國科會工程處
九十一年度計畫
NSC90-2213-E-002-102
“暫時性缺血腦中風病患大腦血容之定量:
使用磁化率對比微灌流磁振造影”
成果報告
計畫主持人:鍾孝文副教授 台大電機系
九十一年十月二十一日
行政院國家科學委員會專題研究計畫成果報告
暫時性缺血腦中風病患大腦血容之定量:
使用磁化率對比微灌流磁振造影
Quantification of cerebral blood capacity on patients with
transient ischemic attack (TIA) using
susceptibility-contrast perfusion-weighted MR imaging
計畫編號:NSC90-2213-E-002-102
執行期限:90 年 8 月 1 日至 91 年 7 月 31 日
主持人:鍾孝文副教授 台大電機系
chung@cc.ee.ntu.edu.tw
一、中文摘要 本計畫之目的在於發展一系列的影像 分析技術,用於動態臨床微灌流磁振造 影,並將給予血管擴張劑 acetazolamide 前 後之大腦血流 (cerebral blood flow) 差異 予以絕對定量,以利計算暫時缺血性中風 (transient ischemic attack) 病患之腦血容積 (cerebrovascular reserve capacity)。暫時缺血 性中風定義為中風症狀於發生後二十四小 時內消除之病患。在計畫一年期之內,我 們以奇異值分解法完成大腦血流的定量 化,並且發現如今國際間廣泛使用的演算 方式具有明顯的誤差,而此誤差與組織平 均穿流時間 (mean transit time) 相關。由於 平均穿流時間在暫時缺血性中風病患大腦 中與正常組織明顯不同,因而計算誤差將 導致無法忽略的錯誤。我們在計畫中進一 步提出改善方案,將誤差由 +/-25% 減低 至約 5%。 關鍵詞:微灌流、磁振、暫時性腦缺血、 絕對定量腦血流、奇異值分解、腦血容。 AbstractThe purpose of this one-year project is to develop a series of image analysis methods
on clinical dynamic susceptibility-contrast perfusion-weighted magnetic resonance (MR) imaging to quantify the cerebrovascular reserve capacity (CRC) during vasodilating challenge task with acetazolamide (diamox). The specific clinical target of the project is transient ischemic attack (TIA), that is, patients with symptoms of ischemic stroke but recovered within 24 hours. Within one fiscal year we have implemented the deconvolution method based on the singular value decomposition to derive cerebral blood flow (CBF), from which the cerebrovascular reserve capacity can be directly computed. The CBF analysis algorithm widely used in most international medical center has been shown to exhibit significant prediction errors dependent on tissue mean-transit-time (MTT), which can vary substantially in pathological conditions encountered in TIA patients. We further proposed a method to remedy this algorithm drawback to reduce the CBF estimation error from the original +/-25% to 5%.
Keywords: perfusion, magnetic resonance, transient ischemic attack, absolute quantification of cerebral blood flow, singular value decomposition, cerebral blood reserve capacity.
二、計畫緣由與目的
Absolute quantification of cerebral blood flow (CBF) has been shown to be feasible with dynamic susceptibility-contrast magnetic resonance imaging, using singular value decomposition (SVD) to deconvolve arterial input function (AIF) from the tissue signal-time response curve (1). Despite its wide acceptance in the international scientific society, SVD exhibits inherent pitfalls leading to estimation errors in the presence of contrast arrival delay or bolus dispersion (2). In this study, we show that the CBF estimation error is dependent on tissue mean transit time (MTT) in the original SVD approach. Since in patients with transient ischemic attack (TIA), the cerebral perfusion could consist of a significant portion of collateral circulation exhibiting lengthened MTT, the inherent non-negligible inaccuracy of the SVD approach may present severe limitations in clinical applications. We estimate the range of this error and further propose an alternative SVD-based method with substantial accuracy improvement in the estimation of CBF.
Computer simulations were performed using single-compartment tissue residue function (R(t)) with MTT varied from 2 to 8 sec to cover the widest range possibly seen in clinical practice. In addition to the original method which determines CBF as the maximum height of R(t), we also investigated an alternative approach for estimating CBF from the width of the impulse response h(t), i.e., the negative derivative of R(t). The method is expressed specifically as the equation:
h(t) F of moment first normalized 0 ) ( t dt t R F CBF [1]
Note that the denominator is directly related to the width of h(t). The estimation errors in CBF of the two methods were compared.
Eleven patients with history of TIA were recruited in this study. Two series of multi-slice dynamic susceptibility-contrast echo-planar perfusion weighted MR imaging (6 slices, TE=44ms, 128x128 in matrix, 23cm FOV, 5mm slice thickness, 75 frames per slice at one-sec time interval) were performed after intravenous bolus injection of 0.2mmol/Kg Gd-DTPA (Magnevist, Schering, Germany). One series of images were acquired before the administration of acetazolamide (Diamox, 15 mg/Kg, Lidar, Germany), whereas the other series was obtained twenty minutes after intravenous diamox injection. Images were obtained on a 1.5T system (Siemens Vision+, Erlangen, Germany). Absolute CBF maps were derived by deconvolving the AIF (assessed from an upstream middle cerebral artery) from tissue concentration-time curves on a pixel-by-pixel basis.
三、結果與討論
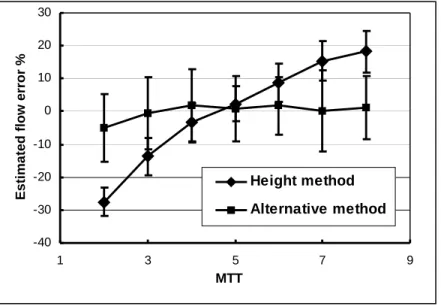
Figure 1 shows the SVD-deconvolved R(t) at two MTT values (2 and 4 sec, respectively) together with their original simulated single exponential decaying functions. Note that the maximum heights were significantly altered, while the widths were largely invariant, implying that CBF estimation from height of R(t) would exhibit significantly larger errors than from width of R(t). Figure 2 shows CBF estimation errors as a function of MTT. It is seen that the original height method shows the
MTT-dependent errors from 25%
under-estimation (at short MTT) to 20% over-estimation (long MTT). In contrast, the alternative approach based on width estimation shows MTT-insensitive errors less than 5%. Patient images showed the expected inconsistencies of cerebrovascular reserve capacity derived using the two approaches. Note that since there lacks a gold standard in patient cerebral perfusion, only the simulation results can demonstrate the efficacy of our proposed method.
We attribute the estimation errors of the original SVD method to the truncation of singular values when the inter-frame interval in dynamic susceptibility MR imaging is relatively long compared with MTT. Note that truncation of singular values was required to reduce influences from inter-frame noise. However, since the decaying R(t) at short MTT itself exhibits high-frequency signal changes similar to inter-frame fluctuations, singular value truncation results in partial elimination of the peak information, leading to corresponding reduction in R(t) height. Under-estimation in CBF hence results, particularly with short MTT. An optimization of singular value truncation with respect to the desired MTT value (1, 3) results in over-compensation of CBF when MTT is abnormally prolonged. Note that the MTT-dependent estimation errors in CBF, with actual MTT values unknown beforehand, are not easily correctable. On the other hand, the alternative approach proposed in this study based on width of R(t) was shown less prone to singular value truncation effects. We therefore conclude that SVD deconvolution using our proposed method is a better and robust approach toward the absolute quantification of CBF.
四、 計畫成果自評
Our efforts spent in this project have created results substantially greater than that mentioned in this brief report. Overall, the project has generated five conference papers, including three presented in the Annual Meeting of the International Society of Magnetic Resonance in Medicine. In addition, two journal articles reporting the findings of perfusion abnormality in ischemic patients have recently been accepted (4, 5), including one to appear in the prestigious
Radiology (5). Achievements from this
project have raised the attention of other domestic medical centers, including Taipei and Kaohsiung Veteran General Hospitals, as well as National Taiwan University Hospital
who have approached us for mutual cooperation. In short, we have confidence that a successful execution of this project will benefit both the medical centers as well as the patients with cerebral ischemia.
五、參考文獻
1. Ostergaard L, Weisskoff RM, Chesler DA, Gyldensted C, Rosen BR. High resolution measurement of cerebral blood flow using intravascular tracer bolus passages. Part II: experimental comparison and preliminary results.
Magnetic Resonance in Medicine.
1996;36:726-736.
2. Calamante F, Gadian DG, Connelly A. Delay and dispersion effects in dynamic susceptibility contrast MRI: Simulations using singular value decomposition.
Magnetic Resonance in Medicine.
2000;44:466-473,.
3. Liu HL, Pu Y, Liu Y, Kickerson L, Andrews T, Fox PT, Gao JH. Cerebral blood flow measurement by dynamic contrast MRI using singular value decomposition with an adaptive threshold.
Magnetic Resonance in Medicine
1999;42:167-172.
4. Liu YJ, Chung HW, Huang IJ, Wang FN, Chin SC, Lee CS, Chen CY. A re-investigation of maximal signal drop in dynamic susceptibility-contrast MR imaging. Journal of Neuroimaging 2002, accepted.
5. Liu YJ, Chen CY, Chung HW, Huang IJ, Lee CS, Chin SC, Liou M. Temporal evolution of neuronal necrosis following ischemic injury in the middle cerebral artery territory: deep watershed versus territorial infarct subtypes on MR perfusion and spectroscopic imaging.
六、圖表
Figure 1. The original simulated single-exponential residue functions and corresponding deconvolved curves at mean transit times of 2.0 and 4.0 seconds. Note the large alterations in maximum heights, while the widths are largely invariant. Thus the newly proposed method based on curve width yields more accurate results than the height method.
-40 -30 -20 -10 0 10 20 30 1 3 5 7 9 MTT Esti ma ted flo w error % Height method Alternative method
Figure 2. CBF estimation errors of two methods as a function of tissue mean transit time. There are MTT-dependent estimation errors ranging from –25% to +20% if using the original method measuring the height of R(t). In contrast, errors are within 5% with the alternative method measuring the width of R(t), showing substantial improvements.