物質使用疾患與精神疾病共病症之研究
88
0
0
全文
(2) 致謝 參年的研究所生涯即將結束了,在這參年的生涯中,讓我學習到 了許多寶貴的知識及許多難得的經驗。很幸運的能在中國醫藥大學遇 到宋老師,他除了繁忙的工作外,還不時提醒並督促我完成論文,處 處為我著想。也感謝宋老師沒有給我很大的壓力,讓我的研究所與工 作能同時進行。而在面對我的畢業論文時也能不厭其煩的教導我。並 且協助我在最後關頭完成論文。也感謝藍老師能夠給我充分的支持讓 我完成學業。 這一路走來,要感謝的人很多,首先我要感謝我的口委:楊俊毓 教授、李中一教授及陳秋瑩副教授,對我的論文提供了許多寶貴的資 源及建議。工作同仁的體量也讓我感激不盡。最後感謝我先生的支 持,並在我趕論文時還給我打氣,讓我能順利完成學業。. i.
(3) 中文摘要 目的:利用國家衛生研究院建立的全民健康保險歸人檔的資料,分析 資料中藥物濫用的逐年盛行及新個案特徵,進而探討其與精神疾病共 病情形。並探討精神分裂症及情感性精神病之就醫情形與藥物、酒精 使用之共病狀況。方法:我們利用國家衛生研究院建立的全民健康保 險歸人檔 1996-2003 年的資料,分析有申報診斷藥物濫用或藥物依賴 記錄的逐年盛行及新個案,進而以 1:3 的方式抽對照樣本,進行病 例對照分析,比較兩者精神疾病的差異。之後,我們接著使用國家衛 生研究院建立的全民健康保險歸人檔 1997-2006 年一百萬人的資料來 分析精神分裂症及情感性精神病的逐年盛行及新個案,和其中與藥物 及酒精濫用共病之情形。結果:在 200,000 人的世代檔中,合計有 796 人(男 72.7%)在 1996 到 2003 年間接受藥物濫用的治療,其中 37 名為未成年患者,發生率由 1997 年的 1.76/10,000 增加到 2003 年的 11.9/10,000,達 6.8 倍。相對應之盛行率為 1.92/10,000 和 14.7/10,000。 進一步的 nested case-control 分析顯示,藥物濫用的人有精神疾病的 盛行率比非藥物濫用者高,尤其是情感性精神病(66.6/1000 對 19.3/1000)、藥物性精神病(40.2/1000 對 1.26/1000) 、精神分裂症 (33.9/1000 對 12.1/1000)和酒癮徵候群(30.2/1000 對 6.7/1000)等, 這些主要精神疾病的勝算比為 4.65(95%信賴區間 3.53-6.13) ,藥物. ii.
(4) 性精神病的勝算比則可達 33.3(p<0.0001)。在健康保險歸人檔 1997-2006 年一百萬人的世代檔中, 精神分裂症及情感性疾患新發生 的個案數比率有逐年下降的情況(精神分裂症在 1997 年是 9.97/10000 至 2006 年是 4.46/10000,情感性疾患在 1997 年是 40.11/10000 至 2006 年是 27.38)。而在酒精依賴、酒精濫用、藥物依賴及藥物濫用則是增 加。結論:健康保險資料不僅顯示國人藥物濫用的成長快速,有精神 疾病的危險較高,應予重視。 關鍵詞:藥物濫用、發生率、盛行率、病例對照研究、國民健康保險 資料、精神分裂症、情感性疾患. iii.
(5) Abstract Purpose: This study investigated the trend of drug abuse care in a national representative sample, and estimated the risk for co-occurring mental disorders among abusers. We also investigated schizophrenia and affective disorders and their co-morbidity relationship with alcohol and drug use disorders. Method: Using a randomly selected cohort with 200,000 persons in 2000 from the insured in the National Health Insurance (NHI) program, the Department of Health, Taiwan, we assessed the annual prevalence and new claims rates for drug abuse treatment in 1996-2003, and conducted a nested case-control analysis to compare the psychiatric co-morbidity between users and nonusers (1:3). Then, we used another randomly selected sample with 1,000,000 persons from 2005. We assessed the prevalence of schizophrenia, affective disorder, alcohol dependence, alcohol abuse, drug dependence and drug abuse in 1997-2006. We also calculated the relative rate ratio to compare the drug and alcohol use disorders by age and year among the persons having schizophrenia or affective disorder and general population.. Results:. Among 796 persons with diagnosed drug use disorders in the 1996-2003 cohort (72.7% males), 37 persons were teens. There was a 6.8-fold increase of new medical claims for drug use disorders in six years, from iv.
(6) 1.76/10,000 in 1997 to 11.9/10,000 in 2003. The corresponding prevalence had a 7.1-fold increase, from 1.92/10,000 to 14.7/10,000, respectively. The case-control analyses showed that abusers were more prevalent than nonusers in mental disorders, particularly for the affective psychosis (ICD 296) (66.6 per 1000 vs. 19.3 per 10000), drug related psychosis (ICD 292) (40.2 per 1000 vs. 1.26 per 1000), schizophrenia (33.9 per 1000 vs. 12.1 per 1000) and alcohol dependence syndrome (30.2 per 1000 vs. 6.7 per 1000). With an overall odds ratio of 4.65 (95% confidence interval (CI) 3.53-6.13) for having psychiatric diseases, the risk to have the drug-associated psychosis was 33.3 folds greater for substance users than for controls. The odds ratio increased to 85.8 if the neurotic disorders were excluded from the data analysis (p<0.0001). In the 1996-2006 cohorts, we found the incidence rates of schizophrenia and affective psychosis declined annually, while the incidence rates of substances dependent and substance abuse were increasing. There was a higher risk of substance use disorders among individuals with schizophrenia or affective disorder. Conclusions: There was a rapid increase in substance use disorders in the recent years in Taiwan. Higher prevalence rates of psychiatric co-morbidities among drug abusers and. v.
(7) vise versa underscore the urgent need to target public health prevention.. Keywords:Universal insurance, mental health, case-control study, prevalence, substance abuse, schizophrenia, affective disorder, Taiwan. vi.
(8) 目錄 致謝………………………………………………………………………….…………i 中文摘要………………………………………………………………………………ii 英文摘要……………………………………………………………………………...iv 目錄……………………………………………………………….......................….. vii 表目錄………………………………………………………..………………..….…viii 圖目錄…………………………………………………………...............................….x 第一章 緒論………………………………………………………………………..…1 第一節 研究背景與研究動機…………………………………………………1 第二節 研究的重要性…………………………………………………………2 第三節 研究目的………………………………………………………………3 第四節 研究問題與研究假設…………………………………………………3 第五節 名詞界定………………………………………………………………3 第二章 文獻查證……………………………………………………………………..4 第ㄧ節 藥物濫用的定義………………………………………………………4 第二節 藥物濫用與精神疾病之共病症………………………………………6 第三節 精神分裂症(Schizophrenia)的定義…………………………………..8 第四節 精神分裂症與酒精和藥物使用之探討………………………………9 第五節 情感性疾患(affective disorders)的定義…………………………..…10 第六節 情感性疾患與酒精和藥物使用之探討………………………..…....12 第七節 研究架構……………………………………………………………..14 第三章 研究方法……………………………………………………………………15 第一節 研究設計…………………………………………………………..…15 第二節 研究對象……………………………………………………..………15 第三節 研究工具的擬定………………….……………………………….....16 第四節資料統計與分析………………………………………………………16 第四章 研究結果………………………………………….………………………...21 第五章 討論…………………………………………………………………………24 研究限制…….….…………………………………………………………..27 第六章 結論與建議…………………………………………………………………28 第一節 結論…………………………………………….……………...……..28 第二節 應用與建議…………………………………………………………..28 參考文獻……………………………………………………………………………..30 附錄………………………………………………………….……………………….54. vii.
(9) 表目錄 Table 1.. The prevalence and incidence of drug use disorders identified from the National Health Insurance cohort data in Taiwan, 1996-2000..………....37 Table 2. The prevalence of mental disorders in cases with drug use disorders diagnosed in the National Health Insurance cohort in Taiwan, 1996-2000 ………….…………………………………........................…38 Table 3. The prevalence of mental disorders identified for controls in the National Health Insurance cohort in Taiwan, 1996-2003.………………………...….39 Table 4. Odds ratios of psychiatric diseases estimated in nested case-control groups of the National Health Insurance cohort in Taiwan, 1996-2003.…….………...40 Table 5. Odds ratios of psychiatric disease (any of drug related psychosis, other organic brain syndrome, schizophrenia, affective psychosis, personality disorder, alcohol dependence syndrome, adjustment reaction) estimated in nested case-control groups of the National Health Insurance cohort in Taiwan, 1996-2003.………………………………………………………..41 Table 6. Prevalence of schizophrenia, alcohol and drug use disorders by year in 1997-2006, Taiwan……………………………………………...…………..42 Table 7. Incidence of schizophrenia, alcohol and drug use disorders by year in 1997-2006, Taiwan……….…………………………….………………..….43 Table 8. Incident cases of schizophrenia by age and sex in 1997-2006, Taiwan….…45 Table 9. Incident cases of affective disorder by age and sex in 1997-2006, Taiwan………………………………………………………………………45 Table 10. Co-morbidity rates (1/10,000) of alcohol dependence, alcohol abuse, drug dependence and drug abuse among schizophrenia cases and non-schizophrenia general population by age in males, in 1997-2006, Taiwan………………………………………………….……….…………47 Table 11. Co-morbidity rates (1/10,000) of alcohol dependence, alcohol abuse, drug dependence and drug abuse among schizophrenia cases and non-schizophrenia general population by age in females, in 1997-2006, Taiwan……………………………… …...…………………..…….48 Table 12. Co-morbidity schizophrenia cases to general population rate ratios of alcohol dependence, alcohol abuse, drug dependence and drug abuse by age in males and females, in 1997-2006, Taiwan….....................…….……….49 Table 13. Co-morbidity rates (1/10,000) of alcohol dependence, alcohol abuse, drug dependence and drug abuse among Affective disorder cases and non-affective disorder general population by age in males, in 1997-2006, Taiwan……………………………….…………………………………….50 Table 14. Co-morbidity rates (1/10,000) of alcohol dependence, alcohol abuse, drug dependence and drug abuse among Affective disorder cases and viii.
(10) non-affective disorder general population by age in females, in 1997-2006, Taiwan……………………..……….………………………… ..…..….51 Table 15. Relative risk of alcohol dependence, alcohol abuse, drug dependence and drug abuse between incident affective cases and general population by age in males and females, in 1997-2006, Taiwan…….…………………....52. ix.
(11) 圖目錄 Figure1. Chronological trend of incidence (per 10,000) of alcohol dependence, alcohol abuse, drug dependence, drug abuse, schizophrenia and affective disorder…………………………………………………………………….44 Figure2. Incidence of schizophrenia, affective disorder, alcohol dependence, alcohol abuse, drug dependence and drug abuse……………………………………46 Figure3. Relative risk ratios of alcohol dependence, alcohol abuse, drug dependence and drug abuse between incident schizophrenia cases and general insured population by age in males, in 1997-2006, Taiwan………………...………53 Figure4. Relative risk ratios of alcohol dependence, alcohol abuse, drug dependence and drug abuse between incident schizophrenia cases and general insured population by age in females, in 1997-2006, Taiwan………………………53. x.
(12) 第一章. 緒論. 第一節 研究背景與研究動機. 近幾年來,全球成癮藥物的使用有快速的變化。在美國,成癮物質的 使用其終生盛行率可達到 26.6%(1-2) 。成癮藥物的使用不僅成長快速,可 能會同時出現的其他醫療問題的研究也受到重視,像 C 型肝炎(hepatities C virus; HCV)、B 型肝炎(hepatities B virus; HBV)和感染人類免疫缺陷病毒 (human immunodeficiency virus, HIV)者(2) 。台灣也有相關的發現(3-5) 。 除了相關身體疾病外,藥物濫用者其他有關精神疾病之共病問題,在文獻 中也多有討論(6-12)。而藥物戒治也常發現對同時有精神疾病患者之戒癮 效果較差;這也相對影響精神疾病之治療,若未同時發現共病問題,常會 影響療效(13-16) 。台灣在近年來則鮮有人探討藥物濫用與精神疾病之相關 性。而台灣在 1996 年開始全民健保制度後,雖然藥物濫用並沒有納入給付, 但是就醫的患者中仍然有物質使用之診斷,且通常就診者多有其他共病 症,即是較嚴重之個案。本研究是要利用全民健康保險的歸人檔醫療相關 資料探討有關藥物濫用與精神疾病之相關性,以提供臨床及公共衛生措施 參考。. 1.
(13) 第二節 研究的重要性. 藥物戒治時常發現,對同時有精神疾病的患者之戒癮效果較差,相對 地,也影響精神疾病之治療,沒有同時發現共病常會影響療效(13-16) 。 在國外的文獻中發現大約半數的藥物使用患者有精神疾病共病之危險 (10,11) 。精神疾病合併物質使用的比率也很高(17) ,而且會影響疾病之 預後(13-16) 。台灣目前除了 HIV、HBV 和 HCV 的探討外,在藥物濫用與 精神疾病之共病症上則鮮少探討。我們可借此研究先瞭解台灣物質濫用與 精神疾病共病之趨勢與相關性,以提供公共衛生及臨床照顧上之參考。. 第三節 研究目的. 本研究利用國家衛生研究院自承保抽樣檔建立的全民健康保險歸人 檔,1996-2003 年 200,000 人的世代檔的資料,用以分析 1996-2003 年間因 藥物濫用接受門診和住院治療之年代盛行率及發生率。以病例對照研究設 計,比較物質使用疾患者與未使用者間之精神疾病之共病情形及勝算比。 進一步分析 1997-2006 全民健康保險歸人檔 1,000,000 人的世代檔的資料中 精神分裂症、情感性疾患、酒精依賴、酒精濫用、藥物依賴及藥物濫用每 年就醫之盛行率及每年新發生之個案數及發生率。並探討精神分裂症及情 感性疾患兩種疾病分別在酒精依賴、酒精濫用、藥物依賴及藥物濫用方面 與無這兩種疾病者之相對危險性。 2.
(14) 第四節. 研究問題與研究假設. 藥物濫用者的精神疾病的共病率高於對照組。由過去的研究已經知 道,藥物濫用者比一般人有較高的精神疾病,精神疾病患也比一般人有較 高的藥物濫用現象。究竟是藥物濫用引發精神疾病或是精神疾病誘發藥物 使用,仍有爭議。本研究暫不探究其間的相關,但相信藥物濫用者的精神 疾病的共病率高於對照組。. 第五節. 名詞界定. 管制藥品:依據「管制藥品管理條例」第三條所稱管制藥品係指下列 藥品:一、成癮性麻醉藥品;二、影響精神藥品;三、其他認為有加強管 理必要之藥品 。 z 戒斷症狀:當吸毒者一再重複使用壹種或多種藥物,漸漸形成生理依賴 性。一旦藥物投與終止或減少時,所產生之非常焦躁、極度不安之身體 症狀,且有強烈需要服用藥物之慾望。 z 耐受性:藥品之藥效,因其反覆使用而減弱,為維持原有效果則需增加 藥量之現象。 z 共病:兩個疾病發生在同一人身上。. 3.
(15) 第二章 文獻查證 第一節 藥物濫用的定義. 近年來有許多專家學者對藥物濫用提出他们的看法。世界衛生組織 (World Health Organization)早在 1969 年將藥物濫用(drug abuse)定義為藥物 過度使用,且用量超過一般醫療上的用量(18) 。大多認為不當的使用某種 物質,且損害個人的健康或功能,甚至影響社會和職業適應,及危害整個 社會秩序即為藥物濫用(19-21) 。美國「總統麻醉藥物及藥物濫用諮詢委員 會」(The President’s Advisory Commission on Narcotic Drug Abuse)指出藥物 濫用行為應包括: 「個人非依專業人員處方而逕自服用藥物、個人以違法方 法取得藥物、用藥程度到達危害個人健康或社區安全程度」 。此外,美國「全 國大麻與藥物濫用委員會」(National Committee on Marijuana and Drug Abuse) 定義藥物濫用為: 「非基於醫療上的需要,或未依醫師處方而使用藥物, 或雖基於醫療上的需要卻過量始用」 。世界衛生組織則將藥物濫用界定為: 因間斷或持續使用某種藥物所產生的心理、生理依賴與併發症狀(22)。 行政院衛生署管制藥品管理局界定藥物濫用為:1)非基於醫療上的需要 而使用的藥物;2)未依醫師處方而使用藥物;3)雖基於醫療上的需要卻過量 使用藥物;4)用藥程度達到傷害個人健康或社區安全程度(23) 。目前所指 的「藥物」同時也包括了其他非醫療用途的違法藥物 (illicit drugs)。依據「毒. 4.
(16) 品危害防治條例」第二條規定, 「毒品,指具有成癮性、濫用性及對社會危 害性之麻醉藥品與其製品及影響精神物質與其製品。毒品依其成癮性、濫 用性及對社會危害性分為四級;」在其所列的藥品中包含所有非以醫藥及 科學目的為用途的藥物,列屬為管制的非法藥物如麻醉藥品、影響精神物 質及其製品等皆視為使用毒品(24) 。 因此廣義來說, 藥物濫用即是施用法律規定會引起濫用之「毒品」 , 而這些被濫用的「藥物」如強力膠及其他吸入劑(inhalant)等;因並不是均屬 藥物,故有「物質濫用」(substance abuse)一詞的稱呼,但國內仍較普遍使 用「藥物濫用」一詞稱之(25) 。 美國出版的精神疾病診斷及統計手冊第四版(Diagnostic and Statistical Manual of Mental DisorderⅣ;DSM-Ⅳ)將物質分為大麻,安非他命,鴉片類 等 11 類,並定義物質濫用:為一種適應不良的物質使用模式,導致臨床上 重大的損害或痛苦,若在同一年期間內出現下列各項中一項(或一項以 上) ,且症狀從未符合同一物質的物質依賴標準,即為物質濫用:(1)一再的 物質使用,造成無法實踐其工作,學業,或家庭的主要角色責任;(2)在物 質使用對身體有害的情況下,仍繼續使用此物質;(3)一再捲入與物質使用 關聯的法律糾紛;(4)縱然由於物質使用的效應已持續或重複造成或加重此 人的社會或人際問題,仍繼續使用此物質(26) 。此即藥物濫用較狹義的定 義,必須符合上述的診斷標準才能稱之。同時在 DSM-Ⅳ中也有針對物質依. 5.
(17) 賴(substance dependence)明確的作出定義:一種適應不良的物質使用模式, 導致臨床上重要的損害或痛苦,若於同一年期間內出現下列各項中三項以 上,即為物質依賴:(1)耐受性;(2)戒斷症狀,因重複使用某種藥物致使當 很快地減少或停止使用該藥物時,所產生的種種明顯生理症狀的情形;(3) 此物質之攝取常比此人所意願更大量或更長時期;(4)對戒除或控制此物質 使用有持續意願,或多次不成功的努力;(5)花費許多時間於取得此物質的 必要活動,使用此物質,或由物質作用恢復過來;(6)因物質使用而放棄或 減少重要的社會,職業或休閒活動;(7)縱然已知道自己已有持續或重複發 生的身體或心理問題,即可能是物質使用所造成或加重,此人仍繼續使用 此物質(26) 。 目前台灣就精神科的診斷是依據 DSM-Ⅳ,而在臨床上因配合健保局的 分類,故將診斷以國際疾病分類碼第九版(ICD-CM-9)上傳給健保局。故本 篇文章中是根據 DSM-Ⅳ及國際疾病分類碼第九版(ICD-CM-9)做依據來做 分析。ICD code 303 是指有酒精依賴或中毒時之診斷;ICD code 304 是指 藥物依賴之診斷;而 ICD code 305 則包含酒精及藥物濫用,可利用細分碼 區分酒精或藥物濫用。. 第二節 藥物濫用與精神疾病之共病症. 藥物濫用的危害包含個人生理健康和家庭社會的和諧。台灣地區在民. 6.
(18) 國 85 年度監獄及醫療機構因安非他命、海洛因濫用所耗費之社會成本約達 新台幣 104 億 8594 萬元,換算成美元大約 3 億 6793 萬美元,平均每人須 負擔的費用約 17.5 美元,雖然此數值加入查緝等成本,但對社會造成健康、 治安等的危害也是不容小覰的(27) 。Chang 等人(3)在南台灣高雄地區勒 戒所及監所的調查,發現藥物濫用者有 67.2%的 C 型肝炎(hepatities C virus; HCV)感染率。在國外也發現藥癮患者 B 型肝炎(hepatities B virus, HBV)和 C 型肝炎感染率,高於非藥癮患者 (2) 。HIV 的盛行率更是不能忽視,隨著 毒品的注射增加危險性:在泰國可高達 90% (28) 。在台灣自 2003 年起靜 脈藥癮感染 HIV 者也有大幅增加,2005 年新增個案 3448 人中,毒癮者有 2269 人,佔了有 67%之高(4,5)。除了藥物濫用引起的身體疾病外,成癮 藥物引起或共同存在之身心狀況也不容忽視。 藥物濫用中常見有人格疾患(personality disorder)(12)。海洛因使用者以反 社會人格為最常見(29) ,且反社會人格有極高藥物濫用率,治療反社會人 格的藥物濫用也效果較差(30) ,在國外的文獻中也發現增加精神疾病之危 險 (6-9) 。大約半數的人有共病(10,11) 。Kalechistein 發現安非他命使用 者比沒有使用者有兩倍的精神照顧使用率及自殺率 (6)。 有文獻報告有 半數的 MDMA 使用者有憂鬱、精神病、焦慮等精神問題(16) 。安非他命 使用者有憂鬱高達 79%、焦慮 76%、妄想 52%、幻覺 44%(32) ,且因安 非他命或鴉片相關的住院患者中有三成有精神病症。而因成癮藥物對精神. 7.
(19) 心理影響有些與精神病症無法區分,加上鮮少患者因藥物濫用而就醫(7)。 甚至於高達七成的藥物濫用及精神疾病共病者未就醫。因此是成癮藥物引 起精神疾病,或是使原有的病惡化或提早發生不易確定。但由於精神疾病 與藥物濫用的診斷常同時出現(33) ,而藥物戒治也常發現同時有精神疾病 之戒癮效果較差,也相對影響精神疾病之治療,沒有同時發現常會影響療 效(13-16) 。台灣目前除了 HIV、HBV 和 HCV 的探討外,在藥物濫用與精 神疾病之共病症上則鮮少有人探討。. 第三節 精神分裂症的定義. 精神分裂症(schizophrenia)係指患者在思考、知覺、情感、動作、生 活適應等多方面,發生持續性的廣泛性障礙的精神症狀。在美國,精神分 裂症的終生盛行率約 1% ,年發生率約 0.5-5.0/10,000(34) 。依美國心理疾 病診斷及統計手冊(DSM-IV)的分類,其主要症狀如下列(26): ● 病症特徵--在至少一個月期間呈現下列兩種症狀(但奇異內容的幻想或 是批評性或對談性的聽幻覺只要一項即可): ¾ 妄想; ¾ 幻覺; ¾ 錯亂言語(語言毫無組織、顛三倒四、前後不連貫、脫離現實的言語); ¾ 錯亂行為或僵直行動(思考紊亂,有怪異行為); 8.
(20) ¾ 負性症狀(面無表情、情感平淡、思考或語言貧乏、生活退縮等) ● 社會生活障礙--在一般社會生活,工作及人際關係有明顯且長期 性的變化,社會生活程度降低。 ● 患病期間至少六個月以上。 ● 上述病情並非由其他情緒障礙、智能障礙、自閉症、藥物濫用或其他身 體疾病所引起。. 第四節 精神分裂症與酒精和藥物使用之探討. 精神分裂症患者有高達 65%有物質使用之盛行(35) 。在舊金山的精神 科住院病人中發現精神病患者有高達 42%有物質濫用的病史尤其是年輕男 性,並且會使病情易惡化,預後不佳(36) 。精神分裂症患者也是有高自殺 率,而有酒精共病症者其危險性較高(37) 。物質濫用的改善可讓精神分裂 症患者較能適應社會,但持續使用者則較易出現精神病及憂鬱症狀進而影 響預後(38) 。國外的文獻報告:經過 12 個月對初發的精神分裂症患者早 期介入,可以減少物質使用率(39) 。在倫敦的一項研究當中發現,初發的 精神分裂症患者之酒精使用率比 14 個月後的追蹤率要高,在一開始是 30 %,追蹤後降到 15%;大麻則由 32%降到 18.5%。而且持續使用者有病情 較嚴重的現象(40) 。有些患者使用酒精及 khat 是為了要減少精神病藥的副 作用,但他們的濫用卻是增加再住院率的一個危險因子(41) 。但大部分的 9.
(21) 患者不會老實的告知有關酒精或非法藥物的使用,甚至會高達一半以上不 會告知有酒精之使用(42) 。 物質濫用對精神分裂症患者的影響,是影響預後,即增加再住院率及 自殺率,甚至讓他們較難適應社會生活,但他們可能是為了減輕藥物的副 作用等需求而自我用藥。故需要早期評估及介入,以免錯失治療良機。. 第五節 情感性疾患的定義. 1994 年版的美國心理疾病診斷及統計手冊(DSM-IV)將情感性疾患 (affective disorders)改稱情緒性疾患(mood disorders),以強調此類疾病乃因 情緒呈現異常的過高或過低所導致。DSM-IV 中雙極性情緒疾患(bipolar disorders)及重鬱症均屬於 ICD-9-CM 296 的分類。雙極性情緒疾患(bipolar disorders)須包含躁型或輕躁型但可有或沒有鬱型;重鬱症則只要包含鬱 型。在美國重鬱症的終生盛行率在女性約 10-25%,在男性約 5-12%,年發 生率約 10-15%。而雙極情緒疾患終生盛行率約 1%(43) 。其主要症狀,如 下述(26): (一)躁期症狀: 當躁期發作時,患者至少會持續一週以上,呈現下列 1 或 2 可能的狀態: 1.高昂的情緒,過度的樂觀和自信(有此症狀後仍須有以下 3-8 中至少 3 項) 2.易怒的情緒(有此症狀後仍須有以下 3-8 中至少 4 項) 10.
(22) 3.減少對睡眠的需求而且不會感到疲倦 4.自大妄想,膨脹的自我意識 5.身體和心理活動的增加 6.話量多、說話速度快,思考快速和衝動 7.判斷力差,容易分心 8.莽撞而有目的之行為 (二)鬱期症狀: 鬱期發作時,患者至少兩週以上情緒極度低落,在兩個星期中出現五種以 上: 1.一天當中大部分的時間都有憂鬱的情緒,而且每一天都是如此。 2.對有趣或好玩的事物失去了興趣,整天如此,天天如此。 3.胃口減弱,造成體重減輕或發育不良。 4.每天都有失眠或是整天沉睡不醒的現象。 5.每天都有心理生理遲鈍或暴躁的情形。 6.每天都有疲憊和精力不足的現象。 7.每天都會覺得自己一無是處,或是有歉疚感。 8.每天感到無法集中精神,無法思考,無法做決定。. 11.
(23) 9.死亡想法不斷湧現。. 第六節 情感性疾患與酒精和藥物使用之探討. 情緒性疾病(mood disorders)包含憂鬱疾患(depressive disorders)及 雙極情緒疾患(bipolar disorders),這兩種疾病相對於無病者有高勝算會有 物質使用疾患。重鬱症的藥物依賴可高達 9.0,酒精依賴有 3.7;而躁症則 分別是 13.9 及 5.7 (44)。而有重鬱症時同時有高比例的人有酒精及藥物 使用的疾病,分別可達 21%和 9%(45)。ㄧ個在 Zurich, Switzerland 的追 蹤研究也發現有躁症症狀者有較高危險性會發生酒精、大麻、苯二氮平 (benzodiazepine, BZD)依賴或濫用。而重鬱症有較高危險性會發生 BZD 依賴 或濫用(46) 。除了酒精及非法藥物外,針對吸入劑使用者的調查發現,情 緒疾患的終生盛行率有 48%,一年當中有焦慮或憂鬱的比率高達 38%,尤 其以女性為較常見(47) 。故情緒性疾病有藥物濫用的共病是不能忽略。因 為在紐約的一項研究中發現躁鬱症患者合併物質使用疾患有較高的暴力行 為(48) 。而且合併有憂鬱及其他藥物濫用的酒精使用者,有較高的急診使 用率及住院率(49) ,而有共病症通常是精神疾病預後不佳的因子,藥物濫 用也一樣會影響預後(50,51) 。物質濫用也會造成憂鬱症較難治療,症狀較 會持續(52) 。除了影響症狀外,也會影響職業功能(53) 。在加拿大的一 個實驗發現,在沒有工作者中有 27%是因為憂鬱、30%是因為焦慮、20%是. 12.
(24) 因為物質依賴而有 34%是同時存在兩個問題(54) 。除了高比率的共病外, 在一篇針對輕青少年的研究也發現,憂鬱情緒可當作出現物質濫用的預測 因子(55),這是我們不能忽視。. 13.
(25) 第七節 研究架構. 全民健康保險 20 萬人歸人檔. 全民健康保險 100 萬人歸人檔. 1996-2003 年世代檔的資料. 1996-2006 年世代檔的資料. 物質濫用、精神疾病發生率和盛行率及彼 此間之共病情形. 14.
(26) 第三章 研究方法 第一節 研究設計. 本研究先利用 1996-2003 年 200,000 人承保抽樣歸人檔的世代資料分析 1996-2003 年間因藥物濫用接受門診和住院治療之盛行率,及 1997-2003 年 間每年新發生之個案數及發生率。再從新發生的物質使用疾患個案中分析 與精神疾病之共病數。之後設計一巢內病例對照研究,以 1:3 的方式抽對 照樣本,進行病例對照分析,比較物質使用疾患者與未使用者間之精神疾 病之盛行率及勝算比。接著,我们再使用 1996-2006 年全民健康保險歸人檔 1,000,000 人的世代檔,分析精神分裂症及情感性疾患每年就醫之盛行程度 及每年新發生之個案數及發生率。並探討這兩種疾病分別有與酒精依賴、 酒精濫用、藥物依賴或藥物濫用共病之相對危險性。本研究將後二者合併 稱為藥物使用。. 第二節 研究對象. 一開始我们使用 1996 至 2003 年全民健康保險歸人檔,歸人檔是以 2000 年承保人口中隨機抽出 200,000 人,回溯他們從 1996 年至 2000 年的就醫資 料,之後追蹤至 2003 年。另外一個母群體是來自 1996 至 2006 年全民健康 保險歸人檔,這個檔是以 2005 年承保人口中隨機抽出 1,000,000 人,回溯. 15.
(27) 他們從 1996 年至 2005 年的就醫資料,之後追蹤至 2006 年。 物質使用疾病及精神疾病是根據國際疾病分類法第九版(ICD-9-CM) 及門診疾病傷害與牙醫分類(A-code)所定。包含住院及門診病患中主診 斷或次診斷。. 第三節 研究工具的擬定. 全民健康保險歸人檔由國家衛生研究院所提供,為了利用健保資料作 為研究材料,國家衛生研究院先後抽樣建立了兩組全民健康保險歸人檔, 一組為 20 萬人的世代檔,另一組為百萬人的世代檔,本研究包含住院及門 診病患資料。且扣除重複病人及 1996 年新發生之個案數,計算各年的新就 醫人數及人口數,進而估算各年發生率。. 第四節 資料統計與分析. 200,000 人的世代檔的資料,依照編年方式,先計算 1996-2003 每年的 物質使用人數及盛行率,扣除 1996 年的病例和每年重複就醫的病人數後, 可以計算 1997-2003 年間每年新就醫的人數和新就醫率,我們認為此新就醫 率和發生率相近。由於物質使用及精神疾病均具年齡差異,盛行病例的精 神疾病共病分析,分年齡(<20,20-29,>29 歲) 分層分析病例組和對照組 16.
(28) 的共病盛行率,比較病例組和對照組的共病盛行率後,我們選出藥物相關 精神病(drug related psychosis) 、精神分裂症(schizophrenia) 、情感性精神 病(affective psychosis) 、精神官能症(neurotic disorder) 、人格違常疾患 (personality disorder)和酒精依賴等計算其勝算比,並以年齡、性別及人 口密度較正。 1,000,000 人的世代檔的資料分析,先計算 1996-2006 年度的精神分裂 症、情感性精神病、酒精依賴、酒精濫用、藥物依賴和藥物濫用的盛行率, 在計算扣除 1996 年及逐年的盛行數後計算各年的發生率。其次分析精神分 裂症和情感性精神病的性別和年齡別發生率。由於物質使用及精神疾病均 具年齡差異,且有未成年、停經、好發年齡及老年人口目前是定義為大於 65 歲,故分年齡(<20,20-29,30-44,45-64,>=65 歲) 分層分析。接著 分析有這兩項病症分別與沒這兩項病症的酒精和藥物使用者的年齡別和性 別共病發生率,並分別計算精神分裂症病例和情感性精神病病例對無此二 病症一般人口之酒精或藥物使用發生率比值。. 17.
(29) 本研究探討各種病症之 A CODE 及 ICD-9-CM 對照如下: 1996-2003 年 200,000 人承保抽樣歸人檔的世代資料: 1. 藥物使用疾患( drug use disorders ): A-code 216、ICD code 304、ICD code 304。 2. 分析精神疾病(ICD code 290-319)分別如下: • 老年及初老年器官精神狀態(Senile and early senile psychotic condition)ICD code 290 • 酒精性精神病(Alcoholic psychosis)ICD code 291 • 藥物性精神病(Drug related psychosis)ICD code 292 • 暫時性器質性精神病態(Transient organic disorder) ICD code 293 • 其他器質性精神病態,慢性(Other organic brain syndrome,chronic) ICD code 294 • 精神分裂症(Schizophrenia)ICD code 295 • 情感性精神病(Affective psychosis)ICD code 296 • 妄想狀態(Paranoid state)ICD code 297 • 其他非器質性精神病(Other and unspecified reactive psychosis) ICD code 298 • 源於兒童期之精神病(Psychosis with origin specific to childhood) 18.
(30) ICD code 299 • 精神官能症(Neurotic disorder)ICD code 300 • 人格違常(Personality disorder)ICD code 301 • 性心理變態及疾患(Psychosexual disorder)ICD code 302 • 酒癮徵候群(Alcohol dependence syndrome)ICD code 303 • 心因性引起生理功能障礙(Psycho-physiological malfunction) ICD code 306 • 他處未歸類之特殊症狀或徵候群(Other and unspecific special symptoms and syndromes)ICD code 307 • 急性壓力性反應(Acute reaction to stress)ICD code 308 • 環境適應障礙(Adjustment reaction)ICD code 309 • 他處未分類之憂鬱性疾患(Depression, not elsewhere classified) ICD code 311 • 兒童期過動徵候群(Hyper kinetic syndrome in childhood) ICD code 314 • 特殊發展遲滯(Other specified delays in development)ICD code 315 • 精神因素,伴存於他處已歸類之疾病者(Psychotic factors associated with diseases classification)ICD code 316. 19.
(31) • 輕度智能不足(Mild mental retardation)ICD code 317 • 其他特定智能不足(Other specific mental retardation)ICD code 318 • 未明示之智能不足(Unspecific mental retardation)ICD code 319 1996-2006 年全民健康保險歸人檔 1,000,000 人的世代檔, 精神分裂症(Schizophrenia)A code 211,ICD code 295; 情感性精神病(Affective psychosis)A code 212、ICD code 296。 酒精依賴(alcohol dependence)A code 215、ICD code 303、 酒精濫用(alcohol )ICD code 305.00、ICD code 305.000、 ICD code 305.1、ICD code 305.02、ICD code 305.03;藥物依賴 A code 216、ICD code 304;藥物濫用 ICD code 305.2-305.9。. 20.
(32) 第四章 研究結果 第一部分 全民健康保險歸人檔 1996-2003 年 200,000 人的世代檔的資 料。 從 1996 年隨機選取 189,999 歸人檔資料世代資料,分析藥物濫用的盛 行和發生率,我們發現有 796 人被診斷藥物濫用疾患(表 1) 。從 1997 年的 新個案發生率 1.76/10,000 增加到 2003 年的 11.9/10,000,有 6.8 倍的增加; 其盛行率則由 1997 年的 1.92/10,000 增加到 2003 年的 14.7/10,000。就所有 病例以 1:3 的方式隨機抽對照樣本之巢內病例對照研究發現,物質使用疾 患者比非物質使用者有較高之精神疾病盛行率,尤其是情感性精神病(ICD 296) ,藥物濫用疾患者和未使用者的盛行率分別是 40.2/1000 和 1.26/1000; 精神分裂症(ICD 295)共病的盛行率分別是 33.9/1000 和 12.1/1000;酒精 使用共病疾患高達 30.2/1000 而未使用者為 6.7/1000;也發現藥物濫用者有 較高的人格疾患(personality disorder)共病(表 2 和表 3)。表 4 顯現較正 人口密度之後藥物濫用者有精神分裂症的勝算比是 2.85(95%信賴區間為 1.68-4.85),情感性精神病則是 3.64(95%信賴區間 2.43-5.46),多變項分析在 排除官能性疾病後則是 9.12(95%信賴區間 4.81-17.3);人格疾患的勝算比是 7.33(95%信賴區間 2.57-20.9)。包含藥物引發之精神病、其他器質性精神病、 精神分裂症、情感性精神病、人格疾患、酒精依賴及環境適應障礙之整體 勝算則為 4.65(95%信賴區間 3.53-6.13)(表 5)。 21.
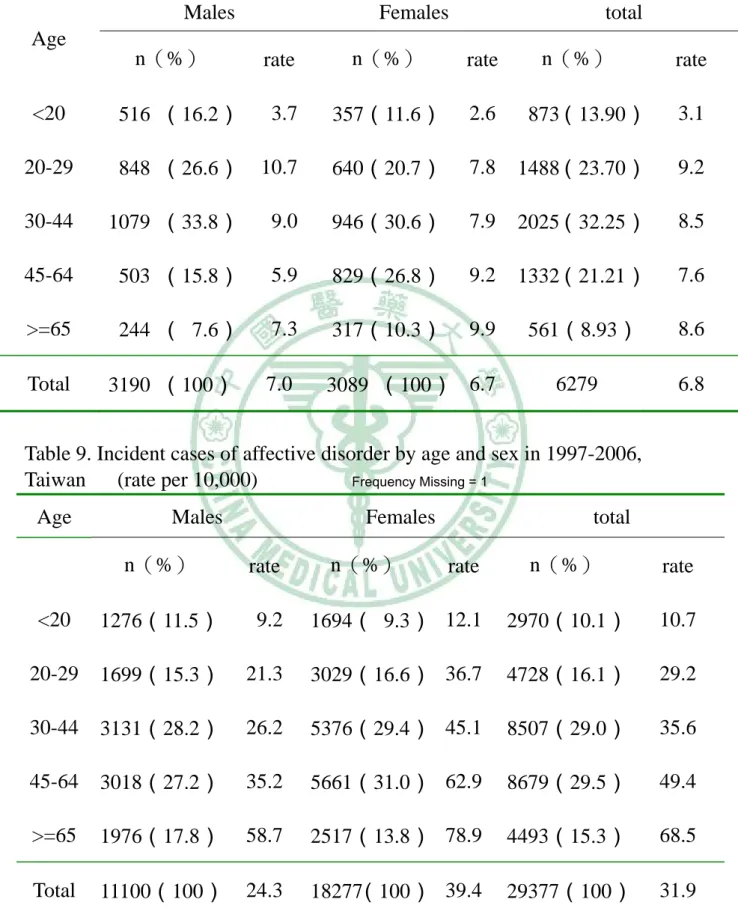
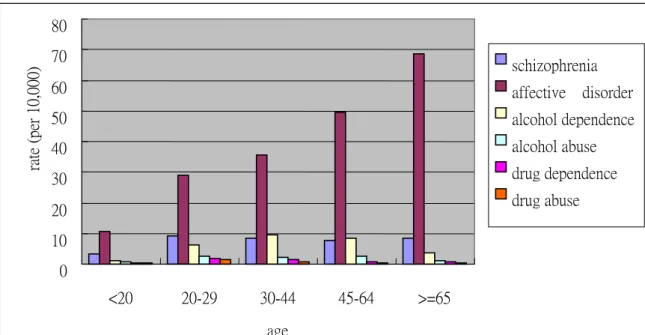
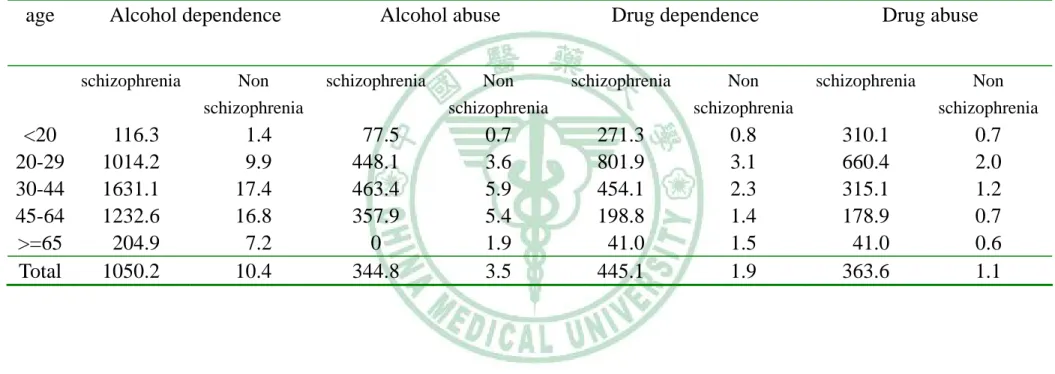
(33) 第二部分 全民健康保險歸人檔 1996-2006 年 1,000,000 人的世代檔的資 料。 我們發現這歸人檔 1,000,000 人口的精神分裂症盛行率由 1996 年的 33.1/10,00 增加到 2006 年的為 48.8/10,000;情感性精神病則由 36.2/10,000 增為 88.3/10,000;酒精依賴也從 4.22/10,000 增到到 13.27/10,000;酒精濫用 由 1.91/10,000 增到 6.63/10,000;藥物濫用從 0.19/10,000 增到 1.86/10,000 (表 6)。而精神分裂症、情感性精神病、酒精依賴、酒精濫用、藥物依賴與藥 物濫用從 1997 年至 2006 年的十年間平均新發生個案率則分別是 6.72/10,000、31.47/10,000、6.97/10,000、2.61/10,000、1.57/10,000 及 1.09/10,000(圖 1,表 7) 。由圖 1 我們可看出精神分裂症的發生率有下降的 趨勢,情感性精神病則在 1999 年後漸趨平穩,而酒精濫用則有上升之現象。 藥物依賴與藥物濫用的發生率則略上升。 全歸人檔人口的性別及年齡分層分析顯示,男性精神分裂症新發患者 在 20-29 歲時達到高峯為 10.7/10,000,而女性則隋年齡增加而持續增加;男 女的總發生率相近,分別為 7.0 和 6.7/10,000(表 8) 。情感性精神病新就醫 率,男女兩性人數均隋年齡增加而增加, 65 歲以上男性達 69.2/10,000,女 性更高為 85.6/10,000,兩性合計平均發生率為 33.9/10,000(表 9) 。圖 2 顯 示情感性精神病的發生不論哪個年齡層均遠高過其他精神病。表 10 說明精 神分裂症患者和對照的年齡別共病發生率,由表 10 可看出男性的精神分裂. 22.
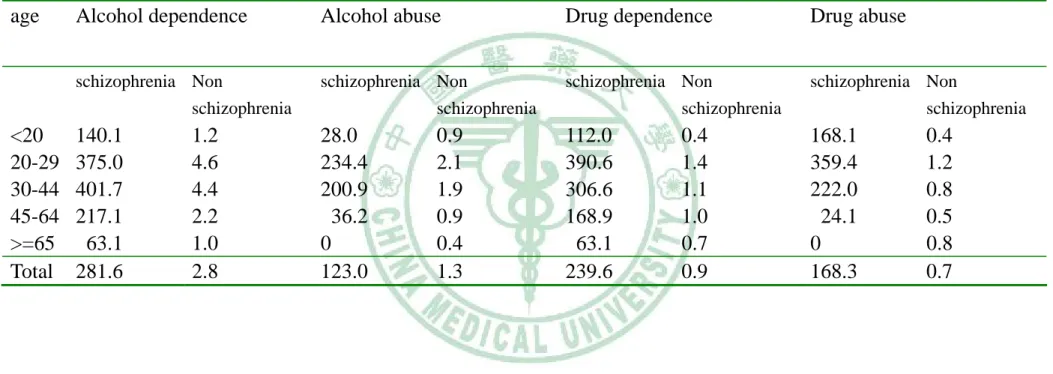
(34) 症患者中有相當高的比率有酒精依賴、酒精濫用、藥物依賴與藥物濫用的 共病症,相對無精神分裂症患者,藥物濫用的危險性比在 20 歲以下者可高 達 419.0(表 12) 。酒精使用共病以 20-29 歲年齡層相對危險性較高;藥物 依賴與藥物濫用則以 20 歲以下者相對危險性較高:藥物依賴與藥物濫用分 別為 361.8 和 419.0,隨年齡遞減(圖 3)。到 65 歲以上的相對危險性分別 為 28.1 和 69.5(表 11) 。女性的精神分裂症患者有酒精依賴、酒精濫用、 藥物依賴與藥物濫用的共病症的比率比男性患者低(表 11) ;她們的酒精依 賴、藥物依賴與藥物濫用相對危險性以 20 歲以下為最高;酒精濫用危險則 以在 20-44 歲間最高(表 12) 。ㄧ般而言,情感性精神病患者的物質使用發 生率較精神分裂症患者的低(表 13,14) 。情感性精神病有酒精依賴、酒精 濫用、藥物依賴、藥物濫用的共病症的年齡分層分析結果顯示,不管是男 性或女性,以 20 歲以下者危險性為最高(表 15) 。. 23.
(35) 第五章討論 台灣在 1996 年開始實施的全民健保制度,雖然不包含監獄中之受刑 人,而且戒癮治療並不包括在給付範圍內,但一開始即有百分之九十的納 保率,至 2003 年納保率高達百分之九十六。故國家衛生研究院利用健保資 料建立的全民健康保險歸人檔,如 1996-2003 年 200,000 人的世代檔的資 料,及 1996-2006 年 1,000,000 人的世代檔的資料,均為提供醫療效應等研 究之好資料。我們利用此資料分析 1996-2003 年及 1996-2006 年間接受治療 的個案。藥物濫用並沒有納入給付、屬於犯罪行為的關係,而且在社會上 是有汙名,唯有較嚴重的個案或有共病症者才會就醫。Watkins 等發現不超 過 3 成的藥物濫用者有尋求精神醫療的照護(33) 。而全民健康保險歸人檔 的資料在藥物濫用部分的代表性和完整性可能低估,但由於其投保率高達 96%,所記載的資料一般而言代表國人的就醫照護的整體,完整性及代表 性很高,因此可做為醫療照護的研究素材。故在藥物濫用方面仍可觀察其 趨勢。 我們從研究中發現,從 1997 年至 2003 年就醫者中新增有藥物使用問 題者有 6.8 倍的成長,1997 年有 34 人(發生率是 1.92/10,000);2003 年有 230 人 (發生率是 14.7/10,000)。但此數字在台灣仍有可能低估,因為並非 所有物質使用者均會使用健康照護系統,在研究中所收納的個案大多是有 其他共病症的患者。在美國的一項流行病學研究中發現(8)有 72% 的藥 24.
(36) 物濫用者至少有一個精神疾病的共病。我們的結果發現藥物濫用者的精神 疾病的共病率是 53.1 %。推估這原因可能是因為精神疾病的共病就醫者少 於因身體疾病而前來就醫,或是因為民眾對精神疾病症狀的隱瞞,還是醫 療照護系統並沒有留意到精神疾病的共病現象,以至於低估了精神疾病的 共病率。有物質使用者比非使用有較高的比率會因為精神疾病使用照護系 統(9) 。這顯示有物質使用者發生精神疾病的機會較高。大部分有共病者 並未就醫,美國一項研究發現有一半以上的人沒有接受治療(10)。 我們發現物質使用者有精神分裂症比一般人的勝算比是 2.8,在調整人 口密度及排除精神官能症後的勝算比是 5.94,與 Regier 發現物質使用者有 精神分裂症比一般人的勝算比 4.6 稍高。在我們的結果中也顯現有較高危 險有情感性精神病,與精神分裂症均屬於重大精神疾病,這與國外的研究 相符合(4-6) 。精神官能症在結果中並沒有增加危險性,甚至會降低,這與 國外的研究不一致。美國一項流行病學研究發現焦慮也會增加使用物質的 比率(9) 。可能是精神官能症在台灣的健保系統中被低估,而低估的原因 可能是未就醫、自我用藥、未被合理診斷等因素。有物質使用者在含精神 分裂症、情感性精神病、藥物引發的精神病、器質性精神病、人格疾患、 酒精依賴及環境適應障礙等的整體勝算比是 4.65。在人格疾患的勝算比 8.56(95% 信賴區間 2. 71-27.0)與國外的研究相近(12)。 我們由 20 萬人的的歸人檔發現與重大精神疾病,如精神分裂症(A 211. 25.
(37) or ICD 295)及情感性疾患(A212 or ICD 296)在藥物濫用人口中的共病率很 高,所以我們進一步分析 1997-2006 全民健康保險歸人檔 1,000,000 人的世 代檔的資料。 歸人檔全人口精神分裂症的年均發生率是 7/10,000,與美國的年發生率 0.5-5/10,000(34)比相對偏高,而年均發生率較高的原因可能是全民健康 保險實施後前幾年就醫率會高於一般的發生率之故。而盛行率較低,低於 百分之ㄧ,可能是就醫率偏低之故,文獻也有提到精神分裂症的就醫率約 5 成(35) 。國人情感性疾患的盛行率有逐年增加的情形,代表民眾就醫的情 形改善。酒精依賴、酒精濫用、藥物依賴和藥物濫用的盛行率也有增加之 情形,因為健保只給付一般疾病照護病不包括戒癮治療,故來就醫者多有 其他急性或慢性的疾病,有些未使用者可能會低估。而增加的趨勢則有可 能是健保是全民保險,故長期下來累積的個案推測應該是逐漸增加,之後 達到一個水平,另外一個可能是長期使用藥物或酒精後可能有其他的共病 症而前來就醫的機會增多。 分析精神分裂症和情感性精神病的性別和年齡別發生率,發現男性精 神分裂症較高比率發生在 20-29 歲最高,女性則有較晚發之趨勢,這與國外 的趨勢相近(34) 。情感性精神病就醫人口有偏高的現象,可能與延遲就醫 的情形相關(56) 。或是疾病原本的好發年齡即較晚。接著分析有這兩項疾 病的人,分別與沒這兩項病症者,比較其有酒精和藥物使用的年齡別和性. 26.
(38) 別的共病發生率及比值,這兩種疾病的明顯高於一般無此病的投保人口, 與國外的研究相符合(35,43-45) 。但因來就醫者多有疾病才會前來,故可 能高估其危險比,但因資料含括其他疾病之就醫,故仍可當作一個參考。. 研究限制. 這個研究有幾個限制。因為藥物濫用是社會所不允許,且非法藥物的使用 更是犯罪行為,所以大部分的民眾不會主動告知醫護人員,除非有相關的 疾病,或是有主動詢問。這可能造成本研究對物質使用疾患有所低估。更 何況全民健保的納保人口中並沒有包括監獄中的受刑人,而且對單純戒癮 的照護也沒有給付,這也是會造成低估的原因。另外,全民健保局的資料 來源的診斷是來自於不同的醫療院所不同的專科醫師,對物質使用疾患和 精神疾病的診斷可能有不同的態度和看法,尤其是較輕微的精神官能症。 這與訪談式調查的研究不同,也會使得本研究會有所偏差。也因為全民健 保沒有給付單純戒癮的照護,會收納至本研究的人可能都是有其他疾病就 醫者,可能也有較多的比例有因藥物或酒精之共病症的問題,這會造成我 們對精神疾病共病的高估。. 27.
(39) 第六章 結論與建議 第一節 結論. 我們的研究發現,近幾年來台灣在物質使用人口增加快速,我們也發現物 質使用者中的精神疾病共病率明顯的比一般人口高。精神分裂症及情感性 疾病的就醫率因全民健保實施後有逐漸增加的現象,但與國外的盛行率比 較起來,顯然有低估的現象。但由我們的研究仍可發現精神分裂症及情感 性疾病在酒精依賴、酒精濫用、藥物依賴和藥物濫用的發生率上高於一般 無病的人口。雖然我們無法從本研究中去探討彼此的因果關係,我們仍須 注意物質使用者與精神疾病的共病現象,以減少治療的困難性並在臨床上 做適當的處理。且因為目前對精神疾病的診斷及照護仍可能少於實際的盛 行率,也提醒我們需要對民眾的精神健康多留意並給予適當的協助。. 第二節 應用與建議. 我們從本研究發現在台灣物質使用疾患與精神疾病有高度密切的相關,由 於共病現象會影響治療的策略及效果,在臨床上我們須注意這個情形,以 減少治療的干擾因子並在臨床上做適當的處理。目前對精神疾病的診斷及 照護仍可能少於實際的盛行率,在公共衛生上可能需要對民眾的精神健康 衛教,減少汙名化的現象,鼓勵民眾留意精神衛生並尋找適當的協助。目. 28.
(40) 前我們無法從本研究中去探討物質使用疾患與精神疾病彼此的因果關係, 將需要進一步的研究來探討。. 29.
(41) 參考文獻 1. Kessler RC, McGonagle KA, Zhao S, Nelson CB, Hughes M, Eshleman S, Wittchen HU, Kendler KS. Lifetime and 12-month prevalence of DSM-III-R psychiatric disorders in the United States. Results from the National Comorbidity Survey. Arch Gen Psychiatry 1994;51(1):8-19. 2. Jiang JJ, Dubios F, Driss F, Carnot F, Thepot V, Pol S, Berthelot P, Brechot C, Nalpas B. Clinical impact of drug addiction in alcoholics. Alcohol Alcoholism 1995;30(1):55-60. 3. Chang CJ, Lin CH, Lee CT, Chang SJ, Ko YC, Liu HW. Hepatitis C virus infection among short-term intravenous drug users in southern Taiwan. Europ J Epidemiol 1999;15:597-601. 4. 楊靖慧:台灣愛滋病流行現況與防治政策。感染控制雜誌 2006;16 (1) :17-23。 5. 王甯祺:愛滋病在台灣的新危機:靜脈毒癮與 C 型肝炎。感染控制雜 誌 2006;16(1):24-26。 6. Regier DA, Farmer ME, Rae DS, Locke BZ, Keith SJ, Judd LL, Goodwin FK. Co-morbidity of mental disorders with alcohol and other drug abuse: results from the Epidemiologic Catchment Area (ECA) Study. JAMA 1990; 264:2511-2518. 7. Kessler RC, Nelson CB, McGonagle KA, Edlund MJ, Frank RG, Leaf PJ. The epidemiology of co-occurring addictive and mental disorders: implications for prevention and service utilization. Am J Orthopsychiat.1996;66(1):17-31. 8. Kessler RC, Nelson CB, McGonagle KA, Liu J, Swartz M, Blazer DG. Co-morbidity of DSM-III-R major depressive disorder in the general population: results from the US National Comorbidity Survey. Br J of Psychiatry 1996:17–30. 9. Grant BF, Stinson FS, Dawson DA, Chou SP, Dufour MC, Compton W, Pickering RP, Kaplan K. Prevalence and co-occurrence of substance use disorders and independent mood and anxiety disorders: results from the 30.
(42) National Epidemiologic Survey on Alcohol and Related Conditions. Arch Gen Psychiatry 2004; 61:807–816 10. Harris KM, Edlund MJ. Use of mental health care and substance abuse treatment among adults with co-occurring disorders. Psychiatr Serv 2005; 56:954-959. 11. Macleod J, Oakes R, Copello A, Crome I, Egger M, Hickman M, Oppenkowski T, Stokes-Lampard H, Davey-Smith G. Psychological and social sequelae of cannabis and other illicit drug use by young people: a systematic review of longitudinal, general population studies. Lancet 2004;363:1579-88. 12. Craig RJ. Personality characteristics of heroin addicts: review of empirical research 1976-1979. Int J Addict 1982;17:227-48. 13. Mueser KT, Yarnold PR, Levinson DF, Singh H, Bellack AS, Kee K, Morrison RL, Yadalam KG. Prevalence of substance abuse in Schizophrenia: demographic and clinical correlates. Schizophr Bull 1990;16:31-56. 14. Shaner A, Khalsa ME, Roberts L, Wilkins J, Anglin D, Hsieh SC. Unrecognized cocaine use among schizophrenia patients. Am J Psychiatry 1993; 150:758-62. 15. Wyatt SA, Ziedonis D. Psychological and psychiatric consequences of amphetamines. in Tarte RE, et al. ed. Handbook of Substance Abuse: Neurobehavioral Pharmacology. NY: Plenum Press 1998:529-44. 16. Schifano F. Chronic atypical psychosis associated with MDMA (ecstasy) abuse. Lancet 1991;338:1335. 17. 莊淑棻、吳守謙、蔡文瑛、李志恆:台灣地區查獲之 MDMA 和 Ketamine 毒品分析。台灣衛誌 2005;24(3):264-273。 18. 林憲:臨床精神醫學。台北:茂昌圖書出版 1982:239。 19. Schladdt RG, Shannon PT. Drug of Choice: Current Perspectives on Drug Use.(2nd ed.). Englewood Cliffs, NJ: Prentice-Hall 1986. 31.
(43) 20. 蘇東平:台灣青少年之藥物濫用(上) 。臨床醫學 1980;5(4):299-305。 21. 林麗芳:國內藥癮治療機構藥物濫用者之流行病學研究。行政院衛生 署八十八年下半年及八十九年度自行研究計劃 2000。 22. 教育部:校園藥物濫用機制。教育部電子報 No. 033; Http://Epaper.edu.tw. 93 年 5 月 28 日。 23. 行政院衛生署管制藥品管理局:反毒專欄。http://www.nbcd.gov.tw。 民國 97 年 6 月。 24. 法務部:毒品危害防制條例。http://law.moj.gov.tw。民國 97 年 04 月 30 日 修正。 25. 李志恆:我國藥物濫用簡史及現況。藥物濫用。台北:行政院衛生署 管制藥品管理局 2002:6。 26. 孔繁鐘、孔繁錦:DSM-IV 精神疾病診斷準則手冊。台北:何紀出版 社 1996。 27. 余萬能、胡文琳、和李志恆:台灣地區藥物濫用社會成本推估出報。 中華衛誌 1998;17(4):360-369。 28. Poshyachinda V. Drug injection and HIV infection among the population of drug abusers in Asia. Bull Narcot 1993; 45:77-90. 29. Craig RJ. Prevalence of personality disorders among cocaine and heroin. Addicts Subst Abus. 2000;21(2):87-94. 30. Goldstein RB, Compton WM, Pulay AJ, Ruan WJ, Pickering RP, Stinson FS, Grant BF. Antisocial behavioral syndromes and DSM-IV drug use disorders in the United States: results from the National Epidemiologic Survey on Alcohol and Related Conditions. Drug Alcohol Depend, 2007;90(2-3):145-58. 31. Schifano F, Di Furia L, Forza G, Minicuci N, Bricolo R. MDMA consumption in the context of polydrug abuse: a report on 150 patients. Drug Alcohol Depend 1998;50:85-90. 32. Hall W, Hando J, Darke S, Ross J. Psychological morbidity and route of administration among amphetamine users in Sydney, Australia. Addiction 1996;91:81-7. 32.
(44) 33. Watkins KE, Burnam A, Kung FY, Paddock S. A national survey of care for persons with co-occurring mental and substance use disorders. Psychiatr Serv 2001;52:1062-8. 34. Sadock BJ, Sadock VA. Kaplan and Sadock’s Synopsis of Psychiatry: behavior sciences, clinical psychiatry. In: Schizophrenia. 9th ed. Philadelphia, PA: Lippincott Willlams and Wilkins,2003: 472. 35. Wobrock T, D'Amelio R, Falkai P. Pharmacotherapy of schizophrenia and comorbid substance use disorder. A systematic review. Nervenarzt. 2008;79(1):17-8, 20-2, 24-6 passim. 36. Vaz Carneiro S, Borrego M, Psychosis and substance abuse. Acta Medica Portug. 2007;20(5):413-22. 37. McGirr A, Turecki G. What is specific to suicide in schizophrenia disorder? Demographic, clinical and behavioural dimensions. Schizophr Res. 2008; 98(1-3):217-24. 38. Potvin S, Stip E, Lipp O, Roy MA, Demers MF, Bouchard RH, Gendron A. Anhedonia and social adaptation predict substance abuse evolution in dual diagnosis schizophrenia. Am J Drug Alcohol Abuse. 2008; 34(1):75-82. 39. Archie S, Rush BR, Akhtar-Danesh N, Norman R, Malla A, Roy P, Zipursky RB. Substance use and abuse in first-episode psychosis: prevalence before and after early intervention. Schizophr Bull, 2007;33(6):1354-63. 40. Harrison I, Joyce EM, Mutsatsa SH, Hutton SB, Huddy V, Kapasi M, Barnes TR. Naturalistic follow-up of co-morbid substance use in schizophrenia: the West London first-episode study. Psycho Med,2008;38(1):79-88. 41. Bimerew MS, Sonn FC, Kortenbout WP. Substance abuse and the risk of readmission of people with schizophrenia at Amanuel Psychiatric Hospital, Ethiopia. Curationis. 2007; 30(2):74-81. 42. de Beaurepaire R, Lukasiewicz M, Beauverie P, Castera S, Dagorne O, 33.
(45) Espaze R, Falissard B, Giroult P, Houery M, Mahuzier G, Matheron I, Niel P, Padovani P, Poisson N, Richier JP, Rocher J, Ruetsh O, Touzeau D, Visinoni A, Molimard R. Comparison of self-reports and biological measures for alcohol, tobacco, and illicit drugs consumption in psychiatric inpatients. Eur Psychiatry, 2007;22(8):540-8. 43. Sadock BJ, Sadock VA. Kaplan and Sadock’s synopsis of psychiatry: behavior sciences, clinical psychiatry. In: Mood Disorders. 9th ed. Philadelphia, PA: Lippincott Willlams and Wilkins, 2003: 535. 44. Grant BF. Comorbidity between DSM-IV drug use disorders and major depression: results of a national survey of adults. J Subst Abuse 1995; 7:481–497. 45. Grant BF, Harford TC. Comorbidity between DSM-IV alcohol use disorders and major depression: results of a national survey. Drug Alcohol Depend 1995; 39:197–206 46. Merikangas KR, Herrell R, Swendsen J, Rossler W, Ajdacic-Gross V, Angst J. Specificity of bipolar spectrum conditions in the comorbidity of mood and substance use disorders: results from the Zurich cohort study. Arch Gen Psychiatry,2008;65(1):47-52. 47. Wu LT, Howard MO. Psychiatric disorders in inhalant users: results from The National Epidemiologic Survey on Alcohol and Related Conditions. Drug Alcohol Depend, 2007;88(2-3):146-55. 48. Garno JL, Gunawardane N, Goldberg JF. Predictors of trait aggression in bipolar disorder. Bipolar Disord, 2008;10(2):285-92. 49. Stewart SH. Alcoholics in acute medical settings have increased risk for other drug, mood, and personality disorders. Int J of Psychiatry Med, 2007; 37(1):59-67. 50. Merikangas KR, Kalaydjian A. Magnitude and impact of comorbidity of mental disorders from epidemiologic surveys. Curr Opin Psychiatry, 2007; 20(4):353-8. 51. Kessler RC. The epidemiology of dual diagnosis. Biol Psychiatry, 2004;56:730-737. 34.
(46) 52. Watkins KE, Paddock SM, Zhang L, Wells KB. Improving Care for Depression in Patients With Comorbid Substance Misuse. Am J Psychiatry, 2006; 163:125–132. 53. Wilk J, West JC, Rae DS, Regier DA. Relationship of comorbid substance and alcohol use disorders to disability among patients in routine psychiatric practice. Am J Addict,2006;15:180-185. 54. el-Guebaly N, Currie S, Williams J, Wang J, Beck CA, Maxwell C, Patten SB. Association of mood, anxiety, and substance use disorders with occupational status and disability in a community sample. Psychiatr Serv, 2007;58(6):863. 55. Mason WA, Hitchings JE, Spoth RL. Emergence of delinquency and depressed mood throughout adolescence as predictors of late adolescent problem substance use. Psycho Addict Behav, 2007; 21(1):13-24. 56. Borges G, Wang PS, Medina-Mora ME, Lara C, Chiu WT. Delay of first treatment of mental and substance use disorders in Mexico. Am J Public Health, 2007;97(9):1638-43.. 35.
(47) 圖表. 36.
(48) Table 1. The prevalence and incidence of drug use disorders identified from the National Health Insurance cohort data in Taiwan, 1996-2003. Year. Population size. Prevalence n (rate per 10000). 1996. 189999. 66(3.47). 1997 1998 1999 2000 2001 2002 2003 Total. 192724 195050 197486 200000 199495 198989 193966 195964. 37(1.92) 62(3.18) 100(5.06) 104(5.20) 113(5.66) 180(9.05) 286(14.7) 796. 37. New claims n (rate per 10000) 34(1.76) 56(2.87) 86(4.35) 86(4.30) 86(4.31) 152(7.64) 230(11.9) 730.
(49) Table 2. The prevalence of mental disorders in cases with drug use disorders diagnosed in the National Health Insurance cohort in Taiwan, 1996-2003.. Psychiatric diseases. Senile and early senile psychotic condition Alcoholic psychosis Drug related psychosis Transient organic disorder Other organic brain syndrome (chronic) Schizophrenia Affective psychosis Paranoid state Other and unspecified reactive psychosis Psychosis with origin specific to childhood Neurotic disorder Personality disorder Psychosexual disorder Alcohol dependence syndrome Psycho-physiological malfunction Other and unspecific special symptoms and syndromes Acute reaction to stress Adjustment reaction Depression, not elsewhere classified Hyper kinetic syndrome in childhood Other specified delays in development Psychotic factors associated with diseases classification Mild mental retardation Other specific mental retardation Unspecific mental retardation. Age(years) <20. 20-29. >29. Total. N=37. N=186. N=573. N=796. n(rate/1000). n(rate/1000). n(rate/1000). n(rate/1000). 0 0 2(54.1) 0 0 2(54.1) 0 0 0 0 0 0 0 2(54.1) 1(27.0) 0. 0 0 15(80.6) 2(10.8) 4(21.5) 7(37.6) 10(53.8) 1(5.38) 1(5.38) 0 17(91.4) 5(26.9) 0 2(10.8) 2(10.8) 10(53.8). 1(1.75) 5(8.73) 15(26.2) 4(6.98) 9(15.7) 18(31.4) 43(75.0) 2(3.49) 6(10.5) 1(1.75) 76(132.6) 7(12.2) 1(1.75) 20(34.9) 5(8.73) 19(33.2). 1(1.26) 5(6.28) 32(40.2) 6(7.54) 13(16.3) 27(33.9) 53(66.6) 3(3.77) 7(8.79) 1(1.26) 93(116.8) 12(15.1) 1(1.26) 24(30.2) 8(10.1) 29(36.4). 0 0 0. 1(5.38) 5(26.9) 0. 2(3.49) 3(5.24) 6(10.5). 3(3.77) 8(10.1) 6(7.54). 0 1(27.0) 0. 0 0 0. 1(1.75) 0 1(1.75). 1(1.26) 1(1.26) 1(1.26). 0 0 0. 0 1(5.38) 0. 2(3.49) 0 1(1.75). 2(2.51) 1(1.26) 1(1.26). 38.
(50) Table 3. The prevalence of mental disorders identified for controls in the National Health Insurance cohort in Taiwan, 1996-2003.. Psychiatric diseases. Senile and early senile psychotic condition Alcoholic psychosis Drug related psychosis Transient organic disorder Other organic brain syndrome (chronic) Schizophrenia Affective psychosis Paranoid state Other and unspecified reactive psychosis Psychosis with origin specific to childhood Neurotic disorder Personality disorder Psychosexual disorder Alcohol dependence syndrome Psycho physiological malfunction Other and unspecific special symptoms and syndromes Acute reaction to stress Adjustment reaction Other specified non-psychotic mental disorder. Depression, not elsewhere classified Other conduct disorder Unspecific emotional disturbance, in childhood and adolescent Hyper kinetic syndrome in childhood Other specified delays in development Psychotic factors associated with diseases classification Mild mental retardation Other specific mental retardation Unspecific mental retardation. Age (years) <20. 20-29. >29. Total. N=111. N=558. N=1719. N=2388. n(rate/1000). n(rate/1000). n(rate/1000). n(rate/1000). 0 0 0 0 0 1(9.0) 1(9.0) 0 0 0 2(18.0) 1(9.0) 0 0 2(18.0) 0. 0 0 2(3.58) 1(1.79) 3(5.38) 7(12.5) 9(16.1) 1(1.79) 3(5.38) 0 49(87.8) 0 12(21.5) 3(5.38) 5(8.96) 20(35.8). 23(13.4) 8(4.65) 1(0.58) 5(2.91) 9(5.24) 21(12.2) 36(20.9) 3(1.75) 12(6.98) 0 259(150.7) 4(2.33) 0 13(7.56) 45(26.2) 79(46.0). 23(9.63) 8(3.35) 3(1.26) 6(2.51) 12(5.03) 29(12.1) 46(19.3) 4(1.68) 15(6.28) 0 310(129.8) 5(2.09) 12(5.03) 16(6.70) 52(21.8) 99(41.5). 1(9.0) 0 0 1(9.0). 0 7(12.5) 2(3.58) 5(8.96). 7(4.07) 3(1.75) 6(3.49) 23(13.4). 8(3.35) 10(4.19) 8(3.35) 29(12.1). 0 0. 2(3.58) 0. 4(2.33) 1(0.58). 6(2.51) 1(0.42). 0 3(27.0) 0. 0 1(1.79) 0. 1(0.58) 0 3(1.75). 1(0.42) 4(1.68) 3(1.26). 0 1(9.0) 1(9.0). 2(3.58) 1(1.79) 1(1.79). 0 2(1.16) 2(1.16). 2(0.84) 4(1.68) 4(1.68). 39.
(51) Table 4. Odds ratios of psychiatric diseases estimated in nested case-control groups of the National Health Insurance cohort in Taiwan, 1996-2003. Drug abuse. Odds ratio (95%CI interval). Yes N=796. No N=2388. n(%). n(%). Univariable. 32(4.0). 3(0.13). 33.3(10.2-109.0). 764(96.0). 2385(99.9). 1.0. 13(1.63). 12(0.50). 3.29(1.49-7.23). 3.22(1.46-7.10). 3.67(1.44-9.36). 783(98.4). 2376(99.5). 1.0. 1.0. 1.0. 27(3.39). 29(1.21). 2.85(1.68-4.85). 2.83(1.67-4.82). 5.94(2.94-12.0). 769(96.6). 2359(98.8). 1.0. 1.0. 1.0. 53(6.66). 46(1.93). 3.63(2.43-5.44). 3.64(2.43-5.46). 9.12(4.81-17.3). 746(93.3). 2342(98.1). 1.0. 1.0. 1.0. 93(11.7). 310(13.0). 0.89(0.69-1.14). 0.87(0.68-1.11). 703(88.3). 2078(87.0). 1.0. 1.0. Adjusted the density of population Including disorder. neurotic Not including neurotic disorder. Drug related psychosis Yes No Other organic brain syndrome Yes No Schizophrenia Yes No Affective psychosis Yes No Neurotic disorder Yes No Personality disorder. **. 33.7(10.3-110.3). **. 1.0. *. ***. ***. **. 7.29(2.56-20.8) 12(1.51) 5(0.21) Yes 784(98.5) 2383(99.8) 1.0 No Alcohol dependence *** 4.61(2.44-8.72) 24(3.02) 16(0.67) Yes 772(97.0) 2372(99.3) 1.0 No Others/unspecific 29(3.64) 99(4.15) 0.87(0.57-1.33) Yes 767(96.4) 2289(95.9) 1.0 No * :p<0.05, **:p<0.001, ***:p<0.0001. 40. 85.8(11.6-632.8). ***. 1.0. *. ***. ***. **. *. ***. ***. **. 7.33(2.57-20.9). 8.56(2.71-27.0). 1.0. 1.0. ***. ***. 4.50(2.38-8.53). 6.01(2.80-12.9). 1.0. 1.0. 0.88(0.58-1.34). 1.15(0.67-1.96). 1.0. 1.0.
(52) Table 5. Odds ratios of psychiatric disease (any of drug related psychosis, other organic brain syndrome, schizophrenia, affective psychosis, personality disorder, alcohol dependence syndrome, adjustment reaction) estimated in nested case-control groups of the National Health Insurance cohort in Taiwan, 1996-2003. Drug use disorder Psychiatric disease. Yes No. Yes. No. N=796 n(%). N=2388 n(%). 131(16.5) 665(83.5). 97(4.1) 2291(95.9). 41. Odds ratio (95% Confidence interval). 4.65(3.53-6.13) 1.0.
(53) Table 6. Prevalence of schizophrenia, alcohol and drug use disorders by year in 1997-2006, Taiwan. Year. 1996 1997 1998 1999 2000 2001 2002 2003 2004 2005 2006. Schizophrenia. n 2790 3036 3287 3476 3619 3888 4170 4353 4656 4758 4847. rate 33.1 34.7 37.1 38.7 39.7 41.9 44.6 45.7 48.7 47.6 48.8. Affective disorder. n 3050 4911 6298 5321 5207 5770 6307 6885 7816 8776 8776. rate 36.2 56.2 71.1 59.2 57.2 32.1 67.4 72.3 81.8 87.8 88.3. Alcohol dependence n 355 511 653 797 889 964 949 1011 1323 1402 1319. Alcohol abuse. rate 4.2 5.8 7.4 8.9 9.8 10.4 10.2 10.6 13.8 14.0 13.3. 42. n 161 51 71 140 208 227 287 381 501 629 659. rate 1.9 0.6 0.8 1.6 2.3 2.4 3.1 4.0 5.2 6.3 6.6. (rate per 10,000). Drug dependence. n 128 120 139 135 172 149 203 226 310 349 253. rate 1.5 1.4 1.6 1.5 1.9 1.6 2.2 2.4 3.2 3.5 2.6. Drug abuse. n 16 17 26 66 103 117 105 143 212 236 185. rate 0.2 0.2 0.3 0.7 1.1 1.3 1.1 1.5 2.2 2.4 1.9.
(54) Table 7. Incidence of schizophrenia, alcohol and drug use disorders by year in 1997-2006, Taiwan (rate per 10,000) Year. Schizophrenia. Affective disorder. 1997 1998 1999 2000 2001 2002 2003 2004 2005 2006 total. n 872 774 702 604 620 595 580 596 497 443 6283. n 3507 3895 2753 2524 2566 2660 2737 2876 3139 2721 29378. rate 10.0 8.7 7.8 6.6 6.7 6.4 6.1 6.2 5.0 4.5 6.7. rate 40.1 44.0 30.7 27.7 27.6 28.4 28.8 30.1 31.4 27.4 31.8. Alcohol dependence n 447 526 599 628 662 628 648 842 807 719 6506. rate 5.1 5.9 6.7 6. 9 7.1 6.7 6.8 8.8 8.1 7.2 7.0. 43. Alcohol abuse. n 45 67 133 186 190 230 298 375 470 443 2437. rate 0.51 0.76 1.48 2.04 2.05 2.46 3.13 3.92 4.70 4.46 2.61. Drug dependence. n 108 121 107 134 107 151 154 219 223 137 1461. rate 1.2 1.4 1.2 1.5 1.2 1.6 1.6 2.3 2.2 1.4 1.6. Drug abuse. n 17 25 63 98 103 86 126 177 190 133 1018. rate 0.2 0.3 0.7 1.1 1.1 0.9 1.3 1.9 1.9 1.3 1.1.
(55) 圖 1. 50 45. Alcohol dependence. 40. Alcohol abuse. 35 Drug dependence. rate (per 10,000). 30 25. Drug abuse. 20 15. Schizophrenia. 10 5. affective disorder. 0 1997. 1998. 1999. 2000. 2001. 2002. 2003. 2004. 2005. 2006. year. Figure 1. Chronological incident trend of (per 10,000) of patients receiving care for alcohol dependence, alcohol abuse, drug dependence, drug abuse, schizophrenia and affective disorder. 44.
(56) Table 8. Incident cases of schizophrenia by age and sex in 1997-2006, Taiwan (rate per 10,000) Frequency Missing = 4 Males. Females. total. Age n(%). rate. n(%). rate. n(%). rate. <20. 516 (16.2). 3.7. 357(11.6). 2.6. 873(13.90). 3.1. 20-29. 848 (26.6). 10.7. 640(20.7). 7.8. 1488(23.70). 9.2. 30-44. 1079 (33.8). 9.0. 946(30.6). 7.9. 2025(32.25). 8.5. 45-64. 503 (15.8). 5.9. 829(26.8). 9.2. 1332(21.21). 7.6. >=65. 244 ( 7.6). 7.3. 317(10.3). 9.9. 561(8.93). 8.6. Total. 3190 (100). 7.0. 3089 (100) 6.7. 6279. 6.8. Table 9. Incident cases of affective disorder by age and sex in 1997-2006, Frequency Missing = 1 Taiwan (rate per 10,000) Age. Males. Females. n(%). rate. <20. 1276(11.5). 9.2. 20-29. 1699(15.3). 30-44. n(%). total n(%). rate. 1694( 9.3) 12.1. 2970(10.1). 10.7. 21.3. 3029(16.6) 36.7. 4728(16.1). 29.2. 3131(28.2). 26.2. 5376(29.4) 45.1. 8507(29.0). 35.6. 45-64. 3018(27.2). 35.2. 5661(31.0) 62.9. 8679(29.5). 49.4. >=65. 1976(17.8). 58.7. 2517(13.8) 78.9. 4493(15.3). 68.5. Total. 11100(100). 24.3. 18277(100) 39.4. 29377(100). 31.9. 45. rate.
(57) 圖 2. 80 rate (per 10,000). 70. schizophrenia. 60. affective. 50. alcohol dependence. 40. alcohol abuse. 30. drug dependence drug abuse. 20 10 0 <20. 20-29. 30-44. 45-64. >=65. age Figure 2. Incidnece of schizophrenia, affective disorder, alcohol dependence, alcohol abuse, drug dependence adn drug abuse. 46. disorder.
(58) Table 10. Co-morbidity rates (1/10,000) of alcohol dependence, alcohol abuse, drug dependence and drug abuse among schizophrenia cases and non-schizophrenia general population by age in males, in 1997-2006, Taiwan. age. <20 20-29 30-44 45-64 >=65 Total. Alcohol dependence. Alcohol abuse. Drug dependence. Drug abuse. schizophrenia. Non schizophrenia. schizophrenia. Non schizophrenia. schizophrenia. Non schizophrenia. schizophrenia. Non schizophrenia. 116.3 1014.2 1631.1 1232.6 204.9 1050.2. 1.4 9.9 17.4 16.8 7.2 10.4. 77.5 448.1 463.4 357.9 0 344.8. 0.7 3.6 5.9 5.4 1.9 3.5. 271.3 801.9 454.1 198.8 41.0 445.1. 0.8 3.1 2.3 1.4 1.5 1.9. 310.1 660.4 315.1 178.9 41.0 363.6. 0.7 2.0 1.2 0.7 0.6 1.1. 47.
數據




+7


相關文件
有無患過傳染病、地方性疾病 (如烏腳病)和其他重要內科 疾病,發病日期、使用藥物及診療情況。對患者以前所患 的疾病,診斷確定者可用病名 ;
而考量到 Covid-19 重症病患的需求,醫院的重症病床數量格外重要。根據統 計,在 OECD 國家間,每十萬人擁有之重症病床數量差距可達 10 倍(如下圖)。. 歐盟疾病管制局 (European
Sam: I scraped my knee and bumped my head.. Smith: What happened
straight brown hair dark brown eyes What does he look like!. He has short
While Korean kids are learning how to ski and snowboard in the snow, Australian kids are learning how to surf and water-ski at the beach3. Some children never play in the snow
I am writing this letter because I want to make a new friend in another country.. Maybe you will come to Gibraltar
Sam: It’s really nice, but don’t you think it’s too expensive.. John: Yeah, I’m not going to buy it, but I wish I could
在使用Paxlovid治療的5天 療程完畢後再5天才開始 高血脂症或心血管疾病患者,有在服用史塔汀類的降膽固醇藥物(Statin) 例如: Simvastatin
