預測第二型糖尿病患者之胰島素注射意圖:應用計畫行為理論並探討情緒之影響 - 政大學術集成
80
0
0
全文
(2) APPROVALS. 立. 政 治 大. ‧. ‧ 國. 學. n. er. io. sit. y. Nat. al. Ch. engchi. 1. i n U. v.
(3) ACKNOWLEDGEMENTS 致謝詞 在政大校園度過的四年光陰,感覺漫長,又似短暫。四年前與四年後的我 有什麼改變?每ㄧ天我是否更認識自己,更發揮潛能,更無所畏懼? 感謝指導教授許文耀老師,應允我進入心理學殿堂,有機會一探這個豐富 而迷人的學科。 感謝四年來啟發我的老師們:李怡青老師,蔣治邦老師,楊建銘老師,錢 玉芬老師,林邦傑老師,林耀盛老師。. 治 政 感謝畢業論文指導,台大呂碧鴻醫師。 大 立. 感謝學長姊、各位同學、學弟妹。因為有每一個人,我的碩士班生涯無比. ‧ 國. 學. 生動精彩,收穫滿滿。. ‧. Where to go from here?. n. al. er. io. sit. y. Nat. It doesn’t matter. Where there’s a will, there’s a way.. Ch. engchi. i n U. v 張榮哲. 2013 年 7 月. (承蒙新竹馬偕紀念醫院醫學研究經費贊助,計畫編號 MMH-HB-101-08,使 本研究得以順利完成,在此致上最大謝意). 2.
(4) CONTENTS APPROVALS ........................................................................................................... 1 ACKNOWLEDGEMENTS ....................................................................................... 2 CONTENTS.............................................................................................................. 3 LIST OF TABLES .................................................................................................... 4 LIST OF FIGURES ................................................................................................... 5 ABSTRACT .............................................................................................................. 6 THE PREDICTION OF INSULIN INJECTION INTENTION AMONG PATIENTS WITH TYPE 2 DIABETES: AN APPLICATION OF TPB AND EXPLORING THE IMPACT OF EMOTIONS ........................................................................................ 8. 政 治 大. Introduction ................................................................................................... 8. 立. Method ........................................................................................................ 29. ‧ 國. 學. Results ......................................................................................................... 36 Discussion ................................................................................................... 47. ‧. CONCLUSION ....................................................................................................... 61. sit. y. Nat. REFERENCES........................................................................................................ 62. io. n. al. er. APPENDIX ............................................................................................................. 69. Ch. engchi. 3. i n U. v.
(5) LIST OF TABLES Table 1. The BIT Questionnaire items and scales……………………………………13 Table 2. Insulin Treatment Appraisal Scale………………………………………….15 Table 3. Means, standard deviations of research variables and the correlation matrix………………………………………………..……….………...........37 Table 4. The simple regression of how each independent variable predicts intention…………………….……………………………….………………38 Table 5. The hierarchical regression of control variables, TPB variables and emotion. 治 政 大 Table 6. Group characteristics and independent t-test comparisons and Chi-square 立. variables in predicting intention of insulin therapy…………………..……..40. values divided based on HbA1C level……………………………..………..43. ‧ 國. 學. Table 7. Comparison of stepwise regressions divided into groups based on HbA1C. ‧. level to predict intention………………………………………..…………...45. sit. y. Nat. Table 8. The comparison of correlation matrixes between better and worse glycemic-. io. n. al. er. control groups……………………………………..………………………...59. Ch. engchi. 4. i n U. v.
(6) LIST OF FIGURES Figure 1. The Theory of Planned Behavior model…………………………………...19 Figure 2. The hypothesized research model……………………………………….…27 Figure 3. The distribution of participants’ intention to use insulin………………..…36 Figure 4. The examination of attitude’s mediating effect between emotion variables and intention……………………………………………………………….42. 立. 政 治 大. ‧. ‧ 國. 學. n. er. io. sit. y. Nat. al. Ch. engchi. 5. i n U. v.
(7) ABSTRACT Insulin injection is an important treatment in the care of type 2 diabetes mellitus. However, psychological insulin resistance (PIR) has long been an obstacle for many patients to achieve optimal glycemic control. The purpose of this research is to identify the influencing factors in decision-making process of type 2 diabetic patients whether or not to undergo insulin therapy. We adopted the theory of planned behavior (TPB) as our theoretical basis, which argues attitude, subjective norm and perceived behavior control (PBC) are determinants of behavioral intention, and intention is the. 治 政 大 and physical responses which were anticipatory emotions (immediate psychological 立 precursor of behavior. Besides, we integrated extra emotion variables into TPB,. toward the behavior itself) and anticipated emotions (affective responses expected to. ‧ 國. 學. be experienced in the future when behavioral outcomes occur), to expanded the. ‧. predictive power of research model. A cross-sectional questionnaire study design was. sit. y. Nat. employed, and a total of 457 currently not using insulin type 2 diabetic patients. io. er. participated in this research. The hierarchical regression analysis revealed that all. al. three TPB variables (attitude, subjective norm, PBC) significantly predict intention to. n. v i n C39.1% use insulin, which account for of intention. After the addition of h e nvariance gchi U. emotional variables, the research model explains intention variance up to 43.2%, with negative anticipatory emotion and negative anticipated emotion being significant determinants. In the comparison of better glycemic-control (HbA1C < 9%) and worse glycemic-control (HbA1C ≧ 9%) participants, negative anticipatory emotion is the only variable in our research model significantly differs between both groups. The results of this research indicate not only TPB is a useful framework in realizing PIR, but also the impact of anticipatory and anticipated emotions cannot be overlooked.. 6.
(8) 摘要 胰島素自我注射是第二型糖尿病的重要治療方法。然而,許多病患的心 因性胰島素抗拒(PIR)使他們拒絕胰島素治療,因而導致血糖控制不良。本研 究目的即嘗試找出影響第二型糖尿病患者接受胰島素治療與否之可能因素。我 們採用計畫行為理論(TPB)為基本架構,此理論主張「態度」、「主觀規 範」、「覺知行為控制」三個變項可決定對某行為之意圖,而意圖可預測此行 為之發生。此外,我們將情緒變項整合進 TPB 架構中以提昇預測力,包括「同 時情緒」(對行為本身當下之心理或生理反應)與「預期情緒」(預期未來行. 政 治 大 為之後果成真時的情緒反應)。我們採自陳式問卷,橫斷研究設計,總計 457 立. ‧ 國. 學. 位目前未使用胰島素之第二型糖尿病患者參與研究。階層迴歸分析結果,三個 TPB 變項(態度、主觀規範、覺知行為控制)均顯著預測胰島素治療之意圖,. ‧. 可解釋 39.1%變異量;加入情緒變項後,整體模式解釋力提昇,可解釋 43.2%意. y. Nat. io. sit. 圖之變異量,「負向同時情緒」及「負向預期情緒」均為顯著預測因子。比較. er. 血糖控制較佳(HbA1C < 9%)與血糖控制較差(HbA1C ≧ 9%)兩組受試者,. al. n. v i n 「負向同時情緒」是研究模型中唯一有顯著差異之變項。本研究結果顯示 TPB Ch engchi U 可成功應用於解釋 PIR,而情緒變項之影響亦不容小覷。. 7.
(9) THE PREDICTION OF INSULIN INJECTION INTENTION AMONG PATIENTS WITH TYPE 2 DIABETES: AN APPLICATION OF TPB AND EXPLORING THE IMPACT OF EMOTIONS Introduction Diabetes mellitus (DM) has become one of the most important health issues in nowadays. The estimated worldwide prevalence of diabetes is 2.8% in year 2000 and 4.4% in year 2030. Namely, there are 171 million people with diabetes in 2000, and the. 政 治 大 2004). In Taiwan, diabetes 立has been one of the top five leading causes of death for. number will be increased to 366 million in 2030 (Wild, Roglic, Green, Sicree, & King,. ‧ 國. 學. decades, and the estimated prevalence has reached 9.2% (Department of Health, 2011). Diabetes mellitus is a metabolic disorder of multiple etiology characterized by. ‧. chronic hyperglycemia with disturbances of carbohydrate, fat, and protein metabolism. sit. y. Nat. resulting from defects of insulin secretion, insulin action, or a combination of both. io. er. (National Diabetes Data Group, 1979). It can be classified into type 1 and type 2 DM.. al. iv n C production. In type 2 diabetes, the blood glucose hrising eng c h i U results from a combination of n. Type 1 diabetes is due to a virtually complete lack of endogenous pancreatic insulin. decreased insulin secretion and decreased insulin sensitivity. The macrovascular disease, including cardiovascular, cerebrovascular and peripheral artery disease, is the most important complication of diabetes. Cardiovascular disease accounts for the majority of mortality and morbidity. Diabetic patients have a risk that is two to three times higher than non-diabetic individuals to develop cardiovascular disease (Ryden et al., 2007). Besides, patients with diabetes are at increased risk for nephropathy, retinopathy and neuropathy, which are called the microvascular disease, can. 8.
(10) result in end-stage renal disease, uremia, blindness, foot ulcers and amputation (American Diabetes Association, 2011). To avoid development of complications, achieving ideal blood sugar control is crucial in the management of diabetes. According to a 10-year follow-up study, the risk of microvascular disease was 25% lower in intensive blood-sugar control group (average HbA1C = 7.0%) compared to conventional treatment group (UKPDS, 1998). The same prospective observational study also concluded that each 1% reduction in updated mean. 政 治 大 for myocardial infarction, 立and 37% for microvascular complications (Stratton et al.,. HbA1C was associated with reductions in risk of 21% for deaths related to diabetes, 14%. ‧ 國. 學. 2000). Clinical trials also support an intensive, multifactorial treatment was associated with a significant lower risk of all-cause death and lower risk of death from. ‧. cardiovascular diseases (Dailey, 2011).. sit. y. Nat. However, the achievement of ideal glycemic targets in diabetes mellitus can be. io. er. very challenging for both patients and physicians. In the US, an analysis using data from. al. iv n C of adults with type 2 diabetes meththe glycemic control en g c h i U goal (HbA1C < 7.0%) (Dodd et n. the National Health and Nutrition Examination Survey (NHANES) revealed only 52.2%. al., 2009). Another study conducted in Hong Kong showed even fewer patients (39.7%) attaining the same glycemic target among Chinese type 2 diabetes patients. The longer disease duration and the more complex treatment regimens, the less optimal glycemic control (Tong et al., 2008). The predicament also exists in Taiwan, revealed in a nationwide survey conducted in 2006 that the percentage of individuals whose HbA1C level met the same goal were merely 22.3% and 32.5% in type 1 and type 2 diabetes, respectively (Yu et al., 2009).. 9.
(11) The majority of DM patients are diagnosed as type 2 diabetes. Unlike type 1 DM, which is onset in the early age of patients and insulin injection is the only way for glycemic control, patients of type 2 DM are usually adults and the comprehensive glycemic treatment includes diet control, physical activities, body weight reduction, oral anti-diabetic drugs (OAD) and insulin injection (Care, 2008). The most common initial medical treatment for type 2 diabetes is OAD. However, OAD failure is inevitable in most type 2 DM patients (Mudaliar & Edelman, 2001). The OAD failure is defined as. 政 治 大 in type 2 diabetes patients. 立In the UK Prospective Diabetes Study (UKPDS), more than. can’t achieve glycemic goal with OAD alone and the use of insulin injection is required. ‧ 國. 學. half (53%) of newly diagnosed type 2 diabetic patients experienced OAD failure and required additional insulin therapy within 6 years (Wright, Burden, Paisey, Cull, &. ‧. Holman, 2002).. sit. y. Nat. When OAD failure occurs, the addition or total shift of insulin therapy is. io. er. necessary for optimal glycemic control in type 2 DM. However, resistance or refusal to. al. iv n C U in the US. The most commonly 33% of patients with type 2 DM h unwilling e n gtoctake h i insulin n. insulin is a common problem in clinical practice. A prospective study showed there was. expressed negative attitudes toward insulin were concern regarding hypoglycemia, permanent need for insulin therapy, less flexibility, and feelings of failure (Larkin et al., 2008). A similar refusal rate was noted among the patients in UK (UKPDS, 1995). In East Asia, insulin resistance is even more profound. A study conducted in Singapore revealed seven of every ten patients (70.6%) with type 2 DM expressed unwillingness to use insulin. Fear of not being able to inject insulin correctly, fear of pain, belief that insulin therapy wound make it difficult to maintain social roles, and belief of insulin. 10.
(12) therapy efficacy are the greatest differences among perceptions between patients willing and unwilling to take insulin (Wong et al., 2011). The refusal of insulin in OAD failure patients with type 2 DM can lead to longterm poor glycemic control and consequent multiple complications. Resistance to insulin therapy is a complex psychological phenomenon, and patients usually have various barriers regarding insulin use. Though there were studies try to identify the possible reasons contributing to insulin resistance in other countries, this issue is seldom explored. 政 治 大 predict acceptance of insulin 立 therapy among patients with type 2 DM, and provide. in Taiwan by now. The object of this study is to investigate the possible factors which. ‧ 國. 學. innovative perspectives for development of intervention programs to promote insulin acceptance in Taiwan.. ‧. n. er. io. sit. y. Nat. al. Ch. engchi. 11. i n U. v.
(13) Psychological Insulin Resistance Psychological insulin resistance (PIR) has long been a major concern in the management of type 2 diabetes. PIR can be defined as psychological opposition towards insulin use in people with DM. PIR impacts both the initiation to and compliance with insulin treatment, and leads to sub-optimal glycemic control. There were considerable studies focusing on this issue. In a systemic review conducted in 2008, a total of 109 articles were reviewed and the synthesis of literature. 政 治 大. revealed that PIR may be impacted by the following: (1) patients’ beliefs and knowledge. 立. about diabetes and insulin (e.g., lack of knowledge about diabetes and insulin therapy;. ‧ 國. 學. erroneous beliefs and misconceptions about the disease and treatment); (2) negative self-. ‧. perceptions and attitudinal barriers (e.g., sense of personal failure or self-blame for the necessity of insulin use; fear of injection); (3) the fear of side effects and complications. y. Nat. io. sit. from insulin use (e.g., the misconception which attributing complications of diabetes to. n. al. er. insulin use; the worry about potential side effects of insulin, like hypoglycemia or body. Ch. i n U. v. weight gain); (4) life style adaptations, restrictions required by insulin use (e.g., fears that. engchi. insulin therapy will be inconvenient and cause a loss of personal freedom, resulting in a sense of powerlessness and adversely affecting independence); (5) social stigma (e.g., the negative connotation carried by vials and syringes; the social embarrassment and social rejection caused by the necessity of using syringes in public). The author concluded “assisting health care professionals to better understand the complex and multifaceted aspects of PIR from the patients’ perspective should result in improved insulin treatment outcomes”. (Brod, Kongso, Lessard, & Christensen, 2009).. 12.
(14) In an effort to develop a psychometric questionnaire to measure psychological barriers to insulin treatment in type 2 diabetic patients, principal component analysis was used in two cross-sectional studies of insulin-naïve patients. A pool of 35 items regarding different attitudes toward insulin treatment was created by an expert panel of experienced diabetes care professionals. Analysis in the first sample (N = 448) yielded five components that accounted for 74.5% of the variance based on 14 items, and the following subscales were identified: fear of injection and self-testing, expectations. 治 政 Scale 1: “Fear of injections and self-testing” 大 1. I am afraid of立 the pain when injecting insulin. ‧ 國. 學. 2. Besides the pain, I am just afraid of injections.. 3. I am afraid of the pain during regular blood-sugar checks.. Nat. 5. People who get insulin feel better.. sit. 4. Insulin works better than pills.. y. ‧. Scale 2: “Expectations regarding positive insulin-related outcomes”. io. Scale 3: “Expected hardship from insulin therapy”. al. er. 6. Insulin can reliably prevent long-term complications due to diabetes.. n. iv n C h e ntogmy 8. I can’t pay as close attention c hdieti asUinsulin treatment requires. 7. I just don’t have enough time for regular doses of insulin.. 9. I can’t organize my day as carefully as insulin treatment requires. Scale 4: “Stigmatization by insulin injections”. 10. Injections in public are embarrassing to me. Pills are more discret. 11. Regular insulin treatment causes feelings of dependence. 12. When people inject insulin, it makes them feel like drug addicts. Scale 5: “Fear of hypoglycemia” 13. An insulin overdose can lead to extremely low blood glucose levels (hypoglycemia). I am afraid of the unpleasant accompanying symptoms. 14. An insulin overdose can lead to extremely low blood glucose levels (hypoglycemia). I have concerns about possible permanent damage to my health. 13. Table 1. The BIT Questionnaire items and scales (Petrak et al., 2007)..
(15) regarding positive insulin-related outcomes, expected hardship from insulin treatment, stigmatization by insulin injections, and fear of hypoglycemia (Table 1). The questionnaire was cross-validated in the second sample (N = 449), with almost identical component loadings and an explained variance of 69.4%. This newly developed scale, The Barriers to Insulin (BIT) Questionnaire, appears to be a reliable and valid measure of PIR and easy to administer clinically (Petrak, et al., 2007). Another appraisal instrument, the Insulin Treatment Appraisal Scale (ITAS; Table. 政 治 大 in type 2 diabetic patients 立(Snoek, Skovlund, & Pouwer, 2007). In a three-month follow-. 2), was developed to assess positive and negative perceptions regarding insulin treatment. ‧ 國. 學. up longitudinal study, a total of 130 type 2 diabetic patients were divided into three subgroups. The first group (N = 57) was on insulin therapy at baseline and remained on. ‧. insulin at follow-up. The second group (N = 44) was initially insulin-naïve and switched. sit. y. Nat. to insulin therapy at follow-up. Patients in the third group (N = 29) remained on an OAD. io. er. regimen throughout. Barriers toward insulin therapy were measured using ITAS. At the. al. iv n C U remained on OAD, whereas it decreased in patients to insulin therapy or heng c h i switched n. three-month follow-up, compared with baseline, the ITAS score increased in patients. remained on insulin treatment (p = .003). This study suggests that negative appraisals of insulin treatment are modifiable by the initiation of insulin therapy, and PIR may be a rather temporary than an unchangeable phenomenon (Hermanns, Mahr, Kulzer, Skovlund, & Haak, 2010). Barriers of type 2 diabetic patients to insulin initiation were explored in another study. The reasons of those non-adherent patients (N = 69) failing to initiate insulin therapy following a new prescription of insulin were investigated by interviews and self-. 14.
(16) strongly disagree. disagree. agree nor disagree. agree. strongly agree. ☐. ☐. ☐. ☐. ☐. ☐. ☐. ☐. ☐. ☐. ☐. ☐. ☐. ☐. ☐. ☐. ☐. ☐. ☐. ☐. ☐. ☐. ☐. ☐. ☐. ☐. ☐. ☐. ☐. ☐. ☐. ☐. ☐. ☐. ☐. ☐. ☐. ☐. ☐. ☐. ☐. ☐. 學. ☐. ☐. ☐. ☐. ☐. ☐. ☐. ☐. ☐. ☐. ‧. ☐. ☐. ☐. ☐. ☐. y. ☐. ☐. ☐. ☐. ☐. sit. ☐. ☐. ☐. ☐. ☐ v i n. ☐. ☐. ☐. ☐. ☐. ☐. ☐. ☐. ☐. ☐. ☐. ☐. ☐. ☐. ☐. ☐. ☐. ☐. ☐. ☐. ☐. 1. Taking insulin means I have failed to manage my diabetes with diet and tablets. 2. Taking insulin means my diabetes has become much worse. 3. Taking insulin helps to prevent complications of diabetes. 4. Taking insulin means other people see me as a sicker person. 5. Taking insulin makes life less flexible. 6. I am afraid of injecting myself with a needle. 7. Taking insulin increases the risk of low blood glucose levels (hypoglycaemia). 8. Taking insulin helps to improve my health. 9. Insulin causes weight gain.. ‧ 國. 立. Nat. 10. Managing insulin injections takes a lot of time and energy. 11. Taking insulin means I have to give up activities I enjoy. 12. Taking insulin means my health will deteriorate. 13. Injecting insulin is embarrassing.. io. 14. Injecting insulin is painful.. n. al. Ch. er. 政 治 大. 15. It is difficult to inject the right amount of insulin correctly at the right time ☐ ☐ every day. 16. Taking insulin makes it more difficult to fulfill my responsibilities (at work, ☐ ☐ at home). 17. Taking insulin helps to maintain good ☐ ☐ control of blood glucose. 18. Being on insulin causes family and friends to be more concerned about ☐ ☐ me. 19. Taking insulin helps to improve my ☐ ☐ energy level. 20. Taking insulin makes me more ☐ ☐ dependent on my doctor. Table 2. Insulin Treatment Appraisal Scale (Snoek, et al., 2007).. engchi U. 15.
(17) administered surveys. Misconceptions regarding insulin risk (35% believed that insulin causes blindness, renal failure, amputations, heart attacks, strokes, or early death), plans to instead work harder on behavioral goals, sense of personal failure, low self-efficacy, injection phobia, hypoglycemia concerns, negative impact on social life and job, inadequate health literacy, health care provider inadequately explaining risks/benefits, and limited insulin self-management training were the most commonly reported reasons for refusal of insulin. (Karter et al., 2010). 政 治 大 which may inhibit or facilitate 立 the initiation of insulin therapy in type 2 diabetic patients. In Taiwan, a retrospective qualitative study was conducted to explore the factors. ‧ 國. 學. Data were collected from interviews with 23 patients using insulin therapy and analyzed by content analysis. The inhibiting factors include cognitive barriers (worry about side. ‧. effects of insulin; worry about complications; the idea that insulin therapy represents a. sit. y. Nat. worsened diabetes), attitudinal barriers (fear of needle; fear of self-injections),. io. er. operational barriers (not capable of doing injections correctly), and psychosocial barriers. al. (restraints of daily life; the perception that can’t inject correctly). The facilitating factors. n. iv n C U (perceived benefits of insulin include the awareness of necessity h toward e n ginsulin c h itherapy therapy), abilities to inject insulin without difficulty, and a trustful doctor-patient relationship. Among all of the inhibiting factors, “restraints of daily life” is the most commonly reported inhibiting factor (79%). On the other hand, “perceived benefits of. insulin therapy” is the most frequently reported facilitating factor (75%). The result also showed the inhibiting factors varied from pre-insulin initiation to post-insulin initiation. For instance, the number of patients reporting “fear of needle” significantly decreased after the initiation of insulin therapy (吳淑華, 陳清惠, & 顏妙芬, 2006).. 16.
(18) To sum up, PIR in type 2 diabetic patients is a complex phenomenon influenced by multiple cognitive, emotional and social factors. Assisting health care professionals in better understanding PIR from the patient’s perspective should result in improved treatment outcomes. Though there had been some empirical researches exploring this issue, the present studies focused mostly on cognitive reasons to refuse insulin therapy (e.g., the misconception which attributing complications of diabetes to insulin; the concern about side effects of insulin). The impact of emotional factors was less discussed. 政 治 大 correlation as statistical analysis. 立 Well-established decision-making theories are seldom and possibly overlooked. Furthermore, the present studies mostly employed simple. ‧ 國. 學. applied as a research structure. It may be helpful to adopt psychological viewpoints for a better understanding of PIR.. ‧. n. er. io. sit. y. Nat. al. Ch. engchi. 17. i n U. v.
(19) The Theory of Planned Behavior The Theory of Planned Behavior (TPB; Ajzen, 1991, 2002) is one of the leading theories in behavioral science. It proposes a model about how human action is guided and how human decision is made. For decades, researchers have conducted hundreds of studies applying and testing the TPB with regard to an array of social and health behaviors (Noar & Zimmerman, 2005). Although there have been many theories regarding changing health-risk behaviors. 政 治 大 1974), Protection Motivation 立 Theory (Rogers, 1975), Theory of Reasoned Action (Ajzen developed in health psychology, for example, the Health Belief Model (Rosenstock,. ‧ 國. 學. & Fishbein, 1980), Social Cognitive Theory (Bandura, 1986), the concept of implementation intentions (Gollwitzer, 1999), the Transtheoretical Model (Prochaska &. ‧. DiClemente, 1983), Precaution Adoption Process Model (Weinstein, Rothman, & Sutton,. sit. y. Nat. 1998) and the Health Action Process Approach model (Schwarzer, 1992). Each of them. io. er. has been empirically supported in various degrees to explain health-related behaviors and. al. iv n C U a clear theoretical account of the because of the following reasons.hFirstly, e n gthecTPB h i offers n. design effective interventions. We chose TPB as our underpin research framework. links between attitudes, intentions and behaviors. Secondly, it states how theses constructs should be operationalized, which makes the design of behavior change interventions easier. Thirdly, TPB has been proved to be one of the most useful models if interventions to change intentions and behaviors are based on it (Armitage & Conner, 2000; Baban & Craciun, 2007). The TPB model (Figure 1) suggests that intentions are the precursors of behavior, and there are three variables which will predict the intention to perform a behavior. It. 18.
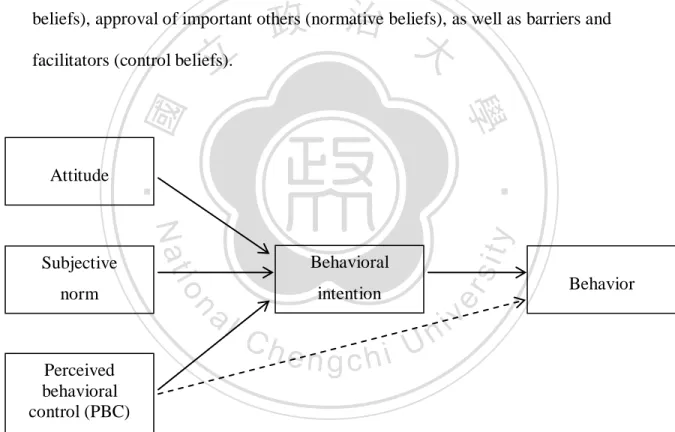
(20) proposes that behavior is a linear function of behavioral intentions and perceived behavioral control (PBC), the perception of individual control over performing the behavior. Intentions, in turn, are assumed to be a linear function of three types of cognitions: attitude (positive or negative evaluation of the behavior), subjective norm (perceived approval of performing the behavior), and PBC. Attitude, subjective norm, and PBC are based on a set of more specific salient behavioral, normative, and control beliefs that reflect perceived outcomes associated with the target behavior (behavioral. 政 治 大. beliefs), approval of important others (normative beliefs), as well as barriers and. 立. facilitators (control beliefs).. y. al. intention. n Perceived behavioral control (PBC). sit. Behavioral. Ch. engchi. er. io. norm. Nat. Subjective. ‧. ‧ 國. 學. Attitude. i n U. Behavior. v. Figure 1. The Theory of Planned Behavior model. The TPB is considered to be a social cognition model. It assumes the human intention toward a specific behavior is determined by the three cognitive beliefs. Other. 19.
(21) often-mentioned factors, like dispositions (e.g., personality traits; self-esteem; emotions; intelligence), demographics (e.g., age; gender; ethnicity; education; income), information (e.g., past experience; knowledge; media exposure), are all considered as “background variables”, which only influence behavior indirectly by affecting behavioral, normative, and control beliefs. If a particular background factor does indeed have an impact on behavior, it influences through one of the three beliefs. The TPB had been used to predict a range of health behaviors, such as physical. 政 治 大 2002), and other health behaviors 立 such as condom use (Kiene, Tennen, & Armeli, 2008) activity (Armitage, 2005; Johnston et al., 2007), eating (M. Conner, Norman, & Bell,. ‧ 國. 學. and prenatal screening in pregnant women (van den Berg et al., 2008). In Taiwan, the TPB also had been applied in various health behavior researches, such as the intention to. ‧. see a psychologist (涂珮瓊, 許文耀, 張正雄, & 陳盈如, 2011), the exercise beliefs of. Nat. sit. y. pregnant women (李靜芳, 姜逸群, 林顯明, & 徐菊容, 2011), and the intention of self-. n. al. er. io. monitoring blood sugar in type 2 diabetic patients(何敏淑, 2008). A meta-analysis. i n U. v. showed that the TPB accounted for 27% variance in behavior, as well as 39% variance in. Ch. engchi. intention. When behavior measures were self-reports, the TPB accounted for 11% more of the variance in behavior than when behavior measures were objective or observed, R2 = .31 and .21 respectively (Armitage & Conner, 2001). However, insufficiencies of the TPB were proposed by succeeding researchers. For example, the change of intentions is not necessarily resulting in the change of real behavior. A meta-analysis which obtained 47 experimental studies of intentionbehavioral relation showed that a medium-to-large change in intention (d = .66) only leaded to a small-to-medium change in behavior (d = .36) (Webb & Sheeran, 2006). In. 20.
(22) another experiment, different interventions focused on behavior beliefs, normative beliefs and control beliefs were delivered to promote participants’ observed exercise behavior. Also change of intentions was noted with behavior-belief and normative-belief interventions, the control-belief intervention was the only one to change real behavior not mediated by cognitions (Sniehotta, 2009). The possible influences of “background factors” were also proposed. A study explored the role of self-schemas found that the more participants perceived themselves. 政 治 大 behavior (Sheeran & Orbell, 立 2000). The mood state of individuals seems to be influential as fit and healthy, the more likely they will translate the exercise intentions to real. ‧ 國. 學. of decision-making process. When participants experienced negative mood state, attitude was more likely to be related to intention than social norm. When participants had a. ‧. positive mood, then social norm, not attitude, was more likely to be related to intention. sit. y. Nat. (Armitage, Conner, & Norman, 1999). Demographic factors may also have impacts on. io. er. decision-making. For example, normative pressure was showed to be a stronger predictor. al. iv n C were more likely to affect the intentions exceed the speed limit (Mark Conner, h e n ofg males c h ito U n. of intentions to speed for men compared to women when driving alone. Social norms. Smith, & McMillan, 2003). Although the TPB has been proved successful and popular, it is possible to further modify or extend the construct of this theory for better prediction of human behaviors. With a better understanding the occurrence of a particular behavior, the more effective intervention programs can be conceived to promote the desired behaviors or decline the undesirable ones.. 21.
(23) Emotions: an Extended Variable for TPB? The incongruence between cognition and affect Most theories used in studying health behaviors are based on cognitive perspectives. For example, the health belief model assumes that the response to the threat of an illness is a function of perceived vulnerability and severity as well as the costs and benefits of the response (Janz & Becker, 1984). The TPB, as previously mentioned, proposes that attitude, subjective norm and PBC are predictors of behavioral intention. 政 治 大 (instrumental) attitude and 立affective (emotional) attitude. The former implies rational. and behavior. The attitude construct can be conceptualized into two parts: the cognitive. ‧ 國. 學. evaluations toward a given behavior, such as good/bad, healthy/unhealthy, safe/danger. The latter is sentimental reactions of individuals toward the same behavior, such as. ‧. enjoyable, liking, worrying, and fearful. For example, a smoker may hold two different. sit. y. Nat. attitudes toward his or her smoking behavior. One of them is cognitive-derived (smoking. io. al. iv n C Some authors had argued hthat e nthese h i Udo not adequately account for the g cmodels n. relaxed).. er. is harmful to my health), the other is affective-derived (smoking makes me happy and. importance of affect in decision–making. For example, Trafimow et al. (2004) found that for many behaviors affect made a larger contribution than cognition to the prediction of behavioral intentions. Affective attitudes but not instrumental attitudes were substantial predictors of behavioral intentions (Kraft, Rise, Sutton, & Roysamb, 2005). In another study, it was concluded that although both cognitive and affective evaluations significantly predicted intentions to perform health behaviors, the influence of affective evaluation was largely direct and that of cognitive evaluation was only partially direct for. 22.
(24) each behavior (Keer, van den Putte, & Neijens, 2010).. Is affect a direct predictor of behavior unmediated by intention? When incongruence exists between cognitive and affective attitudes toward a behavior, the affect has been identified as a stronger predictor of intentions than cognition. Furthermore, some authors even proposed that for some behaviors, there may be a direct effect of affective attitudes on behavior without mediation of intention. Lawton and her. 政 治 大 and health-risk behaviors立 (e.g. smoking, binge-drinking), affective attitude were. colleagues found that for many health-promoting behaviors (e.g. exercise, low-fat diet). ‧ 國. 學. significantly more powerful predictors of behavior than cognitive attitude. The effects of affective attitude were not fully mediated by behavioral intention and had direct influence. ‧. on behavior. Besides, the more the divergence between affective and cognitive attitudes. sit. y. Nat. (e.g. “rationally I know that smoking is bad for my body, but emotionally I really can’t. io. al. er. resist the pleasure of smoking”), the more intensive the relationship between affective. v. n. attitude and behavior (Lawton, Conner, & McEachan, 2009; Lawton, Conner, & Parker, 2007).. Ch. engchi. i n U. How does affect operate in influencing our intentions and behaviors? It is assumed that affect act as a heuristic or mental shortcut in the process of decision-making. It saves an individual strength or cognitive resource to evaluate the pros and cons of a behavior and leads to an efficient decision-making (Finucane, Alhakami, Slovic, & Johnson, 2000). However, the affective influences are not always leading to good decisions or adaptive behaviors. For example, a smoker may dwell in the enjoyment of smoking and overlook the scientific evidences that cigarette has been proved to be one of. 23.
(25) the most important causes of death. In the case of diabetic patients, the fear toward insulin injection may stop them from taking insulin therapy and result in poor glycemic control.. Anticipatory emotions vs. anticipated emotions According to the “risk-as-feelings hypothesis” (Loewenstein, Weber, Hsee, & Welch, 2001), emotional reactions to risky situations often diverge from cognitive. 政 治 大 emotions” and “anticipated 立emotions”. The anticipatory emotions are supposed to be. assessments of risk. The authors also discriminated the difference between “anticipatory. ‧ 國. 學. immediate visceral reactions (e.g., fear, anxiety, dread) to risks and uncertainties. The anticipated emotions are the emotions expected to be experienced in the future when. ‧. outcomes already occur. In other words, the anticipatory emotions are immediate. sit. y. Nat. psychological and physical responses toward the risky situations themselves. The. io. er. anticipated emotions are emotional consequences of the risky situations and more in line. al. iv n C To the extent that decision-making h e n g cresearches h i U have addressed emotions, most of n. with cognitive appraisals.. them take anticipated emotions into account. For example, anticipated regret (Charles Abraham & Sheeran, 2003; M. Conner, Sandberg, McMillan, & Higgins, 2006; Sandberg & Conner, 2008), negative anticipated emotions including regret, worried, sad, sorry, ashamed, anxious, tense, and guilty (Nelissen, de Vet, & Zeelenberg, 2011; Wang, 2011). Positive and negative anticipated emotions had been suggested to play important roles in TPB model (Bagozzi, Dholakia, & Basuroy, 2003; Perugini & Bagozzi, 2001). However, Loewenstein et al. (2001) argued that anticipated emotions are a component of the. 24.
(26) expected consequences of the decision rather than emotions that are experienced at the time of decision. In risky situations, responsive anticipatory emotions often diverge from cognitive evaluations of those risks. When such diverge occurs, anticipatory emotions (neither anticipated emotions nor cognitive assessments) will dominate the behavioral decisions and frequently produce behaviors that don’t appear to be adaptive. It’s possible that in the very moment of making decisions, our behaviors may be governed by more basic drives, like arousals, physical sensations (e.g., pain, hunger) and. 政 治 大 strong impact on sexual-related 立 judgment and decision-making, which included finding anticipatory emotions. Ariely and Loewenstein (2006) found that sexual arousal had a. ‧ 國. 學. sexual stimuli, engaging in morally questionable sexual behavior, and willingness to engage in unsafe sex. Ditto and colleagues (2006) also demonstrated that people can be. ‧. disproportionately influenced by the expected rewards of immediate gratification rather. sit. y. Nat. than the outcomes of performing risky behaviors. When the participants’ emotions were. io. er. aroused by temptation being more immediate, they were less responsive to risk. al. n. iv n C In the case of diabetic patients, h e ntwo h i U emotional responses may be g cparadoxical. information.. experienced concurrently when considering whether or not to take insulin injection. One is the anticipated emotion, which is expected to have in the future when the desired outcome has realized (“I will feel secure and delight when I achieve a good glycemic control using insulin injection”) or the unwanted outcome has occurred (“I will be sad and regretful if I got diabetic complications later due to my refusal of insulin”). Another one is the anticipatory emotion, which is the immediate emotional reaction when thinking about the behavior itself (“I am so scared just thinking about the image that the injection. 25.
(27) needle penetrates my skin and the consequently painful sensation”). The concept of anticipatory and anticipated emotions (also named “futureoriented emotions” in literatures) and their impact on behaviors is a newly emerging research area. The empirical studies had revealed that positively and negatively valenced anticipatory and anticipated emotions can be measured reliably, are empirically distinct, and relate to other constructs in the hypothesized way (Baumgartner, Pieters, & Bagozzi, 2008; Carrera, Caballero, & Munoz, 2012). Authors also tried to integrate these. 政 治 大 al., 2012). Although not 立 enough empirical data to draw a solid conclusion yet, the. emotional variables into traditional TPB model to improve predictive power (Carrera, et. ‧ 國. 學. preliminary analysis indicates the independent influence of anticipatory and anticipated emotions on goal-directed behavior.. ‧. In sum, because of the stressful and unpleasant natures of insulin therapy (Fu,. sit. y. Nat. Qiu, & Radican, 2009; Martinez et al., 2007; Mollema, Snoek, Ader, Heine, & van der. io. er. Ploeg, 2001), it is quite possible that the cognitive and affective attitudes toward insulin. al. iv n C anticipatory emotions is necessary h because i U may exist. e n g the c hincongruence n. will diverge in many diabetic patients. Besides, the distinction between anticipated and. 26.
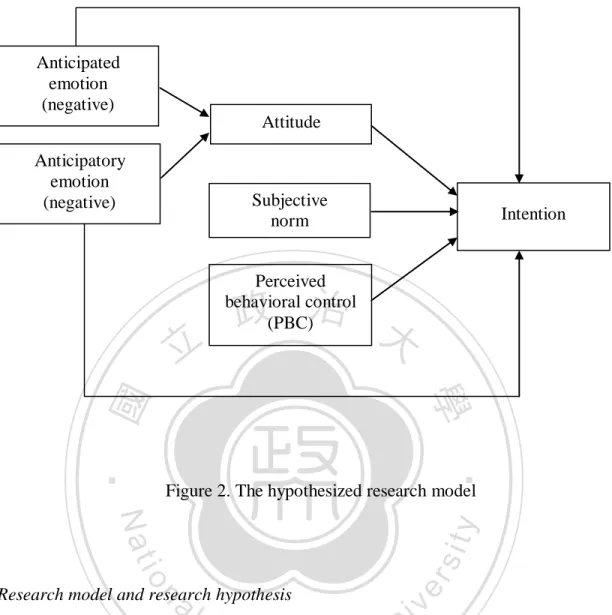
(28) Anticipated emotion (negative) Attitude Anticipatory emotion (negative). Subjective norm. 立. Intention. Perceived behavioral control (PBC). 政 治 大. ‧. ‧ 國. 學 Figure 2. The hypothesized research model. er. io. sit. y. Nat. al. iv n C The aim of this study is h to explore the influencing e n g c h i U factors on the decisionn. Research model and research hypothesis. making process of taking insulin therapy among type 2 diabetic patients. To obtain a better understanding of judgment process, the affective variables (i.e., anticipated emotions and anticipatory emotions) are added to provide extra predictive power in addition to TPB variables. There are two research problems we try to answer in the current study. The first one, is the TPB model suitable for explaining how type 2 diabetic patients make the decision about insulin therapy? The second one, emotions are no more. 27.
(29) than background variables and influencing intention through the mediations of cognitive variables, or they possess an independent position and have impacts on intention directly? The research model is presented in Figure 2. We propose that emotional variables have direct effects on intention even though the influence of three TPB variables has been controlled. Due to the aversive natures of diabetic complications and insulin therapy, the negative (rather than positive) anticipated and anticipatory emotions are chosen to be the affective variables in our model. To examine the influences of. 政 治 大. emotions (direct impacts on intention or indirect effects through attitude), the mediator. 立. 學. ‧ 國. analysis will be adopted.. The research hypotheses are as following.. ‧ sit. y. Nat. Hypothesis 1: The TPB variables (attitude, subjective norm, and PBC) are significant. io. er. predictors on intention to take insulin.. al. v. n. Hypothesis 2: Anticipated emotions are significant predictors on intention of taking. i n C insulin with control h ofe the i U n gTPB c hvariables.. Hypothesis 3: Anticipatory emotions are significant predictors on intention of taking insulin with control of the TPB variables. Hypothesis 4: Emotional variables have direct influence on intention to take insulin which is not mediated by attitude.. 28.
(30) Method Participants Participants were recruited in outpatient departments of endocrine and family medicine in a general hospital located in northern Taiwan. The inclusion and exclusion criteria are described below.. Inclusion criteria. 政 治 大 Have ever taken 立OAD for at least 3 months in the past, without use of self-. 1. Documented type 2 diabetic patients who age greater than 20 years. 2.. ‧ 國. 學. injecting insulin currently.. 3. Ability to give written informed consent after being told of the potential. ‧. benefits and harms of the study.. sit. y. Nat. io. er. Exclusion criteria. al. v. n. 1. Currently experiencing a severe physical or mental impairment which restrict. i n C the patients’ participation. hengchi U. 2. Difficulty in verbal or written communication with experimenters.. The research was conducted after ethical approval had been secured from an institutional review broad (IRB). Once agreed to enroll and informed consents were obtained, the participants completed an inventory which is described below. In return for their contribution, participants received NT$ 100 worth of vouchers after they complete the questionnaire. Among all eligible diabetic patients, 459 agreed to participate during a. 29.
(31) period of three months. Two completed questionnaires were discarded due to too many missing values. Therefore, a final sample of 457 entered analysis. Of these 457 participants, 249 were men and 208 women, ranging in age from 20 to 90 years (M = 59.67, SD = 13.62) and mean duration of diabetes was 6.70 years (SD = 6.72). The average HbA1C was 7.27% (SD = 1.21) and average fasting blood sugar 148.62 mg/dL (SD = 46.81) on the day of recruitment. Participants were of the Hoklo (福 佬, 45.30%), Hakka (客家, 42.67%), mainlanders (外省, 10.72%), aborigines (原住民,. 政 治 大. 1.09%) and foreigners (外籍, 0.22%), which is representative of ethnic groups of the. 立. population where the research was executed. The majority of educational level among. ‧ 國. 學. participants is elementary school (26.91%), followed by university and college (25.16%), senior high school (20.13%), junior high school (13.35%), illiteracy (8.75%) and. ‧. graduate school (5.69%). More participants were recruited in endocrine department (291,. y. Nat. sit. 63.68%) than in family medicine (166, 36.32%). Most participants (48.14%) reported. n. al. er. io. they didn’t have any significant other got diabetes, 41.58% reported at least one family. i n U. v. member with diabetes who thought insulin is beneficial, and the rest (10.28%) reported a. Ch. engchi. diabetes family history with regarding insulin as harmful. Three participants (0.66%) didn’t use any medication for blood sugar control, 155 (33.92%) used one kind of OAD, and 299 (65.43%) were taking two or more kinds of OAD. Participants whose HbA1C equal to or greater than 9% were defined as the ‘poor glycemic control’ group. According to the guideline for diabetes management (Rodbard et al., 2009), these patients are suggested to begin insulin treatment for better glycemic control. In other words, these participants are ‘in urge to use insulin’. We examined the. 30.
(32) decision-making process of the poor glycemic control group in particular, and compare it with other participants’, who are in relative better glycemic controlling status.. Measurements The appendix A is the questionnaire used for this study. Details of measurements are provided as following. 1. Behavioral intention. 政 治 大. Behavioral intention was measured using a single item, ‘如果病情有需要,您是否願. 立. 意每天使用胰島素自我注射控制血糖?’ A 4-point scale was used with response. ‧ 國. 學. alternatives labeled ‘強烈不願意’, ‘不太願意’, ‘願意’, and ‘強烈願意’, where 強烈 不願意= 1 and 強烈願意= 4.. ‧. 2. Attitude. y. Nat. io. sit. The measurements of TPB constructs (attitude, subjective norm, PBC) were designed. n. al. er. base on the guidance of a TPB research manual (Francis et al., 2004). Attitude was. i n U. v. assessed by 4 items, which measured participants’ evaluations toward insulin therapy. Ch. engchi. directly. The 5-point scales were used to measure different appraisals, where 完全不 同意= 1, 不同意= 2, 沒意見= 3, 同意=4 and 非常同意= 5. The second and fourth item were reverse scored.. 31.
(33) 您認為每天使用胰島素自我注射,對您而言是… 完全 不同意 □ □ □ □. 1. 有益的。 2. 危險的。 3. 很有幫助。 4. 無法接受。. 不同意. 沒意見. 同意. □ □ □ □. □ □ □ □. □ □ □ □. 非常 同意 □ □ □ □. 治 政 大norm. The opinions of Four 5-point items were used to measure subjective 立. 3. Subjective norm. participants’ important others were assessed. Every item was anchored with ‘完全不. ‧ 國. 學. 同意’ and ‘非常同意’ at both ends. The items were as following, ‘我的家人(如:配. ‧. 偶、父母、子女),會贊成我打胰島素。’ ‘我的好朋友會贊成我打胰島素。’. n. al. er. io. ‘其他的糖尿病患者,會願意接受胰島素注射治療。’. sit. y. Nat. ‘照顧我的醫護人員(如:主治醫師、護理師、營養師),會贊成我打胰島素。’. 4. Perceived behavioral control (PBC). Ch. engchi. i n U. v. PBC was assessed by measuring participants’ “self-efficacy” and “controllability” toward the behavior. The former 2 items were for self-efficacy and the latter 2 were for controllability. A 5-point scale similar to previous ones was used, and the fourth item was reverse scored. These items were: ‘我有信心可以處理好打胰島素這件事。’ ‘我有足夠的能力,可以正確注射胰島 素。’ ‘我可以自行決定是否要接受胰島素注射治療。’ ‘要不要打胰島素這件 事,並非我所能控制的。’. 32.
(34) 5. Anticipatory emotion For the measurements of negative anticipatory emotions, 6 negative emotions (fear, anxiety, surprise, sad, anger, hatred) were indicated for participants to rate. Emotions were chose to fit the possible affective responses may be evoked by the insulin injection behavior (Baumgartner, et al., 2008; Shaver, Schwartz, Kirson, & O'Connor, 1987). Items were measured on 5-point scales, and were introduced with the directive: ‘想到「我必須每天自行注射胰島素來控制血糖」這件事,讓您感覺:’. 治 普通 政 稍微 大. 6. Anticipated emotion. □. □. □ □ □. □. □. □. □. □. □. □. □. □. □. □. □. □. □. □. □. □. □. □. n. al. □. □. Ch. engchi. sit. io. 6. 厭惡。. Nat. 5. 生氣。. □. □. er. 4. 悲傷。. ‧ 國. 3. 驚訝。. □. □. 學. 2. 焦慮。. 非常強烈. ‧. 立. 1. 害怕。. 強烈. y. 完全沒有. i n U. v. To measure the constructs of anticipated emotions, we used the same design as previous researchers did (C. Abraham & Sheeran, 2004; Bagozzi, et al., 2003; M. Conner, et al., 2006; Wang, 2011). That is, ask participants to imagine a scenario in the future, and ask how they will feel in this fictitious circumstance. A 5-point scale was applied also. For negative anticipated emotions, the directive was as following:. 33.
(35) ‘請您想像一下,如果今天您的主治醫師說您血糖控制不理想,建議使用胰 島素注射控制血糖,而您拒絕了。’ ‘五年後,主治醫師對您說:「由於這五年來沒有注射胰島素,你的血糖控 制不理想,身體器官可能已經受到傷害。」這時您的感覺會是:’ Five negative emotions, including regret, anger, disappointment, guilty and scare, were indicated as possible emotional responses.. 完全沒有 1. 後悔。. □. 立. 普通. 政 治 大 □ □ □. □. □. □. 4. 罪惡感。. □. □. □. 5. 害怕。. □. □. □. □. □. □. □. □. □. □. □. □. io. sit. y. Nat. □. n. al. er. 3. 失望。. 非常強烈. ‧. □. 強烈. 學. □. ‧ 國. 2. 生氣。. 稍微. Ch. i n U. v. To ensure the validity and reliability of emotion measurements with the language used. engchi. in our questionnaire (mandarin), we referred to the ongoing research program: 情緒標 準刺激與反應常模的基礎研究 (A Study on Standard Stimuli and Normative Responses of Emotion in Taiwan. http://ssnre.psy.ntu.edu.tw/ssnre/main.htm). With the permission of principal investigator, we adopted the Chinese translation of basic emotions (Ekman, 2007) and of International Affective Pictures System (Bradley & Lang, 2007) in the subdivision of 情緒圖片 (Taiwan Affective Pictures System, TAPS) as our measurement items.. 34.
(36) 7. Insulin Treatment Appraisal Scale (ITAS) For the test of concurrent validity, the Chinese version of ITAS (Chen et al., 2011) was used to evaluate the perception toward insulin therapy at the same time.. 8. Self-management efficacy For the control of a possible confounding factor, the self-management abilities of. 政 治 大 Management Scale (PDSMS) 立 (林淑滿, 林素蘭, 吳月珠, 張純明, & 吳秀麗, 2011). participants were measured by the Chinese version of Perceived Diabetes Self-. ‧ 國. 學. Statistical tests. ‧. Multiple regression and hierarchical multiple regression were used to test the. Nat. sit. y. theoretical framework. The Statistical Product and Service Solutions (SPSS) program,. n. al. er. io. version 18, was employed for the analysis. Statistical significance was set at p < 0.05.. Ch. engchi. 35. i n U. v.
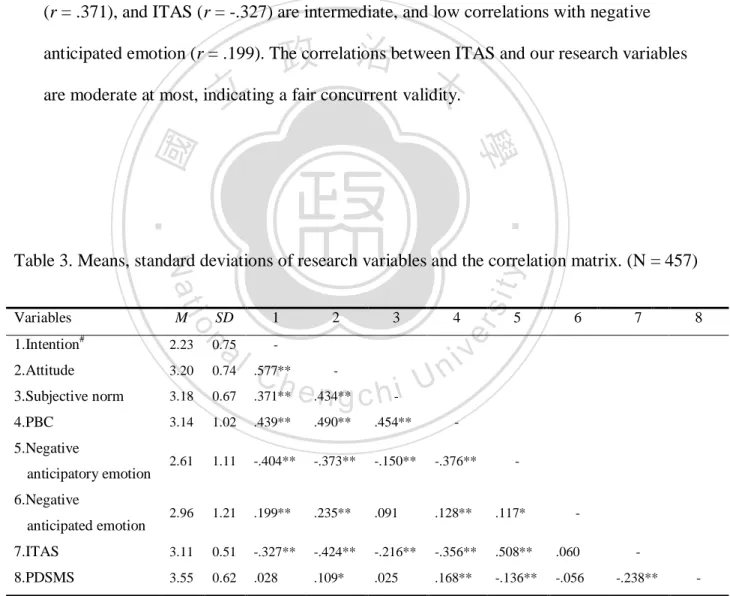
(37) Results More than half of participants (270, 59.08%) indicated that they were unwilling to use insulin therapy (84, 18.38% were strongly unwilling; 186, 40.70% unwilling), compared to 187 (40.92%) said willing to use insulin (183, 40.04% willing; 4, 0.88% strongly willing). The value of insulin intention roughly fits in with normal distribution (Figure 3).. 政 治 大. 立. ‧. ‧ 國. 學. n. er. io. sit. y. Nat. al. Ch. 強烈不願意. engchi. 不太願意. i n U. 願意. v. 非常願意. Figure 3. The distribution of participants’ intention to use insulin A popular statistic tool, Cronbach’s α (Cronbach & Meehl, 1955), was used to examine the reliability of all research variables. The Cronbach’s α value of each independent variable ranges from 0.96 to 0.63. Most measurements have a Cronbach’s α value well above 0.70, with two exceptions: attitude (α = 0.63) and positive anticipatory emotion (α = 0.65). The reliability of PBC improved substantially with exclusion of the. 36.
(38) fourth measuring item (α value raised from 0.64 to 0.80), therefore the former three items were adopted as measurement of this construct. Table 3 presents the means, standard deviations and correlations of all research variables. Intention is significantly correlated with other variables except for PDSMS. There is a high correlation between intention and attitude (r = .577). The correlations of intention with PBC (r = .439), negative anticipatory emotion (r = -.404), subjective norm (r = .371), and ITAS (r = -.327) are intermediate, and low correlations with negative. 政 治 大 are moderate at most, indicating 立 a fair concurrent validity.. anticipated emotion (r = .199). The correlations between ITAS and our research variables. ‧. ‧ 國. 學. 2.23. al. 1. 0.75. -. Ch. 2. 3. sit. SD. 4. er. #. n. 1.Intention. M. io. Variables. y. Nat. Table 3. Means, standard deviations of research variables and the correlation matrix. (N = 457). i n U. 5. 6. 7. v. 2.Attitude. 3.20. 0.74. .577**. 3.Subjective norm. 3.18. 0.67. .371**. 4.PBC. 3.14. 1.02. .439**. .490**. .454**. -. 2.61. 1.11. -.404**. -.373**. -.150**. -.376**. 2.96. 1.21. .199**. .235**. .091. .128**. .117*. 3.11. 0.51. -.327**. -.424**. -.216**. -.356**. .508**. .060. -. 3.55. 0.62. .028. .109*. .025. .168**. -.136**. -.056. -.238**. 5.Negative anticipatory emotion. -. e.434** n g c h-i. 8. -. 6.Negative anticipated emotion 7.ITAS 8.PDSMS #. * p < .05, ** p < .01. Intention: 4-point Likert scale, otherwise 5-point Likert scale.. 37. -. -.
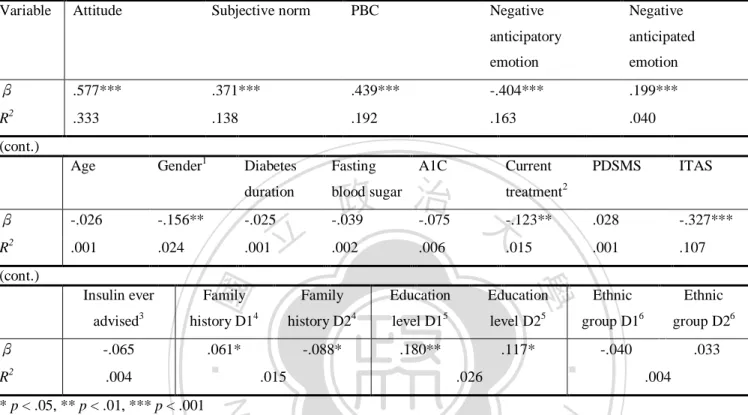
(39) Table 4. The simple regression of how each independent variable predicts intention. (N = 457). Variable. β R. 2. Attitude. Subjective norm. PBC. Negative. Negative. anticipatory. anticipated. emotion. emotion. .577***. .371***. .439***. -.404***. .199***. .333. .138. .192. .163. .040. (cont.) Gender1. Age. A1C. Current. 政 治 大. blood sugar. treatment. PDSMS. ITAS. 2. -.026. -.156**. -.025. -.039. -.075. -.123**. .028. -.327***. .001. .024. .001. .002. .006. .015. .001. .107. Insulin ever advised -.065. R2. .004. Family. history D1. Family 4. 4. Education. 5. 5. history D2. level D1. -.088*. .180**. .061*. .015. level D2 .117* .026. Nat. * p < .05, ** p < .01, *** p < .001. Education. Ethnic. Ethnic 6. group D26. group D1. ‧. β. 3. 學. (cont.). 立. -.040. .033 .004. y. R. 2. Fasting. duration. ‧ 國. β. Diabetes. sit. Dummy variables. 1 Men = 0, women = 1. 2 No OAD or 1 kind OAD = 0, equal to or more than 2 kinds OAD = 1. 3 Never. al. er. io. been told about insulin = 0, ever suggested by physicians to use insulin = 1. 4 D1: No family history = 0, diabetic family. v. n. regarding insulin as harmful = 0, diabetic family regarding insulin as beneficial = 1; D2: No family history = 0, diabetic. Ch. i n U. family regarding insulin as beneficial = 0, diabetic family regarding insulin as harmful = 1. 5 D1: illiteracy and elementary. engchi. school = 0, university/college and graduate school = 0, junior and senior high school = 1; D2: illiteracy and elementary school = 0, junior and senior high school = 0, university/college and graduate school = 1. 6 D1: Hoklo = 0, others = 0, Hakka = 1; Hoklo = 0, Hakka = 0, others = 1.. Table 4 is the simple linear regressions of how intention is affected by each independent variable. All research variables are significantly predictive, and the predictive values of negative anticipatory emotion and ITAS are negative. The most powerful predictor is attitude (β = .577, R2 = .333), followed by PBC (β = .439, R2 = .192), negative anticipatory emotion (β = -.404, R2 = .163), subjective norm (β = .371,. 38.
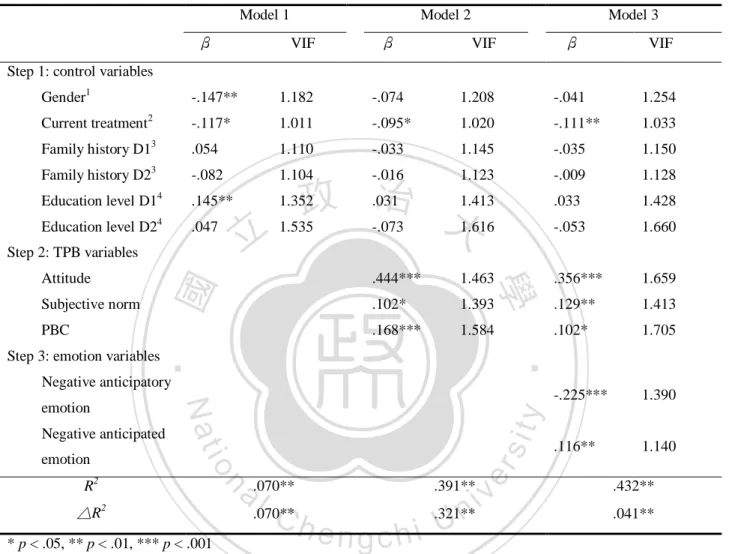
(40) R2 = .138), ITAS (β = -.327, R2 = .107), and negative anticipated emotion (β = .199, R2 = .040). Within background variables, gender, current treatment regimen, family history and educational level are significantly predictive, which will be included in the subsequent analysis as a control. The male participants are more willing to accept insulin therapy than female (β = -.156). Participants who take equal to or more than two kinds of OAD are less likely to use insulin than those who don’t take or take only one kind of. 政 治 大. OAD (β = -.123). The opinion from diabetic family significantly influence intention to. 立. use insulin, the participant has more chance to reject insulin if his or her diabetic family. ‧ 國. 學. think insulin is harmful, and vice versa. Finally, compare to lower educational level (illiteracy and elementary school), participants who get higher education (high school,. ‧. university and graduate school) have more intention in using insulin to control their blood. sit. y. Nat. sugar.. n. al. er. io. To test our hypotheses, a hierarchical regression was conducted first (table 5).. i n U. v. Control variables, TPB variables and emotion variables were entered into analysis in. Ch. engchi. sequence. Low variance inflation factors (VIF) in all three models demonstrate there is no concern of multicollinearity. In model one, the four control variables influence 7.0% of intention variance. In model two, the traditional TPB model accounts for 39.1% variance of participants’ intention to use insulin, producing a significant 32.1% increase of intention explanatory power. All three TPB variables are significant predictors, which support our research hypothesis 1. The standard regression coefficient of attitude, subjective norm and PBC is .444, .102 and .168, respectively. The current treatment is the only control variable which remain significant predictive in model two (β = -.095).. 39.
(41) Table 5. The hierarchical regression of control variables, TPB variables and emotion variables in predicting intention of insulin therapy. (N = 457) Model 1 β. Model 2 VIF. β. Model 3 VIF. β. VIF. Step 1: control variables Gender1 Current treatment. 2. Family history D1. 3 3. Family history D2. -.147**. 1.182. -.074. 1.208. -.041. 1.254. -.117*. 1.011. -.095*. 1.020. -.111**. 1.033. .054. 1.110. -.033. 1.145. -.035. 1.150. -.082. 1.104. -.016. 1.123. -.009. 1.128. Education level D1. 4. .145**. 1.352. .031. 1.413. .033. 1.428. Education level D2. 4. .047. 1.535. -.073. 1.616. -.053. 1.660. .444***. 1.463. .356***. 1.659. .102*. 1.393. .129**. 1.413. .168***. 1.584. .102*. 1.705. Subjective norm PBC. 學. Attitude. ‧. ‧ 國. Step 2: TPB variables. 立. 政 治 大. Step 3: emotion variables. Negative anticipatory. △R. 2. * p < .05, ** p < .01, *** p < .001. -.225***. 1.390. .116**. 1.140. y. a .070** l C .070** h. n. R2. sit. io. emotion. er. Negative anticipated. Nat. emotion. iv .321** n engchi U .391**. .432** .041**. Dummy variables. 1 Men = 0, women = 1. 2 No OAD or 1 kind OAD = 0, equal to or more than 2 kinds OAD = 1. 3 D1: No family history = 0, diabetic family regarding insulin as harmful = 0, diabetic family regarding insulin as beneficial = 1; D2: No family history = 0, diabetic family regarding insulin as beneficial = 0, diabetic family regarding insulin as harmful = 1. 4 D1: illiteracy and elementary school = 0, university/college and graduate school = 0, junior and senior high school = 1; D2: illiteracy and elementary school = 0, junior and senior high school = 0, university/college and graduate school = 1.. In model three, after addition of emotional variables, our hypothesized research model explains a total intention variance up to 43.2%, with an significant increase of. 40.
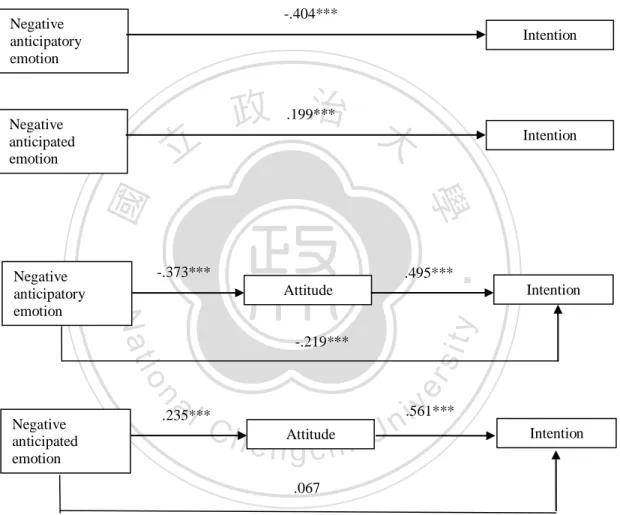
(42) 4.1% explanatory power. Attitude remains the most predictive variable, but a decline in predictive power when influence of emotion variables count (β= .356 in model 3, compare to .444 in model 2). In an order of predictive power, the subsequent variables are: negative anticipatory emotion (β = -.225), subjective norm (β = .129), negative anticipated emotion (β = .116), current treatment (β = -.111), and PBC (β = .102). Such results support our hypothesis 2 and hypothesis 3. What also noteworthy is the current treatment still a significant predictor in model 3, indicates participants use more. 政 治 大. OAD (2 kinds or more) are less willing to consider insulin therapy even controlling the. 立. influences of all variables in our model.. ‧ 國. 學. According to Ajzen (1991), the role of emotions in TPB model are considered as “background variable”, which only influence behavior indirectly through affecting TPB. ‧. variables. To test this idea, we conducted a mediator analysis using a popular method. y. Nat. sit. proposed by Baron and Kenny (1986). With intention as dependent variable and attitude. n. al. er. io. as mediator, the emotion variables were taken as independent variables respectively. i n U. v. (Figure 4). The results revealed with the mediating effect of attitude, negative. Ch. engchi. anticipatory emotion still has significant influences upon intention to use insulin, but negative anticipated emotion doesn’t. The diminished standard regression coefficients indicate partial mediating effects between negative anticipatory emotion and intention (β change from -.404 to -.219, p < .001), and a complete mediating effect between negative anticipated emotion and intention (β change from .199 to .067, p = ns). There is a significant change of effect size with the addition of negative anticipatory emotion (△R2 = .041, p < .001), but not the case with negative anticipated emotion ( △R2 = .004, p = ns).. 41.
(43) Such results supported our hypothesis 4 which emotional variables possess independent position and have direct impacts on intention not mediated by attitude, and this is true especially for negative anticipatory emotion.. -.404***. Negative anticipatory emotion. Intention. ‧. -.373***. .495*** Attitude. y. Intention. er. n. al. sit. -.219***. io Negative anticipated emotion. Intention. 學. ‧ 國. 立. Nat. Negative anticipatory emotion. 政 治 大 .199***. Negative anticipated emotion. Ch. i n U. v. .561***. .235***. e nAttitude gchi. Intention. .067. Figure 4. The examination of attitude’s mediating effect between emotion variables and intention. * p < .05, ** p <. 01, *** p < .001.. 42.
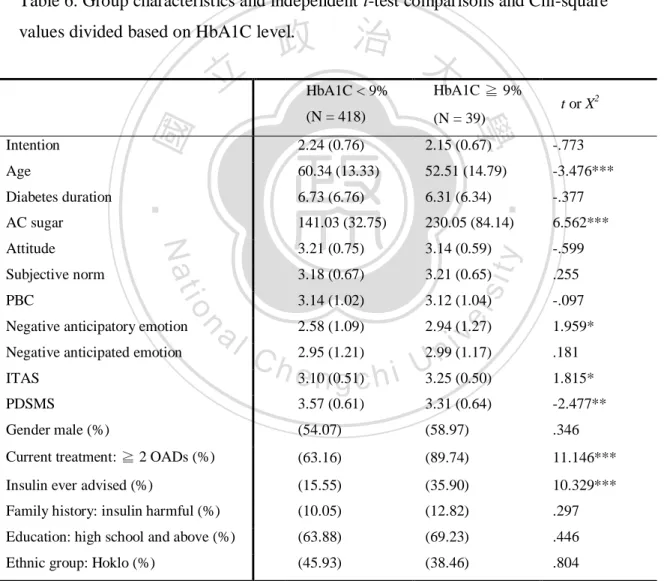
(44) Furthermore, extra analyses were conducted to explore the differences of decision-making process in poor glycemic control (HbA1C ≧ 9%) and relative better glycemic control participants (HbA1C < 9%). An independent t-test and Chi-square analysis using one-tailed test were administered for this purpose (Table 6). There are 39 (8.53%) participants whose HbA1C level equal to or above 9.0% in total.. Table 6. Group characteristics and independent t-test comparisons and Chi-square. 政 治 大. values divided based on HbA1C level.. Subjective norm. io. PBC. al. n. Negative anticipatory emotion Negative anticipated emotion ITAS. t or X2. 2.24 (0.76). 2.15 (0.67). -.773. 60.34 (13.33). 52.51 (14.79). -3.476***. 6.73 (6.76). 6.31 (6.34). -.377. 141.03 (32.75). 230.05 (84.14). 6.562***. 3.21 (0.75). 3.14 (0.59). -.599. 3.18 (0.67). 3.21 (0.65). .255. 3.14 (1.02). 3.12 (1.04). -.097. y. Nat. Attitude. (N = 39). sit. AC sugar. (N = 418). ‧. Diabetes duration. HbA1C ≧ 9%. er. Age. HbA1C < 9%. 學. Intention. ‧ 國. 立. v i(1.17) 2.99 n C h 2.95 (1.21) e3.10n(0.51) g c h i U3.25 (0.50) 2.58 (1.09). 2.94 (1.27). 1.959* .181 1.815*. PDSMS. 3.57 (0.61). 3.31 (0.64). -2.477**. Gender male (%). (54.07). (58.97). .346. Current treatment: ≧ 2 OADs (%). (63.16). (89.74). 11.146***. Insulin ever advised (%). (15.55). (35.90). 10.329***. Family history: insulin harmful (%). (10.05). (12.82). .297. Education: high school and above (%). (63.88). (69.23). .446. Ethnic group: Hoklo (%). (45.93). (38.46). .804. * p < .05, ** p < .01, *** p < .001, one-tailed test. Values are mean (standard deviation) unless otherwise indicated.. 43.
(45) Although participants in worse glycemic control group have more chance being suggested by their physicians to use insulin (35.90% vs. 15.55%; t = 10.329, p < .001), they don’t have more intention in insulin therapy (t = -.773, p = ns). The duration of being diagnosed as diabetic patients doesn’t differ in better-control and worse-control groups (t = -.377, p = ns), but the participants in worse glycemic control group are younger (52.51 years vs. 60.34 years; t = -3.476, p < .001). Values of ITAS and PDSMS are also different between both groups (ITAS: 3.25 vs. 3.10; t = 1.815, p < .05. PDSMS:. 政 治 大 more negative perception立 about insulin, and less self-management ability over their. 3.31 vs. 3.57; t = -2.477, p < .01), indicate participants in worse-control group have a. ‧ 國. 學. diabetes.. The most noteworthy is, among all variables in our hypothesized model, negative. ‧. anticipatory emotion is the only one significantly differ between two groups (2.94 vs.. sit. y. Nat. 2.58; t = 1.959, p < .05). Such a result reveals participants in worse-control group have. io. er. stronger negative feelings toward insulin therapy itself, which may prohibit their. al. iv n C therapy for them to achieve optimal h eglycemic h i Ubut emotionally their strong n g c control, n. acceptance of insulin. In other words, they may rationally realize the necessity of insulin. aversion toward insulin prevents them from taking insulin as a treatment option. In this case, the negative anticipatory emotion could be the most predictive variable of insulin intention in worse-control group. For further verification of this rationale, the stepwise regression was employed to determine which variable is most predictive. The comparison of stepwise regressions using all participants, participants whose HbA1C < 9% and HbA1C ≧ 9% are listed in table 7. The stepwise regression result of better-control group is grossly resemble the one. 44.
(46) of total sample. There are six variables added in these two analyses. The most predictive variable are both attitude (all: β = .352, better-control: β = .349), followed by negative anticipatory emotion (all: β = -.238, better-control: β = -.240). And the. Table 7. Comparison of stepwise regressions divided into groups based on HbA1C level to predict intention. For neat, only the last steps of stepwise regressions are presented.. All (N = 457). -.238***. -.109**. .113**. emotion 6.PBC. .095*. 2.Subjective. -.240***. norm. emotion. .419**. .395**. y. .132**. 5.Negative anticipated. anticipatory. 3.PBC. .106*. 4.Negative. a l anticipated .118** iv n C emotion hengchi U. n. treatment1. 1.Attitude. 2.Negative. io. 4.Current. .349***. β. sit. norm. 1.Attitude. Nat. 3.Subjective. .352***. Added variables. er. emotion. β. Added variables. ‧. anticipatory. β. ‧ 國. 2.Negative. 立. Step 2. R2 = .463***. Step 7. R = .424***. 學. 1. Attitude. HbA1C ≧ 9% (N = 39). 2. Step 7. R = .426***. Added variables. 政 治 大. HbA1C < 9% (N = 418). 2. 5.Current. treatment1 6.Subjective norm. -.115**. .117**. * p < .05, ** p < .01, *** p < .001. 1 Dummy variable: no OAD or 1 kind OAD = 0, equal to or more than 2 kinds OAD = 1. Candidate predictor variables: current treatment, attitude, subjective norm, PBC, negative anticipatory emotion, negative anticipated emotion.. 45.
(47) subsequent in total sample analysis are: subjective norm, current treatment, negative anticipated emotion, and PBC (β = .132, -.109, .113, and .095 respectively), in bettercontrol group analysis are: PBC, negative anticipated emotion, current treatment, and subjective norm (β = .106, .118, -.115, and .117 respectively). In worse-control group, however, the stepwise regression comes to two significantly predictive variables: attitude (β = .419) and subjective norm (β = .395). None of the emotion variable exhibits predictive power toward insulin intention. Such results may suggest the participants in. 政 治 大. worse-control and better-control groups have different decision-making processes about. 立. insulin. We will discuss this in detail in the following chapter.. ‧. ‧ 國. 學. n. er. io. sit. y. Nat. al. Ch. engchi. 46. i n U. v.
(48) Discussion To our knowledge, this study is the first to explore both cognitive and affective factors of how type 2 diabetic patients decide to start insulin therapy. Furthermore, we distinguished affect into two dimensions: one anticipatory, another anticipated. The wellestablished TPB model was adopted as our theoretical basis, with anticipatory and anticipated emotions in addition to expand the predictive power. The results revealed not only three TPB variables (attitude, subjective norm and PBC) significantly predict. 政 治 大 emotion, have considerable 立impacts on decision-making process about insulin. The. intention of insulin therapy, but also emotional variables, especially negative anticipatory. ‧ 國. 學. differences of influencing factors toward insulin intention between better glycemiccontrol and worse glycemic-control diabetic patients also warrant further discussion.. ‧ sit. y. Nat. Intention and demographical variables. io. er. In our survey, the rate of unwilling to take insulin among type 2 diabetic patients. al. iv n C countries (Larkin, et al., 2008; Polonsky, h e n gHajos, i U& Snoek, 2011), yet lower than in c hDain, n. was approximate 60%. This refusal rate is higher than similar studies in Western. other Chinese society (Wong, et al., 2011). It demonstrates the prevalence of PIR and its profound influence on clinical diabetes care. We also found some demographical variables, including gender, current treatment regimen, family history and educational level can solely predict insulin intention. In precedent studies, demographical factors such as male gender, higher educational level were also positively predictive of diabetic patients’ intention to take insulin (Lerman et al., 2009; Wong, et al., 2011). However, in the multiple regression with control of other. 47.
(49) variables’ influence, current treatment regimen is the only demographical factor still remaining predictive. Compare to those who take fewer OAD, the participants taking equal to or more than two kinds of OAD significantly have fewer intention to use insulin. The effect is noteworthy because it exists independently from other cognitive or affective predictors. This could be due to once patients in poor glycemic control refuse insulin, the physicians tend to prescribe more OADs instead. As a result, poor-control yet insulinrefusing patients get more OADs than other diabetic patients. It may be evidenced by our. 政 治 大 worse-control group has立 a higher ratio taking equal to or more than two kind of OADs. comparison between worse-control and better-control participants, which revealed the. ‧ 國. 學. Problem one: How is the utility of TPB model in predicting type 2 diabetic patients’. ‧. intention for insulin therapy?. sit. y. Nat. TPB had been applied successfully in several diabetes-related behaviors. For. io. er. instance, the prediction of self-care behavior (Gatt & Sammut, 2008), the prediction of. al. iv n C U enhancement of insulin Courneya, Birkett, & Sigal, 2010), the intervention he n g c h i for n. aerobic physical activity for type 1 and type 2 diabetes adults (Plotnikoff, Lippke,. administration in young adults with type 1 diabetes (Louch, Dalkin, Bodansky, & Conner, 2013), and the intervention to promote regular physical activity and healthy eating among old adults with type 2 diabetes (White et al., 2012). In our study, the TPB model was demonstrated to be valid in prediction of type 2 diabetic patients’ intention for insulin therapy. The three TPB variables were all significant predictors, in a sequence of predictive power being attitude, PBC and subjective norm. Interestingly, in another study addressing the same issue using a similar theory, the author concluded that the subjective. 48.
數據


+7
相關文件
To ensure the Xianbei and Han people would live together peacefully, Emperor Xiaowen (reigned 471-499) not only moved the capital from Pingcheng to Luoyang, but also carried out
The compilers of the biographies of monks not only wrote about the crucial life experiences of these eminent monks, but also revealed wonderful affi nities that brought them
The well-known halting problem (a decision problem), which is to determine whether or not an algorithm will terminate with a given input, is NP-hard, but
Fayun’s annotation is according to Kumarajiva’s original translation, not only sentences by the strict branch demonstrates it to the Lotus Sutra, also aware of
Regardless of the assumed copula functions, we consistently find that the Chinese market experiences not only a higher degree of dependence but also a higher variation of
It is interesting to discover that the golden ratio appears not only in the fluid sink and heat source induced maximum ground surface horizontal displacements, but also on
After the implementation of the New Scoring Criteria, not only the number of foreign students who came to Taiwan to study increased, but also the number of people who
Doing-undoing (the capacity not only able to use a process to get to a goal, but also to understand the process well enough to work backward from the answer to the starting
