八 十 九 年 度 計 劃 執 行 進 度 報 告
複雜性先天心臟病術前術後心律不整之電生理學機轉:以同步電位及立體
結構定位法研究(1/3)
Car diac Ar r hythmias in Patients with Complex Congenital Hear t Disease
Befor e and After Sur gical Palliations
計劃編號:NSC98-2314-B002-037
主持人:吳美環
國立台灣大學醫學院小兒科
Fir st year : Car diac Rhythm Distur bances in Complex Congenital Hear t Disease Rhythm distur bances in patients with left atr ial isomer ism
ABSTRACT
Objectives. To determine the prevalence and the electrophysiological mechanisms of rhythm disturbances in patients with left atrial isomerism (LAI).
Background. Defective sinus node and atrioventricular conduction tissue have been described in the hearts associated with LAI.
Methods. From 1984 to 1998, a total of 22 patients, and from 1995 to 1998, 3 fetuses, were identified as LAI and constituted the study population. Pathological confirmation was
obtained in 14 patients and 1 fetus.
Results. The age at the last follow-up ranged from 2 to 276 months (90± 70 months). Three fetuses (100%) developed sinus bradycardia and intermittent AV block, and were ended with
heart failure and termination. Associated cardiovascular anomalies of the 22 pediatric
patients were interruption of inferior vena cava (18, 82%), common atrium (9, 41%), AV
canal (14, 64%), double-outlet right ventricle (8, 36%) and pulmonary stenosis (15, 68%).
Over half of the patients (14, 64%) developed bradyarrhythmia (onset age, 1 to 264 months,
median 78 months): junctional escape rhythm as dominant rhythm, 10 (45%), sinus
bradycardia or sinoatrial block, 8 (35%, 5 of the 7 also had dominant junctional rhythm) and
AV block, 2 (9%, both had dominant junctional rhythm). By actuarial analysis, the
probability free from bradyarrhythmia decreased with age and was 80% and 46% at the age of
2 and 6 years, respectively. Two patients experienced fainting attacks. However, junctional
ectopic tachycardia after the cardiac operation occurred in 3 out of 10 patients.
Electrophysiological studies (3 cases) revealed sinus node dysfunction in 2/2 and impaired
AV conduction in 1/2. Besides, a Mahaim-like pathway (progressive shortening of HV
interval during decremental atrial pacing) was identified in both of the patients with His
Conclusions. Over half of the LAI patients may develop bradyarrhythmia at the age of 6 years mainly due to the subnormal sinus node function. Bradyarrhythmia appeared during the fetal
stage may cause preferential loss of the fetuses. Patients with LAI also have a higher chance
to have junctional tachycardia which may be related to the abnormal AV conduction
properties. The high prevalence of Mahaim-like pathway warrants further investigation.
Keyword: left atrial isomerism, heterotaxy syndrome, sinus bradycardia, junctional rhythm,
Left atrial isomerism (LAI), a form of heterotaxy syndrome, is characterized by
the bilateral left atrial morphology of the atria as well as the interruption of inferior vena cava
with azygous continuation (1,2). Intracradiac anomalies may be present, but the severity is
usually less severe than those found in patients with right atrial isomerism (1-4). Associated
intracardiac anomalies usually include partial anomalous pulmonary venous return, common
atrium, atrioventricular (AV) canal, double-outlet right ventricle and pulmonary stenosis,
although the incidence of double-outlet right ventricle and pulmonary stenosis was much
lower than that found in right atrial isomerism. As to the conduction system, the sinus node
has been described as defective, hypoplasic or even absent (5,6). The AV nodes may be
single or paired, but is frequently associated with a discontinuity between the AV node and
the ventricular conduction tissues. Such conduction system may result in sinus node
dysfunction or AV block (7). Atrioventricular block had been shown in 15 % of patients
and nodal rhythm in 12% of the patients with LAI (7). Since most of the patients are
associated with complex congenital heart disease, the long-term prognosis was deemed as
determined by the associated cardiac anomalies and only rarely permanent pacemaker was
implanted. However, the recent advances in surgical or transcatheter palliations for complex
cardiac lesions have improved the long-term outcome. Therefore, it becomes feasible and
mandatory to define more clearly the clinical significance of such defective conduction
system in LAI patients during the long-term follow-up. This longitudinal study on 22 LAI
pediatric patients and 3 LAI fetuses sought to determine the prevalence and the
electrophysiological mechanism of the rhythm disturbances in LAI patients.
METHODS
diagnosed to have heterotaxy syndrome at this institution. From January 1995 to December
1998, by fetal echocardiography 28 fetuses were found to have heterotaxy syndrome.
Among them, 22 pediatric patients (8 male and 14 female) and 3 fetuses were LAI and
constituted the study population. The diagnosis of LAI was based on a combination of
echocardiography, cardiac catheterization/angiography and available magnetic resonance
imaging or computerized tomography (8-11). For fetus study, the diagnosis was obtained by
fetal echocardiography. Open heart surgery in 14 pediatric patients and autopsy in 1 fetus
confirmed the diagnosis. Patients with LAI have 1) bilateral finger-like atrial appendages, 2)
bilateral hyparterial bronchi, or 3) interruption of inferior vena cava with azygous
continuation and with the cross section of azygous vein posterior to the descending aorta at
the level of T10. The diagnosis of rhythm disturbances was based on the serial 12-lead
electrocardiogram. The rhythm found during awake time and persisted in the next follow-up
EKG was defined as dominant rhythm. The diagnosis of cardiac rhythm in fetuses was
based on the fetal echocardiography.
Statistics
Data were expressed as mean± SD. Actuarial event-free curves were drawn according to the
nonparametric estimation by Kaplan and Meier (12). Chi-square test was used to examine
the significance when appropriate.
RESULTS
Demographics
Three fetuses were all ended with termination before the 26 gestation weeks. Common atrium,
complete AV canal and interruption of inferior vena cava with azygous continuation were
months (90± 70 months. median 59 months). The associated cardiac anomalies were
summarized in Table 1. Interruption of the inferior vena cava was found in most of the
patients. The association of AV canal and common atrium was also high. One patient was
found to have no significant intracardiac anomalies. The actuarial analysis of survival of the
patients revealed a ten-year survival of 70% (Fig. 1). Palliative interventions had been
performed in 17 patients (Table 2). The palliations were performed to increase the
pulmonary flow in 7, to repair the septal defect in 4, and to reach a Fontan type circulation in
6.
Rhythm disturbances
All three fetuses developed sinus bradycardia and intermittent AV block before the 26 weeks'
gestation. Hydrops fetalis developed in 2 cases. Sinus rhythm either from the right-sided LA
or left-sided LA was noted in 14 patients at initial presentation, and 6 patients had low atrial
rhythm. During the follow-up, over half of the patients (14/22, 64%) developed
bradyarrhythmia. Junctional escape rhythm as dominant rhythm (varied from 46 to 89/min,
62± 13/min, median 60/min), in 10 (45%), sinus bradycardia or sinoatrial block, in 8 (35%, 5
of the 7 also had dominant junctional escape rhythm) and AV block in, 2 (9%, both had
dominant junctional rhythm). The onset age of the bradyarrhythmia ranged from 1 month to
264 months (75±85 months, median 78 months). By actuarial analysis, the probability being
free from bardyarrhythmias was 80% and 46% at the age of 2 and 6 years, respectively (Fig.
2). However, only two patients experienced fainting attacks. None of the patients had
bradyarrhythmia directly related morbidity and mortality. None had received permanent
pacemaker implantation.
Three patients developed junctional ectopic tachycardia after open heart surgery, and one of
electrophysiological study. One of them had sinus pause detected during Holtor monitoring,
and none of the patients before the development of junctional ectopic tachycardia had
junctional escape rhythm as the dominant rhythm. The juctional ectopic tachycardia varied
with a heart rate from 120 to 215/min and was associated with unstable hemodynamics. The
tachycardia didn't respond to verapamil, digoxin, proprnolol or cardioversion, and was
converted to sinus or low atrial rhythm only after hemodynamics improved by
cardiopulmonary resuscitation in two. Adenosine had been used in one patient and might
temporarily slowed down the rate of tachycardia. One patient had right heart failure after
total cavopulmonary connection operation. He suddenly developed junctional ectopic
tachycardia (maximal rate 215/min) 4 months after the operation. His condition deteriorated
and died on the same day. As compared to the other 7 patients who had also received
intracardiac surgery but without postoperative junctional ectopic tachycardia, we found that
the none of the clinical characteristics, including gender, age at operation, pre-existing rhythm
and ventricular morphology, was associated with a higher risk of developing junctional
ectopic tachycardia after interventions.
Electrophysiological study
Electrophysiological study was performed in 3 under propofol anesthesia, but the study was
limited by the development of junctional ectopic tachycardia with unstable hemodynamics in
one case during rapid atrial pacing. The electrophysiological parameters are summarized in
the Table 3. Alternating rhythm from right or left sided left atria was found in 2 and
junctional rhythm in one. The sinus node function was abnormal in both patients in whom it
had been examined: prolonged maximal corrected sinus recovery time in one and a slow
intrinsic heart rate in the other. The sinus node recovery curve (assessed by Narula method)
node entrance block. The Wenckebach cycle length (the atrial pacing cycle length with loss
of 1:1 AV conduction above the His bundle) of the AV conduction was longer than the
normal age control in one. Whereas in the other patient, the atrium failed to maintain the heart
rate at the pacing cycle length of 300 ms, and therefore limited the study of AV node. By
decremental atrial pacing, we found that, in both patients who had clearly recorded His
potential, the His potential was moved to the ventricular activation at shorter pacing cycle
length (Fig. 3) or even merged into the ventricular activation (Fig.4). The relation between
atrial pacing cycle length and HV interval showed progressively shortened HV interval along
with lengthening of the AH interval during decremental atrial pacing (Fig. 5). But, changes
of the QRS morphology was only evident in one case. Such behavior of AV conduction
suggested the presence of Mahaim-like accessory pathways. However, no tachycardia nor
echo beats were induced. It is possible that the antegrade AV conduction was through AV
node as well as a direct extension from AV node (or His bundle) to fascicular or ventricular
tissue. Since we did not map the discrete potential and the insertion of the accessory
pathway, we preferred to use the term “Mahaim-like fiber” to indicate the behavior of
progressive shortening of the HV interval during decremental atrial pacing. The degree of
QRS changes would depend on the closeness between the location of normal AV node
conduction axis and the Mahaim-like fibers.
DISCUSSION
Although the pathological description of defective conduction system in LAI patients had
been described as early as 1975, the long-term clinical significance remains unclear. This
longitudinal study of 22 LAI patients and 3 fetuses have delineated the high probability of
were the propensity to have junctional ectopic tachycardia and the high incidence of
Mahaim-like accessory pathways in LAI patients.
Natural History of the Bradyarrhythmia in LAI Patients
Previous reports suggest an incidence of bradyarrhythmias ranged from 20 to 30% in LAI
patients (7, 13,14). In this study, the incidence of bradyarrhythmias was as high as 64%.
By event free analysis, the probability free from bradyarrhythmia decreased with age and over
half of the patients would experience bradyarrhythmia when they reached the age of 6 years.
In the series reported by Wren et al (6), bradyarrhythmia at initial presentation was noted in
27% of the patients and by Holtor monitoring in 64% (9/14) of the patients. Since we have
performed serial EKG in most of the patients, the incidence of bradyarrhythmia found at our
study would be more close to that defined by Holtor. The sinus node in LAI patients is
usually abnormal (5,6). As described by Dickinson et al (6), although a sinus node can be
identified on the junction of the right-sided or left-sided atrial appendage with the atrium in
about half of the patients, the sinus node was abnormally small in all. In about one-fourth of
their patients, no sinus node could be identified. The report from Ho et al has disclosed absent
sinus node in three-forth of their patients (5). Such pathological evidences may account for
the high probability of sinus node dysfunction in LAI patients. Furthermore, the function of
the hypoplastic sinus node may deteriorate with time and thereby the probability being free
from bradyarrhythmias in these patients will decrease with age. The sinus node dysfunction in
LAI patients as shown in this study might be present as dominant junctional escape rhythm,
low intrinsic heart rate, prolonged sinus recovery time and sinoatrial entrance block. In the
previous report by Wren et al (7), a significant portion (12%) of LAI patients similarly
developed nodal rhythm. The incidence of nodal rhythm was even higher as shown by
shown in 2 out of the 14 patients receiving Holtor monitoring. As to the AV nodes, four
patterns could be summarized from the previous pathological reports: 1) one AV node with
preserved connection to atrial transitional cells but lost connection to nonbranch or right
bundle, 2) one AV node with normal connection, 3) two AV nodes connected by a sling of
conduction tissue (Monckeberg sling) which descends into the bundle branches, and 4) two
AV nodes lost connection to the sling (5,6). Such varied AV conduction system may result
in a variety of AV conduction disturbances. Previous reports had emphasized the high
incidence of AV block in LAI patients and none of the reports mentioned the occurrences of
tachycardia. The incidence of AV block ranged from 7 to 30% (7, 13,14). The AV block (3
with first-degree, 2 with second-degree and 5 with complete) was demonstrated in 10 out of
67 patients in the report by Wren et al. (7). Garcia et al (13) found complete AV block in 6
out of 30 patients and Rougin et al (14) reported complete AV block in 3 out of 11 cases.
Complete AV block during the fetal life may cause hydrops fetalis and fetal loss (15). In
this report, we have only 2 cases (9%) of AV block and both also had dominant junctional
rhythm. All fetuses developed bradycardia which had been characterized as sinus bradycardia
with intermittent AV block. Based on these observations, we suggest that the
bradyarrhythmias found in LAI patients are mainly due to abnormal sinus node function and
in some cases the abnormal sinus node may be associated with compromised AV conduction.
When the sinus rate is low, the junctional rhythm will appear. However, when the sinus rate
is relatively high, then AV block may appear because the compromised AV conduction is
unmasked at a higher sinus rate.
Tachyarrhythmia in LAI Patients
In this study we have also noticed a propensity (30%) to develop junctional ectopic
postoperative junctional ectopic tachycardia after Fontan type operation, the incidence was
significantly higher (16). Among the 151 patients reported by Friedman et al, 12 patients
(8%) was found to have junctional ectopic tachycardia after the Fontan type operation (16).
Although we have identified the Mahaim-like accessory pathway in these patients, the
tachycardia was not reentrant tachycardia between the accessory pathway and the AV node.
The responses to pacing and drugs suggested an automaticity for the mechanism of
tachycardia. The pathological basis for the Mahaim pathway in normal hearts has been
described as anatomical connections of the AV node to the myocardial septum as well as
connections of the origin of the left bundle branch to the upper part of the interventricular
septum (17). However, the results of nonpharmocological therapy for such preexcitation, e.g.,
radiofrequency ablation or surgical ablation, had suggested that such preexcitation originates
from remnants of the specialized AV ring tissue (18,19). The Mahaim pathways may be
further classified as atriofascicular, nodofascicular or fasciculoventricular pathway based on
the detailed electrophysiological mapping (18). Nonetheless, the anatomic basis for the
nodofascicular and fasciculoventricular pathways is still ill-defined. Furthermore, such
criteria may be not applicable in the presence of associated complex congenital heart disease.
Therefore, based on the findings of progressive shortening of the HV interval during
decremental atrial pacing in the two cases we studied, we could only reach the diagnosis of
Mahaim-like accessory pathways for such abnormal AV conduction. Progressive QRS
changes which depends on the closeness between distal insertion sites of the normal and
accessory pathway were only found in one case. In one case, tachycardia with VA
dissociation developed during rapid atrial pacing study. This junctional tachycardia with a
same QRS morphology of the sinus rhythm was associated with a changing heart rate and was
junctional ectopic tachycardia after cardiac operation. Therefore, in LAI patients although the
abnormal Mahaim-like accessory pathway may potentially serve as reentrant route for
tachycardia, the probability of developing junctional ectopic tachycardia from the abnormal
AV conduction tissue is also high as suggested by the results of this study. In contrast,
although the pathology of right atrial isomerism shared some similarities with LAI in the
presence of AV canal, the presence of such Mahaim-like pathways was not found in RAI
patients (20,21). In stead, RAI patients were prone to develop reentrant tachycardia between
the paired AV nodes (20,21). The influence of situs laterality on the development of cardiac
conduction system was suspected but not defined yet. According to the ring theory for the
development of cardiac conduction system, the sinoatrial ring tissue contributes to the
development of sinus node and transitional cells around the AV node (22,23). As to the
atrioventricular ring, it gives rise to AV nodes and an extension of the conduction bundle
through the inlet septum. We suspect that the bilateral left-sidedness of the atrium may be
associated with an abnormal evolution of the sinoatrial and atrioventricular ring tissues which
results in abnormal sinus node, transitional cells, AV node as well as the extension from the
AV node. In another words, the abnormal AV conduction tissue in LAI may not only have
abnormal connection to the ventricular tissue but also be defective in the regulation of
automaticity. By adrenergic stimulation caused by stress, the AV node will be abnormally
speeded up in rate and lead to junctional ectopic tachycardia. However, these speculations
need to be verified. Previous report had mentioned an evolution of junctional ectopic
tachycardia into complete AV block and the histological findings from patients with
junctional ectopic tachycardia showed His bundle degeneration, Purkinje cell like tumor and
fibroelastosis (23,24). Therefore, it is highly possible that on going pathological changes
conduction as well as junctional ectopic tachycardia. In conclusion, this study defines the
high probability of developing bradyarrhythmias in LAI patients due to abnormal sinus node
function during the long-term follow-up. Varied AV conduction abnormalities may include
compromised AV conduction, junctional ectopic tachycardia after intervention as well as the
association of Mahaim-like accessory pathway. These rhythm disturbances may change the
REFERENCES
1. Van Praagh SV, Santini F, Sanders SP. Cardiac malpositions with special emphasis on
visceral heterotaxy (asplenia and polysplenia syndromes). In: Fyler DC, ed. Nadas' Pediatric
Cardiology. Philadelphia: Hanley & Belfus, Inc., 1992:258-608.
2. Macartney FJ, Tynan M, Smallhorn JF, Huhta JC, Deanfield JE, Anderson RH. Clinical
recognition of atrial isomerism. In: Anderson RH, Marcartney FJ, Shinebourne EA, Tynan M,
eds. Pediatric Cardiology. Vol 5. Edinburgh: Churchill Livingstone, 1883:205-14.
3. Macartney FJ, Zuberbuhler JR, Anderson RH. Morphological considerations pertaining
to recognition of atrial isomerism: consequences for sequential chamber localization. Br Heart
J 1980;44:657-67.
4. De Tommasi SM, Daliento L, Ho SY, Macartney FJ, Anderson RH. Analysis of
atrioventricular junction, ventricular mass, and ventriculoarterial junction in 43 specimens
with atrial isomerism. Br Heart J 1981;45:236-47.
5. Ho SY, Fagg N, Anderson RH, Cook A, Allan L. Disposition of the atrioventricular
conduction tissues in the heart with isomerism of the atrial appendages: its relation to
congenital complete heart block. J Am Coll Cardiol 1992;20:904-10.
6. Dickinson DF, Wilkinson JL, Anderson KR, Smith A, Ho SY, Anderson RH. The cardiac
conduction system in situs ambiguus. Circulation 1979;5:879-85.
7. Wren C, Macartney FJ, Deanfield JE. Cardiac rhythm in atrial isomerism. Am J Cardiol
1987;59:1156-8.
8. Huhta JC, Smallhorn JF, Macartney FJ. Two-dimensional echocardiographic diagnosis of
situs. Br Heart J 1982;48:97-108.
9. Freedom RM, Culham JAG, Moes CAF. Asplenia and polysplenia. In: Freedom RM,
Publishing Co., 1984;643-54.
10. Wang JK, Li YW, Chiu IS, et al. Usefulness of magnetic resonance imaging in the
assessment of venoatrial connection, atrial morphology, bronchial situs, and other anomalies
in right atrial isomerism. Am J Cardiol 1994;74:701-4.
11. Chen SJ, Li YW, Wang JK, et al. Usefulness of electron beam computed tomography in
children with heterotaxy syndrome. Am J Cardiol 1998;81:188-94.
12. Kaplan EL, Meier P: Nonparametric estimation from in complete observation. J Am
Statist Assci 1982;53:457-481.
13. Garcia OL, Mehta AV, Pickoff AS et al. Left isomerism and complete atrioventricular
Block: a report of six cases. Am J Cardiol 1981;48:1103-7.
14. Roguin N, Pelled B, Freundlich E, Yahalom M, Riss E. Atrioventricular block in situs
ambiguus and left isomerism (polysplenia syndrome). PACE 1984;7:18-22.
15. Phoon CK, Villegas MD, Ursell PC, Silverman NH. Left atrial isomerism detected in
fetal life. Am J Cardiol 1996;77:1083-8.
16. Cecchin F, Hohnsrude CL, Perry JC, Friedman RA. Effect of age and surgical technique
on symptomatic arrhythmias after the Fontan procedure. Am J Cardiol 1995;76:386-91.
17. Mahaim I. Kent's fibers and the A-V paraspecific conduction through the upper
connections of the bundle of His-Tawara. Am Heart J 1947;33:651-3.
18. Kottkamp H, Hindricks G, Shenasa H et al. Variants of preexcitation -- Specialized
atriofascicular pathways, nodofascicular pathways, and fasciculoventricular pathways:
Electrophysiologic findings and target sites for radiofrequency catheter ablation. J Cardiovasc
Electrophysiol 1996;7:916-30.
19. Gillette PC, Garson A Jr, Cooley DA, et al. Prolonged and decremental antegrade
tachycardia of left bundle branch block pattern without Wolff-Parkinson-White configuration
during sinus rhythm. Am Heart J 1982;103:66-74.
20. Wu MH, Lin JL, Wang JK, Chiu IS, Young ML. Electrophysiological properties of dual
atrioventricular nodes in patients with right atrial isomerism. Br Heart J 1995;75:553-5.
21. Wu MH, Wang JK, Lin JL et al. Supraventricular tachycardia in patients with right atrial
isomerism. J Am Coll Cardiol 1998;32:773-9.
22. Anderson RH, Davies MJ, Becker AE: Atrioventricular ring specialized tissue in the
normal heart. Eur J Cardiol 1974;2:219-30.
23. Ho SY, Anderson RH. Embryology and anatomy of the normal and abnormal conduction
system. In: Gillette PC, Garson A, Jr. eds. Pediatric arrhythmias: electrophysiology and
pacing. WB Saunders 1990:2-27.
24. Henneveld H;Htter P, Bink-Boelkens M, Sreeram N. Junctional ectopic tachycardia
evolving into complete heart block. Heart 1998;80:627-8.
25. Rossi L, Piffer R, Turolla E et al. Multifolcal Purkinje-like tumor of the heart.
Occurrence with other anatomic abnormalities in the atrioventricular junction of an infant
with junctional ectopic tachycardia, Lown-Ganong-Levine syndrome, and sudden death.
Figur e legends
Figure 1. The actuarial survival curve for the 22 patients with left atrial isomerism. The
number in the parentheses indicates the number of the patients stayed in the study at the
time-pint. The survival decreased with age. The survival at 5 years and 10 years was 87%
and 70% , respectively.
Figure 2. The probability free from bradyarrhythmias in 22 patients with left atrial isomerism.
The number in the parentheses indicates the number of the patients stayed in the study at the
time-pint. The probability free from bradyarrhythmias decreased with age.
Figure 3. The intracardiac electrocardiograms taken during atrial pacing at 600 ms (left) and
310 ms (right), respectively in a 4 years old girl (case 3 in table 3). The HV interval was
much shorter at the pacing cycle length of 310 ms than that at pacing cycle length of 600 ms.
The changes of QRS morphology can be identified in lead II (not shown), III (not shown),
aVF, V1 and V2 (not shown).
Figure 4. The intracardiac electrocardiograms taken during atrial pacing at 480 ms (left) and
300 ms (right) respectively in another 4 years old girl (case 1 in table 3). The HV interval
was much shorter and merged unto the ventricular activation at the pacing cycle length of
300ms than that at pacing cycle length of 480 ms.
Figure 5. The relations between the HV interval and the atrial pacing cycle length of the case
3 (A) and case 1 (B). In both, the HV interval was progressively shortened and the AH
Table 1. Intracardiac anomalies in 22 patients with left atrial isomerism
Interruption of IVC 18(82%)
Partial anomalous pulmonary venous return 6(27%)
Common atrium 9(41%) Atrioventricular canal 14(64%) Double-outlet RV 8(36%) Pulmonary stenosis 15(68%) Mitral atresia/hypoplasia 6(27%) Coarctation of aorta 1(5%)
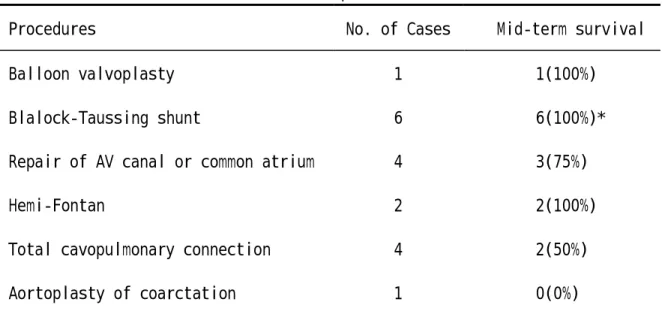
Table 2. Palliative interventions in 22 patients with left atrial isomerism
Procedures No. of Cases Mid-term survival
Balloon valvoplasty 1 1(100%)
Blalock-Taussing shunt 6 6(100%)*
Repair of AV canal or common atrium 4 3(75%)
Hemi-Fontan 2 2(100%)
Total cavopulmonary connection 4 2(50%)
Aortoplasty of coarctation 1 0(0%)
* One received total cavopulmonay connection 4 years after the shunt but died 4 months after the definite operation.
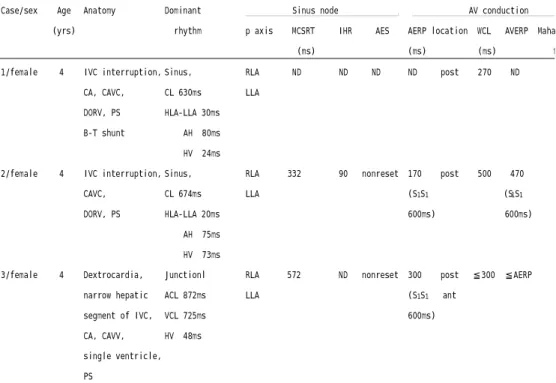
Table 3.Electrophysiological data in 3 LAI patients Case/sex Age (yrs) Anatomy Dominant rhythm Sinus node .
p axis MCSRT IHR AES (ms)
AV conduction .
AERP location WCL AVERP Mahaim-like (ms) (ms) fiber 1/female 4 IVC interruption,
CA, CAVC, DORV, PS B-T shunt Sinus, CL 630ms HLA-LLA 30ms AH 80ms HV 24ms RLA ND ND ND LLA ND post 270 ND (+)
2/female 4 IVC interruption, CAVC, DORV, PS Sinus, CL 674ms HLA-LLA 20ms AH 75ms HV 73ms RLA 332 90 nonreset LLA 170 post 500 470 (?) (S1S1 (S1S1 600ms) 600ms) 3/female 4 Dextrocardia, narrow hepatic segment of IVC, CA, CAVV, single ventricle, PS Junctionl ACL 872ms VCL 725ms HV 48ms RLA 572 ND nonreset LLA 300 post ≦300 ≦AERP (+) (S1S1 ant 600ms)
Abbreviations: ACL:atrial cycle length, AERP:atrial effective refractory period, AVERP:atrioventricular refract ory period, B-T shunt:Blalock-Taussig shunt, CA:common atrium, CAVC:common AV canal, DORV:double-outlet right ventricle, IHR:intrinsic heart rate, IVC:inferior vena cava, JET:junctional ectopic tachycardia, LLA:left-sided left atrium, MCSRT:maximal corrected sinus recovery time, PS:pulmonary stenosis, RLA:right-sided left atrium, TCPC:total cavopulmonary connection, VAWCL:ventriculo-atrial Wenckebach cycle length, VCL:ventricular cycle length, WCL:Wenckebach cycle length.
Table 4. Comparions between the partients with and without junctional ectopic tachycardia after intracardiae repair
with JET (n=3) without JET (n=7) Male/Female 1/2 2/4 Age at op (yr) 5.3±1.5 9.2±8.2 Dominant Junctional Rhythm
0 4 Ventricular morphology 2 ventricle 3 single ventricle 0 5 2