遺傳諮詢的品質對唐氏症兒的父母之心理適應、家庭功能、
婚姻關係和親子關係之影響(III)
計畫類別: 個別型計畫 計畫編號: NSC93-3112-H-002-005- 執行期間: 93 年 05 月 01 日至 94 年 04 月 30 日 執行單位: 國立臺灣大學醫學院精神科 計畫主持人: 高淑芬 共同主持人: 李明濱 計畫參與人員: 陳明坊 報告類型: 完整報告 處理方式: 本計畫可公開查詢中 華 民 國 94 年 7 月 26 日
行政院國家科學委員會補助專題研究計畫
□期中進度報告
遺傳諮詢的品質對唐氏症兒的父母之心理適應、家庭功能、婚姻關係
和親子關係之影響(第三年)
計畫類別:
;
個別型計畫 □ 整合型計畫
計畫編號:NSC 93- 3112 - H - 002 - 005 -
執行期間: 93 年 5 月 1 日至 94 年 4 月 30 日
計畫主持人:高淑芬 副教授
共同主持人:李明濱 教授
計畫參與人員: 陳明坊
成果報告類型(依經費核定清單規定繳交):□精簡報告
;
完整報告
本成果報告包括以下應繳交之附件:
□赴國外出差或研習心得報告一份
□赴大陸地區出差或研習心得報告一份
□出席國際學術會議心得報告及發表之論文各一份
□國際合作研究計畫國外研究報告書一份
處理方式:除產學合作研究計畫、提升產業技術及人才培育研究計畫、列
管計畫及下列情形者外,得立即公開查詢
□涉及專利或其他智慧財產權,□一年□二年後可公開查詢
執行單位:國立台灣大學醫學院精神科
中 華 民 國 九十四 年 七 月 三十 日
前言: 唐氏症(DS)是智能不足最常見的染色體疾患,有典型的外表特徵。在醫 療、經濟、家庭負擔及個人學習表現上,患有唐氏症對其個人、家庭、和社會有 巨大的衝擊。 目的: 為了瞭解對唐氏兒父母接受遺傳諮詢的現況,父母對遺傳諮詢經驗的滿意 程度,以及影響遺傳諮詢滿意度之相關因素。並探討唐氏症對於家庭的親子關 係、養育方式、父母親的心理適應、婚姻關係之影響。 方法: 樣本包括的 45 個唐氏症家庭和 50 位非唐氏症家庭。在唐氏症家庭中,共 有43 位母親及 34 位父親完成所有的測驗評估,只有 32 個家庭父親與母親皆完 成測驗。本研究工具包含半結構式會談以獲得遺傳諮詢的內容和懷孕生產史,以 及自填問卷評估父母的心理適應和生活品質、親子關係和孩子的氣質和情緒行 為。 結果: 研究結果顯示唐氏兒父母的遺傳諮詢 82%由醫生進行,平均諮詢時間為 26 分鐘(標準差= 23.5),只有 20%的父母對遺傳諮詢的經驗感到滿意。諮商者 的態度冷漠、敷衍,提供的資訊不夠充足,進行諮詢的地點不適當,進行時間太 短等都讓父母感到不滿意。而父母當時的情緒、經濟狀況、外向性格也會影響遺 傳諮詢的滿意度。唐氏兒有較多的行為問題,其父母親顯現出較多的心理症狀, 而其手足較易受到父母的忽略。 結論:目前國內對唐氏兒父母的遺傳諮詢,大多是由醫生單方面告知父母有關唐 氏症的相關訊息,缺乏雙方的溝通,以及提供心理支持、後續心理輔導、治療的 工作。增進遺傳諮詢品質最重要的是改進諮商者的態度,給予父母宣洩情緒的機 會和提供足夠的資訊,以協助唐氏兒家庭心理、生活、親子關係等各方面的適應。 除了父母的心理健康之外,對唐氏兒之手足的照顧也應該受到重視。 關鍵詞:唐氏症、遺傳諮詢、父母適應、家庭功能、教育方式
Context: Down syndrome (DS) is the most common genetic form of mental
retardation with a typical physical phenotype. Its impact on individual, family, and society is tremendous in terms of medical treatment, financial cost, family burden, and personal underachievement.
Objective: To examine the content and pattern of genetic counseling and to
determine the factors affecting the extent of satisfaction with genetic counseling among parents of children with DS. Also, we examined parental psychopathology, parenting style, and behavioral characteristics among children with DS, their siblings, and controls.
Methods: The sample consisted of one exposed group, including 45 families of
children with DS, and one unexposed group, including 50 families of children without DS. Among DS families, only 34 families were assessed completely, including 43 mothers and 34 fathers. Each parent received a semi-structured interview including information about patterns of genetic counseling and their satisfaction with
counseling; the questionnaires about parental mental status, family function, dyadic adjustment, parenting style, and child’s behavioral problems and temperament.
Results: Physicians had informed 82% of the parents that their child had DS. The
mean duration of the counseling session was 26 minutes (standard deviation = 23.5). The majority of parents reported that they did not have a chance to ask question or express their feelings. They also noted that they did not receive enough information regarding the etiology, outcome, and treatment of DS. Predictors of increased satisfaction with genetic counseling included extroverted parents and lower parental economic status, positive counselor’s attitude, longer duration of counseling, more information provided, and no negative immediate emotional reaction. Parents of children with DS suffered from more psychopathology, children with DS
demonstrated more behavioral problems, and their siblings may not get enough care or parental control than their counterparts.
Conclusion: This study suggests the need for better doctor-patient communication
and for greater attention to the scope of genetic counseling sessions for DS in Taiwan. The mental health prevention of parents and siblings of children with DS need to be emphasized not less than that of children with DS.
中 文 摘 要...I Abstract ... II 目 錄... III 前 言...1 研 究 目 的...2 文 獻 探 討...3 研 究 方 法...5 研究對象...5 研究步驟...5 研究工具...5 統計分析...7 結 果...8 一、社會人口學資料...8 二、遺傳諮詢的內容和形式...8 三、遺傳諮詢的滿意度與影響因素...9 四、唐氏兒與非唐氏兒父母的人格特質與心理狀態...9 五、唐氏兒與非唐氏兒父母的婚姻與家庭關係...10 六、唐氏兒、其手足與非唐氏兒三組在行為與情緒問題之差異...10 七、唐氏兒、其手足與非唐氏兒之父母與其親子關係之差異...10 八、父母親在親子關係之差異...10 結 論...11 一、遺傳諮詢的現況...11 二、影響遺傳諮詢滿意度的因素...11 三、理想的遺傳諮詢...12 四、唐氏兒父母的心理適應、婚姻關係與家庭關係...12 五、唐氏兒的行為問題與親子關係...12 六、唐氏兒之手足的行為問題與親子關係...12 七、研究的限制...13 八、臨床意涵...13 參 考 文 獻...14 附 表...20
Table 1 Sample characteristics...20
Table 2 Circumstances at the first contact for genetic counseling...21
Table 3 Content of genetic counseling about Down syndrome ...22
Table 4 Association between parents’ characteristics and their satisfaction with genetic counseling...23
Table 6 Dyadic adjustment and Family function by Down syndrome and control parents ...25 Table 7 Emotional and behavior problems by children with Down syndrome, siblings and controls ...26 Table 8 Parental attitude toward children with Down syndrome, siblings and controls...26 附錄一 遺傳諮詢的內容及影響諮詢滿意度的相關因子—以唐氏症為例...27 附錄二 Parenting, Parental Characteristics, and Behavioral Problems among Children with Down Syndrome, Their Siblings and Controls ...44
前 言
近二十多年來基因科技的快速進展,不論是在分子遺傳或是遺傳流行病學,都是 最熱門的研究方向。隨著基因科技在生物科學上的廣泛應用,有關基因科技的倫理問 題逐漸受到重視。許多有關遺傳、染色體異常或基因突變的相關疾病的基因診斷、諮 詢及後續處置,是否合乎倫理和人性,以及是否符合社會的規範等議題,不斷的在醫 療、法律、家庭和社會的情境中發生。然而到目前為止,並沒有研究深入去探討目前 台灣有關遺傳諮詢的現況,以及遺傳諮詢的品質及內容對患者以及其家人的影響程 度,或者發展出協助家庭去照顧和教養這些基因異常患者的相關政策。 唐氏症(Trisomy 21)是造成智能不足最常見的染色體疾患,其盛行率是 1-1.5/1000 活產兒,除了智能不足外,唐氏症患者具有典型的一些外表特徵,也常併發心臟、血 管、胃腸及血液方面的異常。患有唐氏症對患者本身及他的家庭和社會將會帶來巨大 的衝擊,目前國內少有針對遺傳諮詢以及其相關影響的研究資料。本研究的目的希望 以唐氏兒為例,探討有關遺傳諮詢的內容和形式,以及遺傳諮詢對唐氏兒及其父母和 兄弟姊妹的影響。此外,也希望藉由這個研究的結果可提供國人對目前遺傳諮詢現況 的瞭解,並且與國外的情形進一步的比較,以作為改進遺傳諮詢的專業品質的參考資 料。研 究 目 的
1. 在瞭解台灣目前針對唐氏症兒父母的遺傳諮詢的內容和型態。 2. 唐氏兒之父母對於遺傳諮詢經驗的滿意狀況。 3. 以父母的年齡、教育程度、社經地位、人格特質以及遺傳諮詢的經驗探討影響遺 傳諮詢滿意度的因素。 4. 探討唐氏兒的父母和非唐氏兒父母在身心狀況、婚姻問題以及家庭關係之差異。 5. 比較唐氏兒、其手足以及非唐氏兒這三組,在行為和情緒問題之差異。 6. 探討唐氏兒、其手足以及非唐氏兒之父母與他們的親子關係之差異。 7. 探討父親與母親對待孩子方式的差異。文 獻 探 討
基因工程的廣泛研究,不論是在分子遺傳結構上或是基因流行遺傳病學,都是 生物學或是藥學一直以來重要而且熱門的研究方向,未來,基因工程也將是研究方 向一個重要指標。當科學家們致力於基因遺傳的探討和研究時,其發展對人類生活 可能產生之巨大影響,近十年來,有關基因工程倫理問題,也伴隨著基因工程在生 物學上的應用而逐漸受到重視。遺傳諮詢,就是在強調倫理的原則之下,著重專業 遺傳諮詢師應該要以何種方式以及如何傳遞給個案有關基因遺傳上的發現,並解釋 因為此項基因遺傳的變化可能衍生而來的心理社會之功能改變(Murray, 1976)。 遺傳諮詢一向被認為是醫療人員與個案之間複雜的溝通過程,其中包含了與個 案以及家族成員討論產前檢查中發現呈現陽性反應之遺傳疾病、新生兒伴隨有醫療 上之問題,以及家族史中帶有的遺傳疾病。大部分的遺傳諮詢師認為有效的而且有 益處的遺傳諮詢有幾項倫理原則及人性價值應該被尊重而且是重要的:尊重個案自 主性以及非指導性語氣、友善的、不具攻擊性的;誠實並且真誠的告知真實情況;豐 富性的資料或是資源提供(Yarborough, Scott, & Dixon, 1989)。遺傳諮商師的態度是 決定基因諮商成功與否,以及個案日後社會心理是否能適應良好之重要因素(Wertz & Fletcher, 1988)。本研究提供醫學倫理用於遺傳諮詢之檢驗,所採用之個案為唐氏症兒童,因為 唐氏症(trisomy21)是遺傳性疾病中最常見的一種,是造成智能不足最主要已知的 染色體疾患,其盛行率是1-1.5/1000 活產兒(Stoll, Alembik, Dott, & Roth, 1998)。唐 氏兒生理以及臉部外觀表現特徵有:新生兒期持續性低血壓、眼球向上且向外歪 斜、短且鼻梁平坦的鼻子以及虹膜中間有白色班點。唐氏兒手指短小,小指頭向內 彎,有些可能缺少手掌骨,掌紋可能只有單條。頭顱圍通常很小甚至是極小(Cooley & Graham, 1991; Stoll, et al., 1998)。由於以上這些特徵,使得唐氏兒自嬰兒期即開 始就與其他非唐氏症兒童顯得十分不同。唐氏兒伴隨有低智商(平均智商低於50), 隨著年齡增加還有下降之趨勢。唐氏兒還常有心血管方面之疾病(Freeman, et al., 1998)、腸胃畸形(Marty, et al., 1995; Torfs, Bateson, & Curry, 1992)、血液異常 (Kivivuori, Rajantie, & Siimes, 1996; Zipursky, Brown, Christensen, Sutherland, & Doyle, 1997)以及癲癇症(Dalton & Crapper-McLachlan, 1986)。並且,他們在三十歲 左右就漸漸地產生一些衰老的徵兆,例如:稀少的頭髮、乾燥而且縐折的皮膚、神 經性的改變等等。這些與其他兒童不同的成長改變以及過程,唐氏兒本身面臨的低 學業成就,家庭所需要付出之龐大教育或是醫療費用造成唐氏兒不僅是個人而且是 其整個家庭甚至社會巨大而顯著的影響(Stoll, et al., 1998)。 在台灣,母親產檢若發現結果未出生之胎兒患有唐氏症,其遺傳諮詢經常是由 婦產科醫師執行。大部分的父母也都會選擇經由人工流產的方式結束胎兒生命 (Williamson, Harris, Church, Fiddler, & Rhind, 1996; Yagel & Anteby, 1998)。而對於唐 氏兒的父母,遺傳諮詢是由婦產科醫師、小兒科醫師、護理人員或是遺傳諮詢師執 行,大都決定於第一次診斷為唐氏症的地點和時間,因此,並不是由專業遺傳諮詢 人員執行。研究顯示,父母被告知唐氏症診斷的過程,會對其日後的適應以及他們 對待孩子的方式產生影響(Springer & Steele, 1980),適當和高品質的遺傳諮詢以及
對唐氏兒持續的生理照顧,可以幫助唐氏兒父母親在新生兒時期逐漸適應壓力。國 外的研究顯示:多數的父母對於被告知診斷結果的遺傳諮詢經驗感到不滿意。不滿 意的原因包括:諮商者的態度冷漠、缺乏溝通技巧;提供與疾病相關之訊息不夠充 足,許多疑問仍沒有得到答案;告知的時機不適當,過早或是太晚告知;告知時沒 有配偶或孩子在身旁;諮商者所具備之基本知識不足;諮商者傳遞過多負面訊息 (Cunningham, Morgan, & McGucken, 1984; Hedov, Wikblad, & Anneren, 2002; Quine & Pahl, 1986; Quine & Rutter, 1994; Spahis & Wilson, 1999)。
遺傳諮詢的進行可以參考下列指導原則:(1)環境的地點與陳設,(2)評估 個案家庭之背景資料、教育程度及過去經驗,(3)選擇一個最適宜個案家庭當時 所遭遇情境的策略,最後(4)評估個案家庭是否有確實瞭解被提供的資訊(Garwick, Patterson, Bennett, & Blum, 1995)。對父母而言,諮商者的專業知識、諮詢時機、諮 詢環境、諮商者的態度為影響遺傳諮詢滿意度之重要指標(Spahis & Wilson, 1999)。 在遺傳諮詢時,多數父母希望能夠說出自己的疑問、表達自己的情緒。父母希望可 以儘早知道有關孩子的診斷;希望諮商者在諮詢時能表現出支持與同理心;希望能 夠得到與孩子的疾病有關的完整訊息(Quine & Pahl, 1986; Quine & Rutter, 1994)。除 了第一次的遺傳諮詢之外,接下來的心理支持以及相關建議也是很重要的,除了心 理輔導或治療以外,與其他有唐氏兒家庭接觸也可以成為唐氏兒父母安慰與建議的 來源(Quine & Pahl, 1987)。
研究顯示,養育一個有發展障礙的孩子,會給父母親、家庭關係、親子關係帶來 負面的影響(Bristol, Gallagher, & Schopler, 1988; Dyson, 1997a)。而部分研究顯示許多 家庭在這種情況下仍能夠有效率的去應對、適應(Bennett & DeLuca, 1996b; Ferguson, 2002)。國內相關研究顯示台灣的唐氏兒家庭受到多樣及程度不一的衝擊(黃璉華, 1994),父母認知真相後會出現不同的調適行為(蔣欣欣 & 喻永生, 1997)。一般而言, 母親擔負了起較多照顧孩子的責任(Krauss, 1993),國外大多數的研究顯示養育唐氏兒 對於母親的影響會大於父親(Beckman, 1991a; Goldberg, Morris, Simmons, Fowler, & Levison, 1990a; Pelchat, et al., 1999),台灣的研究也顯示相同的結果(Cheng & Tang, 1995)。與正常孩子的母親相比,唐氏症兒的母親經歷了較多的焦慮、憂鬱、以及心 理壓力(Shek & Cheung, 1990)。除了父母親之外,唐氏兒的手足同樣會面對心理適應 的問題(Dyson, 1989)。部分研究認為唐氏兒之手足會出現較多焦慮、行為、情感問題 (Lavigne & Ryan, 1979a; Poznanski, 1969a),而其他研究認為並無影響(Lobato, Barbour, Hall, & Miller, 1987; McHale, Sloan, & Simeonsson, 1986)。目前並無研究探討父母親對 唐氏兒及其手足教養方式的差異。 根據以上研究結果,本研究的目的在探討:(1)台灣目前針對唐氏症兒父母的遺 傳諮詢的內容和型態;(2)唐氏兒之父母對於遺傳諮詢經驗的滿意狀況;(3)以父母 的年齡、教育程度、社經地位、人格特質以及遺傳諮詢的經驗探討影響遺傳諮詢滿意 度的因素;(4)唐氏兒的父母和非唐氏兒父母在身心狀況、婚姻問題以及家庭關係之 差異;(5)唐氏兒、其手足以及非唐氏兒這三組,在行為和情緒問題之差異;(6)唐 氏兒、其手足以及非唐氏兒之父母對他們的教養方式之差異;(7)父親與母親對待孩 子方式的差異。希望依據此研究,探討唐氏症對一個家庭的影響,將唐氏兒家庭接受 遺傳諮詢的經驗及想法提供國內作為改進遺傳諮詢方式與品質的參考。
研 究 方 法
研究對象
本研究樣本包括 45 個 1 歲到 10 歲經醫師診斷並領有殘障手冊患有唐氏症的兒童 之家庭,以及50 個非唐氏症兒童之家庭。其中 32 個家庭父母親皆完成此研究,共有 43 位母親及 34 位父親完成所有的評估。研究步驟
本研究經過台大醫院倫理委員會的同意進行,經由三個途徑收集個案家庭:(1) 經由台大醫院的病歷資料確定為唐氏症的病人,寄發研究目的和進行方式的說明信給 家長,以徵得其同意進行訪談;(2)透過中華民國唐氏症關愛協進會先徵詢有唐氏症 孩子的父母參加研究的意願;(3)地毯式地接洽台北縣市所有的特殊教育發展中心和 國小的特教班的老師,詢問有無患有唐氏症的學生,若有,且老師同意代轉研究說明 書給家長,則再經由老師轉交研究說明書。 最後有 45 個唐氏症家庭參與研究,一位有家庭親職諮詢背景的碩士負責會談母 親及父親以獲得有關被告知有唐氏症孩子的遺傳諮詢經驗,以及訪談母親以獲得懷孕 生產史。父母親並且完成自填式問卷。父母親同意會談錄音者,給予錄音,以做為控 制研究品質,和將來質性研究分析之用。會談的內容經由會談者和第一作者共同討論 以決定最符合受訪者的情形之代碼。研究工具
壹.自填量表部份(TableⅠ和 TableⅡ): 一. 簡式性格量表(MPI)簡式性格量表(Maudsley Personality Inventory, MPI)乃李明濱等人(M.B. Lee, Hsien, Lin, & Lee, 1990a; M. B. Lee & Lee, 1990)改編自 Eysenck(H.J. Eysenck, 1962)的性格量表,包括 30 題項目,涵蓋神經質、外向及社會期 許三個向度。
二. 簡式症狀量表(BSRS)
簡式症狀量表(Brief Symptom Rating Scale,BSRS)是李明濱等人(M. B. Lee & Lee, 1990)根據 Derogatis(Derogatis, Lipman, & Covi, 1973; Derogatis, Rickels, & Rock, 1976)所編著之 SCL-90-R 修訂並翻譯成中文,BSRS 共包 含50 個項目,分為 5 級評分,臨床應用證明此量表的評估有良好的信、效 度,能找出10 個向度的症狀;包括身體化症狀、強迫性症狀、人際間敏感、 憂鬱、焦慮、敵意、畏懼、疑心、離群、附加症狀。
三. 兩性適應量表(DAS)
兩性適應量表(Dyadic Adjustment Scale,DAS)編自 Spanier(Spanier, 1976), 為32 題的自陳式量表,主要為評估婚姻及兩性適應。包括四個向度:意見一 致性(dyadic consensus)、滿意度(dyadic satisfaction)、凝聚力(dyadic
cohesion)、表達愛的方式(affectionate expression)。 四. 家庭適應量表(FACEIII)
家庭適應凝聚量表(Family Adhesion and Cohehsion Evaluation Scale, FACEIII)編自 Olslon(Olson, 1991)為 30 題的自陳式量表,其著重於評估家 庭系統中的凝聚力和適應性(Green, Harris, Forte, & Robinson, 1991a; Olson, 1991)。使用 Circumplex Model Approach,在 FACES III 得到高分代表其為 一平衡的家庭類型;低分則代表極端型,而所謂的平衡型,是指其能以一 較為有效的方式來運作整個家庭系統。
五. 親子關係量表(PBI)
親子關係量表(Parental Bonding Inventory, PBI)乃編自 Parker (Parker, 1979) 的題量表,共25 題,父母親對待他們的孩子的行為模式和態度,可分別為 照顧(care)和保護(protection)兩個量表。在照顧分量表得到高分,反應 出富有感情及溫暖;相對的,低分則指出父母親態度為拒絕、冷淡或冷漠。 在保護分量表得高分顯示父母有過度保護、控制、命令及鼓勵孩子心理依 賴的傾向;低分則表示父母允許或鼓勵兒童獨立及自主。而保護分量表又 可進一步分為兩向度,分別為「鼓勵行為自主」和「拒絕心理上的獨立自 主」。 六. 兒童行為量表(CBCL) 兒童行為量表包括112 題,中文版 CBCL 以建立信效度,且廣用於兒童行 為研究,衍生出八大行為問題:不專心、焦慮/憂慮、攻擊性、違法、身體 抱怨、社交問題、退縮、怪異想法,及二大行為面向;內在性及外在性行 為症候群(Achenbach, 1991a)。 貳.會談量表: 一. 社會人口學資料 包括父母基本資料、居住地、父母的工作、教育程度及婚姻狀態。 二. 遺傳諮商會談量表 包括遺傳諮商的時機、地點、型式、內容、諮商者、對基因諮商的整體評估 以及理想中的基因諮商方式。 三. 懷孕史、生產史及發展史 包括母親懷孕前、期間、分娩過程的情形以及孩子出生後的發展情形和滿意 度。 四. 養育史 包括養育經驗、養育子女的精神及經濟付出
統計分析
本研究樣本的社會人口學特質以及遺傳諮詢的形式和內容等描述性結果主以百 分比來呈現類別變項,以平均值(標準差)來呈現連續變項。將此十個向度的分數加總 後作為代表遺傳諮詢滿意度的分數,以一般線性模式分析父母的人格特質、遺傳諮詢 經驗與遺傳諮詢滿意度之間的關係,並將所有與遺傳諮詢滿意度有顯著關係的變項(p < 0.1)納入為預測變項,進行統計模式選擇,以找出影響遺傳諮詢滿意度的最重要的 因素。在比較唐氏兒與非唐氏兒父母的身心適應,婚姻關係與家庭關係上用的是多變 量分析。對小孩子的態度以及比較唐氏症兒童、其手足及非唐氏症兒童三組的行為問 題上,因為彼此之間並非獨立事件,因此是用混合統計法(Mixed - model)的變異數分 析,並以Duncan's multiple range test 進行事後比較。對於類別變項的比較是用卡方檢 定作初步的分析。所有的統計分析以SAS 8.2 (SAS Institute Inc, Cary, NC)軟體執行。結 果
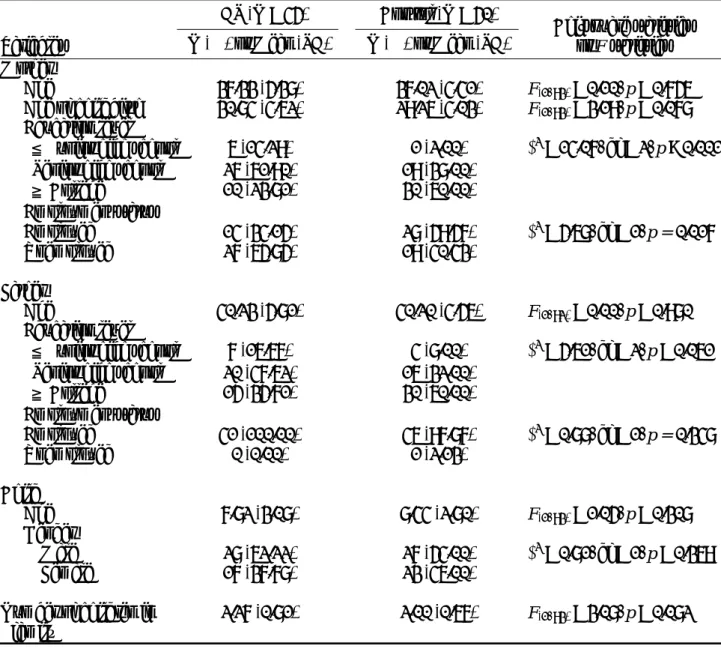
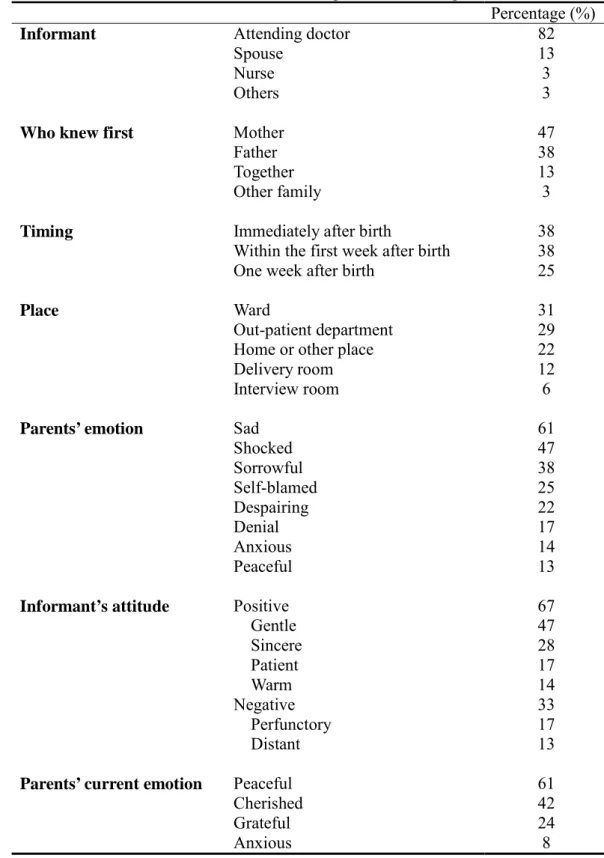
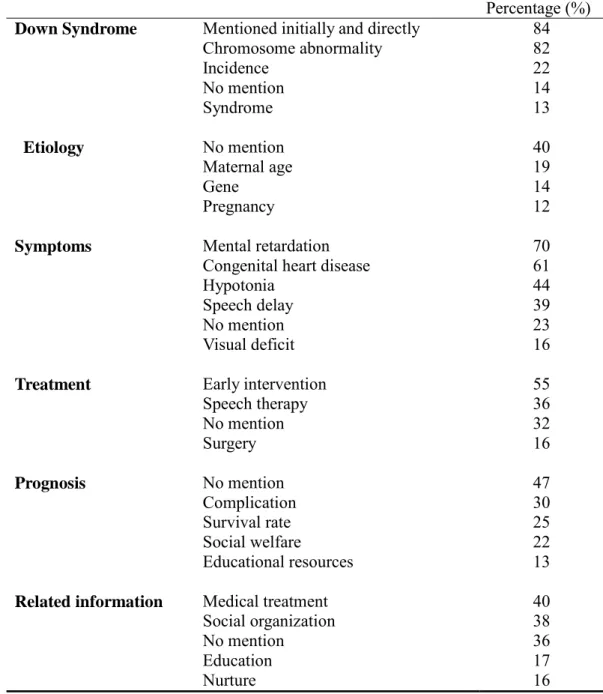
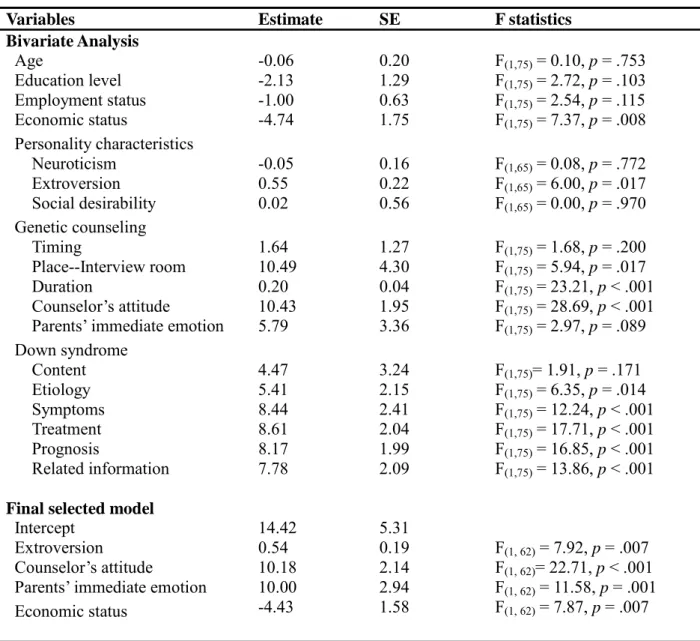
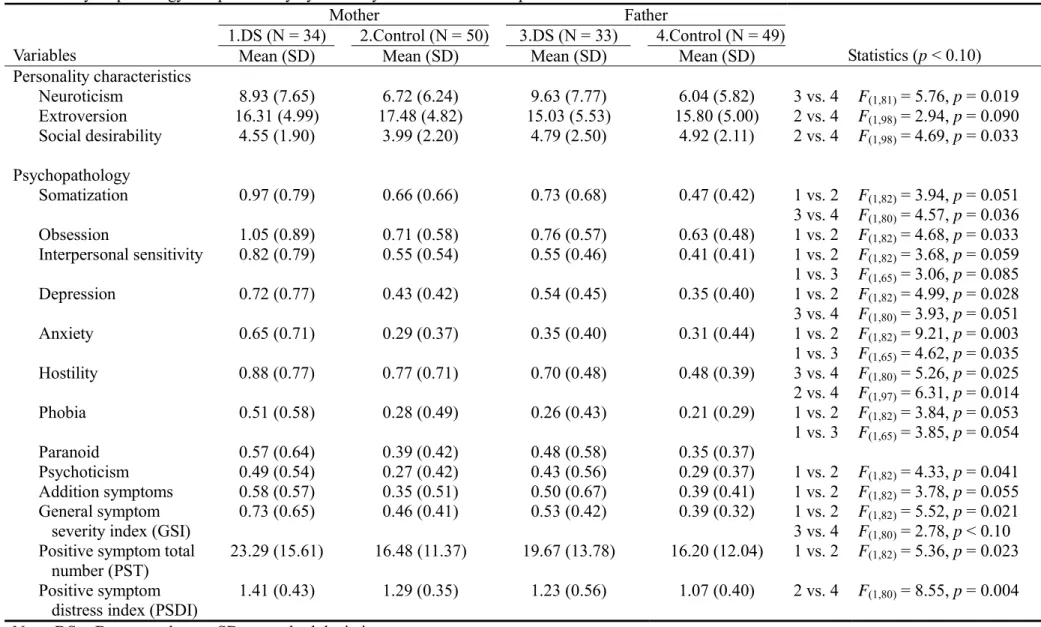
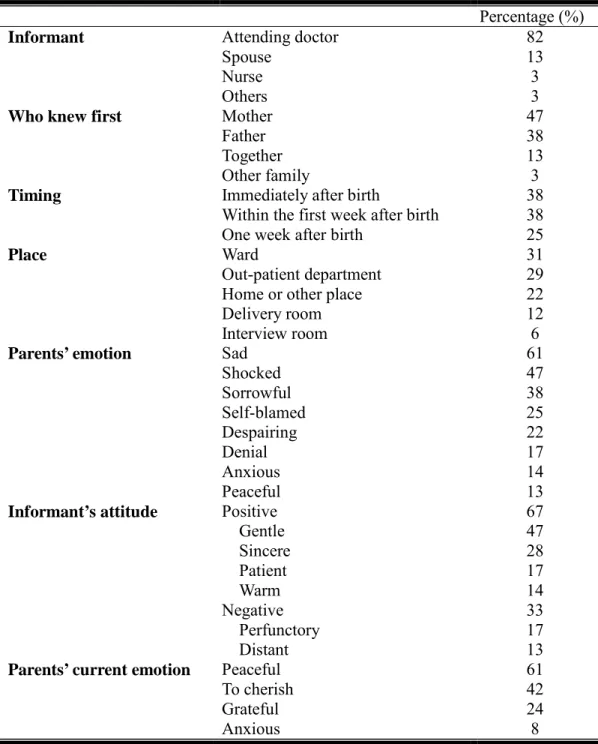
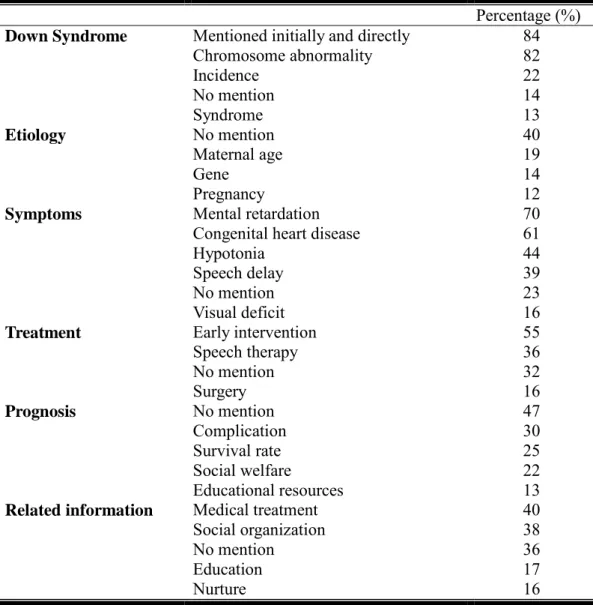
一、社會人口學資料 社會人口學資料請見Table 1。45 位唐氏兒的平均年齡為 7.8 歲(標準差= 3.1), 其中有28 個男生,17 個女生,男女的平均年齡並無差異(F = 0.01, df = 1,43, p = 0.920)。在這 45 個家庭中,只有一個家庭父母親已離婚。接受研究訪談的 34 位父親 之平均年齡為40.3 歲(標準差= 5.7),43 位母親之平均年齡為 37.4 歲(標準差= 5.4)。 42%的父親教育程度為高中(職),19%為國中以下,26%為專科,只有 13%教育程 度在大學以上。60%的母親教育程度為高中(職),國中以下和專科各佔 15%,教育 程度在大學以上的只有10%。74%的父親從事技術性質的工作,16%為無技術性工作 或沒有工作,10%從為專業或半專業人士。60%的母親為全職家庭主婦,其他 40%的 職業婦女之中,最多從事非手操技術性工作,佔23%;其次是無技術性工作,佔 13 %;而手操技術性和專業工作各佔2%。27%的家庭經濟狀況為中下或低收入戶,其 餘皆為小康。 二、遺傳諮詢的內容和形式 關於唐氏兒父母接受遺傳諮詢的情形詳見Table 2。在 77 位父母親之中,有 82% 是由醫生告知唐氏症的診斷。與配偶同時得知的只佔13%,大多是父親或母親其中一 方先知道。得知的時間多是產後馬上得知,或在產後一星期以內得知,各佔38%。告 知的地點最多是在病床上,其次是醫院門診、家裡或另約地點,只有少數在醫院會談 室進行。當父母知道孩子是唐氏症時,第一時間的情緒反應,大多覺得難過、震驚或 是悲傷,部分父母感到絕望、自責以及否認。 遺傳諮詢進行時,除了諮商者(醫生)之外,30%有護士在場,但並沒有任何社 工人員或心理師在場。父母親陳述有關諮商者的態度方面,大多是溫和(47%)、正 面(33%)、誠懇的(28%),有部分父母感覺諮商者只是敷衍了事(17%)、冷淡的 (13%)。整個諮詢的時間短則 2 分鐘長至 2 小時,平均諮詢時間 26 分鐘(標準差= 23.5)。在會談時與諮商者的互動情形方面,65%的父母表示沒有得到情緒上的支持或 安慰,78%沒有被鼓勵發問,高達 91%的父母表示沒有獲得表達或宣洩情緒的機會。 在遺傳諮詢結束後,47%並沒有任何轉介或後續處理,只有 4%的父母有接受後續的 心理輔導或治療。 關於遺傳諮詢的內容請見 Table 3。有 84%的諮商者一開始就提到孩子是唐氏症。 有關唐氏症的內容描述方面,大多數提到染色體異常,少部分會提到發生機率或詳細 介紹唐氏症徵候群。在唐氏症病因方面,40%的諮商者完全沒有說明病因,少部分會 提到母親年齡、遺傳因素、懷孕過程的影響。對可能症狀的描述方面,較多提到的是 智能不足、先天性心臟病、肌肉張力不好以及語言障礙。在治療方式方面,大多會告 知需要早期療育,部分提到需要語言治療,但有33%完全沒有告知可能的治療方式。 有47%的諮商者沒有提到對唐氏症的長期預後,只有 30%會提到可能的併發症。接 近40%會提供醫療方面、社會性團體等相關資料,然而有 36%的醫護人員沒有告訴 父母任何有關教養、醫療及成長等方面的訊息。 唐氏症兒父母理想中的遺傳諮詢形式,57%希望是由醫生告知,也有 51%的人希望由專業的遺傳諮詢人員告知。96%希望是以面對面的告知方式,93%的人希望告知 當時配偶能在身邊,而有14%的人希望社工人員也在場。希望被告知的地點,有 53 %希望在醫院的會談室,24%希望在醫院的門診,不到 10%的父母希望是在產房或病 房裡。父母很期待被告知唐氏症的病因(64%)、症狀(62%)、長期預後(55%)、 治療方式(63%)、復健方式(59%)、教養方式(68%)及相關資源(70%)等內容。 養育一個唐氏症的孩子,55%的父母認為對人生觀是正面的影響,21%認為是負 面影響。對夫妻關係的影響,43%認為是正面的,18%認為是負面的,有 33%的人認 為沒有影響。59%的父母認為對親子關係是正面的影響。在家庭生活方面,40%認為 影響是正面的,21%認為是負面的,33%覺得沒有影響。對於整體生活而言,35%表 示是正面的,25%表示是負面的,31%認為沒有影響。約有 10%的父母表示正、負向 影響同時存在。唐氏兒的父母在此次接受訪談時的情緒,61%的父母情緒是平靜的, 42%表示比以前更珍惜,24%是感恩的,而有 8%的父母仍處於焦慮、自責的情緒。 三、遺傳諮詢的滿意度與影響因素 整體而言,只有將近 20%的父母是感到滿意的。而有超過 40%的父母不滿意諮商 者所提供的相關社會、教育資源,以及有關唐氏症的後續處置建議。也有超過30%的 父母對諮商者提供有關唐氏症的知識感到不滿意、會談時間不夠充足,以及在會談時 沒有得到適當的情緒支持。 以一般線性模式分析父母的個人特質、遺傳諮詢經驗與遺傳諮詢滿意度之間的關 係,結果詳見Table 4。單因子分析的結果顯示:父母的經濟狀況越好,對遺傳諮詢的 滿意度越低。而個性越外向者、諮詢的地點若是在醫院的會談室,而非醫院門診或病 房諮詢、進行時間越久、諮商者的態度或父母當時的情緒是正面的,遺傳諮詢滿意度 也越高。在遺傳諮詢的內容方面,有關唐氏症之病因、可能症狀、治療或復健方式、 長期預後、相關資料等各方面的訊息,諮商者提供越多資訊可以增加父母對遺傳諮詢 的滿意度。而父母的年齡、教育程度、職業、遺傳諮詢的時機與遺傳諮詢滿意度之間 沒有顯著的關係。 將所有與遺傳諮詢滿意度有顯著關係的項目作為預測變項放入統計模式,以反向 選擇決定最後的模式(final model),以找出影響遺傳諮詢滿意度最顯著之因素。最後 有顯著的包括外向性格、諮商者的態度、父母當時的情緒以及經濟狀況。父母個性越 外向,對遺傳諮詢較容易感到滿意。諮商者的態度若是正面、溫暖、誠懇、耐心的, 父母對遺傳諮詢越感到滿意。在接受遺傳諮詢時父母的情緒若是平靜的,較沒有負面 的情緒,父母對遺傳諮詢也較會感到滿意。而父母的經濟狀況若越好,可能他們對遺 傳諮詢的要求會越高,因此越不易感到滿意。 四、唐氏兒與非唐氏兒父母的人格特質與心理狀態 唐氏兒與非唐氏兒父母的人格特質與心理狀態詳見 Table 5。結果顯示,與非唐氏 兒母親相比,唐氏兒母親在各分量表的分數普遍較高,在強迫性症狀、憂鬱、焦慮、 離群、一般症狀指數以及陽性症狀總數的差異達到顯著,而在身體化症狀、人際間敏 感、畏懼、附加症狀等分量表的差異則是臨界地顯著。唐氏兒父親則是在神經質、身 體化症狀上顯著高於非唐氏兒父親,在憂鬱、一般症狀指數的差異達臨界地顯著。
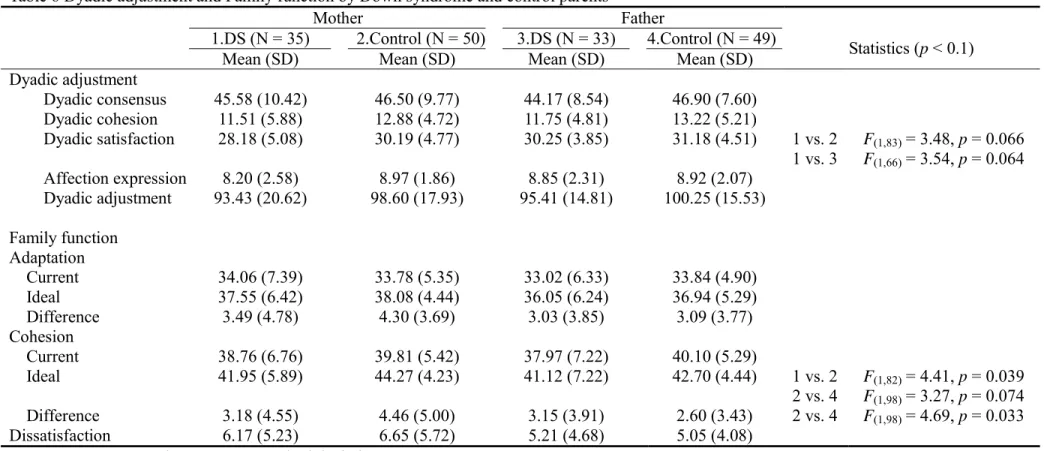
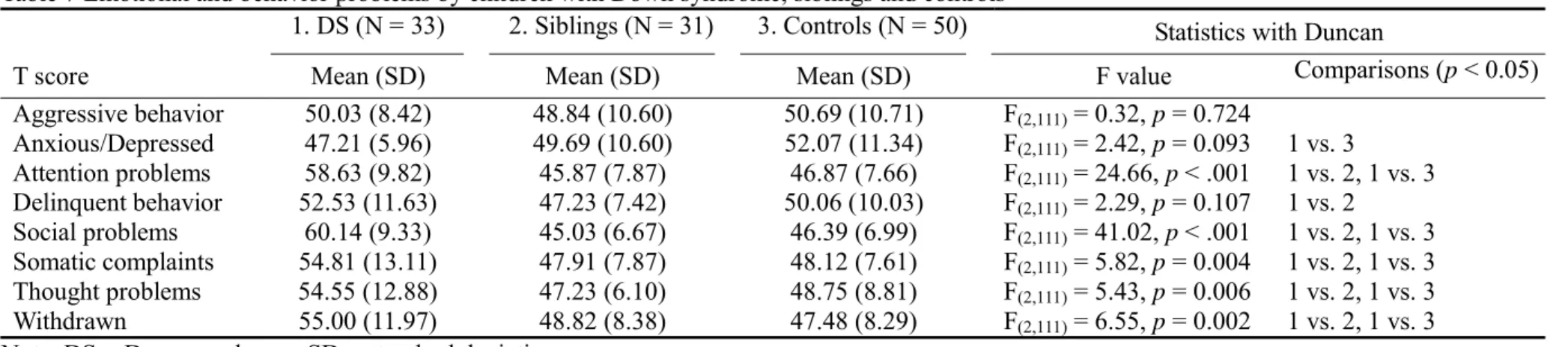
比較父親與母親的差異,唐氏兒的母親顯著比父親焦慮,在人際間敏感性、畏懼 的表現上母親臨界地高於父親。在非唐氏兒的雙親方面,母親在敵意的表現、陽性症 狀嚴重度上顯著高於父親,而在社會期許的人格特質上父親顯著高於母親。 五、唐氏兒與非唐氏兒父母的婚姻與家庭關係 唐氏兒與非唐氏兒父母的婚姻與家庭關係詳見 Table 6。在婚姻兩性關係方面,唐 氏兒與非唐氏兒父母在各項分量表上無顯著的差異。而在對婚姻的滿意度方面,唐氏 兒母親臨界地低於唐氏兒父親和非唐氏兒母親。在家庭關係方面,理想中的家庭凝聚 力分數,非唐氏兒母親顯著高於唐氏兒母親,臨界地高於非唐氏兒父親。非唐氏兒母 親在理想中的家庭凝聚力與現實的差距方面顯著高於父親。 六、唐氏兒、其手足與非唐氏兒三組在行為與情緒問題之差異 唐氏兒、其手足與非唐氏兒的行為與情緒問題比較詳見 Table 7。結果顯示,唐氏 兒在注意力、社交、身體化症狀、想法與退避等問題顯著比其手足、非唐氏兒嚴重, 但比非唐氏兒顯現出較少的焦慮、憂鬱等症狀。對唐氏兒父母而言,唐氏兒表現出比 其手足多不好的、違反規定的行為。唐氏兒之手足與非唐氏症兒在行為和情緒等問題 上並無顯著差異。 七、唐氏兒、其手足與非唐氏兒之父母與其親子關係之差異 唐氏兒、其手足與非唐氏兒之父母與其親子關係之差異詳見 Table 8。在母親方 面,唐氏兒之手足所得到的情感與照顧顯著比非唐氏兒少,母親給予其的保護也比唐 氏兒和非唐氏兒少。另外,唐氏兒之手足的母親對其權威式控制也顯著較非唐氏兒 少。在父親方面,唐氏兒之手足得到父親的保護顯著少於唐氏兒及非唐氏兒,以及較 唐氏兒少的權威式控制。而父親較會對唐氏兒過度保護,顯著高於其手足與非唐氏兒。 八、父母親在親子關係之差異 父母親在親子關係之差異請見 Table 8。在唐氏兒父母方面,對於唐氏兒母親比父 親展現出較多的情感與照顧(p=.026),而父親則展現較多的照顧(p=.027)與過度保 護(p=.025)。而在對待唐氏兒手足方面,父親與母親的表現沒有差異。此外,非唐 氏兒父母對待孩子的態度也無顯著差異(p=.147~.997)。
結 論
在前兩年的研究當中發現,遺傳諮詢的經驗滿意與否對父母的身心狀態、婚姻關 係、親子關係並沒有影響。而在家庭功能和家庭互動上,有負向諮商經驗的父母親會 有較多家庭適應或家庭互動上的困難。遺傳諮詢品質的好壞對於父母的影響不是在當 場的感覺和情緒的反應,而是後續他們對這個疾病的瞭解、對這個疾病他們是否知道 如何協助小孩去獲得足夠的支援,和從知道這個病後他們認知上的接受度、安排自己 的生活、教養小孩及重新定位自己、再次出發。不論由醫師或是專業的遺傳諮詢人員 給予足夠且品質良好的遺傳諮詢應該是非常重要。雖然目前看到其對親子關係並無太 大影響,但是可以想像一個對整個家庭關係滿意度上有問題的父母如何發揮他們的潛 能來照顧唐氏症的兒童,這樣的結果更突顯出遺傳諮詢品質的重要性。 一、遺傳諮詢的現況 本研究以有唐氏兒的家庭為研究對象提供國內遺傳諮詢的現況,以及影響遺傳諮 詢滿意度的因素。從77 位唐氏症兒父母的諮詢經驗中發現,目前台灣的醫療體系對 於唐氏症這類遺傳、染色體疾患並沒有十分完整健全的處理程序。遺傳諮詢是如何進 行的,大多取決於第一次診斷為唐氏症的時間與地點。八成左右的父母是由醫生進行 遺傳諮詢,而諮詢地點只有6%在醫院的會談室。大多數的遺傳諮詢並非坐下來進行 的,平均諮詢的時間只有26 分鐘。遺傳諮詢進行時,大多沒有給父母機會發問或鼓 勵他們表達他們的看法,因此,無法解決他們的疑惑或提供足夠的資訊。對於父母剛 知道這個訊息時的震驚、不安和焦慮,在諮詢時也沒有給他們表達或宣洩情緒的機 會。在遺傳諮詢後,只有4%的父母有接受後續的心理諮詢與輔導,不到四成的諮商 者會提供相關學會或協會的訊息,讓父母可以得到進一步的資訊和協助。從這些結果 來看,可以說不能算是完整的遺傳諮詢,僅僅只是醫生單方面告知父母唐氏症的訊息 而已,缺少雙方的溝通以及提供心理的支持。 二、影響遺傳諮詢滿意度的因素 本研究發現許多與遺傳諮詢滿意度有關的因素,其中部分與國外的研究結果一 致:諮商者的態度冷漠、敷衍,提供的唐氏症相關訊息不夠充足,都是令父母感到不 滿意的原因(Cunningham et al., 1984; Hedov et al., 2002; Quine & Pahl, 1986; Quine & Rutter, 1994)。而在許多研究結果中都有提到的告知時機,在本研究中與遺傳諮詢滿 意度並沒有顯著的關連,或許是因為國外的研究大都以多種遺傳、染色體疾患做為樣 本,與其他遺傳疾病不同的是,患有唐氏症的嬰兒在外表具有典型的特徵,大多在短 時間內就會被發現進而診斷,因此較無諮詢時機的問題。本研究獨特的發現是父母的 經濟地位、外向性格、遺傳諮詢的地點、進行的時間長短以及父母當時的情緒也會影 響遺傳諮詢滿意度。其中影響遺傳諮詢滿意度最重要之因素為:父母之外向性格、諮 商者的態度、父母當時的情緒以及經濟狀況。諮商者的態度是決定遺傳諮詢成功與 否,以及個案日後社會心理是否能適應良好的重要因素(Wertz & Fletcher, 1988)。由此 可知,增進遺傳諮詢品質的方法十分重要的一點是諮商者的態度要正面、溫和、誠懇 而且有耐心,雖然父母的個性和經濟狀況等因素無法改變,至少可以透過諮詢或進一 步的心理輔導、治療,協助父母表達或宣洩內心的不安與焦慮、給予情緒上的支持與安慰,緩和他們第一次得到診斷結果時震驚、無助的情緒,使父母能較容易接受及適 應孩子為唐氏症的事實,及早準備進行孩子的醫療、發展和教育的療育。
三、理想的遺傳諮詢
國內唐氏兒父母理想的遺傳諮詢形式,與國外的研究結果大多一致(Quine & Pahl, 1986; Quine & Rutter, 1994; Spahis & Wilson, 1999),都希望諮商者具備足夠的專業知 識,能夠得到關於唐氏症種種相關的訊息。進行遺傳諮詢的地點,希望能在一個單獨、 不受打擾的空間,例如醫院的會談室,能夠與諮商者面對面坐下來好好的談,而且配 偶也能一同在場。或許是因為國內的醫病關係中,醫生是屬於專業權威的一方,病患 對醫生的診斷多抱持服從、接受態度,而且國內對於遺傳諮詢的概念尚未普及化,因 此多數父母仍希望是由醫生來進行遺傳諮詢,其次才是受過專業訓練的遺傳諮詢人 員。然而不論是醫生或專業的諮詢人員,除了對該疾病具備充分的專業知識以外,諮 詢會談的技巧和態度是需要專業訓練的。除了讓個案或相關家人能夠充分了解此項疾 病之外,還能以具有同理心的態度去了解患者以及他的家人內心的感受,以協助他們 心理、生活、家庭等各方面的適應。 四、唐氏兒父母的心理適應、婚姻關係與家庭關係 由結果可看出唐氏兒的母親卻實有較多的身心症狀,這或許與母親在家庭中必須 扮演的角色有關。由於母親必須花較多的時間去照顧患有唐氏症的孩子,包括其生活 起居、身體問題、或是特殊教育等問題,結果也間接顯示母親相對於父親感受到更多 的壓力(Cheng & Tang, 1995)。而在婚姻關係與家庭關係方面,本研究結果支持部分過 去的研究結果,養育唐氏症的孩子並不會對婚姻或家庭帶來負面的影響(Bennett & DeLuca, 1996; Ferguson, 2002; Fishman & Wolf, 1991),顯示出唐氏兒家庭對於孩子的 身體障礙所造成的問題,能夠順利解決與克服,並維持良好的夫妻互動與家庭凝聚力。 五、唐氏兒的行為問題與親子關係
由於唐氏症造成的智能不足與發展障礙,導致唐氏兒與正常發展的孩子相比有 較多的注意力、社交、思想、退縮等問題,但是較少焦慮和憂鬱的症狀,或許可以唐 氏兒的個性來解釋,相關文獻顯示唐氏兒的個性是比較溫和與友善的(Gibbs & Thorpe, 1983; Gunn & Berry, 1985)。過去的研究較少探討唐氏兒的親子關係,由本研究結果可 知,唐氏兒的母親對待他/她的方式與非唐氏兒母親沒有差別,然而唐氏兒父親傾向 於對他/她過度保護。 六、唐氏兒之手足的行為問題與親子關係 過去有關唐氏兒對其手足影響的研究尚未有一致的結論,而本研究顯示,唐氏兒 之手足並未有較多的情緒和行為問題。在親子關係方面,與唐氏兒相比,其手足從母 親那裡獲得的照顧顯著較少,雙親也傾向給於其較多的行為自由。這些唐氏兒之手足 所受到教養差異在與非唐氏兒相比時也會發現。這些現象或許是因為母親必須負起照 顧唐氏兒生活起居的責任,因此對其發展正常的手足的關注相對減少。父母也可能指 派他/她去照顧患唐氏症的手足,因此給予他/她較多的行為自由以及鼓勵他/她獨立。 對於唐氏兒與其手足在親子關係方面的研究,過去並未受到重視,然而,根據本研究 的結果,家有唐氏兒確實會影響到父母與家中其他孩子的關係,這個議題值得後續進
一步的研究。 七、研究的限制 本研究最困難之處,在於唐氏症的個案少,而且並不在醫療機構長期治療,尤其 鮮少在作者所執業的精神科門診,所以收案不易。加上過去醫療和遺傳諮詢的品質對 這類病人的照護稍嫌不足,導致收案時遇到不少父母抱怨、發洩對醫療的諸多不滿, 最後還是拒絕參加研究。因此研究群經過兩年的努力,只收集77 位父母的資料。由 於母樣本的數目不知,因此,本研究結果應用到其他有唐氏症或染色體異常孩子的家 庭的外推性是存疑的。然而本研究應是少數國際上的研究專門探討針對唐氏症遺傳諮 詢品質的研究,而收集的個案數不亞於國際上相關的研究。其他的優點包括並用半結 構會談和自填問卷收集資料,並採用具有良好信效度的量表。 八、臨床意涵 本研究的結果顯示目前台灣針對先天染色體異常疾病(例如唐氏症)的遺傳諮詢 品質仍有改善的空間,以減少如唐氏症患童本身缺陷對他們自己和家庭的衝擊,以增 加他們的力量和應對能力去適應和解決面臨的困境。除了增進對唐氏兒醫療照顧、特 殊教育之外,唐氏兒父母和手足的心理健康也十分需要重視。希望透過這個研究,能 讓國人對現行的遺傳諮詢情形有初步的了解,提供國內的醫療體系作為改進相關疾病 諮詢的參考,帶給所有為遺傳、染色體疾病所苦的患者及家庭足夠和適切的協助。除 了唐氏症等染色體疾病以外,其他早期發病具有明顯的遺傳傾向的疾病,例如自閉 症,也很值得去探討其遺傳諮詢的現況和滿意度。
參 考 文 獻
Abbeduto, L., Seltzer, M. M., Shattuck, P., Krauss, M. W., Orsmond, G., & Murphy, M. M. (2004). Psychological well-being and coping in mothers of youths with autism, Down syndrome, or fragile X syndrome. American Journal of Mental Retardation,
109, 237-254.
Achenbach, T. M. (1991a). Mannual for the Child Behavior Checklist/4-18 and 1991 Profile. In (Ed.)^(Eds.), (ed., Vol., pp.). Burlington: Department of Psychiatry, University of Vermont.
Achenbach, T. M. (1991b). Manual for the Child Behavior Checklist/4-18 and 1991 Profile. In (Ed.)^(Eds.), (ed., Vol., pp.). Burlington: Department of Psychiatry, University of Vermont.
Beckman, P. J. (1991a). Comparison of mothers' and fathers' perceptions of the effect of young children with and without disabilities. American Journal of Mental
Retardation., 95, 585-595.
Beckman, P. J. (1991b). Comparison of mothers' and fathers' perceptions of the effect of young children with and without disabilities. American Journal of Mental
Retardation, 95, 585-595.
Bennett, T., & DeLuca, D. A. (1996a). Families of children with disabilities: positive adaptation across the life cycle. Social Work in Education, 18, 31-44.
Bennett, T., & DeLuca, D. A. (1996b). Families of children with disabilities: positive adaption across the life cycle. Social Work in Education, 18, 31-44.
Bond, M. H., & Huang, K. K. (1986). The social psychology of Chinese people. (Trans. ed. Vol.). Hong Kong: Oxford University Press.
Bristol, M. M., Gallagher, J. J., & Schopler, E. (1988). Mothers and fathers of young developmentally disabled and nondisabled boys: Adaptation and spousal support.
Developmental Psychology, 24, 441-451.
Cahill, B. M., & Glidden, L. M. (1996). Influence of child diagnosis on family and parental functioning: Down syndrome versus other disabilities. American Journal of Mental
Retardation, 101, 149-160.
Chao, R. K. (1994). Beyond parental control and authoritarian parenting style: understanding Chinese parenting through the cultural notion of training. Child
Development, 65, 1111-1119.
Chen, Y. Y., Lee, M. B., Lee, Y. J., & Tseng, M. C. (1998). Psychiatric morbidity and associated psychosocial characteristics of women with pregnancy loss. Taiwanese
Journal of Psychiatry, 12, 194-206.
Cheng, P., & Tang, C. S. (1995). Coping and psychological distress of Chinese parents of children with Down syndrome. Mental Retardation, 33, 10-20.
Cooley, W. C., & Graham, J. M., Jr. (1991). Down syndrome--an update and review for the primary pediatrician. Clinical Pediatrics, 30, 233-253.
Cox, B. J., Enns, M. W., & Clara, I. P. (2000). The Parental Bonding Instrument:
confirmatory evidence for a three-factor model in a psychiatric clinical sample and in the National Comorbidity Survey. Social Psychiatry & Psychiatric Epidemiology,
35, 353-357.
Cummings, S. T., Bayley, H. C., & Rie, H. E. (1966). Effects of the child's deficiency on the mother: a study of mothers of mentally retarded, chronically ill and neurotic children. American Journal of Orthopsychiatry, 36, 595-608.
Cunningham, C. C., Morgan, P. A., & McGucken, R. B. (1984). Down's syndrome: is dissatisfaction with disclosure of diagnosis inevitable? Developmental Medicine &
Child Neurology, 26, 33-39.
Cuskelly, M., & Dadds, M. (1992). Behavioural problems in children with Down's syndrome and their siblings. Journal of Child Psychology & Psychiatry & Allied
Disciplines, 33, 749-761.
Dalton, A. J., & Crapper-McLachlan, D. R. (1986). Clinical expression of Alzheimer's disease in Down's syndrome. Psychiatric Clinics of North America, 9, 659-670. Damrosch, S. P., & Perry, L. A. (1989). Self-reported adjustment, chronic sorrow, and
coping of parents of children with Down syndrome. Nursing Research, 38, 25-30. Derogatis, L. R., Lipman, R. S., & Covi, L. (1973). The SCL-90: an outpatient psychiatric
rating scale. Psychopharmacology Bulletin, 9, 13-18.
Derogatis, L. R., Rickels, K., & Rock, A. F. (1976). The SCL-90 and the MMPI: a strp in the validation of a new self-report scale. British Journal of Psychiatry, 128, 280-289.
Dyson, L. L. (1989). Adjustment of siblings of handicapped children: a comparison.
Journal of Pediatric Psychology, 14, 215-229.
Dyson, L. L. (1991). Families of young children with handicaps: parental stress and family functioning. American Journal of Mental Retardation, 95, 623-629.
Dyson, L. L. (1997a). Fathers and mothers of school-age children with developmental disabilities: parental stress, family functioning, and social support. American
Journal of Mental Retardation., 102, 267-279.
Dyson, L. L. (1997b). Fathers and mothers of school-age children with developmental disabilities: parental stress, family functioning, and social support. American
Journal of Mental Retardation, 102, 267-279.
Eysenck, H. J. (1962). The Maudsley Personality Inventory Manual (Trans. ed. Vol.). San Diego. CA: Educational and Industrial Testing Service.
Eysenck, S. G. B. (1965). Manual of the Junior Eysenck Personality Inventory. In (Ed.)^(Eds.), (ed., Vol., pp.). London: University of London Press.
Ferguson, P. M. (2002). A Place in the Family: An Historical Interpretation of Research on Parental Reactions To Having a Child with a Disability. Journal of Special
Education, 36, 124-130.
Fidler, D. J., Hodapp, R. M., & Dykens, E. M. (2000). Stress in families of young children with Down syndrome, Williams syndrome, and Smith-Magenis syndrome. Early
Education & Development, 11, 395-406.
Fisman, S., & Wolf, L. (1991). The handicapped child: psychological effects of parental, marital, and sibling relationships. Psychiatric Clinics of North America, 14, 199-217.
Flynt, S. W., & Wood, T. A. (1989). Stress and coping of mothers of children with moderate mental retardation. American Journal of Mental Retardation, 94, 278-283.
Freeman, S. B., Taft, L. F., Dooley, K. J., Allran, K., Sherman, S. L., Hassold, T. J., et al. (1998). Population-based study of congenital heart defects in Down syndrome.
American Journal of Medical Genetics, 80, 213-217.
Garwick, A. W., Patterson, J., Bennett, F. C., & Blum, R. W. (1995). Breaking the news. How families first learn about their child's chronic condition. Archives of Pediatrics
& Adolescent Medicine, 149, 991-997.
of children with a similar degree of mental retardation. British Journal of Psychiatry,
149, 161-171.
Gibbs, M. V., & Thorpe, J. G. (1983). Personality stereotype of noninstitutionalized Down syndrome children. American Journal of Mental Deficiency, 87, 601-605.
Goldberg, S., Morris, P., Simmons, R. J., Fowler, R. S., & Levison, H. (1990a). Chronic illness in infancy and parenting stress: a comparison of three groups of parents.
Journal of Pediatric Psychology., 15, 347-358.
Goldberg, S., Morris, P., Simmons, R. J., Fowler, R. S., & Levison, H. (1990b). Chronic illness in infancy and parenting stress: a comparison of three groups of parents.
Journal of Pediatric Psychology, 15, 347-358.
Green, R. G., Harris, R. N., Jr., Forte, J. A., & Robinson, M. (1991a). Evaluating FACES III and the Circumplex Model: 2,440 families. Family Process., 30, 55-73.
Green, R. G., Harris, R. N., Jr., Forte, J. A., & Robinson, M. (1991b). Evaluating FACES III and the Circumplex Model: 2,440 families. Family Process, 30, 55-73.
Gunn, P., & Berry, P. (1985). The temperament of Down's syndrome toddlers and their siblings. Journal of Child Psychology & Psychiatry & Allied Disciplines, 26, 973-979.
Hauser-Cram, P., Warfield, M. E., Shonkoff, J. P., Krauss, M. W., Sayer, A., & Upshur, C. C. (2001). Children with disabilities: a longitudinal study of child development and parent well-being. Monographs of the Society for Research in Child Development,
66, 1-114.
Hedov, G., Wikblad, K., & Anneren, G. (2002). First information and support provided to parents of children with Down syndrome in Sweden: clinical goals and parental experiences.[see comment]. Acta Paediatrica, 91, 1344-1349.
Kasari, C., & Sigman, M. (1997). Linking parental perceptions to interactions in young children with autism. Journal of Autism & Developmental Disorders, 27, 39-57. Kendler, K. S., Sham, P. C., & MacLean, C. J. (1997). The determinants of parenting: an
epidemiological, multi-informant, retrospective study. Psychological Medicine, 27, 549-563.
Kivivuori, S. M., Rajantie, J., & Siimes, M. A. (1996). Peripheral blood cell counts in infants with Down's syndrome. Clinical Genetics, 49, 15-19.
Krauss, M. W. (1993). Child-related and parenting stress: similarities and differences between mothers and fathers of children with disabilities. American Journal of
Mental Retardation, 97, 393-404.
Lam, L. W., & Mackenzie, A. E. (2002). Coping with a child with Down syndrome: the experiences of mothers in Hong Kong. Qualitative Health Research, 12, 223-237. Lavigne, J. V., & Ryan, M. (1979a). Psychologic adjustment of siblings of children with
chronic illness. Pediatrics., 63, 616-627.
Lavigne, J. V., & Ryan, M. (1979b). Psychologic adjustment of siblings of children with chronic illness. Pediatrics, 63, 616-627.
Lee, M. B., Hsien, R., Lin, H. N., & Lee, Y. J. (1990a). Personality as an effective predictor of outcome for neurotic disorder. Chinese Psychiatry, 4, 111-121.
Lee, M. B., Hsien, R., Lin, H. N., & Lee, Y. J. (1990b). Personality as an effective predictor of outcome of neurotic disorders. Chinese Psychiatry, 4, 111-121.
Lee, M. B., & Lee, Y. J. (1990). A cross-sectional epidemiological study of psychiatric comorbidity in hospitalized medically ill. Chinese Psychiatry, 4, 10-26.
Development and Verification of Validity and Reliability of a Short Screening Instrument to Identify Psychiatric Morbidity. Journal of Formosa Medical
Association, 102, 6871-6894.
Lin, C. C., & Fu, V. R. (1990). A comparison of child-rearing practices among Chinese, immigrant Chinese, and Caucasian-American parents. Child Development, 61, 429-433.
Lobato, D., Barbour, L., Hall, L. J., & Miller, C. T. (1987). Psychosocial characteristics of preschool siblings of handicapped and nonhandicapped children. Journal of
Abnormal Child Psychology, 15, 329-338.
Marino, B., Digilio, M. C., Grazioli, S., Formigari, R., Mingarelli, R., Giannotti, A., et al. (1996). Associated cardiac anomalies in isolated and syndromic patients with tetralogy of Fallot. American Journal of Cardiology, 77, 505-508.
Marty, T. L., Seo, T., Matlak, M. E., Sullivan, J. J., Black, R. E., & Johnson, D. G. (1995). Gastrointestinal function after surgical correction of Hirschsprung's disease: long-term follow-up in 135 patients. Journal of Pediatric Surgery, 30, 655-658. McHale, S. M., Sloan, J., & Simeonsson, R. J. (1986). Sibling relationships of children
with autistic, mentally retarded, and nonhandicapped brothers and sisters. Journal
of Autism & Developmental Disorders, 16, 399-413.
Miller, A. C., Gordon, R. M., Daniele, R. J., & Diller, L. (1992). Stress, appraisal, and coping in mothers of disabled and nondisabled children. Journal of Pediatric
Psychology, 17, 587-605.
Murray, R. F., Jr. (1976). Psychosocial aspects of genetic counseling. Social Work in Health
Care, 2, 13-23.
Olson, D. H. (1991). Three-dimensional (3-D) Circumplex Model and revised scoring of FACES III. Family Process, 30, 74-79.
Parker, G. (1979). Parental Characteristics in Relation to Depressive Disorders. British
Journal of Psychiatry, 134, 138-147.
Pelchat, D., Ricard, N., Bouchard, J. M., Perreault, M., Saucier, J. F., Berthiaume, M., et al. (1999). Adaptation of parents in relation to their 6-month-old infant's type of
disability. Child: Care, Health & Development, 25, 377-397.
Piven, J., & Palmer, P. (1999). Psychiatric disorder and the broad autism phenotype: evidence from a family study of multiple-incidence autism families. American
Journal of Psychiatry, 156, 557-563.
Poznanski, E. (1969a). Psychiatric difficulities in siblings of handicapped children. Clinical
Pediatrics., 8, 232-234.
Poznanski, E. (1969b). Psychiatric difficulties in siblings of handicapped children. Clinical
Pediatrics, 8, 232-234.
Quine, L., & Pahl, J. (1986). First diagnosis of severe mental handicap: characteristics of unsatisfactory encounters between doctors and parents. Social Science & Medicine,
22, 53-62.
Quine, L., & Pahl, J. (1987). First diagnosis of severe handicap: a study of parental reactions. Developmental Medicine & Child Neurology, 29, 232-242.
Quine, L., & Rutter, D. R. (1994). First diagnosis of severe mental and physical disability: a study of doctor-parent communication. Journal of Child Psychology & Psychiatry
& Allied Disciplines, 35, 1273-1287.
Rabkin, J. G., & Struening, E. L. (1976). Live events, stress, and illness. Science, 194, 1013-1020.
Rodrigue, J. R., Morgan, S. B., & Geffken, G. R. (1992). Psychosocial adaptation of fathers of children with autism, Down syndrome, and normal development. Journal of
Autism & Developmental Disorders, 22, 249-263.
Ryde-Brandt, B. (1991). Defence strategies and anxiety in mothers of disabled children.
European Journal of Personality, 5, 367-377.
Shek, D. T., & Cheung, C.-k. (1990). Locus of coping in a sample of Chinese working parents: Reliance on self or seeking help from others. Social Behavior &
Personality, 18, 327-345.
Sloper, P., Knussen, C., Turner, S., & Cunningham, C. (1991). Factors related to stress and satisfaction with life in families of children with Down's syndrome. Journal of
Child Psychology & Psychiatry & Allied Disciplines, 32, 655-676.
Spahis, J. K., & Wilson, G. N. (1999). Down syndrome: perinatal complications and counseling experiences in 216 patients. American Journal of Medical Genetics, 89, 96-99.
Spanier, G. B. (1976). Measuring dyadic adjustment: New scales for assessing the quality of marriage and similar dyads. Journal of Marriage & the Family, 38, 15-28. Springer, A., & Steele, M. W. (1980). Effects of physicians' early parental counseling on
rearing of Down syndrome children. American Journal of Mental Deficiency, 85, 1-5.
Stoll, C., Alembik, Y., Dott, B., & Roth, M. P. (1998). Study of Down syndrome in 238,942 consecutive births. Annales de Genetique, 41, 44-51.
Stores, R., Stores, G., Fellows, B., & Buckley, S. (1998). Daytime behaviour problems and maternal stress in children with Down's syndrome, their siblings, and
non-intellectually disabled and other intellectually disabled peers. Journal of
Intellectual Disability Research, 42, 228-237.
Torfs, C. P., Bateson, T. F., & Curry, C. J. (1992). Anorectal and esophageal anomalies with Down syndrome. American Journal of Medical Genetics, 44, 847; discussion 848-850.
Wertz, D. C., & Fletcher, J. C. (1988). Attitudes of genetic counselors: a multinational survey. American Journal of Human Genetics, 42, 592-600.
Williamson, P., Harris, R., Church, S., Fiddler, M., & Rhind, J. (1996). Prenatal genetic services for Down's syndrome: access and provision in 1990-1991. Steering Committee of the National Confidential Enquiry into Counselling for Genetic Disorders. British Journal of Obstetrics & Gynaecology, 103, 676-683. Yagel, S., & Anteby, E. (1998). A rational approach to prenatal screening and
intervention.[comment]. Human Reproduction, 13, 1126-1128.
Yang, H. J., Chen, W. J., & Soong, W. T. (2001). Rates and patterns of comorbidity of adolescent behavioral syndromes as reported by parents and teachers in a Taiwanese nonreferred sample. Journal of the American Academy of Child & Adolescent
Psychiatry, 40, 1045-1052.
Yarborough, M., Scott, J. A., & Dixon, L. K. (1989). The role of beneficence in clinical genetics: non-directive counseling reconsidered. Theoretical Medicine, 10, 139-149. Zipursky, A., Brown, E., Christensen, H., Sutherland, R., & Doyle, J. (1997). Leukemia
and/or myeloproliferative syndrome in neonates with Down syndrome. Seminars in
Perinatology, 21, 97-101.
蔣欣欣, & 喻永生. (1997). 唐氏症嬰幼兒父母認知真相後之調適過程. 護理研究, 5,
附 表
Table 1 Sample characteristics
DS (N = 45) Control (N = 50)
Variables N (%) or Mean (SD) N (%) or Mean (SD) Chi-square statistics or F statistics Mother
Age 37.33 (5.38) 37.02 (4.41) F(1, 93) = 0.10, p = 0.756
Age of childbirth 30.84 (4.62) 29.26 (4.03) F(1, 93) = 3.19, p = 0.078
Education level
≦Junior high school 6 (14.29) 1 (2.00) χ2 = 14.07, df = 2, p < 0.001 Senior high school 26 (61.90) 19 (38.00)
≧College 10 (23.81) 30 (60.00) Employment status Employed 14 (34.15) 28 (59.57) χ2 = 5.68, df = 1, p = 0.017 Unemployed 27 (65.85) 19 (40.43) Father Age 40.23 (5.81) 40.20 (4.56) F(1, 92) = 0.00, p = 0.980 Education level
≦Junior high school 7 (16.67) 4 (8.00) χ2 = 5.61, df = 2, p = 0.061 Senior high school 20 (47.62) 16 (32.00)
≧College 15 (35.71) 30 (60.00) Employment status Employed 41 (100.00) 46 (97.87) χ2 = 0.88, df = 1, p = 0.348 Unemployed 0 (0.00) 1 (2.13) Child Age 7.82 (3.08) 8.44 (2.80) F(1, 93) = 1.05, p = 0.308 Gender Male 28 (62.22) 27 (54.00) χ2 = 0.81, df = 1, p = 0.369 Female 17 (37.78) 23 (46.00) Number of children in family 2.27 (0.81) 2.00 (0.67) F(1, 93) = 3.08, p = 0.082
Table 2 Circumstances at the first contact for genetic counseling
Percentage (%)
Informant Attending doctor 82
Spouse 13 Nurse 3
Others 3
Who knew first Mother 47
Father 38
Together 13 Other family 3
Timing Immediately after birth 38
Within the first week after birth 38 One week after birth 25
Place Ward 31
Out-patient department 29 Home or other place 22 Delivery room 12 Interview room 6
Parents’ emotion Sad 61
Shocked 47 Sorrowful 38 Self-blamed 25 Despairing 22 Denial 17 Anxious 14 Peaceful 13
Informant’s attitude Positive 67
Gentle 47 Sincere 28 Patient 17 Warm 14 Negative 33 Perfunctory 17 Distant 13
Parents’ current emotion Peaceful 61
Cherished 42 Grateful 24 Anxious 8
Table 3 Content of genetic counseling about Down syndrome
Percentage (%)
Down Syndrome Mentioned initially and directly 84
Chromosome abnormality 82 Incidence 22 No mention 14 Syndrome 13 Etiology No mention 40 Maternal age 19 Gene 14 Pregnancy 12
Symptoms Mental retardation 70
Congenital heart disease 61
Hypotonia 44 Speech delay 39
No mention 23 Visual deficit 16
Treatment Early intervention 55
Speech therapy 36 No mention 32 Surgery 16 Prognosis No mention 47 Complication 30 Survival rate 25 Social welfare 22 Educational resources 13
Related information Medical treatment 40
Social organization 38 No mention 36 Education 17 Nurture 16
Table 4 Association between parents’ characteristics and their satisfaction with genetic counseling
Variables Estimate SE F statistics Bivariate Analysis Age -0.06 0.20 F(1,75) = 0.10, p = .753 Education level -2.13 1.29 F(1,75) = 2.72, p = .103 Employment status -1.00 0.63 F(1,75) = 2.54, p = .115 Economic status -4.74 1.75 F(1,75) = 7.37, p = .008 Personality characteristics Neuroticism -0.05 0.16 F(1,65) = 0.08, p = .772 Extroversion 0.55 0.22 F(1,65) = 6.00, p = .017 Social desirability 0.02 0.56 F(1,65) = 0.00, p = .970 Genetic counseling Timing 1.64 1.27 F(1,75) = 1.68, p = .200 Place--Interview room 10.49 4.30 F(1,75) = 5.94, p = .017 Duration 0.20 0.04 F(1,75) = 23.21, p < .001 Counselor’s attitude 10.43 1.95 F(1,75) = 28.69, p < .001
Parents’ immediate emotion 5.79 3.36 F(1,75) = 2.97, p = .089
Down syndrome Content 4.47 3.24 F(1,75)= 1.91, p = .171 Etiology 5.41 2.15 F(1,75) = 6.35, p = .014 Symptoms 8.44 2.41 F(1,75) = 12.24, p < .001 Treatment 8.61 2.04 F(1,75) = 17.71, p < .001 Prognosis 8.17 1.99 F(1,75) = 16.85, p < .001 Related information 7.78 2.09 F(1,75) = 13.86, p < .001
Final selected model
Intercept 14.42 5.31
Extroversion 0.54 0.19 F(1, 62) = 7.92, p = .007
Counselor’s attitude 10.18 2.14 F(1, 62)= 22.71, p < .001
Parents’ immediate emotion 10.00 2.94 F(1, 62) = 11.58, p = .001
Table 5 Psychopathology and personality by Down syndrome and control parents
Mother Father
1.DS (N = 34) 2.Control (N = 50) 3.DS (N = 33) 4.Control (N = 49)
Variables Mean (SD) Mean (SD) Mean (SD) Mean (SD) Statistics (p < 0.10)
Personality characteristics Neuroticism 8.93 (7.65) 6.72 (6.24) 9.63 (7.77) 6.04 (5.82) 3 vs. 4 F(1,81) = 5.76, p = 0.019 Extroversion 16.31 (4.99) 17.48 (4.82) 15.03 (5.53) 15.80 (5.00) 2 vs. 4 F(1,98) = 2.94, p = 0.090 Social desirability 4.55 (1.90) 3.99 (2.20) 4.79 (2.50) 4.92 (2.11) 2 vs. 4 F(1,98) = 4.69, p = 0.033 Psychopathology Somatization 0.97 (0.79) 0.66 (0.66) 0.73 (0.68) 0.47 (0.42) 1 vs. 2 3 vs. 4 F(1,82) = 3.94, p = 0.051 F(1,80) = 4.57, p = 0.036 Obsession 1.05 (0.89) 0.71 (0.58) 0.76 (0.57) 0.63 (0.48) 1 vs. 2 F(1,82) = 4.68, p = 0.033 Interpersonal sensitivity 0.82 (0.79) 0.55 (0.54) 0.55 (0.46) 0.41 (0.41) 1 vs. 2 1 vs. 3 F(1,82) = 3.68, p = 0.059 F(1,65) = 3.06, p = 0.085 Depression 0.72 (0.77) 0.43 (0.42) 0.54 (0.45) 0.35 (0.40) 1 vs. 2 3 vs. 4 F(1,82) = 4.99, p = 0.028 F(1,80) = 3.93, p = 0.051 Anxiety 0.65 (0.71) 0.29 (0.37) 0.35 (0.40) 0.31 (0.44) 1 vs. 2 1 vs. 3 F(1,82) = 9.21, p = 0.003 F(1,65) = 4.62, p = 0.035 Hostility 0.88 (0.77) 0.77 (0.71) 0.70 (0.48) 0.48 (0.39) 3 vs. 4 2 vs. 4 F(1,80) = 5.26, p = 0.025 F(1,97) = 6.31, p = 0.014 Phobia 0.51 (0.58) 0.28 (0.49) 0.26 (0.43) 0.21 (0.29) 1 vs. 2 1 vs. 3 F(1,82) = 3.84, p = 0.053 F(1,65) = 3.85, p = 0.054 Paranoid 0.57 (0.64) 0.39 (0.42) 0.48 (0.58) 0.35 (0.37) Psychoticism 0.49 (0.54) 0.27 (0.42) 0.43 (0.56) 0.29 (0.37) 1 vs. 2 F(1,82) = 4.33, p = 0.041 Addition symptoms 0.58 (0.57) 0.35 (0.51) 0.50 (0.67) 0.39 (0.41) 1 vs. 2 F(1,82) = 3.78, p = 0.055 General symptom severity index (GSI)
0.73 (0.65) 0.46 (0.41) 0.53 (0.42) 0.39 (0.32) 1 vs. 2
3 vs. 4
F(1,82) = 5.52, p = 0.021
F(1,80) = 2.78, p < 0.10
Positive symptom total number (PST)
23.29 (15.61) 16.48 (11.37) 19.67 (13.78) 16.20 (12.04) 1 vs. 2 F(1,82) = 5.36, p = 0.023
Positive symptom
distress index (PSDI) 1.41 (0.43) 1.29 (0.35) 1.23 (0.56) 1.07 (0.40) 2 vs. 4
F(1,80) = 8.55, p = 0.004
Table 6 Dyadic adjustment and Family function by Down syndrome and control parents
Mother Father
1.DS (N = 35) 2.Control (N = 50) 3.DS (N = 33) 4.Control (N = 49)
Mean (SD) Mean (SD) Mean (SD) Mean (SD) Statistics (p < 0.1)
Dyadic adjustment Dyadic consensus 45.58 (10.42) 46.50 (9.77) 44.17 (8.54) 46.90 (7.60) Dyadic cohesion 11.51 (5.88) 12.88 (4.72) 11.75 (4.81) 13.22 (5.21) Dyadic satisfaction 28.18 (5.08) 30.19 (4.77) 30.25 (3.85) 31.18 (4.51) 1 vs. 2 1 vs. 3 F(1,83) = 3.48, p = 0.066 F(1,66) = 3.54, p = 0.064 Affection expression 8.20 (2.58) 8.97 (1.86) 8.85 (2.31) 8.92 (2.07) Dyadic adjustment 93.43 (20.62) 98.60 (17.93) 95.41 (14.81) 100.25 (15.53) Family function Adaptation Current 34.06 (7.39) 33.78 (5.35) 33.02 (6.33) 33.84 (4.90) Ideal 37.55 (6.42) 38.08 (4.44) 36.05 (6.24) 36.94 (5.29) Difference 3.49 (4.78) 4.30 (3.69) 3.03 (3.85) 3.09 (3.77) Cohesion Current 38.76 (6.76) 39.81 (5.42) 37.97 (7.22) 40.10 (5.29) Ideal 41.95 (5.89) 44.27 (4.23) 41.12 (7.22) 42.70 (4.44) 1 vs. 2 2 vs. 4 F(1,82) = 4.41, p = 0.039 F(1,98) = 3.27, p = 0.074 Difference 3.18 (4.55) 4.46 (5.00) 3.15 (3.91) 2.60 (3.43) 2 vs. 4 F(1,98) = 4.69, p = 0.033 Dissatisfaction 6.17 (5.23) 6.65 (5.72) 5.21 (4.68) 5.05 (4.08)
Table 7 Emotional and behavior problems by children with Down syndrome, siblings and controls
1. DS (N = 33) 2. Siblings (N = 31) 3. Controls (N = 50) Statistics with Duncan
T score Mean (SD) Mean (SD) Mean (SD) F value Comparisons (p < 0.05)
Aggressive behavior 50.03 (8.42) 48.84 (10.60) 50.69 (10.71) F(2,111) = 0.32, p = 0.724 Anxious/Depressed 47.21 (5.96) 49.69 (10.60) 52.07 (11.34) F(2,111) = 2.42, p = 0.093 1 vs. 3 Attention problems 58.63 (9.82) 45.87 (7.87) 46.87 (7.66) F(2,111) = 24.66, p < .001 1 vs. 2, 1 vs. 3 Delinquent behavior 52.53 (11.63) 47.23 (7.42) 50.06 (10.03) F(2,111) = 2.29, p = 0.107 1 vs. 2 Social problems 60.14 (9.33) 45.03 (6.67) 46.39 (6.99) F(2,111) = 41.02, p < .001 1 vs. 2, 1 vs. 3 Somatic complaints 54.81 (13.11) 47.91 (7.87) 48.12 (7.61) F(2,111) = 5.82, p = 0.004 1 vs. 2, 1 vs. 3 Thought problems 54.55 (12.88) 47.23 (6.10) 48.75 (8.81) F(2,111) = 5.43, p = 0.006 1 vs. 2, 1 vs. 3 Withdrawn 55.00 (11.97) 48.82 (8.38) 47.48 (8.29) F(2,111) = 6.55, p = 0.002 1 vs. 2, 1 vs. 3
Note. DS = Down syndrome; SD = standard deviation.
Table 8 Parental attitude toward children with Down syndrome, siblings and controls
1.DS 2.Siblings 3.Controls Statistics with Duncan
Mean (SD) Mean (SD) Mean (SD) F value Comparisons (p < 0.05)
Mother (N = 40) (N = 32) (N = 50) Affection 27.53 (4.31) 26.85 (4.78) 29.10 (4.27) F(2,119) = 2.85, p = 0.062 2 vs. 3 Protection 14.74 (5.16) 12.26 (4.97) 14.94 (4.64) F(2,119) = 3.32, p = 0.040 1 vs. 2, 2 vs. 3 Overprotection 8.03 (3.33) 6.50 (4.13) 7.84 (3.25) F(2,119) = 1.95, p = 0.147 Authoritative controlling 6.71 (2.98) 5.76 (2.80) 7.10 (2.27) F(2,119) = 2.50, p = 0.086 2 vs. 3 Father (N = 37) (N = 25) (N = 50) Affection 25.27 (4.40) 25.07 (4.26) 26.01 (5.19) F(2,106) = 0.42, p = 0.661 Protection 17.08 (3.79) 12.56 (4.97) 14.48 (4.44) F(2,106) =8.42, p < .001 1 vs. 2, 1 vs. 3 Overprotection 9.65 (2.83) 6.80 (3.19) 7.89 (3.20) F(2,106) =6.90, p = 0.002 1 vs. 2, 1 vs. 3 Authoritative controlling 7.43 (2.81) 5.76 (2.68) 6.58 (2.71) F(2,106) = 2.84, p = 0.063 1 vs. 2
附錄一
遺傳諮詢的內容及影響諮詢滿意度的相關因子—以唐氏症為例
摘 要
目的:為了瞭解唐氏兒父母接受遺傳諮詢的現況,父母對遺傳諮詢經驗的滿意程度, 以及影響遺傳諮詢滿意度之相關因素。
方法:本研究訪談了77 位唐氏兒的父母有關遺傳諮詢的內容及滿意度評估,父母並 完成簡式性格量表(Maudsley Personality Inventory, MPI)等自填式問卷。
結果:研究結果顯示唐氏兒父母的遺傳諮詢82%由醫生進行,平均諮詢時間為 26 分 鐘(標準差= 23.5),只有20%的父母對遺傳諮詢的經驗感到滿意。諮商者的態度冷漠、 敷衍,提供的資訊不夠充足,進行諮詢的地點不適當,進行時間太短等都讓父母感到 不滿意。而父母當時的情緒、經濟狀況、外向性格也會影響遺傳諮詢的滿意度。 結論:目前國內對唐氏兒父母的遺傳諮詢,大多是由醫生單方面告知父母有關唐氏症 的相關訊息,缺乏雙方的溝通,以及提供心理支持、後續心理輔導、治療的工作。增 進遺傳諮詢品質最重要的是改進諮商者的態度,給予父母宣洩情緒的機會和提供足夠 的資訊,以協助唐氏兒家庭心理、生活、親子關係等各方面的適應。 關鍵詞:唐氏症,遺傳諮詢,遺傳諮詢滿意度