Elsevier Editorial System(tm) for Journal of the Formosan Medical Association Manuscript Draft
Manuscript Number: JFMA-D-11-00060R1
Title: Haemophilus influenzae type b combination vaccines and atopic disorders: a prospective cohort study
Article Type: Original Article
Keywords: atopic dermatitis, recurrent wheezing, Haemophilus influenzae type b, vaccines Corresponding Author: Professor Pau-Chung Chen, M.D., Ph.D.
Corresponding Author's Institution: National Taiwan University College of Public Health First Author: I-Jen Wang
Order of Authors: I-Jen Wang; Li-Min Huang; Yueliang Leon Guo; Wu-Shiun Hsieh; Tien-Jen Lin; Pau-Chung Chen, M.D., Ph.D.
Abstract: Background/Purpose: Epidemiologic evidence for an association between vaccinations and atopy development is inconsistent. We evaluated the influence of Haemophilus influenzae type b (Hib) combination vaccines in 6 month old infants on the prevalence of atopic disorders in 18 month old children.
Methods: We used multistage, stratified systematic sampling to recruit 24,200 mother-newborn pairs from the Taiwan national birth registration in 2005. Vaccination status was ascertained through official vaccine cards, while risk factors for atopic disorders were gathered by questionnaires at 6 months of age. Information about development of atopic dermatitis (AD) and recurrent wheezing was collected at 18 months of age. The relationship between atopic disorders and Hib combination vaccines, diphtheria-pertussis-tetanus-Hib and oral poliomyelitis vaccines (Hib&OPV) and DPT-Hib-inactivated poliomyelitis vaccines (DPT-Hib-IPV), were estimated by multiple logistic regression. Results: A total of 19,968 children completed the follow-up and participated in the study. AD was noted in 1584 (7.9%) infants while recurrent wheezing was found in 1,220 (6.1%). The adjusted ORs (95% CI) for the development of AD in the DPT-Hib&OPV and DPT-Hib-IPV vaccination groups were given as 1.38 (1.15-1.65) and 1.49 (1.29-1.72), compared to those without Hib vaccination (DTP&OPV
vaccination). However, the association between DPT-Hib&OPV and DPT-Hib-IPV vaccinations and recurrent wheezing failed to reach statistical significance.
Conclusion: There is a minimal risk for AD after receiving Hib combination vaccines. Whether the trivial adverse impact to increased risk of atopic disorders outweighs the Hib vaccination importance in public health for infectious diseases spreading warrants further investigation.
Response to Reviewers: Dear Reviewers,
Thank you for your precious commentary. We have made several changes in this manuscript as
requested carefully and hope it will fulfill your requirement. Detailed corrections are listed below point by point and manuscript revisions are clearly underlined. A revised version of our manuscript has been taken into account the comments with great efforts and please consider for eventual publication of this manuscript.
Reply to Reviewer 1 General comments: Question
1.This manuscript is well written with careful design. The sample size is adequate with good follow-up. It has taken into account most hereditary and environmental factors that might foster allergy
development. The statistics are sound. Answer
Thank you for your commentary. Question
2. My concern is that it may be too early to be sure of the Hib vaccination on atopic disorders at 18 month old, at which time, the children just received the last boostered dose. Besides, wheezing at or before this age could be wheezing associated with viral infection, which may not be allergy-related. Answer
Thank you for your suggestion. This is one of our limitation. The ages of the children in our study might be too young to fully evaluate the risk of atopic disorders. However, approximately 60% of AD cases arose in the first year of life. That 7.9% of the children in our study developed AD also suggested that the age of the children was not a major limitation.
As you mentioned, it is true that wheezing at or before this age could be wheezing associated with viral infection, which may not be allergy-related. Therefore, we tried to restrict our subjects to children ever had recurrent wheezing in the chest more than 3 episodes. Recurrent wheezing is much more related than one episode of wheezing.15 Moreover, it may be because wheezing is not very allergy-specific that we did not find significant association of the Hib vaccination on wheezing.
Question
3.The authors should be careful about the wording of the conclusion. "minimal" or "trivial" usually suggest it's OK to receive Hib, instead of needing further investigations.
Answer
Thank you for your suggestion. We have changed “minimal risk” to ‘There is a “potential risk” for AD after receiving Hib combination vaccines.’ Please replace it with the better words if you have. Thank you very much !
Other points : Question
1) 本研究外籍母親在 DTP and OPV 組高達 29.5%,與他組約 6~7%明顯有差異,在 table 1 中並無顯
示外籍新娘之國籍種類(大陸、印尼、越南等), 請詳列各組國藉不同之比例,並依此修正 table 4 或其
他研究之結果。 Answer
謝謝您的建議, 已詳列各組國藉不同之比例 於 Table 1 之 Maternal Nationality 項目. 並依此修正其他 研究之結果。 (請看 Table 1)
2) 外籍母親如此高之情形下,請問問卷有依國籍之不同做區分外,若無,如何排除文字上及語言上 之障礙,以確保問卷回答之正確性。 Answer 有6 種不同語言的問卷依不同國籍所會的的語言給外籍母親填寫,若母親仍不清楚,訪員會打電話 依母親所會的的語言再詢問一次,排除文字上及語言上之障礙,以確保問卷回答之正確性。 Question 3) 本研究是依問卷來診斷異位性皮膚炎,有相當大之不確定性,在討論中請提出佐證本研究問卷用 來診斷異位性皮膚炎的臨床正確性有多少,是否是目前最好的診斷工具,並討論此問卷與其他用來 診斷異位性皮膚炎問卷正確性之比較。 Answer
AD was diagnosed using four different criteria, the Hanifin and Rajka criteria, the Schultz-Larsen criteria, the Danish Allergy Research Centre (DARC) criteria developed for this study and doctor-diagnosed visible eczema with typical morphology and atopic distribution. Additionally, the U.K. diagnostic criteria based on a questionnaire were used at 1 year of age. The diagnostic criteria
developed by Hanifin and Rajka are most widely accepted (Hanifin et al. 1998). A comparison between criteria for diagnosing atopic eczema in infants has been performed in one study by Johnke et al.2005. Agreement between the four criteria was analysed at each time point and over time, and agreement between the four criteria and the U.K. questionnaire criteria was analysed. The pairwise agreement between criteria showed good agreement, with rates varying between 93% and 97% and kappa scores between 0.6 and 0.8. Agreement analysis of diagnoses between the four criteria demonstrated that cumulative incidences showed better agreement than point prevalence values. Agreement between different criteria for diagnosing AD was acceptable, but the mild cases constituted a diagnostic problem, although they were in the minority. Repeated examinations gave better agreement between diagnostic criteria than just one examination.
Although the diagnostic criteria developed by Hanifin and Rajka are most widely accepted, it must be performed by a physician. Since it is difficult to use Hanifin and Rajka criteria in large epidemiological studies and the agreement between different criteria for diagnosing AD was acceptable, we chose maternal report doctor-diagnosed visible eczema with typical morphology and atopic distribution to diagnose AD, which has been previously used by many studies.
Discussion:
Our study was limited by the use of questionnaire for ascertaining AD, which might not be accurate as the standard diagnostic criteria by a dermatologist (Hanifin et al. 1980). Nevertheless, maternal report of doctor-diagnosed visible eczema with typical morphology and atopic distribution has been
previously validated versus clinical examination in the studies performed in the United States and Denmark (Laughter et al. 2000; Benn et al. 2004) and has been used by many epidemiological studies (Moore et al. 2004, Purvise al.2005; Wang et al. 2007.)
Reference:
Johnke H, Vach W, Norberg LA, Bindslev-Jensen C, Host A, Andersen KE. A comparison between criteria for diagnosing atopic eczema in infants. Br J Dermatol 2005;153:352-8.
Laughter D, Istvan JA, Tofte SJ, Hanifin JM. The prevalence of atopic dermatitis in Oregon schoolchildren. J Am Acad Dermatol 2000;43:649-55.
Benn CS, Wohlfahrt J, Aaby P, et al. Breastfeeding and risk of atopic dermatitis, by parental history of allergy, during the first 18 months of life. Am J Epidemiol 2004;160:217-23.
Moore MM, Rifas-Shiman SL, Rich-Edwards JW, et al. Perinatal predictors of atopic dermatitis occurring in the first six months of life. Pediatrics 2004;113:468-74.
Purvis DJ, Thompson JM, Clark PM, Robinson E, Black PN, Wild CJ, Mitchell EA.
Risk factors for atopic dermatitis in New Zealand children at 3.5 years of age. Br J Dermatol. 2005;152:742-9.
Wang IJ, Guo YL, Wen HJ, et al. Environmental risk factors for early infantile atopic dermatitis. Pediatric Allergy Immunol 2007;18; 441-7.
---Table Diagnostic Features of Atopic Dermatitis (Hanifin and Rajka criteria)
________________________________________ Major features
Pruritus
Chronic or relapsing dermatitis
Personal or family history of atopic disease
Typical distribution and morphology of atopic dermatitis rash: Facial and extensor surfaces in infants and young children Flexure lichenification in older children and adults Minor features
Eyes
Cataracts (anterior subcapsular) Keratoconus
Infraorbital folds affected Facial pallor Palmar hyperlinearity Xerosis Pityriasis alba White dermatographism Ichthyosis Keratosis pilaris
Nonspecific dermatitis of the hands and feet Nipple eczema
Positive type I hypersensitivity skin tests Propensity for cutaneous infections Elevated serum IgE level
Food intolerance
Impaired cell-mediated immunity Erythroderma
Early age of onset
*The diagnosis of atopic dermatitis should be suspected if three major criteria and three minor criteria are present. --- Question 4) 家庭收入也是影響本研究會有誤差之因素,請問家庭收入依 <5 萬,5 萬~10 萬,及>10 萬分配之 依據。 Answer 根據訪查前行政院主計處的家庭收支調查,顯示台北縣平均每戶家庭收入為 4 萬~5 萬,因此本研究 以5 萬設為一級距,將本研究之家庭收入變項區分為小於 5 萬,5 萬-10 萬及大於 10 萬。
Question
5) 城鄉差距的定義如何?是如何區分出來的,請補充在文章中。 Answer
Urban area: city 都市、城市 Suburban: town 鎮、鄉 Rural area: village 村、鄰 已補充在文章Table 1 footnot 中 在城市與鄉村的分類上,常見以都市化程度為依據,以人口密度為重要指標。依據人口密度高且暫 離率低的歸類為城市,而人口密度低且暫離率高的歸為鄉村。 城市與鄉村的差異,城市與鄉村居民的組成也會有所差異。基於城鄉組成因素、環境條件和產業結 構等差異之狀況下,造成城市聚落居民和鄉村聚落居民社經條件、社會組成和社會網絡關係等的差 異。城市與鄉村的特性、發展與課題都有所不同,台灣的城市有明顯的現代化,並且有完善的基本 設施、行政組織和金融機構等多方面的生活配備,但是有較嚴重的社會問題,還有實質環境的問題 ,像是交通擁擠、住宅問題或廢棄物等問題。反觀鄉村的發展並沒有城市來的健全,但不會擁有城 市那麼多社會問題的出現,可是鄉村有人口流失、撫養率偏高與公共設施不足等課題需要解決。 Question 6) 請加入另一個表格,將三組疫苗注射組發生異位性皮膚炎的各項變數(影響因子)的統計結果及方法 呈現出來。 Answer 已將發生異位性皮膚炎的各項變數(影響因子)的統計結果及方法呈現於以下表格
After adjusting for potential confounders of infant gender, preterm birth, maternal history of atopy, maternal education and nationality, family income, place of residence, duration of breast feeding, older siblings, fungi at house wall, and ETS exposure, the effect of vaccination on AD still persists.
---
Table3 The potential confounders for atopic dermatitis and recurrent wheezing Atopic dermatitis N=1584 Recurrent wheezing
N=1220
n (%) Crude OR
(95% CI) n (%) Crude OR (95% CI)
Maternal education (%)
Junior high school and below 97(6.1) 1 152(12.5) 1
Senior high school and above 1485(93.9) 0.57 (0.45-0.72)* 1067(87.5) 1.02(0.83-1.25)
Maternal nationality (%)
Taiwan 1498(94.6) 1 1102(90.3) 1
Foreign countries 86(5.4) 1.70(1.37-2.25)* 118(9.7) 1.34(1.07-1.68) Place of residence since birth (%)
Urban area 891(56.4) 1 531(43.6) 1
Rural area 284(18.0) 1.19(1.01-1.40)* 291(23.9) 1.18(1.02-1.39)* Family income per month (NT$) (%)
50,000 491(31.0) 1 448(36.8) 1
50,000~100,000 831(52.5) 0.65(0.55-0.76)* 645(52.9) 0.98(0.79-1.21) >100,000 260(16.4) 0.80(0.69-0.93)* 126(10.3) 1.21(1.00-1.48)
---
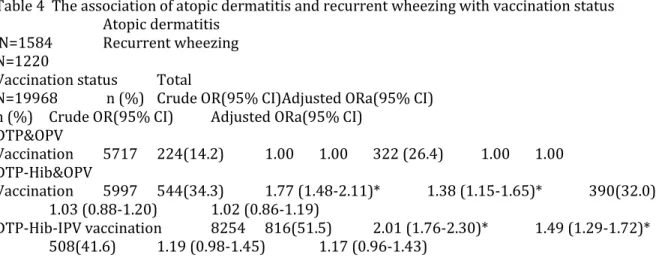
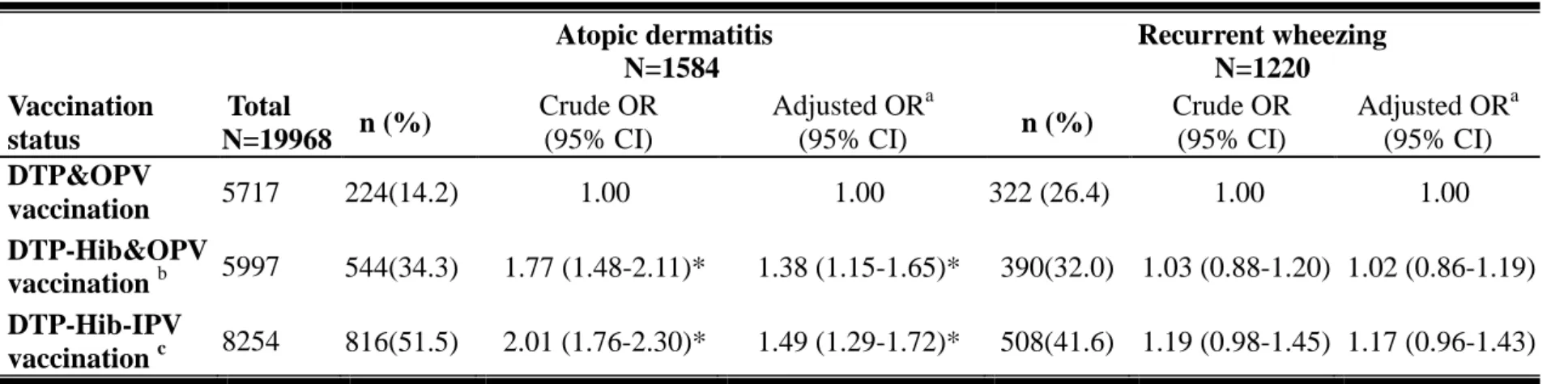
Table 4 The association of atopic dermatitis and recurrent wheezing with vaccination status Atopic dermatitis
N=1584 Recurrent wheezing N=1220
Vaccination status Total
N=19968 n (%) Crude OR(95% CI)Adjusted ORa(95% CI) n (%) Crude OR(95% CI) Adjusted ORa(95% CI)
DTP&OPV Vaccination 5717 224(14.2) 1.00 1.00 322 (26.4) 1.00 1.00 DTP-Hib&OPV Vaccination 5997 544(34.3) 1.77 (1.48-2.11)* 1.38 (1.15-1.65)* 390(32.0) 1.03 (0.88-1.20) 1.02 (0.86-1.19) DTP-Hib-IPV vaccination 8254 816(51.5) 2.01 (1.76-2.30)* 1.49 (1.29-1.72)* 508(41.6) 1.19 (0.98-1.45) 1.17 (0.96-1.43) ---
a. Model is adjusted for infant gender, preterm birth, maternal history of atopy, maternal education and nationality, family income, place of residence, duration of breast feeding, older siblings, fungi at house wall, and ETS exposure
Question
7) 討論中均沒有提到反覆喘鳴為何在三組疫苗注射組並無差異性,其他的研究結果也可比較,請補 充。
Answer
為何反覆喘鳴在三組疫苗注射組並無差異性,已加入其他類似研究做補充於 Discussion.如 reference 25 Interestingly, we found infants with Hib vaccination was associated with AD while compared to those without Hib vaccination. However, Hib vaccination failed to reach statistically significant association with recurrent infant wheezing. Different pathogenesis between AD and wheezing might account for this finding. Another cohort study in Taiwan, with similar prevalence of wheezing, found that recurrent infant wheezing during the first 18 months of age may not be related with allergy sensitization.25 Alternatively, it was associated with the Clara cell protein 10 (CC10) G+38A polymorphism and lower CC10 levels. Further follow up of this cohort is warranted to clarify this problem.
25. Yang KD, Ou CY, Chang JC, et al. Infant frequent wheezing correlated to Clara cell protein 10 (CC10) polymorphism and concentration, but not allergy sensitization, in a perinatal cohort study. J Allergy Clin Immunol 2007;120:842-8.
Reply to Reviewer 2 Question
1. This is a well-designed and successful follow up cohort study, but the one-year follow up is too short to conclude the association between vaccination and atopic disorders.
Answer
Thank you for your suggestion. This is one of our potential limitation. The ages of the children in our study might be too young to fully evaluate the risk of atopic diseases. However, approximately 60% of AD cases arose in the first year of life.26 That 7.9% of the children in our study developed AD also suggested that the age of the children was not a major limitation. We will try to follow up this cohort and get better results in the future.
Question
2. It is also important to obtain the prevalence of atopic dermatitis and recurrent wheezing in the cohort study, and found that infants with the DPT-Hib&OPV and DPT-Hib-IPV vaccination were significantly assocaited with AD while compared to those without Hib vaccination
(DTP&OPVvaccination), but the DPT-Hib&OPV and DPT-Hib-IPV vaccinations failed to reach statistical significance with recurrent wheezing. The infant recurrent wheezing rate was similar to that reported by another cohort study done in Taiwan (J Allergy Clin Immunol 120:842-8, 2007), in which the recurrent infant wheezing was not significantly associated with allergy sensitization. The authors may be able to discuss the results derived from these 2 cohort studies done in Taiwan, and make a better interpretation on why infants with the DPT-Hib&OPV and DPT-Hib-IPV vaccination were significantly assocaited with AD while compared to those without Hib vaccination (DTP&OPVvaccination), but the DPT-Hib&OPV and DPT-Hib-IPV vaccinations failed to reach statistical significance with recurrent wheezing.
Answer
Thank you for your suggestion. We have discussed the results derived from these 2 cohort studies done in Taiwan. We have made a better interpretation and have added this study in our reference. (See page 12 last paragraph and reference 25)
Interestingly, we found infants with Hib vaccination was associated with AD while compared to those without Hib vaccination. However, Hib vaccination failed to reach statistically significant association with recurrent infant wheezing. Different pathogenesis between AD and wheezing might account for this finding. Another cohort study in Taiwan, with similar prevalence of wheezing, found that recurrent infant wheezing during the first 18 months of age may not be related with allergy sensitization.25 Alternatively, it was associated with the Clara cell protein 10 (CC10) G+38A polymorphism and lower CC10 levels. Further follow up of this cohort is warranted to clarify this problem.
25. Yang KD, Ou CY, Chang JC, et al. Infant frequent wheezing correlated to Clara cell protein 10 (CC10) polymorphism and concentration, but not allergy sensitization, in a perinatal cohort study. J Allergy Clin Immunol 2007;120:842-8.
3. This cohort has been followed up for at least 5 years, if the authors could show some data regarding the atopic rates in 3 years of age, they may be able to provide a better correlation between vaccination and atopic disorder, for repeated infant wheezing disorders in 18 months old are not significantly linked to atopic diseases.
Answer
It’s a very good suggestion. However, the data regarding the atopic rates in 3 years of age is not available now. We have tried our best to analyze the data we have.
Dear Editor-in-Chief, May 23, 2011
Thank you for your precious commentary. We have made several changes in this
manuscript as demanded. A revised version of our manuscript has been taken into account the comments of the editors with great efforts and please consider for eventual publication of this manuscript. Thank you for your kind consideration and critical review. All of us look forward to hearing from you.
With best wishes,
Professor Pau-Chung Chen,
Institute of Occupational Medicine and Industrial Hygiene, National Taiwan University College of Public Health #17, Syujhou Road, Taipei 10055, Taiwan.
Tel.: +886-2-33668088 Fax: +886-2-23582402 Email: [email protected]
Dear Reviewers,
Thank you for your precious commentary. We have made several changes in this manuscript as requested carefully and hope it will fulfill your requirement. Detailed corrections are listed below point by point and manuscript revisions are clearly underlined. A revised version of our manuscript has been taken into account the comments with great efforts and please consider for eventual publication of this manuscript.
Reply to Reviewer 1
General comments:
Question
1.This manuscript is well written with careful design. The sample size is adequate with good follow-up. It has taken into account most hereditary and environmental factors that might foster allergy development. The statistics are sound.
Answer
Thank you for your commentary.
Question
2. My concern is that it may be too early to be sure of the Hib vaccination on atopic disorders at 18 month old, at which time, the children just received the last boostered dose. Besides, wheezing at or before this age could be wheezing associated with viral infection, which may not be allergy-related.
Answer
Thank you for your suggestion. This is one of our limitation. The ages of the children in our study might be too young to fully evaluate the risk of atopic disorders. However,
approximately 60% of AD cases arose in the first year of life. That 7.9% of the children in our study developed AD also suggested that the age of the children was not a major limitation.
As you mentioned, it is true that wheezing at or before this age could be wheezing associated with viral infection, which may not be allergy-related. Therefore, we tried to restrict our
subjects to children ever had recurrent wheezing in the chest more than 3 episodes. Recurrent wheezing is much more allergy-related than one episode of wheezing.15 Moreover, it may be because wheezing is not very allergy-specific that we did not find significant association of the Hib vaccination on wheezing.
Question
3.The authors should be careful about the wording of the conclusion. "minimal" or "trivial" usually suggest it's OK to receive Hib, instead of needing further investigations.
Answer
Thank you for your suggestion. We have changed “minimal risk” to „There is a “potential risk” for AD after receiving Hib combination vaccines.‟ Please replace it with the better words if you have. Thank you very much !
Other points :
Question
1) 本研究外籍母親在 DTP and OPV 組高達 29.5%,與他組約 6~7%明顯有差異,在 table 1 中並無顯示外籍新娘之國籍種類(大陸、印尼、越南等), 請詳列各組國藉不同之比例, 並依此修正 table 4 或其他研究之結果。
Answer
謝謝您的建議, 已詳列各組國藉不同之比例 於 Table 1 之 Maternal Nationality 項目. 並依此修正其他研究之結果。 (請看 Table 1)
Question
2) 外籍母親如此高之情形下,請問問卷有依國籍之不同做區分外,若無,如何排除文 字上及語言上之障礙,以確保問卷回答之正確性。
Answer
有 6 種不同語言的問卷依不同國籍所會的的語言給外籍母親填寫,若母親仍不清楚,訪 員會打電話依母親所會的的語言再詢問一次,排除文字上及語言上之障礙,以確保問卷 回答之正確性。Question
3) 本研究是依問卷來診斷異位性皮膚炎,有相當大之不確定性,在討論中請提出佐證 本研究問卷用來診斷異位性皮膚炎的臨床正確性有多少,是否是目前最好的診斷工具, 並討論此問卷與其他用來診斷異位性皮膚炎問卷正確性之比較。Answer
AD was diagnosed using four different criteria, the Hanifin and Rajka criteria, the
Schultz-Larsen criteria, the Danish Allergy Research Centre (DARC) criteria developed for this study and doctor-diagnosed visible eczema with typical morphology and atopic
distribution. Additionally, the U.K. diagnostic criteria based on a questionnaire were used at 1 year of age. The diagnostic criteria developed by Hanifin and Rajka are most widely accepted (Hanifin et al. 1998). A comparison between criteria for diagnosing atopic eczema in infants has been performed in one study by Johnke et al.2005. Agreement between the four criteria was analysed at each time point and over time, and agreement between the four criteria and the U.K. questionnaire criteria was analysed. The pairwise agreement between criteria showed good agreement, with rates varying between 93% and 97% and kappa scores between 0.6 and 0.8. Agreement analysis of diagnoses between the four criteria demonstrated that cumulative incidences showed better agreement than point prevalence values. Agreement between different criteria for diagnosing AD was acceptable, but the mild cases constituted a diagnostic problem, although they were in the minority. Repeated examinations gave better
agreement between diagnostic criteria than just one examination.
Although the diagnostic criteria developed by Hanifin and Rajka are most widely accepted, it must be performed by a physician. Since it is difficult to use Hanifin and Rajka criteria in large epidemiological studies and the agreement between different criteria for diagnosing AD was acceptable, we chose maternal report doctor-diagnosed visible eczema with typical morphology and atopic distribution to diagnose AD, which has been previously used by many studies.
Discussion:
Our study was limited by the use of questionnaire for ascertaining AD, which might not be accurate as the standard diagnostic criteria by a dermatologist (Hanifin et al. 1980).
Nevertheless, maternal report of doctor-diagnosed visible eczema with typical morphology and atopic distribution has been previously validated versus clinical examination in the studies performed in the United States and Denmark (Laughter et al. 2000; Benn et al. 2004) and has been used by many epidemiological studies (Moore et al. 2004, Purvise al.2005; Wang et al. 2007.)
Reference:
Johnke H, Vach W, Norberg LA, Bindslev-Jensen C, Host A, Andersen KE. A comparison between criteria for diagnosing atopic eczema in infants. Br J Dermatol 2005;153:352-8. Laughter D, Istvan JA, Tofte SJ, Hanifin JM. The prevalence of atopic dermatitis in Oregon schoolchildren. J Am Acad Dermatol 2000;43:649-55.
Benn CS, Wohlfahrt J, Aaby P, et al. Breastfeeding and risk of atopic dermatitis, by parental history of allergy, during the first 18 months of life. Am J Epidemiol 2004;160:217-23. Moore MM, Rifas-Shiman SL, Rich-Edwards JW, et al. Perinatal predictors of atopic dermatitis occurring in the first six months of life. Pediatrics 2004;113:468-74. Purvis DJ, Thompson JM, Clark PM, Robinson E, Black PN, Wild CJ, Mitchell EA.
Risk factors for atopic dermatitis in New Zealand children at 3.5 years of age. Br J Dermatol. 2005;152:742-9.
Wang IJ, Guo YL, Wen HJ, et al. Environmental risk factors for early infantile atopic dermatitis. Pediatric Allergy Immunol 2007;18; 441-7.
--- Table Diagnostic Features of Atopic Dermatitis (Hanifin and Rajka criteria)
Major features
Pruritus
Chronic or relapsing dermatitis
Personal or family history of atopic disease
Typical distribution and morphology of atopic dermatitis rash: Facial and extensor surfaces in infants and young children
Flexure lichenification in older children and adults
Minor features
Eyes
Cataracts (anterior subcapsular) Keratoconus
Infraorbital folds affected Facial pallor Palmar hyperlinearity Xerosis Pityriasis alba White dermatographism Ichthyosis Keratosis pilaris
Nonspecific dermatitis of the hands and feet Nipple eczema
Positive type I hypersensitivity skin tests Propensity for cutaneous infections Elevated serum IgE level
Food intolerance
Impaired cell-mediated immunity Erythroderma
Early age of onset
*The diagnosis of atopic dermatitis should be suspected if three major criteria and three minor criteria are present.
Question
4) 家庭收入也是影響本研究會有誤差之因素,請問家庭收入依 <5 萬,5 萬~10 萬,及 >10 萬分配之依據。Answer
根據訪查前行政院主計處的家庭收支調查,顯示台北縣平均每戶家庭收入為 4 萬~5 萬, 因此本研究以 5 萬設為一級距,將本研究之家庭收入變項區分為小於 5 萬,5 萬-10 萬 及大於 10 萬。Question
5) 城鄉差距的定義如何?是如何區分出來的,請補充在文章中。Answer
Urban area: city 都市、城市 Suburban: town 鎮、鄉 Rural area: village 村、鄰 已補充在文章 Table 1 footnot 中 在城市與鄉村的分類上,常見以都市化程度為依據,以人口密度為重要指標。依據人口 密度高且暫離率低的歸類為城市,而人口密度低且暫離率高的歸為鄉村。 城市與鄉村的差異,城市與鄉村居民的組成也會有所差異。基於城鄉組成因素、環境條 件和產業結構等差異之狀況下,造成城市聚落居民和鄉村聚落居民社經條件、社會組成 和社會網絡關係等的差異。城市與鄉村的特性、發展與課題都有所不同,台灣的城市有 明顯的現代化,並且有完善的基本設施、行政組織和金融機構等多方面的生活配備,但 是有較嚴重的社會問題,還有實質環境的問題,像是交通擁擠、住宅問題或廢棄物等問
題。反觀鄉村的發展並沒有城市來的健全,但不會擁有城市那麼多社會問題的出現,可 是鄉村有人口流失、撫養率偏高與公共設施不足等課題需要解決。
Question
6) 請加入另一個表格,將三組疫苗注射組發生異位性皮膚炎的各項變數(影響因子)的統 計結果及方法呈現出來。Answer
已將發生異位性皮膚炎的各項變數(影響因子)的統計結果及方法呈現於以下表格 After adjusting for potential confounders of infant gender, preterm birth, maternal history of atopy, maternal education and nationality, family income, place of residence, duration of breast feeding, older siblings, fungi at house wall, and ETS exposure, the effect of vaccination on AD still persists.Table3 The potential confounders for atopic dermatitis and recurrent wheezing
Atopic dermatitis N=1584 Recurrent wheezing N=1220 n (%) Crude OR (95% CI) n (%) Crude OR (95% CI) Maternal education (%)
Junior high school and below 97(6.1) 1 152(12.5) 1
Senior high school and above 1485(93.9) 0.57 (0.45-0.72)* 1067(87.5) 1.02(0.83-1.25)
Maternal nationality (%)
Taiwan 1498(94.6) 1 1102(90.3) 1
Foreign countries 86(5.4) 1.70(1.37-2.25)* 118(9.7) 1.34(1.07-1.68)
Place of residence since birth (%)
Urban area 891(56.4) 1 531(43.6) 1
Suburban 405(25.6) 1.49(1.30-1.72)* 396(32.5) 0.92(0.79-1.07) Rural area
284(18.0) 1.19(1.01-1.40)* 291(23.9) 1.18(1.02-1.39) *
Table 4 The association of atopic dermatitis and recurrent wheezing with vaccination status Atopic dermatitis N=1584 Recurrent wheezing N=1220 Vaccination status Total N=19968 n (%) Crude OR (95% CI) Adjusted ORa (95% CI) n (%) Crude OR (95% CI) Adjusted ORa (95% CI) DTP&OPV Vaccination 5717 224(14.2) 1.00 1.00 322 (26.4) 1.00 1.00 DTP-Hib&OPV Vaccination 5997 544(34.3) 1.77 (1.48-2.11)* 1.38 (1.15-1.65)* 390(32.0) 1.03 (0.88-1.20) 1.02 (0.86-1.19) DTP-Hib-IPV vaccination 8254 816(51.5) 2.01 (1.76-2.30)* 1.49 (1.29-1.72)* 508(41.6) 1.19 (0.98-1.45) 1.17 (0.96-1.43) a
Model is adjusted for infant gender, preterm birth, maternal history of atopy, maternal education and nationality, family income, place of residence, duration of breast feeding, older siblings, fungi at house wall, and ETS exposure
Question
7) 討論中均沒有提到反覆喘鳴在三組疫苗注射組並無差異性,其他的研究結果也可比 較,請補充。Answer
為何反覆喘鳴在三組疫苗注射組並無差異性,已加入其他類似研究做補充於 Discussion. 如 reference 25Interestingly, we found infants with Hib vaccination was associated with AD while compared to those without Hib vaccination. However, Hib vaccination failed to reach statistically significant association with recurrent infant wheezing. Different pathogenesis between AD
Family income per month (NT$) (%)
50,000 491(31.0) 1 448(36.8) 1
50,000~100,000 831(52.5) 0.65(0.55-0.76)* 645(52.9) 0.98(0.79-1.21) >100,000 260(16.4) 0.80(0.69-0.93)* 126(10.3) 1.21(1.00-1.48)
and wheezing might account for this finding. Another cohort study in Taiwan, with similar prevalence of wheezing, found that recurrent infant wheezing during the first 18 months of age may not be related with allergy sensitization.25 Alternatively, it was associated with the Clara cell protein 10 (CC10) G+38A polymorphism and lower CC10 levels. Further follow up of this cohort is warranted to clarify this problem.
25. Yang KD, Ou CY, Chang JC, et al. Infant frequent wheezing correlated to Clara cell protein 10 (CC10) polymorphism and concentration, but not allergy sensitization, in a perinatal cohort study. J Allergy Clin Immunol 2007;120:842-8.
Reply to Reviewer 2
Question
1. This is a well-designed and successful follow up cohort study, but the one-year follow up is too short to conclude the association between vaccination and atopic disorders.
Answer
Thank you for your suggestion. This is one of our potential limitation. The ages of the children in our study might be too young to fully evaluate the risk of atopic diseases. However, approximately 60% of AD cases arose in the first year of life.26 That 7.9% of the children in our study developed AD also suggested that the age of the children was not a major limitation. We will try to follow up this cohort and get better results in the future.
Question
2. It is also important to obtain the prevalence of atopic dermatitis and recurrent wheezing in the cohort study, and found that infants with the DPT-Hib&OPV and DPT-Hib-IPV
vaccination were significantly assocaited with AD while compared to those without Hib vaccination (DTP&OPVvaccination), but the DPT-Hib&OPV and DPT-Hib-IPV vaccinations
failed to reach statistical significance with recurrent wheezing. The infant recurrent wheezing rate was similar to that reported by another cohort study done in Taiwan (J Allergy Clin Immunol 120:842-8, 2007), in which the recurrent infant wheezing was not significantly associated with allergy sensitization. The authors may be able to discuss the results derived from these 2 cohort studies done in Taiwan, and make a better interpretation on why infants with the DPT-Hib&OPV and DPT-Hib-IPV vaccination were significantly assocaited with AD while compared to those without Hib vaccination (DTP&OPVvaccination), but the DPT-Hib&OPV and DPT-Hib-IPV vaccinations failed to reach statistical significance with recurrent wheezing.
Answer
Thank you for your suggestion. We have discussed the results derived from these 2 cohort studies done in Taiwan. We have made a better interpretation and have added this study in our reference. (See page 12 last paragraph and reference 25)
Interestingly, we found infants with Hib vaccination was associated with AD while compared to those without Hib vaccination. However, Hib vaccination failed to reach statistically significant association with recurrent infant wheezing. Different pathogenesis between AD and wheezing might account for this finding. Another cohort study in Taiwan, with similar prevalence of wheezing, found that recurrent infant wheezing during the first 18 months of age may not be related with allergy sensitization.25 Alternatively, it was associated with the Clara cell protein 10 (CC10) G+38A polymorphism and lower CC10 levels. Further follow up of this cohort is warranted to clarify this problem.
25. Yang KD, Ou CY, Chang JC, et al. Infant frequent wheezing correlated to Clara cell protein 10 (CC10) polymorphism and concentration, but not allergy sensitization, in a perinatal cohort study. J Allergy Clin Immunol 2007;120:842-8.
Question
3. This cohort has been followed up for at least 5 years, if the authors could show some data regarding the atopic rates in 3 years of age, they may be able to provide a better correlation between vaccination and atopic disorder, for repeated infant wheezing disorders in 18 months
old are not significantly linked to atopic diseases.
Answer
It‟s a very good suggestion. However, the data regarding the atopic rates in 3 years of age is not available now. We have tried our best to analyze the data we have.
1 2 3 4 5 6 7 8 9 10 11 12 13 14 15 16 17 18 19 20 21 22 23 24 25 26 27 28 29 30 31 32 33 34 35 36 37 38 39 40 41 42 43 44 45 46 47 48 49 50 51 52 53 54 55 56 57 58 59 60 61 62 63 64 65
Haemophilus influenzae type b combination vaccines
and atopic disorders: a prospective cohort study
I-Jen Wang,1,2,3 Li-Min Huang,4 Yueliang Leon Guo,5 Wu-Shiun Hsieh,4 Tien-Jen Lin,6 Pau-Chung Chen7
1
Department of Pediatrics, Taipei Hospital, Department of Health, Taipei, Taiwan;
2
College of Public Health, China Medical University, Taichung, Taiwan;
3
College of Medicine, Fu Jen Catholic University, Taipei, Taiwan;
4
Department of Pediatrics, National Taiwan University Hospital, Taipei, Taiwan;
5
Department of Environmental and Occupational Medicine, National Taiwan University Hospital, Taipei, Taiwan;
6
Taipei Medical University, Wan Fang Hospital, Taipei, Taiwan;
7
Institute of Occupational Medicine and Industrial Hygiene, National Taiwan University College of Public Health, Taipei, Taiwan
Running title: Hib combination vaccines and atopic disorders Word count: 2589
Correspondence to: Professor Pau-Chung Chen
Institute of Occupational Medicine and Industrial Hygiene, National Taiwan University College of Public Health
Room 733, #17 Syujhou Road, Taipei 10055, Taiwan Phone: +886-2-3322 8088
Fax: +886-2-2358 2402 Email:[email protected]
1 2 3 4 5 6 7 8 9 10 11 12 13 14 15 16 17 18 19 20 21 22 23 24 25 26 27 28 29 30 31 32 33 34 35 36 37 38 39 40 41 42 43 44 45 46 47 48 49 50 51 52 53 54 55 56 57 58 59 60 61 62 63 64 65
Abstract
Background/Purpose: Epidemiologic evidence for an association between
vaccinations and atopy development is inconsistent. We evaluated the influence of Haemophilus influenzae type b (Hib) combination vaccines in 6 month old infants on the prevalence of atopic disorders in 18 month old children.
Methods: We used multistage, stratified systematic sampling to recruit 24,200
mother-newborn pairs from the Taiwan national birth registration in 2005. Vaccination status was ascertained through official vaccine cards, while risk factors for atopic disorders were gathered by questionnaires at 6 months of age. Information about development of atopic dermatitis (AD) and recurrent wheezing was collected at 18 months of age. The relationship between atopic disorders and Hib combination vaccines, diphtheria-pertussis-tetanus-Hib and oral poliomyelitis vaccines
(DPT-Hib&OPV) and DPT-Hib-inactivated poliomyelitis vaccines (DPT-Hib-IPV), were estimated by multiple logistic regression.
Results: A total of 19,968 children completed the follow-up and participated in the
study. AD was noted in 1584 (7.9%) infants while recurrent wheezing was found in 1,220 (6.1%). The adjusted ORs (95% CI) for the development of AD in the
DPT-Hib&OPV and DPT-Hib-IPV vaccination groups were given as 1.38 (1.15-1.65) and 1.49 (1.29-1.72), compared to those without Hib vaccination (DTP&OPV
vaccination). However, the association between DPT-Hib&OPV and DPT-Hib-IPV vaccinations and recurrent wheezing failed to reach statistical significance.
Conclusion: There is a potential risk for AD after receiving Hib combination vaccines. Whether the trivial adverse impact to increased risk of atopic disorders outweighs the Hib vaccination importance in public health for infectious diseases spreading warrants further investigation.
1 2 3 4 5 6 7 8 9 10 11 12 13 14 15 16 17 18 19 20 21 22 23 24 25 26 27 28 29 30 31 32 33 34 35 36 37 38 39 40 41 42 43 44 45 46 47 48 49 50 51 52 53 54 55 56 57 58 59 60 61 62 63 64 65
Key words: atopic dermatitis, recurrent wheezing, Haemophilus influenzae type b,
1 2 3 4 5 6 7 8 9 10 11 12 13 14 15 16 17 18 19 20 21 22 23 24 25 26 27 28 29 30 31 32 33 34 35 36 37 38 39 40 41 42 43 44 45 46 47 48 49 50 51 52 53 54 55 56 57 58 59 60 61 62 63 64 65
Introduction
The prevalence of atopic diseases has increased considerably over the past decades.1 The hygiene hypothesis has emerged, linking reduced microbial exposure and infections early in life with the development of allergic diseases.2 Early childhood immunizations have been viewed as promoters of atopic disease development by stimulating a Th2-type immune response or decreasing microbial pressure, which shifts the balance between Th1 and Th2 immunity.3 Because serious infectious diseases have been almost eradicated in some populations, whether the possible adverse effects of vaccinations may take precedence over their preventive action should be paid more attention. Since vaccination is universally recommended for infants, any association between childhood vaccinations and the occurrence of a common serious condition such as allergic diseases could be of considerable public health importance.
The possible effects of Bacillus Calmette-Gue´rin (BCG), oral poliomyelitis (OPV), measles-mumps-rubella vaccination (MMR), and diphtheria-tetanus-pertussis (DTP) vaccinations on atopic disease have been studied.4-7 Neonatal BCG vaccination was reported to be associated with a significantly lower prevalence of wheeze and asthma.4 A study in U.K. indicated a slight increase in AD risk at 12 years of age in those who had received the DTP vaccine.6 Furthermore, a Danish population-based cross-sectional study demonstrated an almost two fold increase in AD risk in children after receiving MMR vaccine.7 However, no conclusive data on the relationship of Haemophilus influenzae type b (Hib) vaccines and Hib combination vaccines with atopic disorders are yet available because they were introduced recently to most vaccination programs.8-10 The studies suffered from some drawbacks such as information bias, selection bias, medical care utilization bias, and reverse causation
1 2 3 4 5 6 7 8 9 10 11 12 13 14 15 16 17 18 19 20 21 22 23 24 25 26 27 28 29 30 31 32 33 34 35 36 37 38 39 40 41 42 43 44 45 46 47 48 49 50 51 52 53 54 55 56 57 58 59 60 61 62 63 64 65
because of cross sectional design. One study even showed a mixed Th1–Th2 response after the Hib vaccination of 19 adults.11 Biological plausibility for a causal
relationship is not apparent. Therefore, more evidence concerning Hib vaccination as a potential risk factor for atopic disorders is necessary. In this study, we investigated the risk of atopic dermatitis and recurrent wheezing after receiving Hib combination vaccines.
1 2 3 4 5 6 7 8 9 10 11 12 13 14 15 16 17 18 19 20 21 22 23 24 25 26 27 28 29 30 31 32 33 34 35 36 37 38 39 40 41 42 43 44 45 46 47 48 49 50 51 52 53 54 55 56 57 58 59 60 61 62 63 64 65
Methods
Childhood Vaccinations in Taiwan
The Hib vaccine was first introduced into Taiwan in 1997. Although the
government authorities encourage Hib vaccinations, this vaccine has remained “at one's own expense” until now. During the time of this study, infants in their first 6 months might receive Hib vaccination either as a combined DTP-Hib vaccination and oral poliomyelitis vaccination (DPT-Hib&OPV, so called four combination vaccine) given simultaneously or a combined DPT-Hib-inactivated poliomyelitis vaccination (DPT-Hib-IPV, so called five combination vaccine) as a single injection at 2, 4, and 6 months of age. Other vaccinations that are injected before 6 months of age are
DTP&OPV, BCG, and hepatitis B vaccines (HBV), and MMR mass vaccinations in
National Immunization Program. In Taiwan, each vaccination is recorded in the child‟s health card, which has to be examined before primary school entry. Therefore, parents are required to maintain accurate health cards of their children. After
vaccination, nurses update the child‟s health card kept by parents and register this information in the government computerized immunization system. Since the computerized immunization tracking system depends on the reporting of each
vaccination by the infant welfare center, we could not rule out that vaccinations were incompletely reported. Therefore, we ascertained vaccination status in the first 6 months of life by reviewing the child‟s health card during a home interview by trained interviewers.
Study Population and Sampling Strategy
The Taiwan Birth Cohort Study is a prospective longitudinal cohort study. In the study, we used a multistage stratified systematic sampling design to obtain
1 2 3 4 5 6 7 8 9 10 11 12 13 14 15 16 17 18 19 20 21 22 23 24 25 26 27 28 29 30 31 32 33 34 35 36 37 38 39 40 41 42 43 44 45 46 47 48 49 50 51 52 53 54 55 56 57 58 59 60 61 62 63 64 65
categorized a total of 369 towns in Taiwan into 12 strata according to the
administrative division (four strata) and the total fertility rate (three strata). Using the principle of probability proportional to size, we randomly sampled 90 out of 369 towns in Taiwan. A total of 24,200 pairs of parents and newborns from these 90 towns were recruited. All study participants signed informed consent as approved by the Institutional Review Board of the National Taiwan University Hospital.
Data Collection and Case Definition
We conducted a home interview with the postpartum parents at 6 and 18 months after the delivery using a structured questionnaire as previously described.12,13 Cases of AD were defined as physician-diagnosed AD through the questions „Has your child ever had AD diagnosed by a doctor?‟, and „Has your child ever had recurrent itchy rash for at least 4 consecutive half-months periods over elbows, knees, face, wrists, or generalized (4 or more localizations)?‟12-14Children whose mothers reported that the child ever had wheezing in the chest more than 3 episodes were classified as having recurrent wheezing.15 Questions about potential confounders and prenatal and postnatal risk factors were asked at 6 months of age, including maternal age and education, family income, maternal history of atopy, maternal smoking during
pregnancy, diet and supplements during pregnancy, duration of breast feeding, age of introduction of solid foods, number of siblings, day care, pet raising, carpets at home, environmental tobacco smoke (ETS), fungi on the house wall, and place of residence. From the records of the collaborating hospitals, we collected neonate health data at birth, such as gender, head circumference, birth body weight, height, weeks of gestation, parity, and type of delivery.
Statistical Analysis
1 2 3 4 5 6 7 8 9 10 11 12 13 14 15 16 17 18 19 20 21 22 23 24 25 26 27 28 29 30 31 32 33 34 35 36 37 38 39 40 41 42 43 44 45 46 47 48 49 50 51 52 53 54 55 56 57 58 59 60 61 62 63 64 65
standing for no Hib vaccination and DPT-Hib&OPV or DPT-Hib-IPV vaccination standing for receiving Hib vaccination, with the DTP&OPV vaccination used as the reference category. For the association between vaccination status with atopic
disorders, odds ratios (ORs) with 95% confidence intervals (95% CIs) were calculated by logistic regression models. Analyses were performed in both univariate and
multivariate models. Potential confounders, including infant gender, preterm birth, birth weight, maternal age and history of atopy, maternal education and nationality, maternal smoking during pregnancy, family income, duration of breast feeding, day care, number of older siblings, pet raising, fungi at house wall, carpets at home, postnatal ETS exposure, MMR and Japanese B encephalitis (JBE) vaccinations, and place of residence were taken into consideration. Variables were included in the model if they changed the univariate point estimate by at least 10%. All hypothesis testing was two-sided at the significance level of 0.05 and was performed using SAS Software Version 8.2.
1 2 3 4 5 6 7 8 9 10 11 12 13 14 15 16 17 18 19 20 21 22 23 24 25 26 27 28 29 30 31 32 33 34 35 36 37 38 39 40 41 42 43 44 45 46 47 48 49 50 51 52 53 54 55 56 57 58 59 60 61 62 63 64 65
Results
We excluded those with loss follow-up and incomplete questionnaires, multiple gestation (twins, triplets, etc), inability to answer questions, plan to move out of the area before delivery, children with immunodeficiency, structural airway abnormalities, congenital defects, and history of severe vaccination allergy. At 18 months of age, 20,172 (83.4%) children completed the follow-up. Since almost all children received DTP, OPV, BCG, or HBV mass vaccinations in National Immunization Program, we excluded those without these vaccinations. We also restricted our analyses to infants at risk for a first episode of AD or recurrent wheezing after 6 months of age to
exclude potential reverse causation between vaccinations and atopic disorders. Finally, 19,968 (99.0%) children were included in this study (Figure 1). There were no
significant difference of the characteristics between the 204 non-participants and the 19,968 participants, including maternal age, maternal history of atopy, birth weight, gestational age, gender, and parity.
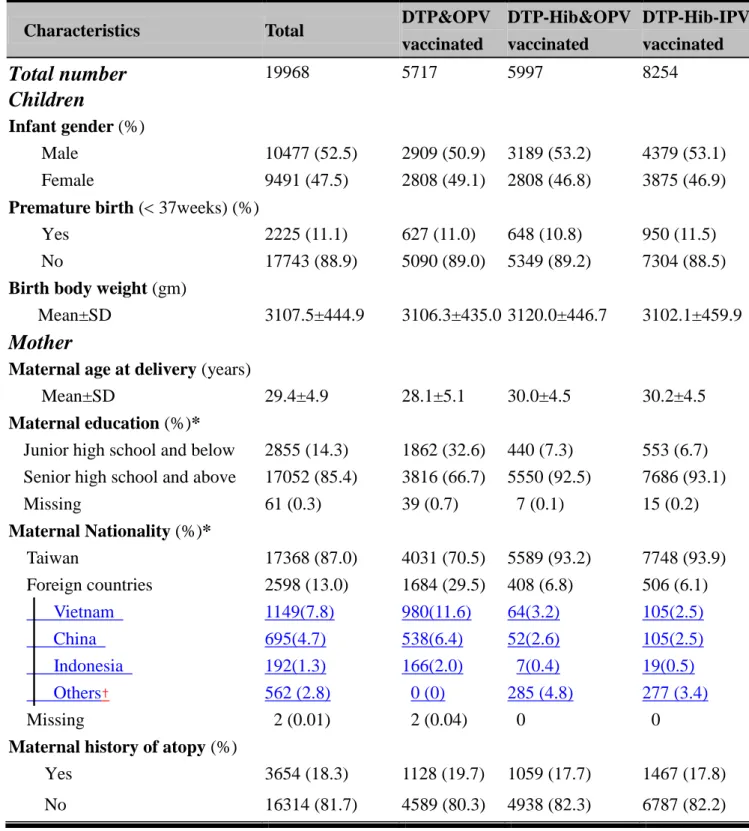
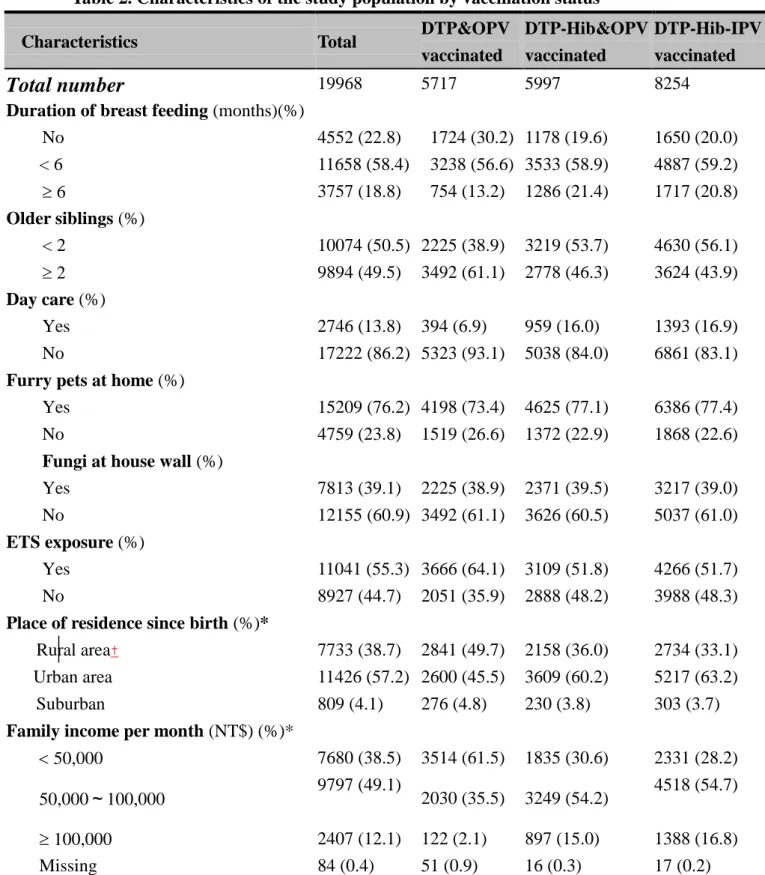
The demographic characteristics of children, mother, and environmental factors were displayed in Table 1 and Table 2. There was no significant difference among the three vaccination groups with the exception of maternal education, maternal
nationality, family income, and place of residence. Children with higher maternal education, mothers of Taiwan nationality, higher family income, and living in urban areas received more Hib combination vaccines.
During the study period, a diagnosis of AD was made in 1584 (7.9%) out of 19,968 children while recurrent wheezing was found in 1220 (6.1%) children. By the age of 6 months, 5997 (30.0%) of the infants received DPT-Hib&OPV vaccination while 8254 (41.3%) of the infants received DPT-Hib-IPV vaccination. Table 3 showed odds ratios (ORs) with 95% confidence intervals (95% CI) for the relationships between
1 2 3 4 5 6 7 8 9 10 11 12 13 14 15 16 17 18 19 20 21 22 23 24 25 26 27 28 29 30 31 32 33 34 35 36 37 38 39 40 41 42 43 44 45 46 47 48 49 50 51 52 53 54 55 56 57 58 59 60 61 62 63 64 65
vaccination status and atopic disorders. In the multivariate analysis, the adjusted ORs (95% CI) for the development of AD in the DPT-Hib&OPV and DPT-Hib-IPV vaccination groups were given as 1.38 (1.15-1.65) and 1.49 (1.29-1.72), compared to those without Hib vaccination (DTP&OPV vaccination). However, the association between DPT-Hib&OPV and DPT-Hib-IPV vaccinations and recurrent wheezing failed to reach statistical significance.
1 2 3 4 5 6 7 8 9 10 11 12 13 14 15 16 17 18 19 20 21 22 23 24 25 26 27 28 29 30 31 32 33 34 35 36 37 38 39 40 41 42 43 44 45 46 47 48 49 50 51 52 53 54 55 56 57 58 59 60 61 62 63 64 65
Discussion
Compared with DTP and OPV vaccines, few studies have evaluated whether Hib vaccination has any effect on atopic disorders and the results have been inconsistent. In this cohort study, we found a weak association between Hib combiantion vaccines and AD, compared to those without Hib vaccination. A survey of 1,943
schoolchildren aged 5-14 years in Eastern Germany also found a positive association between Hib vaccination and asthma (OR, 1.86; 95% CI, 1.05-3.32).8 On the contrary, Kummeling et al. discovered that the risk of eczema or recurrent wheeze at 1 year of age did not differ between infants with different vaccination status at the age of 6 months.10 However, infant eczema and recurrent wheezing at such young age may be fairly unspecific for atopy. Bernsen et al estimated the risk of atopic disorders at ages 8–12 years to be 1.09 (95% CI: 0.75-1.58) following Hib vaccination in the first year of life in Netherlands.9 He claimed that the result might be underestimated due to selection bias and nondifferential misclassification in this cross-sectional study. Many factors could interfere with the effect of Hib vaccination and atopy such as age and ethnicity of study population, validation of vaccination status, the vaccination schedule, and the number of inoculations.3 Furthermore, various brands of vaccines that differed in the number of antigens, protein carriers and the type of adjuvants might also account for the discrepant findings of these studies.
There are theoretical reasons to suspect a correlation of atopic disorders with Hib vaccination. One possible mechanism is that vaccination may shift the immunologic balance toward a Th2-type immune response.3,16An IgE response to vaccine antigens is frequently detected in the sera of children after primary vaccination.17 After booster vaccination, more than 90% of children have detectable IgE against the vaccine antigens.18 Moreover, the IgE response to vaccine antigens seems to be more
1 2 3 4 5 6 7 8 9 10 11 12 13 14 15 16 17 18 19 20 21 22 23 24 25 26 27 28 29 30 31 32 33 34 35 36 37 38 39 40 41 42 43 44 45 46 47 48 49 50 51 52 53 54 55 56 57 58 59 60 61 62 63 64 65
prominent among atopic individuals.17,19Another possibility is that vaccines or their adjuvants may have direct IgE-potentiating effects.20 Hib vaccine comes with adjuvants such as aluminum salts and oil-based emulsions to enhance antibody production. The elevated humoral response induced by aluminum salts is associated with a predominant Th2-type immune response.20 Trace amounts of streptomycin, neomycin, and polymyxin B in the vaccine may also trigger allergic reactions.20 On the other side, modern subunit vaccines may not activate dendritic cells efficiently and may impair regulation of the adaptive immune response since they often lack
microbial antigens such as lipopolysaccharide, heat shock proteins and the CpG motif of bacterial DNA.21,22 Hib vaccine is an inactivated vaccine and is unlikely to mimic a natural infection-mediated immune response that protects against the development of allergic diseases. Furthermore, infants require multiple Hib immunizations because of immature T cell-dependent antibody responses. CD4 T cell responses are usually slower to develop, less readily sustained, and more easily biased towards a Th2-type response.23 In fetal life, the immune system is skewed toward TH2-type immunity, but after birth, it becomes progressively skewed toward TH1-type responses, which are crucial for a host defense against infections.24 When infants encounter with
environmental allergens or receive many inactivated vaccines early in life, the normal progression from TH2- to TH1-type immunity after birth might be disturbed and favors detoured to the Th2-skewed pathway.24
Interestingly, we found infants with Hib vaccination was associated with AD while compared to those without Hib vaccination. However, Hib vaccination failed to reach statistically significant association with recurrent infant wheezing. Different
pathogenesis between AD and wheezing might account for this finding. Another cohort study in Taiwan, with similar prevalence of wheezing, found that recurrent
1 2 3 4 5 6 7 8 9 10 11 12 13 14 15 16 17 18 19 20 21 22 23 24 25 26 27 28 29 30 31 32 33 34 35 36 37 38 39 40 41 42 43 44 45 46 47 48 49 50 51 52 53 54 55 56 57 58 59 60 61 62 63 64 65
infant wheezing during the first 18 months of age may not be related with allergy sensitization.25 Alternatively, it was associated with the Clara cell protein 10 (CC10) G+38A polymorphism and lower CC10 levels.25 Further follow up of this cohort is warranted to clarify this problem.
Our study population was a homogeneous group and all adhered to the same religious group. Therefore, the main reason for not receiving Hib combination vaccines in our study was that the vaccination had not yet been introduced into the National Vaccination Program and it was not free. This implied that probably “family income” was an important confounder. As shown in Table 1, children with higher family income, mothers of Taiwan nationality, higher maternal education, and living in urban areas received more Hib combination vaccines. These variables were taken into consideration in the statistical analyses and were included in the final model if they changed the univariate point estimate by at least 10%. However, the statistical significance of the association between Hib vaccine and AD was retained even after adjusting for the potential confounders. In addition, medical care utilization bias did not influence our results because more than 99% of participants were covered by national health insurance in Taiwan, suggesting that bias from differential access to medical care was not possible.
Motives to abstain from vaccinations, such as infant‟s illness or fear of side effects such as allergies, might lead to the reverse causation of vaccination effects. Children with severe allergy to vaccine components or immunodeficiency failed to receive some vaccinations, however, they were excluded from our study subjects.
Furthermore, “infant‟s illness” was often a reason for delayed vaccination but not for refusal to vaccination. Children were usually brought to immunizations by their mothers. Therefore, “fear of side effects such as allergies” would only be the case if
1 2 3 4 5 6 7 8 9 10 11 12 13 14 15 16 17 18 19 20 21 22 23 24 25 26 27 28 29 30 31 32 33 34 35 36 37 38 39 40 41 42 43 44 45 46 47 48 49 50 51 52 53 54 55 56 57 58 59 60 61 62 63 64 65
fear of side effects was related to an increased risk of atopic disorders by a maternal history of atopic diseases. Remes et al. reported that allergic manifestations in parents may affect the vaccination rate of children.26 However, maternal history of atopic diseases. It had been included as a potential confounder in our statistical analyses. Furthermore, if measurement error did occur, it tended to be toward the null and the effect of vaccination was likely to be underestimated.
One of the potential limitations in our study is the relatively short follow-up. The ages of the children in our study might be too young to fully evaluate the risk of atopic diseases. However, approximately 60% of AD cases arose in the first year of life.27 That 7.9% of the children in our study developed AD also suggested that the age of the children was not a major limitation. Furthermore, our study was limited by the use of questionnaire for ascertaining AD, which might not be accurate as the standard diagnostic criteria by a dermatologist.28 Nevertheless, maternal report of doctor-diagnosed visible eczema with typical morphology and atopic distribution has been previously validated versus clinical examination in the studies performed in the United States and Denmark and has been used by many epidemiological studies.12-14, 29, 30
The strengths of our study included the large sample size and the population based prospective cohort design, with relatively short intervals between subsequent
follow-up questionnaires, which decreased the possibility of recall bias. Because of the large sample size, we were able to control for numerous potential confounders by the statistical analysis. Therefore, we are fairly confident about our results. The multistage stratified systematic sampling including urban, suburban, and rural population could enhance generality. In addition, we used the official child‟s health card to confirm the vaccination status of each child, which increased the validity of
1 2 3 4 5 6 7 8 9 10 11 12 13 14 15 16 17 18 19 20 21 22 23 24 25 26 27 28 29 30 31 32 33 34 35 36 37 38 39 40 41 42 43 44 45 46 47 48 49 50 51 52 53 54 55 56 57 58 59 60 61 62 63 64 65
the results and decreased misclassification. We compared a subset of the health cards to the information contained in medical charts and found that the data was totally in agreement with medical charts. Therefore, we were confident about the validity of the vaccination status. Since the follow-up rate was high, selection bias could not be a major problem in our study. Moreover, the prevalence of most variables in those lost in the follow-up and in those completed the followed-up was not significantly different from each other.
In conclusion, we found there is a minimal risk for AD after receiving Hib combination vaccines. Just as Guillan-Barré syndrome and the influenza vaccine, whether the trivial adverse impact to increased risk of atopic disorders outweighs the Hib vaccination importance in public health for infectious diseases spreading warrants further investigation.
1 2 3 4 5 6 7 8 9 10 11 12 13 14 15 16 17 18 19 20 21 22 23 24 25 26 27 28 29 30 31 32 33 34 35 36 37 38 39 40 41 42 43 44 45 46 47 48 49 50 51 52 53 54 55 56 57 58 59 60 61 62 63 64 65
Acknowledgement: Funding for this study was provided by the grants from the
Bureau of Health Promotion, Department of Health (DOH94-HP-1802, DOH95-HP-1802 and DOH96-HP-1702), and the National Science Council (NSC 97-2314-B-192 -001 -MY2) of Taiwan. All the authors have declared that they have no conflict of interest. We appreciate the support and statistical assistance from Professor Tung-Liang Chiang, Institute of Health Policy and Management, National Taiwan University College of Public Health, Taipei, Taiwan; Professor Shio-Jean Lin, Department of Pediatrics, National Cheng Kung University Hospital and College of Medicine, National Cheng Kung University, Tainan, Taiwan; and Professor Yi-Li Chuang, Population and Health Research Center, Bureau of Health Promotion, Department of Health, Taichung, Taiwan.
1 2 3 4 5 6 7 8 9 10 11 12 13 14 15 16 17 18 19 20 21 22 23 24 25 26 27 28 29 30 31 32 33 34 35 36 37 38 39 40 41 42 43 44 45 46 47 48 49 50 51 52 53 54 55 56 57 58 59 60 61 62 63 64 65
References
1. Masoli M, Fabian D, Holt S, Beasley R. The global burden of asthma: executive summary of the GINA Dissemination Committee Report. Allergy
2004;59:469-78.
2. Romagnani S. The increased prevalence of allergy and the hygiene hypothesis: missing immune deviation, reduced immune suppression, or both? Immunology 2004;112:352-63.
3. McDonald KL, Huq SI, Lix LM, Becker AB, Kozyrskyj AL. Delay in diphtheria, pertussis, tetanus vaccination is associated with a reduced risk of childhood asthma. J Allergy Clin Immunol 2008;121:626-31.
4. Linehan MF, Frank TL, Hazell ML Francis HC, Morris JA, Baxter DN, Niven RM: Is the prevalence of wheeze in children altered by neonatal BCG
vaccination? J Allergy Clin Immunol 2007;119:1079–085.
5. Nakajima K, Dharmage SC, Carlin JB Wharton CL, Jenkins MA, Giles GG, Abramson MJ, Haydn Walters E, Hopper JL: Is childhood immunisation
associated with atopic disease from age 7 to 32 years? Thorax 2007; 62:270-75. 6. Farooqi IS, Hopkin JM. Early childhood infection and atopic disorder: Thorax
1998; 53:927–32.
7. Olesen AB, Juul S, Thestrup-Pedersen K: Atopic dermatitis increased following vaccination for measles, mumps, and infection. Acta Derm Venereol 2003; 83:445–50.
8. Laubereau B, Grote V, Holscher G, et al. Vaccination against influenzae type b and atopy in East German schoolchildren. Eur J Med Res 2002;7:387–92. 9. Bernsen RM, Koes BW, de Jongste JC, van der Wouden JC. Haemophilus
1 2 3 4 5 6 7 8 9 10 11 12 13 14 15 16 17 18 19 20 21 22 23 24 25 26 27 28 29 30 31 32 33 34 35 36 37 38 39 40 41 42 43 44 45 46 47 48 49 50 51 52 53 54 55 56 57 58 59 60 61 62 63 64 65
children. Pediatr Pulmonol 2006;41:463-9.
10. Kummeling I, Thijs C, Stelma F, Huber M, van den Brandt PA, Dagnelie PC. Diphtheria, pertussis, poliomyelitis, tetanus, and Haemophilus influenzae type b vaccinations and risk of eczema and recurrent wheeze in the first year of life: the KOALA Birth Cohort Study. Pediatrics 2007;119:e367-73.
11. Kamboj KK, King CL, Greenspan NS, Kirchner HL, Schreiber JR. Immunization with Haemophilus influenzae type b-CRM(197) conjugate vaccine elicits a mixed Th1 and Th2 CD(4+) T cell cytokine response that correlates with the isotype of antipolysaccharide antibody. J Infect Dis 2001;184:931–5.
12. Wang IJ, Guo YL, Wen HJ, et al. Environmental risk factors for early infantile atopic dermatitis. Pediatric Allergy Immunol 2007;18; 441-7.
13. Moore MM, Rifas-Shiman SL, Rich-Edwards JW, et al. Perinatal predictors of atopic dermatitis occurring in the first six months of life. Pediatrics
2004;113:468-74.
14. Benn CS, Wohlfahrt J, Aaby P, et al. Breastfeeding and risk of atopic dermatitis, by parental history of allergy, during the first 18 months of life. Am J Epidemiol 2004;160:217-23.
15. Castro-Rodriguez JA, Rodrigo GJ. Efficacy of inhaled corticosteroids in infants and preschoolers with recurrent wheezing and asthma: a systematic review with meta-analysis. Pediatrics 2009;123:e519-25.
16. Ryan M, Murphy G, Ryan E, et al. Distinct T-cell subtypes induced with whole cell and acellular pertussis vaccines in children. Immunology 1998;93:1–10. 17. Dannemann A, van Ree R, Kulig M Bergmann RL, Bauer P, Forster J,
Guggenmoos-Holzmann I, Aalberse RC, Wahn U: Specific IgE and IgG4 immune responses to tetanus and diphtheria toxoid in atopic and nonatopic children during
1 2 3 4 5 6 7 8 9 10 11 12 13 14 15 16 17 18 19 20 21 22 23 24 25 26 27 28 29 30 31 32 33 34 35 36 37 38 39 40 41 42 43 44 45 46 47 48 49 50 51 52 53 54 55 56 57 58 59 60 61 62 63 64 65
the first two years of life. Int Arch Allergy Immunol 1996;111:262–67.
18. Mark A, Björkstén B, Granström M: Immunoglobulin E responses to diphtheria and tetanus toxoids after booster with aluminium-adsorbed and fluid DT-vaccines.
Vaccine 1995;13:669–73.
19. Nilsson L, Grüber C, Granström M Björkstén B, Kjellman NI: Pertussis IgE and atopic disease. Allergy 1998;53:1195–201.
20. Nossal GJ. Host immunobiology and vaccine development. Lancet 1997;350 :1316–319.
21. Wendling U, Paul L, van der Zee R, Prakken B, Singh M, van Eden W: A conserved mycobacterial heat shock protein (hsp) 70 sequence prevents adjuvant arthritis upon nasal administration and induces IL-10-producing T cells that cross-react with the mammalian selfhsp70 homologue. J Immunol
2000;164 :2711–717.
22. Prakken BJ, Wendling U, van der Zee R, Rutten VP, Kuis W, van Eden W: Induction of IL-10 and inhibition of experimental arthritis are specific features of microbial heat shock proteins that are absent for other evolutionarily conserved immunodominant proteins. J Immunol 2001;167 :4147–153.
23. Wilson CB, Kollmann TR: Induction of antigen-specific immunity in human neonates and infants. Nestle Nutr Workshop Ser Pediatr Program 2008;61:183-95. 24. Björkstén B: Perinatal events in relation to sensitization in the human. Am J
Respir Crit Care Med 2000;162:S105-07.
25. Yang KD, Ou CY, Chang JC, et al. Infant frequent wheezing correlated to Clara cell protein 10 (CC10) polymorphism and concentration, but not allergy
sensitization, in a perinatal cohort study. J Allergy Clin Immunol 2007;120:842-8.
1 2 3 4 5 6 7 8 9 10 11 12 13 14 15 16 17 18 19 20 21 22 23 24 25 26 27 28 29 30 31 32 33 34 35 36 37 38 39 40 41 42 43 44 45 46 47 48 49 50 51 52 53 54 55 56 57 58 59 60 61 62 63 64 65
exposure in infancy decreases the subsequent risk of frequent wheeze but not of atopy. J Allergy Clin Immunol 2001;108:509-15.
27. Charman C, Williams HC. Epidemiology. In: Bieber T, Leung DYM, eds. Atopic dermatitis. 1st ed. New York: Marcel Dekker Inc 2002:21-2.
28. Hanifin JM, Rajka G. Diagnostic features of atopic eczema. Acta Dermatol
Venereol 1980;92:44-7.
29.Laughter D, Istvan JA, Tofte SJ, Hanifin JM. The prevalence of atopic dermatitis in Oregon schoolchildren. J Am Acad Dermatol 2000;43:649-55.
30. Purvis DJ, Thompson JM, Clark PM, et al.Risk factors for atopic dermatitis in New Zealand children at 3.5 years of age. Br J Dermatol 2005;152:742-9.