J
OURNAL OFC
LINICALM
ICROBIOLOGY, Apr. 2005, p. 1600–1603
Vol. 43, No. 4
0095-1137/05/$08.00
⫹0 doi:10.1128/JCM.43.4.1600–1603.2005
Copyright © 2005, American Society for Microbiology. All Rights Reserved.
Colonization of Human Immunodeficiency Virus-Infected Outpatients
in Taiwan with Candida Species
Chien-Ching Hung,
1Yun-Liang Yang,
2Tsai-Ling Lauderdale,
3L. Clifford McDonald,
3Chin-Fu Hsiao,
4Hsiao-Hsu Cheng,
3Yong An Ho,
3and Hsiu-Jung Lo
3*
Division of Infectious Diseases, Department of Internal Medicine, National Taiwan University Hospital,
and Department of Parasitology, National Taiwan University College of Medicine,
Taipei,
1Department of Biological Science and Technology, National Chiao
Tung University, Hsinchu,
2and Division of Clinical Research
3and
Division of Biostatistics and Bioinformatics,
4National Health
Research Institutes, Zhunan Town, Miaoli County,
Taiwan, Republic of China
Received 26 September 2004/Returned for modification 25 October 2004/Accepted 22 November 2004
To understand the Candida colonization of human immunodeficiency virus (HIV)-infected outpatients in
Taiwan, we have conducted a prospective cohort study of Candida colonization and its risk factors at the
National Taiwan University Hospital from 1999 to 2002. More than 50% of the patients were colonized with
Candida species, and 12% developed symptomatic candidiasis. Patients colonized with fluconazole-resistant
strains of Candida species had a higher prevalence of candidiasis than those colonized with susceptible strains.
Our analysis found that antibiotic treatment and lower CD4
ⴙcounts (<200 cells/mm
3) increased the rate of
oropharyngeal candidiasis in HIV-infected patients, while antiretroviral therapy protected patients from the
development of candidiasis.
Mucosal candidiasis, including oropharyngeal, esophageal,
and vaginal candidiasis, is common among human
immunode-ficiency virus (HIV)-infected patients (4, 11). In particular,
oropharyngeal candidiasis occurs in up to 90% of patients
during the course of HIV infection (17). Progressive
cell-mediated immunodeficiency, with CD4
⫹lymphocyte counts
less than 200 cells/mm
3, is a risk factor for colonization with
Candida species and the development of candidiasis (3). The
widespread use of azole antifungal agents for the treatment of
mucosal candidiasis results in colonization with less susceptible
organisms and the development of resistance (4, 15). Thus,
oropharyngeal candidiasis due to drug-resistant fungi is an
emerging problem for patients infected with HIV (18).
The overall prevalence of known HIV infection in Taiwan
remains relatively low (0.01%) (9). As in most other
industri-alized countries, the majority of HIV-infected patients in
Tai-wan receive care in the outpatient setting. Therefore, to better
understand the epidemiology of Candida species carriage
among HIV-infected outpatients in Taiwan, we undertook a
study to determine the prevalence of oropharyngeal
coloniza-tion. Our objectives were to assess the colonization status and
the risk factors for colonization and the development of
can-didiasis in HIV-infected outpatients in Taiwan. The
suscepti-bilities of those Candida isolates to antifungal drugs were also
determined.
MATERIALS AND METHODS
Study population and data collection.HIV-infected patients were monitored regularly in the outpatient infectious diseases clinic of National Taiwan Univer-sity Hospital, a major referral hospital for the management of HIV-related complications. The patients were enrolled after they provided informed verbal consent. This was a prospective study performed by the use of three surveys, conducted from May to June 1999, May to September 2001, and January to April 2002. A standardized data collection form was used to retrieve demographic information, the most recent CD4⫹lymphocyte count, and the highly active antiretroviral therapy (HAART) prescribed. In addition, clinical information for the previous 3 months was obtained and included information on whether the patient had a history of oral or esophageal candidiasis or hospitalization and the antibacterial and antifungal drugs received.
Sampling and microbiologic processing.Oropharyngeal swab specimens for culture were obtained from all patients by using a dry sponge swab (EZ Cul-turette; Becton Dickinson, Sparks, Md.). All swabs were maintained at room temperature and were transported to the laboratory within 24 h. They were then plated on solid medium within 12 h of arrival. The swabs collected in 1999 were plated on Sabouraud dextrose with chloramphenicol and gentamicin (BBL), and those collected in 2001 and 2002 were plated on Chromagar Candida (BBL). All plates were incubated at 30°C. Three independent colonies were selected from each positive culture. Additional colonies were selected from cultures with more than one morphotype. All isolates were first subjected to the germ tube assay. For germ tube assay-positive isolates, a temperature sensitivity assay was per-formed to differentiate Candida albicans from Candida dubliniensis (growth
* Corresponding author. Mailing address: Division of Clinical
Re-search, National Health Research Institutes, 35 Keyan Rd., Zhunan
Town, Miaoli County, 350, Taiwan, Republic of China. Phone:
886-2-2652-4095. Fax: 886-2-2789-0254. E-mail: [email protected].
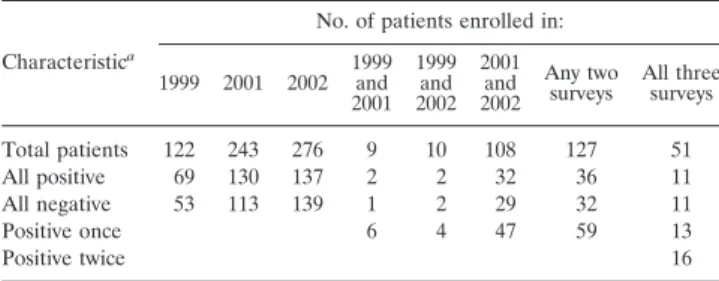
TABLE 1. Numbers of patients in three surveys
Characteristica
No. of patients enrolled in: 1999 2001 2002 1999 and 2001 1999 and 2002 2001 and 2002 Any two
surveys All threesurveys Total patients 122 243 276 9 10 108 127 51
All positive 69 130 137 2 2 32 36 11
All negative 53 113 139 1 2 29 32 11
Positive once 6 4 47 59 13
Positive twice 16
aPositive, positive for yeast by culture; negative, negative for yeast by culture.
1600
defect at 42°C). The VITEK yeast biochemical card (YBC; bioMerieux, St. Louis, Mo.) was used to identify those isolates that failed to form germ tubes and isolates that formed germ tubes but that failed to grow at 42°C. We used the API 32C system (bioMerieux) to assess our results when the VITEK YBC yielded results of less than 90% certainty.
Antifungal susceptibility testing.The MICs of antifungal drugs were deter-mined by in vitro antifungal susceptibility testing according to the M27-A guide-lines published in 1997 by the National Committee of Clinical Laboratory Stan-dards (NCCLS) (10). RPMI 1640 medium (31800-022; Gibco BRL) was used for dilution and growth of the yeast culture. The growth end point of each isolate was determined with a spectrophotometer (Spectra MAX Plus; Molecular Devices Corp., Sunnyvale, Calif.). The MICs were also interpreted according to NCCLS guidelines. The amphotericin B MIC was determined, as the MIC of amphoter-icin B is needed to completely inhibit the growth of isolates after 48 h of incubation at 35°C. Isolates for which the amphotericin B MIC wasⱖ2 g/ml were considered amphotericin B resistant.
The fluconazole MIC was defined as the concentration of fluconazole needed to reduce the turbidity to 50% after 48 h of incubation at 35°C. Isolates for which fluconazole MICs wereⱖ64 g/ml, 16 to 32 g/ml, and <8 g/ml were defined as resistant, susceptible-dose dependent, and susceptible to fluconazole, respec-tively.
Statistical analysis.All clinical laboratory data were entered into a relational database designed in Access 97 software (Microsoft, Redland, Wash.). The chi-square test was used to study the association of factors with incident or persistent oral yeast species colonization. Risk factors for patients with oropha-ryngeal colonization were identified by multiple logistic regression.
RESULTS
Patients.
A total of 122, 243, and 276 patients were enrolled
in this study in 1999, 2001, and 2002, respectively (Table 1).
The majority (91%) of the patients were men. The CD4
⫹counts were available for 599 patients, and the average CD4
⫹count was 279.5 cells/mm
3. Only 15.3% of the patients had
CD4
⫹counts greater than 500 cells/mm
3, while 43.9% of the
patients had CD4
⫹counts less than 200 cells/mm
3and 13% of
the patients had CD4
⫹counts less than 50 cells/mm
3.
Conse-quently, 84.4% of the patients were receiving HAART. A total
of 35.3% of patients also received antibiotics as treatment or
primary or secondary prophylaxis for opportunistic infections.
A total of 127 patients were enrolled in two of the three
surveys. Of these, 32 were negative for yeasts by culture, 36
were positive for yeasts in both surveys, and 59 were positive
for yeasts by culture only once. Of 51 patients who were
en-rolled in all three surveys, 11 patients were negative for yeasts
by culture and 11 patients were positive for yeasts by culture in
all three surveys. Of the remaining 29 patients, 13 patients
were positive for yeasts by culture once and 16 patients were
positive for yeasts by culture twice.
Distribution of yeasts.
Yeast culture positivity rates in 1999,
2001, and 2002 were 56.6% (69 of 122 patients), 53.5% (130 of
243 patients), and 49.6% (137 of 276 patients), respectively.
One isolate of each Candida species from each patient in each
survey was analyzed (Table 2). C. albicans was the most
com-mon species and accounted for 91, 86, and 85.2% of the
iso-lates in 1999, 2001, and 2002, respectively. A total of 338
isolates were recovered; and these consisted of 293 (86.7%) C.
albicans isolates, 10 (3%) Candida glabrata isolates, 10 (3%)
Candida parapsilosis isolates, 7 (2.1%) Candida tropicalis
iso-lates, 5 (1.5%) Candida lusitaniae isoiso-lates, and 13 (3.7%) other
isolates. Four, nine, and nine different Candida species were
isolated from patients in the 1999, 2001, and 2002 surveys,
respectively.
Antifungal susceptibilities of yeasts.
The susceptibilities to
antifungal agents of one Candida species isolate among
mul-tiple isolates collected from each patient were analyzed (Table
2). Of 262 isolates, the amphotericin B MICs for 12 (4.6%),
188 (71.8%), 61 (23.3%), and 1 (0.4%) isolates were <0.25,
0.5, 1, and 2
g/ml, respectively. The only resistant isolate was
a Candida famata isolate. A total of 244 (93.1%), 12 (4.6%),
and 6 (2.3%) isolates were susceptible, susceptible-dose
de-pendent, and resistant to fluconazole, respectively (Table 3).
Of six fluconazole-resistant isolates, five were C. albicans. The
prevalence of candidiasis was higher among patients colonized
with fluconazole-resistant Candida species than among those
colonized with fluconazole-susceptible isolates (P
⬍ 0.05).
On the basis of multivariate analysis, antibiotic treatment
and lower CD4
⫹counts (
⬍200 cells/mm
3) were independent
risk factors for oropharyngeal colonization among the patients.
In contrast, treatment with HAART and antifungal drugs
de-creased the odds of oropharyngeal colonization. There were 83
episodes of candidiasis among 641 patients within the 3 months
prior to the oropharyngeal swab specimen culture, and 12.3%
of the patients had received antifungal therapy during that
period. On the basis of the multivariate analysis, antibiotic
treatment and lower CD4
⫹counts (
⬍200 cells/mm
3) were also
independent risk factors for the development of oropharyngeal
TABLE 2. Distribution of Candida species
Species
No. of isolates collected No. of isolates tested 1999 2001 2002 Total 1999 2001 2002 Total
Candida albicans
61
111
121
293
61
91
66
218
Candida glabrata
5
5
10
5
5
10
Candida parapsilosis
3
3
4
10
3
3
4
10
Candida tropicalis
4
3
7
4
3
7
Candida lusitaniae
1
4
5
1
4
5
Candida famata
2
1
3
2
1
3
Candida guilliermondii
1
2
3
1
2
3
Candida sake
2
2
2
2
Others
3
2
5
3
1
4
Total
67
129
142
338
67
109
86
262
TABLE 3. Susceptibilities of the Candida species to fluconazole
Yr
No. (%) of isolates for which fluconazole MIC (g/ml) was:
0.125 0.25 0.5 1 2 4 8 16–32 ⱖ64 Total
1999
13 (19.4)
38 (56.7)
3 (4.4)
2 (3)
4 (6)
2 (3)
2 (3)
2 (3)
1 (1.5)
67
2001
6 (5.5)
39 (35.8)
26 (23.8)
12 (11)
9 (8.2)
4 (3.7)
7 (6.4)
3 (2.8)
3 (2.8)
109
2002
4 (4.7)
26 (30.2)
16 (18.6)
17 (19.8)
2 (2.3)
6 (7)
6 (7)
7 (8.1)
2 (2.3)
86
Total
23 (8.8)
103 (39.3)
45 (17.2)
31 (11.8)
15 (5.7)
12 (4.6)
15 (5.7)
12 (4.6)
6 (2.3)
262
candidiasis among the patients (Table 4). In contrast, the odds
of oropharyngeal candidiasis decreased 5.2-fold for
HIV-infected patients receiving antiretroviral therapy.
DISCUSSION
In this study 52.4% of HIV-infected outpatients were
colo-nized with yeasts. This rate is slightly lower than those found in
previous surveys (i.e., 60 to 63%) (1, 11). Symptomatic oral
candidiasis has been reported to occur in 7 to 48% of
HIV-infected patients and in 43 to 93% of patients with progressive
immunodeficiency (8, 16). In the present study, 12.9% of
HIV-infected patients had developed candidiasis within the 3
months before the surveys.
Fluconazole is widely used for the treatment of mucosal
candidiasis, resulting in colonization with less susceptible
or-ganisms and the development of resistance among usually
sus-ceptible species, such as C. albicans (4, 15). Candida krusei was
isolated once in the present study. Surprisingly, the fluconazole
MIC for this species was 0.25
g/ml, even though C. krusei is
considered less susceptible to fluconazole than other species
(12). Another interesting result was the finding that all five C.
lusitaniae isolates were susceptible to amphotericin B, even
though C. lusitaniae has been reported to be relatively resistant
to amphotericin B (6). The overall resistance rates to
ampho-tericin B and fluconazole were 0.4 and 2.3%, respectively,
which are lower than those indicated in previous reports from
Taiwan (7, 19).
Oral colonization with yeasts is known to be significantly
higher among HIV-infected patients than healthy individuals
(11). In addition to a reduction in the HIV load and
restora-tion of the immune system, antiretroviral therapy may have a
more intrinsic role in the elimination of Candida species in
HIV-infected patients (2). Thus, the frequency of
oropharyn-geal candidiasis decreased with antiretroviral therapy in the
present study, as well as in previous studies (2, 5). Our findings
of a significantly increased risk of oropharyngeal colonization
and candidiasis in HIV-infected patients with progressive
im-munodeficiency (CD4
⫹count less than 200 cells/mm
3) is
con-sistent with the findings described in previous reports (3, 11).
In a previous report by Ohmit et al. (11), antibiotic treatment
was associated with incident or persistent oral Candida species
colonization but not oropharyngeal candidiasis. In contrast, we
found that antibiotic treatment was associated not only with
oropharyngeal colonization but also with candidiasis. The
dif-ference between these two studies may lie in the populations
studied.
Systemic candidemia is recognized as an important, albeit
uncommon, cause of mortality (14). Up to 47% of
HIV-in-fected patients with candidemia may succumb to their infection
(13). In contrast, mucosal candidiasis does not contribute to
morbidity or a significant reduction in quality of life but,
rather, contributes to increased medical costs for the treatment
of HIV infection. We therefore recommend that HIV-infected
patients who are receiving antibiotics and who have CD4
⫹counts below 200 cells/mm
3be carefully monitored for
candi-diasis.
ACKNOWLEDGMENTS
We thank Bristol-Myers Squibb and Pfizer for supplying the pure
powders of amphotericin B and fluconazole, respectively.
REFERENCES
1. Campisi, G., G. Pizzo, M. E. Milici, S. Mancuso, and V. Margiotta. 2002. Candidal carriage in the oral cavity of human immunodeficiency virus-in-fected subjects. Oral Surg. Oral Med. Oral Pathol. Oral Radiol. Endodont.
93:281–286.
2. Dios, P. D., A. Ocampo, C. Miralles, J. Limeres, and I. Tomas. 2000. Chang-ing prevalence of human immunodeficiency virus-associated oral lesions. Oral Surg. Oral Med. Oral Pathol. Oral Radiol. Endodont. 90:403–404. 3. Feigal, D. W., M. H. Katz, D. Greenspan, J. Westenhouse, W. Winkelstein,
Jr., W. Lang, M. Samuel, S. P. Buchbinder, N. A. Hessol, and A. R. Lifson.
1991. The prevalence of oral lesions in HIV-infected homosexual and bisex-ual men: three San Francisco epidemiological cohorts. AIDS 5:519–525. 4. Fichtenbaum, C. J., S. Koletar, C. Yiannoutsos, F. Holland, J. Pottage, S. E.
Cohn, A. Walawander, P. Frame, J. Feinberg, M. Saag, C. Van der Horst, and W. G. Powderly. 2000. Refractory mucosal candidiasis in advanced human immunodeficiency virus infection. Clin. Infect. Dis. 30:749–756. 5. Gottfredsson, M., G. M. Cox, O. S. Indridason, G. M. de Almeida, A. E.
Heald, and J. R. Perfect. 1999. Association of plasma levels of human immunodeficiency virus type 1 RNA and oropharyngeal Candida coloniza-tion. J. Infect. Dis. 180:534–537.
6. Hadfield, T. L., M. B. Smith, R. E. Winn, M. G. Rinaldi, and C. Guerra. 1987. Mycoses caused by Candida lusitaniae. Rev. Infect. Dis. 9:1006–1012. 7. Hsueh, P. R., M. L. Chen, C. C. Sun, W. H. Chen, H. J. Pan, L. S. Yang, S. C.
Chang, S. W. Ho, C. Y. Lee, W. C. Hsieh, and K. T. Luh.2002. Antimicrobial drug resistance in pathogens causing nosocomial infections at a university hospital in Taiwan, 1981-1999. Emerg. Infect. Dis. 8:63–68.
8. Lupetti, A., G. Guzzi, A. Paladini, K. Swart, M. Campa, and S. Senesi. 1995. Molecular typing of Candida albicans in oral candidiasis: karyotype epide-miology with human immunodeficiency virus-seropositive patients in com-parison with that with healthy carriers. J. Clin. Microbiol. 33:1238–1242. 9. McDonald, L. C., T. L. Lauderdale, H. J. Lo, J. J. Tsai, and C. C. Hung. 2003.
Colonization of HIV-infected outpatients in Taiwan with methicillin-resis-tant and methicillin-susceptible Staphylococcus aureus. Int. J. STD AIDS
14:473–477.
10. National Committee for Clinical Laboratory Standards. 1997. Reference method for broth dilution antifungal susceptibility testing of yeasts; approved standard. M27-A. National Committee for Clinical Laboratory Standards, Wayne, Pa.
11. Ohmit, S. E., J. D. Sobel, P. Schuman, A. Duerr, K. Mayer, A. Rompalo, and
R. S. Klein.2003. Longitudinal study of mucosal Candida species coloniza-tion and candidiasis among human immunodeficiency virus (HIV)-seropos-itive and at-risk HIV-seronegative women. J. Infect. Dis. 188:118–127. 12. Orozco, A. S., L. M. Higginbotham, C. A. Hitchcock, T. Parkinson, D.
Falconer, A. S. Ibrahim, M. A. Ghannoum, and S. G. Filler.1998. Mecha-nism of fluconazole resistance in Candida krusei. Antimicrob. Agents Che-mother. 42:2645–2649.
13. Pappas, P. G., J. H. Rex, J. Lee, R. J. Hamill, R. A. Larsen, W. Powderly,
C. A. Kauffman, N. Hyslop, J. E. Mangino, S. Chapman, H. W. Horowitz, J. E. Edwards, and W. E. Dismukes.2003. A prospective observational study of candidemia: epidemiology, therapy, and influences on mortality in hospi-talized adult and pediatric patients. Clin. Infect. Dis. 37:634–643. 14. Patel, R., D. Portela, A. D. Badley, W. S. Harmsen, J. J. Larson-Keller, D. M.
Ilstrup, M. R. Keating, R. H. Wiesner, R. A. Krom, and C. V. Paya.1996. Risk factors of invasive Candida and non-Candida fungal infections after liver transplantation. Transplantation 62:926–934.
15. Perea, S., J. L. Lopez-Ribot, W. R. Kirkpatrick, R. K. McAtee, R. A.
Santil-lan, M. Martinez, D. Calabrese, D. Sanglard, and T. F. Patterson.2001.
TABLE 4. Multiple regression for candidiasis versus noncandidiasis
Risk factor Factor value Odds ratio 95% Confidence limit P value
Antiretroviral therapy
False vs true
5.249
1.815, 15.18
0.0022
Antifungal received
False vs true
0.023
0.009, 0.058
⬍0.0001
Antibiotics received
False vs true
0.254
0.086, 0.745
0.0125
CD4 counts
0–199 vs
ⱖ200
6.095
2.038, 18.229
0.0012
Prevalence of molecular mechanisms of resistance to azole antifungal agents in Candida albicans strains displaying high-level fluconazole resistance iso-lated from human immunodeficiency virus-infected patients. Antimicrob. Agents Chemother. 45:2676–2684.
16. Powderly, W. G., K. Robinson, and E. J. Keath. 1992. Molecular typing of
Candida albicans isolated from oral lesions of HIV-infected individuals.
AIDS 6:81–84.
17. Samaranayake, L. P. 1992. Oral mycoses in HIV infection. Oral Surg. Oral Med. Oral Pathol. 73:171–180.
18. Vanden Bossche, H., P. Marichal, and F. C. Odds. 1994. Molecular mech-anisms of drug resistance in fungi. Trends Microbiol. 2:393–400. 19. Yang, Y. L., H. H. Cheng, Y. A. Ho, C. F. Hsiao, and H. J. Lo. 2003.
Fluconazole resistance rate of Candida species from different regions and hospital types in Taiwan. J. Microbiol. Immunol. Infect. 36:187–191.