms, and hypersensitive to allergen contributes to the development of ADHD (19). Early reports regarding the
co-occurrence of urbanization and ADHD are conflicting to this study. Despite
epidemiology studies had shown an increasing rate of allergies with urbanization (24), a previous large population-based study did not show the correlation between
urbanization of atopic dermatitis and ADHD (12). Similarly in our results showed that incidence of ADHD are significant than controls in all urbanization level, implies the unassociated condition with urbanization.
Another hypothesis regarding the etiologies is that they share common comorbidities such as sleep disturbance. As previous studies concerned allergic rhinitis as a risk factor for ADHD, it is the most investigated in either population-based studies or laboratory immunization research (11, 15, 16). It is known to be frequently cause sleep disturbance in childhood result in poor concentration and distractive behavior, or ADHD cause psychology distress and subsequent an exacerbating factor for atopic conditions controversially (6, 7, 9-11). Children with ADHD had positive skin prick test results to common allergens consistent with allergic rhinitis (11), and was also suggested an increased rates of allergic
sensitization in a pediatric population (15). For issues of atopic dermatitis, children with atopic dermatitis have significant sleep problems and cause lower quality of life, and were taken into account potential confounders of the severity and comorbidities subsequent higher levels of ADHD (12, 13, 21). Rare large studies concern the
association of asthma. A population-based twin study showed the influence of
genetics effects, and childhood asthma is associated with the subsequent development of hyperactivity in early adolescence (10). In contrast, although ADHD is traditionally assumed to be male predominant, we did not find a significant difference by gender in AD. When adjusted for age, urbanization and mutual 4 atopic diseases, ADHD was associated with AD except asthma in both genders. The confirmatory factor analysis of their study suggested that AD have a significant effect on childhood behavioral disorders (17). To date, none had reported allergic conjunctivitis to be a risk factor for ADHD.
With regards to the distribution of duration between AD and ADHD, it mostly took 20 to 80 months to diagnose ADHD, which explains why the level of diagnosis of ADHD was lower in preschoolers. It is likely to present from early childhood, and possibly be related to immunity through increased exposure to respiratory infections and subsequent neurobehavioral disorders. The pathophysiology is proposed as allergic rhinitis subsequent sinusitis caused by streptococcal infections consequent various pediatric autoimmune neuropsychiatric disorders, including ADHD (18, 19). This may match a developmental pattern for a cluster of ADHD that begins in early childhood, and tends to increasingly commonly begin with school entry (7).
Although the stimulant drugs and tricyclic antidepressants are effective for ADHD, manage the associated atopic condition may facilitate improvement of symptom and minimize medication for children with ADHD. Therefore the associated symptoms with AD and medication for it could play major roles in the ADHD symptoms. Linkage between AD and ADHD could be through the histamine pathway, suggest that antihistamine drugs may be effective for treating ADHD. The potential
therapeutic role of antihistamine in ADHD may offer a future alternative treatment choice for patients with dual diagnoses, but definite pathophysiology mechanism and clinical trial require further verification for definite treatment efficacy.
Limitation of this study include the information of clinical condition, laboratory data, images and severity of the disorders are not available. Moreover, the residual confounding cannot completely be ruled out based on the available data. Neither the recording of the associated severity of comorbidities, nor the educational background of the parents was available to enhance the possibilities to draw causal conclusions. These results cannot clarify to treat a subclinical state or a state in a latent period, and whether these states influence the results.
CONCLUSIONS
Our results suggest there are strong correlations between childhood ADHD and AD. If the association indeed improves to be causal, then effective treatment of atopic
symptoms would have exciting potential as a strategy for the prevention of ADHD. We suggest children with ADHD may require combination of allergen prevention, integrated diagnosis and management strategies. Moreover, determining and avoiding triggers for AD may reduce the predisposition to ADHD, and consequently reduce medical burden. We look forward the pathophysiology research and longitudinal study for follow-up children with atopic conditions and neurobehavioral problem to add substantial evidence to support the correlations.
ACKNOWLEDGMENTS
This study was supported by the National Sciences Council, Executive Yuan (grant numbers NSC 100-2621-M-039-001), Taiwan Department of Health Clinical Trial and Research Center for Excellence (grant number DOH100-TD-B-111-004) and Taiwan Department of Health Cancer Research Center of Excellence (DOH100-TD-C-111-005).
DISCLOSURE
REFERENCES
1. Berger WE. Overview of allergic rhinitis. Ann Allergy Asthma Immunol. 2003; 90(Suppl 3):7-12.
2. Masoli M, Fabian D, Holt S, Beasley R. The global burden of asthma: executive summary of the GINA Dissemination Committee report. Allergy. 2004; 59:469-78.
3. Williams HC. Clinical practice. Atopic dermatitis. N Engl J Med. 2005; 352:2314-24.
4. Rosario N, Bielory L. Epidemiology of allergic conjunctivitis. Curr Opin Allergy Clin Immuno. 2011; 11:471-6.
5. Halken S. Prevention of allergic disease in childhood: clinical and
epidemiological aspects of primary and secondary allergy prevention. Pediatr Allergy Immuno. 2004; 15 Suppl 16: 9-32.
6. Blaiss MS. Pediatric allergic rhinitis: physical and mental complications. Allergy Asthma Proc. 2008; 29: 1-6.
7. Polanczyk G, de Lima MS, Horta BL, Biederman J, Rohde LA. The worldwide prevalence of ADHD: a systematic review and metaregression analysis. Am J Psychiatr. 2007; 164:942-8.
8. Biederman J, Faraone SV. Attention-deficit hyperactivity disorder. Lancet. 2005; 366:237-48.
9. Millichap JG. Etiologic classification of attention-deficit/hyperactivity disorder.
Pediatrics. 2008; 121: 358-65.
10. Mogensen N, Larsson H, Lundholm C, Almqvist C. Association between childhood asthma and ADHD symptoms in adolescence--a prospective population-based twin study. Allergy. 2011; 66:1224-30.
11. Brawley A, Silverman B, Kearney S, et al. Allergic rhinitis in children with attention-deficit/hyperactivity disorder. Ann Allergy Asthma Immunol. 2004; 92:663-7.
12. Romanos M, Gerlach M, Warnke A, Schmitt J. Association of
attention-deficit/hyperactivity disorder and atopic eczema modified by sleep disturbance in a large population-based sample. J Epidemiol Community Health. 2010; 64:269-73.
13. Camfferman D, Kennedy JD, Gold M, Martin AJ, Winwood P, Lushington K.
Eczema, sleep, and behavior in children. J Clin Sleep Med. 2010; 15; 6:581-8.
14. Schmitt J, Romanos M, Schmitt NM, Meurer M, Kirch W. Atopic eczema and attention-deficit/hyperactivity disorder in a population-based sample of children and adolescents. JAMA. 2009; 18; 301:724-6.
15. Suwan P, Akaramethathip D, Noipayak P. Association between allergic sensitization and attention deficit hyperactivity disorder (ADHD). Asian Pac J Allergy Immunol. 2011; 29: 57-65.
16. Tsai MC, Lin HK, Lin CH, Fu LS. Prevalence of attention deficit/hyperactivity disorder in pediatric allergic rhinitis: a nationwide population-based study. Allergy Asthma Proc. 2011; 32:41-6.
17. Schmitt J, Buske-Kirschbaum A, Roessner V. Is atopic disease a risk factor for attention-deficit/hyperactivity disorder? A systematic review. Allergy. 2010; 65:1506-24.
18. Dykewicz MS, Hamilos DL. Rhinitis and sinusitis. J Allergy Clin Immunol. 2010; 125: S103-15.
19. Marshall P. Attention deficit disorder and allergy: a neurochemical model of the relation between the illnesses. Psychol Bull. 1989; 106:434-46.
20. Pelsser LM, Buitelaar JK, Savelkoul HF. ADHD as a (non) allergic
hypersensitivity disorder: a hypothesis. Pediatr Allergy Immunol. 2009; 20: 107-12.
21. Sung V, Hiscock H, Sciberras E, Efron D. Sleep problems in children with
family. Arch Pediatr Adolesc Med. 2008; 162:336-42.
22. Nicolaou N, Siddique N, Custovic A. Allergic disease in urban and rural
populations: increasing prevalence with increasing urbanization. Allergy. 2005; 60:1357-60.
23. Yu JH, Lue KH, Lu KH, Sun HL, Lin YH, Chou MC. The relationship of air pollution to the prevalence of allergic diseases in Taichung and Chu-Shan in 2002. J Microbiol Immunol Infec. 2005; 38: 123-6.
24. Viinanen A, Munhbayarlah S, Narantsetseg L, M, et al. Prevalence of asthma, allergic rhinocongunctivitis and allergic sensitisation in Mongolia. Allergy. 2005; 60: 1370–1377.
25. Yukawa K, Iso H, Tanaka T, et al. Down-regulation of dopamine transporter and abnormal behavior in STAT6-deficient mice. Int J Mol Med. 2005; 15:819-25. 26. Shyu CS, Lin HK, Lin CH, Fu LS. Prevalence of attention-deficit/hyperactivity
disorder in patients with pediatric allergic disorders: a nationwide, population-based study. J Microbiol Immunol Infect. 2012; 45:237-42.
TABLE 1. Comparison of demographic status and atopic diseases between the ADHD and non-ADHD groups with odds ratios measured in univariate logistic regression analysis Non-ADHD N=18,768 ADHD N=4,692 n % n % OR (95% CI)
Gender Female 4,140 22.1 1,035 22.1 1.00 (reference) Male 14,628 77.9 3,657 77.9 1.00 (0.93-1.08) Age (years) <7 1,300 6.9 325 6.9 1.00 (reference) 7-12 13,152 70.1 3,288 70.1 1.00 (0.88-1.14) 12-18 4,316 23.0 1,079 23.0 1.00 (0.871.15) Mean (SD) 8.93 (3.03) 8.91 (3.02) 1.00 (0.99-1.01) Urbanization† 1 5,077 27.1 1,655 35.3 1.00 (reference) 2 5,574 29.7 1,461 31.1 0.80 (0.74-0.87)*** 3 3,707 19.8 856 18.2 0.71 (0.65-0.78)*** 4 2,614 13.9 472 10.1 0.55 (0.50-0.62)*** 5 1,795 9.6 248 5.3 0.42 (0.37-0.49)*** Atopic Diseases† Allergic rhinitis 6,062 32.3 2,172 46.3 1.81 (1.69-1.93)*** Allergic conjunctivitis 4,338 23.1 1,580 33.7 1.69 (1.58-1.81)*** Atopic dermatitis 778 4.2 339 7.2 1.80 (1.58-2.05)*** Asthma 450 2.4 165 3.5 1.48 (1.24-1.78)***
OR, odds ratio; CI, confidence interval
†Chi-square test p <0.0001
FIGURE 1. Distribution of duration between diagnosis of atopic diseases and ADHD.
TABLE 2. Adjusted odds ratios of ADHD by gender for association with atopic diseases in multivariate logistic regression.
All Girls Boys
OR (95% CI) OR (95% CI) OR (95% CI)
Atopic diseases†
Allergic rhinitis 1.59 (1.49-1.71)*** 1.84 (1.59-2.13)*** 1.54 (1.42-1.66)*** Allergic conjunctivitis 1.43 (1.33-1.54)*** 1.63 (1.40-1.91)*** 1.39 (1.28-1.50)*** Atopic dermatitis 1.40 (1.22-1.61)*** 1.66 (1.25-2.21)*** 1.33 (1.14-1.56)***
Asthma 1.15 (0.95-1.38) 0.88 (0.57-1.36) 1.22 (1.00-1.50)
Number of atopic diseases
0 1.00 (reference) 1.00 (reference) 1.00 (reference)
1 1.63 (1.51-1.75)*** 1.81 (1.55-2.11)*** 1.58 (1.45-1.72)***
2 2.25 (2.06-2.47)*** 2.88 (2.35-3.53)*** 2.12 (1.91-2.34)***
≥ 3 2.79 (2.33-3.35)*** 3.87 (2.57-5.83)*** 2.58 (2.10-3.15)***
p for trend <0.0001 <0.0001 <0.0001
Adjusted for age, urbanization. The “All” column was adjusted for sex
† Adjusted for age, urbanization and mutual 4 allergic diseases
TABLE 3. Adjusted odds ratios of ADHD by agefor association with atopic diseases in multivariate logistic regression.
Age, years <7 N=1,625 7-12 N=16,440 12-18 N=5,395
OR (95% CI) OR (95% CI) OR (95% CI)
Atopic diseases†
Allergic rhinitis 1.75 (1.33-2.30)*** 1.59 (1.47-1.73)*** 1.59 (1.37-1.83)*** Allergic conjunctivitis 1.29 (0.23-1.81) 1.45 (1.33-1.58)*** 1.42 (1.22-1.65)*** Atopic dermatitis 1.92 (1.41-3.24)* 1.35 (1.16-1.58)*** 1.49 (1.06-2.10)*
Asthma 1.82 (0.93-3.54) 1.11 (0.90-1.38) 1.10 (0.66-1.82)
Number of atopic diseases
0 1.00 (reference) 1.00 (reference) 1.00 (reference)
1 1.80 (1.37-2.38)*** 1.66 (1.52-1.81)*** 1.54 (1.32-1.79)*** 2 2.82 (1.90-4.20)*** 2.24 (2.01-2.49)*** 2.28 (1.88-277)*** ≥ 3 2.63 (1.03-6.74)* 2.85 (2.33-3.50)*** 2.75 (1.78-4.23)***
p for trend <0.0001 <0.0001 <0.0001
Adjusted for sex, urbanization.
† Adjusted for sex, urbanization and mutual 4 allergic diseases