Abstract—Knowledge sharing of technology innovation on mobile learning is the main developmental force in the 21st century knowledge-based economy. In the new era of mobile society and information explosion, for college students who are receiving different kinds of information how to quickly learn and absorb different kinds of information to become their own knowledge and share it with friends are an important challenge. This study is aimed at the factors of students’ knowledge sharing of health technology in technological and professional colleges, validating a scale to measure the current situation for students’ knowledge sharing of health technology and to test some models for constructing students’ knowledge sharing of health technology. To achieve this goal, the following methods were adopted: literature review, Delphi survey, professional interview and sampling questionnaire survey (3,012 students from 16 technological and professional colleges in Taiwan) to examine the students’ knowledge sharing of health technology. The results showed that the students’ knowledge sharing of health technology consisted of behavior norm, sharing attitude, sharing intention, sharing behavior and sharing control in terms of the theory of planning behavior (TPB). The models of students’ knowledge sharing of health technology were tested with good fit through structural equation modeling (SEM). Since the path correlation of model was based on TPB, the following hypotheses concerning the students’ knowledge sharing behavior were supported: sharing attitude toward sharing intention, behavioral norm toward sharing intention, behavioral control toward sharing intention, sharing intention toward sharing behavior, and behavioral control toward sharing behavior, which all had positive effects. Finally, conclusions and suggestions were proposed for all forms of teaching, such as embedded teaching in health technological literacy, the methods of research and statistics, the policy of promoting students to the holistic health, and further research including a bridge building between the technological and professional colleges and industries for teachers and practitioners, then constructing a significant wireless connectivity of knowledge sharing with hardware and software of mobile learning in health technology should be considered.
Key words—Health Technology, Structural Equation modeling, Technological Colleges, Knowledge Sharing, Theory of Planning Behavior.
I. INTRODUCTION
HE number of technological and professional colleges in Taiwan increased to 78 in the 2007-2008 school year and
has been increasingly expanded. Since the higher technological and vocational education deregulated, current students of higher education place themselves to the modern technological environment; they use and depend on technology more than the students in the past. The technology is helpful for their learning and training, but it’s better not to impact of their health. And the technology is originally one kind of process of question- solving in modern society, and the people use it with resources and creativity to solve effectively the practical questions. Then mobile learning is the exciting art of using mobile technologies to enhance the learning experience. However, the students face all kinds of technological environments, and they addict themselves to it and extricate themselves with difficulty. The survey discovered 11% of college students who spent over six hours on the Internet every day, and thus they were stricken by headache, sleep disorder, and anxiety, and also could agitate restlessly when they were not on the Internet. They lost all interests in life and addicted themselves to network which threatened seriously their health. The current health technology had the direct and indirect influence to users' health of mind, body, physiological and psychological wound or psychogenic diseases and so on[8]. The college students contact frequently the technology, but they often lack actually the health technological literacy and do not understand the pros and cons of both sides of technology to impact of the health. Then they pursue constantly the innovative products, and neglect the fact that it would initiate the serious problems in mind and body health and hoodwink their advantages.
Although the related articles of knowledge management and knowledge transfer were many in recent years, those based on the theory of planning behavior of social psychology to explain the knowledge sharing behavior of health technology actually were extremely rare. All the knowledge transfer or sharing behavior usually carry on in organizations, such as the hospital doctor's knowledge sharing [27], or the individual nurse knowledge transfer in hospitals[31]. There was not yet a paper in view of students’ knowledge sharing of health technology in technology universities. Therefore, the authors intend to explore the students’ knowledge sharing of health technology in technology universities according to many years of teaching experience in technology universities.
【
附錄5】
A study on the Knowledge Sharing of
Health Technology for Technological College
Students’ Mobile Learning
Chin-Mou Cheng, Li-Jung Chen
II. DOCUMENTARY ANALYSIS A. The meaning of health technology
The health technology is one kind of technology which is associated directly with person's health, and promotion of person's health and prevention of diseases. Using this technology, one could improve the condition to restore the health for sickness (medical service), and would strengthen the longevity with health caring for no sickness (health care). The health technology contains the health service to promote health, to prevent and the treating method of disease, as well as the improvement condition and restoration of the health (http://www.ncchta.org/). The health technology is not only the exquisite, innovative utensil or medicine, but also contains the related health activity, as well as using medicine and health caring, such as accepting the innovative technology to protect health with a positive effectiveness [9]. At present for the vitality diet holding a preventive medicine and health status of reconstruction, it has two functions: treatment of illness and health caring (http://life.edu.tw/). This study explores the students’ cognition of health technology in technological and professional colleges under the technological environment to health cognition which contains medical and health caring of body and mind to share the health knowledge sharing behavior.
The college students should consider the impact of their health under the technological environment [30]. Because of lacking the cognition of health technology to share initiatively the health knowledge; they heavily rely on the network technology and bring about a morbid state, unhealthy, and an abnormal mind [15] [29]. It wants to compile a suitable quantitative tool to understand their health technological knowledge sharing [10] [23] [14]. We understand the meaning of health technology through literature review about the impact of health under the technological environment. Due to the rapid advancement of mobile communication and wireless transmission technology, many scholars in academia believed that these new technologies will have a great impact on the way of learning in the future. With advances in information and communication technology, wireless communication and mobile devices are most applied to education recently. As a matter of fact, mobile Learning can be implemented accordingly by effectively applying short-message services as learning content delivery methods, provided by mobile phone system to deliver different learning content types.
Many mobile learning projects from around the world have been focused on repurposing existing content to work on a mobile device to solve knowledge sharing needs (http://www.clomedia.com). Digital mobile learning activity may be described through a learner creating their own data or communicating with peers, mentors or in other learning relationships[22]. Enabling students to get the information and learning what they need in the format, device and time frame they want, while being able to collaborate and learn from one another to create and share knowledge, is the key to performance.
B. Theory of Planning Behavior
Based on the Theory of Planning Behavior (TPB), the attitude, subjective norm and perceived behavioral control affect the behavior and intention. The more advantageous attitude, subjective norm and perceived behavioral control are, the stronger individual intention to solve behavior question is. Perceived behavioral control refers to the individual perception of difficulty to carry out the advantageous behavior and corresponds to self-efficacy which affects directly the behavior intention and behavior. The factors which affect directly or indirectly the knowledge sharing behavior are subjective norm, attitude intention, perceived behavioral control and so on [27]. However, actual behaviors on Internet usage and perceptions on the usefulness of the Internet were more important than affective responses toward computer networks in predicting adolescents’ Internet addiction[31].
To predict whether a person intends to do something, we need to know: Whether the person is in favor of doing it (attitude); how much social pressure the person feels in doing it (subjective norm); whether the person feels in control of the action in question (perceived behavioral control)
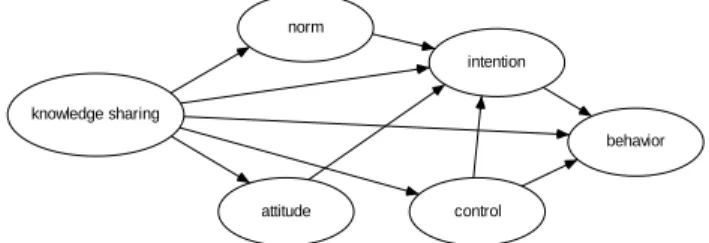
By changing these three ‘predictors’, we can increase the chance that the person will intend to do a desired action and thus increase the person’s chance of actually doing it. In a clinical consultation, the clinician’s treatment decisions and actions are examples of intentional behavior. The Theory of Planned Behavior can be useful in designing strategies to help people to adopt healthy behaviors TPB developed initiatively in 1975[17], from 1975 to January 2007,;apparently, hundreds of researchers have used this theory[1] [2] [3] [4] [5] [6] to know the influence of attitudes on behavior, intention to behavior and the relationship of attitude, personality and behavior TPB had been widely utilized to the medical behavior, lifelong study, health, on-line declaring goods [33], information system and so on, and therefore this research explores initiatively the knowledge sharing of health technology. The research model was constructed as shown in Figure 1.
knowledge sharing norm attitude intention control behavior
Figure 1 The research model C. Knowledge transfer (sharing)
The focus of knowledge management is knowledge sharing in 21st century knowledge-based economy. The industries of the related health take gradually the knowledge as the standard community group and form a link with the healing institute and the consumers to reduce the cost of organizations, promoting the quality by sharing knowledge[7]. But the related knowledge sharing research, such as individual knowledge transfer [32] and knowledge transfer of network community
[12]. This study explores the knowledge sharing behavior of health technology from students’ viewpoint. The related papers, such as factors impacting nurses’ transference of theoretical knowledge of holistic care into clinical practice [20]; knowledge sharing behavior of physicians in hospitals.[27] . The healthy professional of educational situation may penetrate the training to share knowledge of health technology [28]. In hospitals the clients who want to share health knowledge are few [29]. The health knowledge is created by a cooperative relation way to produce a innovative knowledge transfer [11]. A study of taxpayers’ intentions explores the acceptance of electronic tax filing, showing the influence of attitude, subjective norm, and self-efficacy toward intention [17]. Knowledge sharing behavior of health technology, for example, “I share something right after it is gained from the elder member of a family about the health technological knowledge.” The related articles showed that the sharing health technology knowledge was decided by intention, subjective norm, perceived behavior control and what not [24] [19] [20] [13].The hypotheses of this study are derived from TPB, after the sharing attitude, norm, control, and intention, then sharing behavior, and use structure equation. modeling(SEM) to confirm these hypotheses.
III. RESEARCH DESIGN A. Research Hypotheses
The research hypotheses are derived from TPB and the related literature review mentioned above, and these hypotheses are listed as follows:
A1 There is a positive correlation between the sharing attitude and sharing intention.
A2 There is a positive correlation between the behavioral norm and sharing intention.
A3 There is a positive correlation between the behavioral control and sharing intention.
A4 There is a positive correlation between the sharing intention and sharing behavior.
A5 There is a positive correlation between the behavioral control and sharing behavior.
B. Method 1 Samples
By using survey method with cluster and stratified random sampling from 16 technological and professional colleges in Taiwan, 3,600 questionnaires were sent out, and 3,012 of effective questionnaires were returned, with a survey reaching 83.67% of return-ratio.
2 Research tool
The completion of scale about knowledge sharing of health technology for college students as a measuring tool which is derived from the process of literature analysis, by means of consulting with 10 experts and the Delphi questionnaire survey of which 16 experts’ opinions tend to be consistent with and develop the official scale. Using the confirmatory factor analysis (CFA), this study supposes that the knowledge sharing
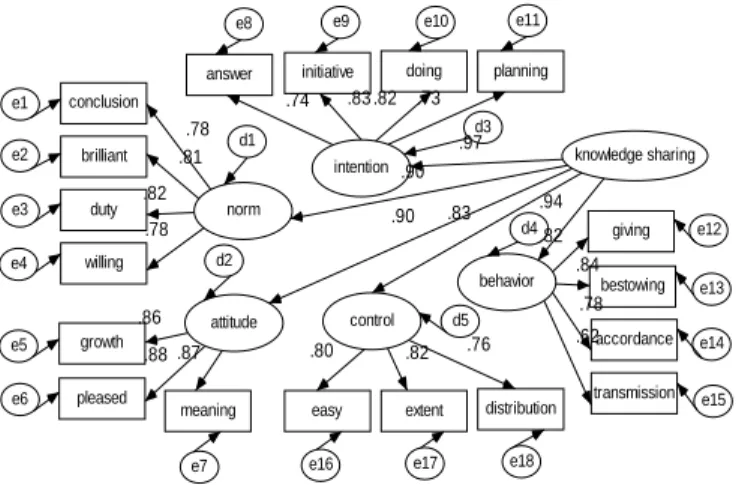
of health technology (second-order factor) for college students contains 5 variables: behavioral norm, sharing attitude, behavioral control, sharing intention and sharing behavior (first order factor). This scale consists of 18 items and analyzes with two-order CFA by using AMOS6.0 statistics software shown in Figure 2.
conclusion
brilliant
duty
willing
answer initiative doing planning
growth
pleased
meaning easy extent distribution giving bestowing accordance transmission norm intention control attitude behavior .78 .76 e1 e2 e3 e4 e5 e6
e7 e16 e17 e18
e15 e14 e13 e12 e11 e10 e9 e8 d3 d4 .78 .82 .81 .82 d2 d1 d5 .86 .88 .87 knowledge sharing .83 .83 .74 .84 .82 .80 .73 .62 .78 .90 .90 .94 .82 .97
Figure2 Two-order factor model of scale
On the individual variable of this model, the all standardized loading coefficients of observation variables are in a very high significant level as shown in Figure 2. It showed that the hypotheses of theoretical models and the actual observational material were very good fit as shown in Table 1. Therefore, the 5 variables(norm, attitude, intention, behavior and control) of first-order factor were suitably used to explain 18 observational variables, and the knowledge sharing of health technology of second-order factor explains the 5 first-order factor whose standardized loading coefficients were .831, .895, .899, .935, and .966, respectively. In the 5 latent variables, norm consisted of conclusion, brilliant, duty and willing; attitude consisted of growth, pleased and meaning; intention consisted of answer, initiative, doing and planning; behavior consisted of giving, bestowing, accordance and transmission; and control consisted of easy, extent and distribution.
Table 1 Two-order factor analysis good fit test
Good fit indicator norm data Judgment
Chi-square/df <3 P>.001
1.498 P=.002
Good fit RMSEA <0.05 0.014 Good fit
RMR <0.05 0.009 Good fit
SRMR <0.05 0.039 Good fit
GFI >0.9 0.994 Good fit
AGFI >0.9 0.989 Good fit
NFI >0.9 0.996 Good fit
NNFI >0.9 0.998 Good fit
CFI >0.9 0.999 Good fit
IFI >0.9 0.999 Good fit
RFI >0.9 0.993 Good fit
PNFI >0.5 0.586 Good fit
PGFI >0.5 0.523 Good fit
CN >200 2057 Good fit
3 Factor analysis
constructed. The knowledge sharing of health technology(18 items) was suitably used to implement the factor analysis by Kaiser- Meyer- Olkin Measure of Sampling Adequacy (coefficient=.967, Chi-square =32101.783, p < .001). The knowledge sharing of health technology (second-order factor) contains the behavioral norm, sharing attitude, behavioral control, sharing intention, and sharing behavior (first-order factor). Therefore, this scale embraced the whole construction effect.
4 Reliability analysis
As to a reliability analysis, Table 2 showed that the scale items Cronbach's alpha coefficient of knowledge sharing were all over .80, with the entire scale reaching as high as .955, and Guttman Split-half alpha coefficient all over .70, and it demonstrated that the consistence of internal contents was very intense. Explaining the item-total correlation and factor loading of latent variables in an order way, norm(4 items) range from .669 to .774; attitude (3items) range from .767 to .810; intention (4 items) range from .701 to .798; behavior (4 items) range from .603 to .793; and control(3 items) range from .635 to .726. The tem-total correlations were all over .60, and the factor loadings were all over .63.
Therefore, the above-mentioned scale (Appendix A) of knowledge sharing of health technology for students in technological and professional colleges is a suitable measuring tool with high validity and reliability. A multi-item method was used to increase the accuracy of measurement, and each item was based on a six point Likert scale. Eighteen measured items were used to reflect the components of the TPB models. Table 2 Factor analysis, reliability analysis
Factor item-total factor loading Cronbach'sα Split-half
Knowledge sharing (18 items) .955 .892
norm (4 items) .875 .836 conclusion .669 .711 brilliant .715 .752 duty .737 .774 willing .732 .770 attitude (3items) .901 .795 growth .767 .804 pleased .768 .805 meaning .773 .810 intention (4 items) .853 .840 answer .701 .744 initiative .765 .798 doing .751 .785 planning .706 .737 behavior (4 items) .842 .811 giving .759 .791 bestowing .761 .793 accordance .726 .758 transmission .603 .637 control(3 items) .834 .753 easy .696 .726 extent .688 .716 distribution .635 .667
IV. RESULTS AND DISCUSSION
The findings showed the background factors of technological and professional colleges students, such as: gender, educational system, department, using technology, social relationship, family relationship and awareness of health; besides the age; it showed differences on the scale contents of knowledge sharing of health technology in technological and professional colleges. The research hypotheses of this study were examined as shown in Figure 3.
conclusion
brilliant
duty
willing
answer initiative doing planning
growth
pleased
meaning easy extent distribution giving bestowing accordance transmission norm intention control attitude behavior .77 .76 e1 e2 e3 e4 e5 e6
e7 e16 e17 e18
e15 e14 e13 e12 e11 e10 e9 e8 d3 d4 .79 .83 .80 .81 d2 d1 d5 .87 .87 .86 knowledge sharing .76 .83 .74 .83 .82 .80 .73 .63 .79 .24 .37 .94 .93 -1.02 -.87 .36 .82 2.81
Figure 3 The model concerning knowledge sharing of health technology and examining hypotheses
From Figure 3 we could find that the A1-A5 research hypotheses were examined by using the revised model, and there were all positive effects. The findings also support TPB applied to the forecast and explaining knowledge sharing behavior of health technology. The path correlation of model was according to TPB, and the following hypotheses were concerned with the knowledge sharing behavior as the students in technological and professional colleges proved(A1-A5): sharing attitude toward sharing intention, behavioral norm toward sharing intention, behavioral control toward sharing intention, sharing intention toward sharing behavior, and behavioral control toward sharing behavior, and all showed positive effects. Based on the TPB, knowledge sharing of health technology by using multi-groups (man group, female group) model analysis, the results also conform to the TPB findings [35] [26] [36]. It is truly said that to predict whether students in technological and professional colleges intend to do knowledge sharing, we know: the students are in favor of doing knowledge sharing (sharing attitude), feel social pressure to do knowledge sharing (behavioral norm), and feel in control of the action in sharing question (behavioral control), and then these three ‘predictors’ will let students intend to do a desired knowledge sharing(sharing intention) and hence increase the students’ chance of actually doing knowledge sharing.
V. CONCLUSIONS AND SUGGESTIONS
This study discovered the background factors of technology universities students, such as: gender, educational system, department, using technology, social relationship, family relationship and awareness of health; besides the age, revealing
the significant differences on scale contents of knowledge sharing of health technology. Then the model of knowledge sharing structure of health technology for university students had a good suitably fit through structural equation modeling (SEM). The hypotheses derived from literature review were proved just as TPB had conformed. It meant that the sharing attitude had a positive correlation toward behavioral intention; behavioral norm also had a positive correlation toward sharing intention; behavioral control also had a positive correlation toward sharing intention; sharing intention also had a positive correlation toward sharing behavior, and behavioral control also had a positive correlation toward sharing behavior. In other words, the more positive sharing attitude of students in technological and professional colleges toward health technological knowledge are, the more obvious their sharing intention to health technological knowledge are; the more effective their behavioral norm from family or group are, the more obvious their sharing intention to health technological knowledge are; the easier their behavioral control of perception are, the stronger their sharing intention; the more obvious their sharing intention to health technological knowledge are; the more frequentative their actual sharing behavior of health technological knowledge are; and the easier their behavioral control of perception, the more frequentative their actual sharing behavior of health technological knowledge are.
The suggestions were proposed for related forms of teaching, such as embedded teaching of enhancing the knowledge sharing of health technology for students in technological and professional colleges. It can serve as references for further research, like bridge building between the technological and professional colleges and industries for teachers and practitioners. Then the papers of choiceness or high quality of the related health technology could be submitted to international journals to promote the research level of professional and vocational universities. Finally, it proves feasible to use the structural equation modeling (SEM) to construct a model of knowledge sharing on health technology in cooperation between schools and industries in the foreseeable future.
Finally, the mobile features are indeed considered useful [18] for nursing and medical students by using wireless personal digital assistants (PDAs) [32] to construct a significant wireless connectivity of knowledge sharing with hardware and software of mobile learning in health technology. New communication technology, especially mobile communication technology, is supposed to be effective in encouraging interaction between the student and the instructor and improving learning efficiency [25]. Additionally, the adaptive task assignment for multiple mobile learning via swarm intelligence approach to share knowledge [37]. All of this should be concerned about.
APPENDIX
A Scale of knowledge sharing of health technology items Option: six point from 1(extreme agreement) to 6(extreme disagreement)
Item content option
1. Most people who are important to me think that I should share knowledge of health technology with others
2. People whose opinions I value would approve of my behavior to share knowledge of health technology with others 3. I have the duty to share knowledge of health technology with
others for I am a team member.
4. Most people who are concerned with me share their health technological knowledge with others.
5. If I share my health technological knowledge with other members, I feel very beneficial.
6. If I share my health technological knowledge with other members, I feel very pleasant.
7. If I share my health technological knowledge with other members, I feel very meaningful.
8. I always will intend to share health technological knowledge with my classmates, if they ask.
9. I always will intend initiatively to share health technological knowledge with others.
10. I always will make an effort to share health technological knowledge with others.
11. I always will plan to share health technological knowledge with others.
12. I will necessarily share health technological knowledge with others obtained from family members or elder people 13. I will immediately share health technological knowledge
with my good friends obtained from teachers or schoolmates.
14. I will instantly share health technological knowledge with other people obtained from the multimedia technology. 15. I will transmit the health technological messages to my good
friends by using email.
16. For me to share my health technological knowledge is always possible.
17. It is mostly up to me whether or not I share health technological knowledge.
18. I believe that there is much control I have to share my health technological knowledge with others.
ACKNOWLEDGMENT
This is part of a larger study on knowledge sharing of health technology that has been generously supported by the National Science Council of Taiwan, (NSC 95-2516-S-242-002).
REFERENCES
[1] Ajzen, I., & Fishbein, M. (1980). Understanding attitudes and predicting social behavior. Englewood Cliffs, NJ: Prentice-Hall.
[2] Ajzen, I., (1985). From Intention to Actions: A Theory of Planned Behavior, in J. Kuhl and J. Bechmann (Eds), Action-Control: From Cognition to Behavior, Springer, Heidelberg, 11-39.
[3] Ajzen, I. (1991). The theory of planned behavior. Organizational Behavior and Human Decision Processes, 50, 179-211.
[4] Ajzen, I. (2002). Perceived behavioral control, self-efficacy, locus of control, and the theory of planned behavior. Journal of Applied Social Psychology, 32, 665-683.
[5] Ajzen, I. (2005). Attitudes, personality, and behavior (2nd. Edition). Milton-Keynes, England: Open University Press / McGraw-Hill.
[6] Ajzen, I., & Fishbein, M. (2005). The influence of attitudes on behavior. In D. Albarracín, B. T. Johnson, & M. P. Zanna (Eds.), The handbook of attitudes (pp.173-221). Mahwah, NJ: Erlbaum.
[7] Bose, R. (2003). Knowledge management- enabled health care management systems: capabilities, infrastructure, and decision-support. Expert Systems with Applications. 24. 59–71.
[8] [8]Burdea, G. C., Coiffet, P. (2003), Virtual Reality Technology (2nd edition), John Wiley & Sons, Inc., Hoboken, New Jersey.
[9] Calnana, M., Montanerb, D., Horne, R.(2005). How acceptable are innovative health-care technologies? A survey of public beliefs and attitudes. Social Science & Medicine, 60, 1937-1948.
[10] Caplan, S. E. (2002), Problematic Internet use and psychosocial well-being: development of a theory-based-cognitive-behavioral measurement instrument, Computers in Human Behavior, 18, 553-575. [11] Carayannis, Elias G. (1999) Knowledge transfer through technological
hyperlearning in five industries Technovation, Vol: 19, Issue: 3, 141-161. [12] Chen Chun-Yu (2006). A Model of Knowledge Transfer and Research Innovation Performance in a Cyber-Based Community, Industrial Technology Education, National Kuohsuing Normal University. [13] Chou, S.-W. (2005).Designing good institutional contexts for innovation
in a technology- mediated learning environment. Journal of Computer Assisted Learning 21, pp269–280.
[14] Collins, R. P., (2004), The measurement of perceptual curiosity, Personality and Individual Differences, 36, 1127-1141.
[15] Davis, R. A. (2001), A cognitive-behavioral model of pathological
Internet use, Computers and Human Behavior, 17, 187-195.
[16] Fishbein, M., & Ajzen, I. (1975). Belief, attitude, intention, and behavior: An introduction to theory and research. Reading, MA: Addison-Wesley [17] Fu, J.-R., Farn,C.-K., Chao, W.- P. (2006). Acceptance of electronic tax
filing: A study of taxpayer intentions. Information & Management, 43, 109-126.
[18] Garrett, B. M.; Jackson, C. (2006).A mobile clinical e-portfolio for nursing and medical students, using wireless personal digital assistants (PDAs) Nurse Education Today. 26, 647–654.
[19] Hakkinen, Paivi; Jarvela, Sanna (2006). Sharing and constructing perspectives in web-based conferencing. Computers & Education. 47. 433–447.
[20] Henderson, S. (2002). Factors impacting on nurses’ transference of theoretical knowledge of holistic care into clinical practice. Nurse Education in Practice. 2, 244–250.
[21] Low, L., O’Connell, M. (2006).‘Learner-centric design of digital mobile learning’. Paper presented at Learning on the Move, Brisbane, Australia. Retrieved 25 October 2006.
[22] Luarn, Pin., Lin Hsin-Hui (2005). Toward an understanding of the behavioral intention to use mobile banking. Computers in Human Behavior, 21, 873–891.
[23] Novak, T. N. & Hoffman, D. L.,( 2000), Modeling the Structure of the Flow Experience Among Web Users, Research: Manuscripts. http://elab.vanderbilt.edu/
[24] Phuanukoonnon, S., Brough, M., Bryan, J. H.(2006). Folk knowledge about dengue mosquitoes and contributions of health belief model in dengue control promotion. Acta Tropica. 99. 6–14.
[25] Rau, Pei-Luen , Gao, Q., Wu, Li-Mei.(2008). Using mobile communication technology in high school education: Motivation, pressure, and learning performance. Computers & Education. 50, 1, 1-22.
[26] Rhodes, R., Courneya, K. (2005). Threshold assessment of attitude, subjective norm, and perceived behavioral control for predicting exercise intention. Psychology of Sport and Exercise. 6, 349-361.
[27] Ryu, S., Ho, S. H., Han, I. (2003). Knowledge sharing behavior of physicians in hospitals, Expert Systems with Applications, 25, 113–122. [28] Shafer, M. S., Rhode, R., Chong, J. (2004). Using distance education to promote the transfer of motivational interviewing skills among behavioral health professionals, Journal of Substance Abuse Treatment, 26, 141–148.
[29] Shapira, N. A. (2000). Psychiatric features of individuals with problematic internet use, Journal of Affective Disorders, 57, 267-272. [30] Steinemann, A. (2000). Rethinking human health impact assessment,
Environmental Impact Assessment Review, 20, 627–645
[31] Tsai, C. C., Lin, S. J (2001).Analysis of Attitudes Toward Computer Networks and Internet Addiction of Taiwanese Adolescents. Cyberpsychology and Behavior, 4(3), 373-376.
[32] Tsai, Ling-Long (2004). Individual knowledge transfer, business management is the doctoral dissertation, National Cheng-Kung university.
[33] Virvou, M.; Alepis, E. (2005). Mobile educational features in authoring tools for personalised tutoring. Computers & Education. 44, 53–68. [34] Whiddett, R., Hunter, I., Engelbrecht, J., Handy, J. (2006).Patients’
attitudes towards sharing their health information. International Journal of Medical Informatics. 75, 530-541.
[35] Wu, I.-L., Chen, J.-L.(2005). An extension of Trust and TAM model with TPB in the initial adoption of on-line tax: An empirical study. Int. J. Human-Computer Studies 62 784–808
[36] Yi, M.Y., Jackson, J. D., Park, J. S., Probst, J. C.(2006). Understanding information technology acceptance by individual professionals: Toward an integrative view. Information & Management. 43. 350–363. [37] Zhang, Dandan; Xie, Guangming; Yu, Junzhi; Wang, Long (2007).
Adaptive task assignment for multiple mobile robots via swarm intelligence approach. Robotics and Autonomous Systems. 55, 7, 572-588.
Chin-Mou Cheng
Ph.D Department of Industrial Technology Education, National Kaohsiung Normal University; Associate Professor, College of Humanities and
Management, Fooyin University
Li-Jung Chen
Ph.D candidate, Department of Industrial Technology Education, National Kaohsiung Normal University