Helicobacter pylori Infection Increases Subsequent Ischemic Stroke
Risk: A Nationwide Population-based Retrospective Cohort Study
Running title: Helicobacter pylori Infection, Risk of Ischemic Stroke
Wei-Shih Huang, MD; Cheng-Li Lin, MSc; Chon-Haw Tsai, MD; Chia-Hung Kao, MD
From the Department of Neurology, China Medical University Hospital, Taichung, Taiwan (W.S.H., C.H.T.); Graduate Institute of Clinical Medical Science and School of Medicine, College of Medicine, Taichung, Taiwan (W.S.H., C.H.T., C.H.K.); Management Office for Health Data, China Medical University Hospital, Taichung, Taiwan (C.L.L.); Department of Nuclear Medicine and PET Center, China Medical University Hospital, Taichung, Taiwan (C.H.K.)
Correspondence should be addressed to Dr. Chia-Hung Kao, Graduate Institute of Clinical Medicine Science and School of Medicine, College of Medicine, China Medical University, No. 2, Yuh-Der Road, Taichung 404, Taiwan. Tel: +886 4 22052121x7412; Fax: +886 4 22336174; E-mail: [email protected]
Contribution
Wei-Shih Huang, Chon-Haw Tsai, and Chia-Hung Kao are responsible for the study design, coordination and drafted the manuscript. Cheng-Li Lin collected data and performed analysis. Chon-Haw Tsai and Chia-Hung Kao provided some intellectual recommendation and reviewed the manuscript. All authors wrote the final version of the manuscript. All authors read and approved the final manuscript.
Acknowledgments
This study was supported in part by the Taiwan Ministry of Health and Welfare Clinical Trial and Research Center of Excellence (DOH102-TD-B-111-004), China Medical University Hospital (DMR-102-014), Academia Sinica Taiwan Biobank, Stroke Biosignature Project (BM102021169), Tseng-Lien Lin Foundation, Taichung, Taiwan and Katsuzo and Kiyo Aoshima Memorial Funds, Japan.
Conflicts of Interest
The authors report no conflicts of interest or financial interest associated with this work, both collectively and individually.
Abstract
Background and Purpose: The association of Helicobacter pylori infection (HP-I) with ischemic stroke (IS) incidence has been studied, but conflicting results have been reported. The purpose of this study was to investigate the association between chronic HP-I and the risk of acute IS by using data from the Taiwan National Health
Insurance Research Database.
Methods: We identified17 332 patients with HP-I and 69 328 randomly selected age- and gender-matched controls from January 1, 2000 to December 31, 2010. Both cohorts were followed up until the occurrence of IS or until censored. The Cox proportional hazards model was used for assessing the association of HP-I with IS. Results: Compared with the control cohort, patients diagnosed with HP-I exhibited a higher incidence rate of IS (14.8 vs 8.45 per 1000 person-years) and a hazard ratio (HR) of 1.521.54 (95% confidence interval [CI] = 1.40–1.65). The HRs for IS were
1.491.51 (1.37–1.62) in patients diagnosed with HP-I who had one admission, increasing to 2.262.30 (1.71–1.98) for those who had 2 or more admissions when adjusted for age, sex, and comorbidities (P for trend < .0001). In addition, we observed a significantly positive association between nonembolic IS and increased admissions (P for trend < .0001), but negative association with embolic IS.
Conclusion: Chronic HP-I is significantly associated with an increased risk of IS, particularly nonembolic IS. Anti-HP therapy may be beneficial to IS prevention.
Introduction
Helicobacter pylori (HP) is a gram-negative, spiral-shaped microaerophilic bacterium. HP may be a lifelong bacterial infection of the gastric mucosa that is primarily acquired during childhood. HP infection (HP-I) is a widespread infection in humans, and its prevalence is positively correlated with population age.1–3 The
seroprevalence of HP-I was positively observed in approximately 50% of the world’s population and the results indicated higher numbers of HP-I in developing than in developed countries.4 Large proportions of Asian populations, particularly the Chinese, Japanese, and Korean populations, are infected with HP.2–3
HP-I can cause various diseases, such as chronic gastritis, peptic ulcers, and gastric cancer.1,5 In addition, HP has been associated both epidemiologically and
pathogenetically with coronary atherosclerosis,6 but data on the relationship between chronic HP-I and ischemic stroke (IS) are conflicting.7–12
Stroke is the leading cause of death and disability for both men and women worldwide, and IS is the most common type of stroke.13–16 Identifying potential risk factors is an effective method for preventing IS. The traditional risk factors for IS do not explain every clinical and epidemiological feature of the disease. The purpose of our study was to assess the relationship between chronic HP-I and the risk of acute IS by using data recorded from the National Health Insurance Research Database
(NHIRD) of Taiwan.
Materials and Methods Data Sources
We used inpatient claims data from Taiwan’s NHIRD, which were provided by the National Health Research Institutes (NHRI) from 1996 to 2010. The Taiwanese government launched the National Health Insurance (NHI) program in March 1995 and approximately 99% of the 23.74 million people in Taiwan were covered by the end of 2009.17 The NHIRD is derived from the NHI program established by the Bureau of National Health Insurance. The International Classification of Diseases, 9th Revision, Clinical Modification (ICD-9-CM) was used to determine health status. In addition, this study was approved by the Institutional Review Board of China Medical University in Central Taiwan (CMU-REC-101-012).
Study patients
We identified 17 332 patients with newly diagnosed HP-I (ICD-9-CM code: 041.86) in the inpatient claims data of the NHIRD in 2000–2010 as the HP-I cohort, and the HP-I diagnosis date was used as the index date. We excluded patients with history of stroke before the index date and those for which information on age or gender was missing. Four study patients in the comparison cohort for every patient diagnosed with HP-I were randomly selected from the insured people without a
history of HP-I or stroke, and then frequency-matched for age (± 5 y), gender, and index year. The HP-I cohort comprised 17 332 patients and the control cohort comprised 69 328 patients.
Measurement
The demographic factors in this study were gender and age. Age was categorized into 4 groups: ≤ 35, 36–50, 51–65, and > 65 years. We considered diabetes CM code: 250), hypertension CM codes: 401-405), hyperlipidemia (ICD-9-CM code: 272), congestive heart failure (CHF; ICD-9-(ICD-9-CM codes: 398.91, 402, 404.01, 404.03, 404.10, 404.11, 404.13, 404.91, 404.93, and 428), coronary artery disease (CAD; ICD-9-CM codes: 410-414), atrial fibrillation (AF; ICD-9-CM code: 427.31), chronic obstructive pulmonary disease (COPD; ICD-9-CM code:491, 492, and 496) and asthma (ICD-9-CM code:493, 494) to be comorbidities that were potential confounders for the association of HP-I with IS.
The endpoints were the first diagnosis date of IS (ICD-9-CM codes: 433-438), death and loss to follow-up, and December 31, 2010. The IS cases were grouped into embolic IS (ICD-9-CM code: 434.11) and nonembolic IS (ICD-9-CM codes: 433-438; except embolic IS, ICD-9-CM 434.11).
Statistical analysis
Proportions were calculated for the study patients for categorical variables including gender, age, and comorbidity. The t test was used for the continuous variables and the
chi-square test was used for the categorical variables. The incidence rates of IS were calculated by dividing the number of newly diagnosed cases by the number of person-years. The number of person-years was calculated by summing the number of years from the entry date to the endpoint determined according to the incidence of stroke, death, loss to follow-up, and the end of follow-up. We used the Kaplan-Meier (K-M) estimation method to depict the survival curves of nonembolic IS for patients
diagnosed with and those not diagnosed with HP-I. We then used the log-rank test to evaluate whether the K-M curves differed. The Cox proportional hazard regression and 95% confidence interval (CI) were used to estimate the independent effect of HP-I by adjusting for gender, sex, and comorbidity. Statistical significance was
considered to be P < .05 in all analyses. SAS version 9.3 was used for the statistical analyses.
Results
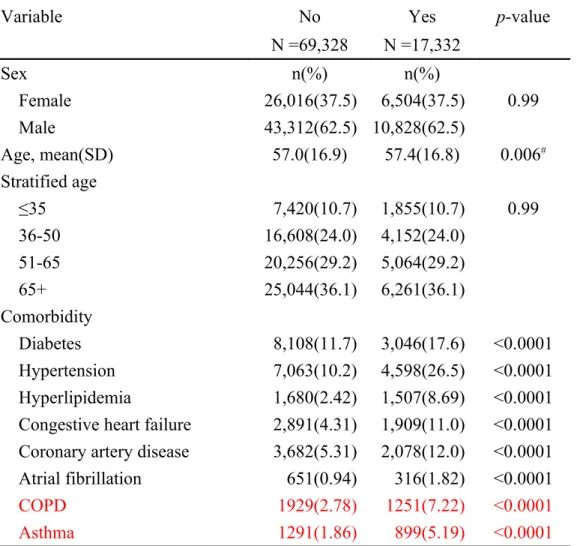
Table 1 shows the baseline demographic factors and comorbidity of the study patients according to HP-I status. The distributions of gender and age were the same for both cohorts. Compared with the participants without HP-I, patients with HP-I exhibited a higher prevalence of diabetes (17.6% vs 11.7%), hypertension (26.5% vs 10.2%), hyperlipidemia (8.7% vs 2.4%), CHF (11.0% vs 4.3%), CAD (12.0% vs 5.3%), AF (1.8% vs 0.9%), COPD (7.22% vs 2.78%) and asthma (5.19% vs 1.86%).
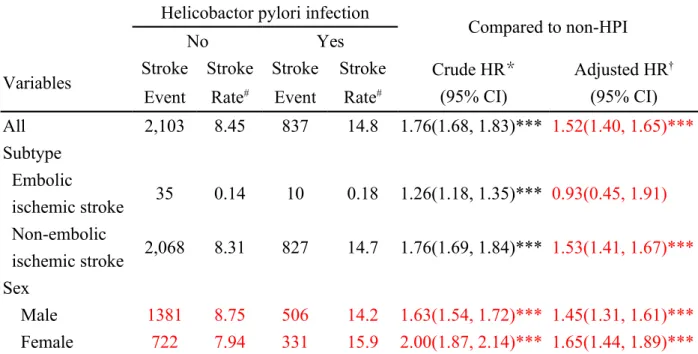
Table 2 shows the incidence rates and HRs for IS according to HP-I status. Overall, the incidence of IS was higher in the HP-I cohort than in the control cohort (14.8 vs 8.45 per 1000 person-years), with an HR of 1.52 (95% CI = 1.40–1.65) when adjusting for age, gender, and comorbidity. Furthermore, patients with HP-I were 0.93
times more likely to develop embolic IS (95% CI = 0.45–1.91) and were 1.53 times more likely to develop nonembolic IS (95% CI = 1.41–1.67) than the control patients after adjusting for age, sex, and comorbidities. The sex-specific HP-I cohort to non- HP-I cohort relative risk of ischemic stroke were significant for both men (HR=1.45, 95% CI=1.31-1.61) and women (adjusted HR=1.65, 95% CI=1.44-1.89).
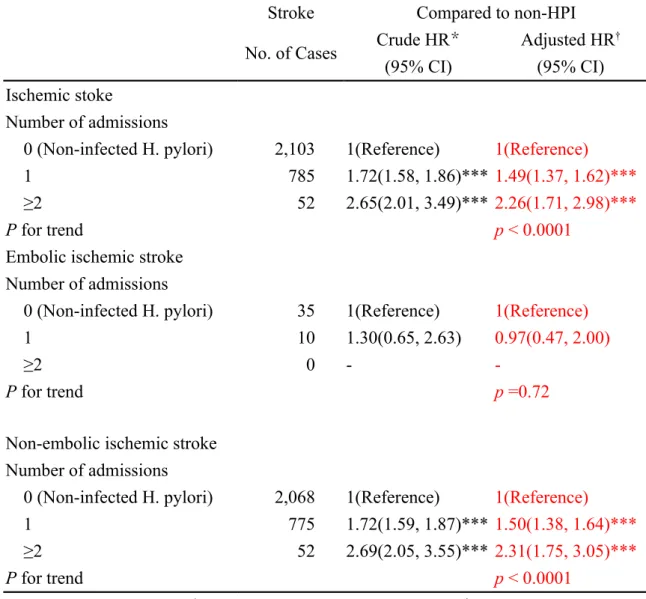
Table 3 shows the unadjusted and multivariate adjusted HRs for nonembolic IS according to HP-I status and stratified according to the number of admissions. Compared with patients without HP-I, the HRs for IS were 1.49 (95% CI = 1.37– 1.62) in HP-infected patients who had one admission, increasing to 2.26 (95% CI =
1.71–2.98) for those who had 2 or more admissions when adjusted for age, sex, and comorbidities. In addition, we observed a significantly positive association between nonembolic IS and increased admissions (P for trend < .0001).
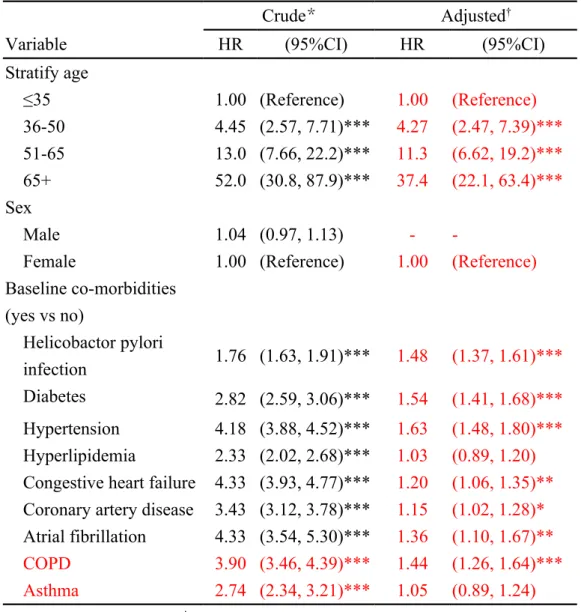
Table 4 shows the unadjusted and multivariate adjusted HRs for nonembolic IS associated with HP-I and covariates. In the multivariate analysis, the HRs for
than in those aged ≤ 35 years (HR = 4.27, 95% CI = 2.47–7.39 for those aged 36–50 y; HR = 11.3, 95% CI = 6.62–19.2 for those aged 51–65 y; HR = 37.4, 95% CI =
22.1–63.4 for those aged > 65 y). Significant associations were observed between nonembolic IS and HP-I, diabetes, hypertension, CHF, CAD, AF and COPD, and the respective adjusted HRs were 1.54 (95% CI = 1.41–1.68), 1.63 (95% CI = 1.48–1.80),
1.20 (95% CI = 1.06–1.35), 1.15 (95% CI = 1.02–1.28), 1.36 (95% CI = 1.10–1.67), and 1.44 (95% CI = 1.26–1.64).
The cumulative incidence curves for nonembolic IS according to HP-I status are illustrated in Figure 1. We used the log-rank test to examine the cumulative incidence of nonembolic IS between the HP-I cohort and the control cohort. We determined that the cumulative incidence of nonembolic IS was significantly higher in patients with HP-I than in patients without HP-I (P < .001).
Discussion
Compared with the control cohort, patients diagnosed with HP-I exhibited a higher incidence rate of IS (14.8 vs 8.45 per 1000 person-years) and a hazard ratio (HR) of
1.521.54 (95% confidence interval [CI] = 1.40–1.65, table 2). The HRs for IS were
1.491.51 (1.37–1.62) in patients diagnosed with HP-I who had one admission, increasing to 2.262.30 (1.71–1.98) for those who had 2 or more admissions when adjusted for age, sex, and comorbidities (P for trend < .0001). In addition, we
observed a significantly positive association between nonembolic IS and increased admissions (P for trend < .0001, table 3), but negative association with embolic IS. The association of HP-I with the risk of IS has been widely studied since 19987; however, it remains undetermined because conflicting results have been reported. A case-control study involving 145 cases and 160 controls by Heuschmann et al. indicated that HP seropositivity is not associated with the risk of IS.11 However, after subgroup analyses, they determined that HP seropositivity is associated with a 3.31-fold risk of IS caused by small artery occlusion and a 0.21-3.31-fold risk of cardioembolic stroke. Similarly, a recent case-control study involving 150 Chinese patients and 131 controls indicated that HP seropositivity is not associated with the risk of IS and its subtypes.12 Nevertheless, several studies have reported that chronic HP-I is positively associated with the risk of IS.9–10,18–19 A case-control study involving 62 acute IS and 143 healthy controls by Sawayama et al. suggested that HP seropositivity is
significantly associated with an increased risk of IS, particularly that caused by small artery occlusion.9 A meta-analysis by Wang et al. revealed that chronic HP-I is significantly associated with an increased risk of IS, particularly noncardioembolic IS.10The positive association was also reported by 2 other studies.18–19 The presence of specific HP DNA in human atherosclerotic plaques detected using a PCR were also reported.20–21
The mechanisms by which chronic HP-I increases the risk of IS are still not
completely understood. Previous animal and epidemiological studies have indicated that chronic inflammation and autoimmune processes caused by chronic HP-I
promote atherosclerosis and the incidence of atherosclerosis-related diseases, such as stroke and coronary artery disease.22–24 Most inflammatory reactions have been attributed to cytokines, such as interleukins, which are responsible for the upregulation of adhesion molecules, recruitment and activation of leucocytes, promotion of leukocyte-endothelium interaction, and conversion of the local endothelium to a prothrombotic state.25 A higher value of plasma fibrinogen concentration was observed in HP-infected Cag A-positive stroke patients than in HP-negative controls, suggesting that plasma fibrinogen may play a role in IS.8,26–28 Fibrinogen is an acute phase protein and its level strongly corresponds with the process of atherogenesis. Fibrinogen seems to participate directly in the earlier phases of atherosclerotic plaque formation and arterial thrombosis. Moreover, fibrinogen is a vital component of acute and chronic inflammatory responses.29–30
The use of a nationwide population-based dataset that provides a sufficient sample size and statistical power to explore the link between HP and IS is a particular strength of this study. In addition, the patients in our study displayed a wide range of demographic characteristics, which enabled stratified analyses to be performed
according to sex, age, and comorbidities. Nevertheless, this study has limitations. First, the principal concern is the degree of accuracy in coding the HP-I and
IS. Second, detailed information, such as data on smoking habits, body mass index, socioeconomic status, and family history, and Cag-A strains are not available in the NHIRD. All of these variables are major risk factors for stroke. All of these variables are possible risk factors for IS. To minimize confounding from smoking habit factors, we have included in the data analysis with smoking related disorders such as coronary artery disease, COPD, and asthma for adjustment. The over all measured adjusted IS risk associated with changed little from the crude risk. In addition less than 5% women are smoker in Taiwan, the IS risk associated with
HP-I was greater for women than for men. However, because NHIRD covers
almost the entire population of Taiwan and the reimbursement policy is
universally the same. It is likely that the distribution of influence would also be the same between the study and control groups. Third, the database does not include body mass index (BMI) information so we excluded people with Triple H (hypertension, hyperlipidemia, hyperglycemia (DM)) to reduce the influence of obesity as Triple H and obesity is highly correlated. We acknowledge that this is a limitation of the present study.Fourth Third, evidence derived from a cohort study is generally of a lower quality than that derived from randomized control trials.
A cohort study design is subject to numerous biases regarding confounding adjustment. Despite our meticulous study design using adequate controls for confounding factors, bias may have occurred in unmeasured and unknown confounders.
Conclusion
In summary, this study indicated that chronic HP-I is significantly associated with an increased risk of IS, particularly nonembolic IS. Anti-HP therapy may have a
beneficial influence on IS prevention. An additional ideal prospective trial that examines the association of HP-I with IS, involving antibacterial and
References
1. Marshall BJ. Unidentified curved bacilli on gastric epithelium in active chronic gastritis. Lancet 1983; 1: 1273-1275
2. Suerbaum S, Michetti P. Helicobacter pylori infection. N Engl J Med 2002; 347:1175–1186
3. Ford AC, Axon AT. Epidemiology of Helicobacter pylori infection and public health implications. Helicobacter 2010;15(Suppl 1):1–6
4. Matysiak-Budnik T, Megraud F. Epidemiology of Helicobacter pylori infection with special reference to professional risk. J Physiol Pharmacol 1997; 48: 3-17 5. Cavaleiro-Pinto M, Peleteiro B, Lunet N, Barros H. Helicobacter pylori infection
and gastric cardia cancer: systematic review and meta-analysis. Cancer Causes Control 2011;22:375–387
6. Ross R. Atherosclerosis--an inflammatory disease. N Engl J Med. 1999;340: 115-26.
7. Markus HS, Mendall MA. Helicobacter pylori infection: a risk factor for ischaemic cerebrovascular disease and carotid atheroma. J Neurol Neurosurg Psychiatry 1998; 64:104–107
8. Majka J, Rog T, Konturek PC, Konturek SJ, Bielanski W, Kowalsky M, et al. Influence of chronic Helicobacter pylori infection on ischemic cerebral stroke risk factors. Med Sci Monit 2002;8: CR675–684
9. Sawayama Y, Ariyama I, Hamada M, Otaguro S, Machi T, Taira Y, et al. Association between chronic Helicobacter pylori infection and acute ischemic stroke: Fukuoka Harasanshin Atherosclerosis Trial (FHAT). Atherosclerosis 2005;178:303–309
10. Wang ZW, Li Y, Huang LY, Guan QK, Xu da W, Zhou WK, et al. Helicobacter
pylori infection contributes to high risk of ischemic stroke: evidence from a meta-analysis. J Neurol 2012;259:2527-37
11. Heuschmann PU, Neureiter D, Gesslein M, Craiovan B, Maass M, Faller G, et al. Association between infection with Helicobacter pylori and Chlamydia
pneumoniae and risk of ischemic stroke subtypes: Results from a population-based case-control study. Stroke 2001;32:2253–2258
12. Yang X, Gao Y, Zhao X, Tang Y, Su Y. Chronic Helicobacter pylori infection and ischemic stroke subtypes. Neurol Res 2011;33:467–472
13. The top 10 causes of death, World Health Organization.
http://www.who.int/mediacentre/factsheets/fs310/en/
14. World Health Organization (2008). The Global Burden of Disease: 2004 Update. Geneva: World Health Organization.
15. Di Carlo A. Human and economic burden of stroke. Age Ageing. 2009;38: 4–5 16. Gunarathne A, Patel JV, Gammon B, Gill PS, Hughes EA, Lip GY. Ischemic
ethnicity-related clinical features. Stroke 2009 40:e415–e423
17. Cheng TM. Taiwan’s National Health Insurance system: high value for the dollar. In Okma, K.G.H. and Crivelli, L. ed. Six Countries, Six Reform Models: The Health Reform Experience of Israel, the Netherlands, New Zealand,
Singapore, Switzerland and Taiwan. New Jersey: World Scientific, 2009, pp.71-204.
18. Masoud SA, Arami MA, Kucheki E. Association between infection with
Helicobacter pylori and cerebral noncardioembolic ischemic stroke. Neurol India 2005;53: 303–306; discussion 306–307
19. Park MH, Min JY, Koh SB, Kim BJ, Park MK, Park KW, et al. Helicobacter pylori infection and the CD14 C(-260)T gene polymorphism in ischemic stroke. Thromb Res 2006;118:671–677
20. Amerisio SF, Fridman EA, Leiguarda RC, Sevlever GE. Detection of
Helicobacter pylori in human carotid atherosclerotic plaques. Stroke 2001; 32: 385-391
21. Kowalski M, Rees W, Konturek PC, Grove R, Scheffold T, Meixner H, et al. Detection of Helicobacter pylori specific DNA in human atheromatous coronary arteries and its association to prior myocardial infarction and unstable angina. Digest Liver Dis 2002; 34: 398-402
paraoxonase-1 activity in Helicobacter pylori infected subjects. Atherosclerosis 2008;196:270–274
23. Ayada K, Yokota K, Kobayashi K, Shoenfeld Y, Matsuura E, Oguma K. Chronic infections and atherosclerosis. Clin Rev Allergy Immunol 2009;37:44–48
24. Matsuura E, Kobayashi K, Matsunami Y, Shen L, Quan N, Makarova M, et al. Autoimmunity, infectious immunity, and atherosclerosis. J Clin Immunol 2009;29:714–721
25. Clark WM. Cytokines and reperfusion injury. Neurology 1997; 49(suppl 4): 10-14
26. Patel P, Carrington D, Strachan DP, Leatham E, Goggin P, Northfield TC, et al. Fibrinogen: a link between chronic infection and coronary heart disease. Lancet 1994; 34: 1634-1635
27. Zito F, Di Castelnuovo A, D'Orazio A, Negrini R, De Lucia D, Donati MB, et al. Helicobacter pylori infection and the risk of myocardial infarction: role of fibrinogen and its genetic control. Thromb Haemost 1999; 82: 14-18
28. De Bastiani R, Gabrielli M, Ubaldi E, Benedetto E, Sanna G, Cottone C et al.
High prevalence of Cag-A positive H. pylori strains in ischemic stroke: a primary care multicenter study. Helicobacter. 2008;13:274-7.
29. Smith EB. Fibrinogen, fibrin and fibrin degradation products in relation to atherosclerosis. Clin Haemathol 1986; 15: 355-370
30. Gabay C, Kushner I. Acute-phase proteins and other systemic responses to inflammation. N Engl J Med 1999; 340: 448-454.
Figure Legend:
Figure 1. Cummulative incidence of non-embolic ischemic stroke in patients with and without helicobactor pylori infection
Table 1 Demographic characteristics and comorbidity in patient with and without Helicobactor pylori infection
Variable
Helicobactor pylori infection
p-value No Yes N =69,328 N =17,332 Sex n(%) n(%) Female 26,016(37.5) 6,504(37.5) 0.99 Male 43,312(62.5) 10,828(62.5) Age, mean(SD) 57.0(16.9) 57.4(16.8) 0.006# Stratified age ≤35 7,420(10.7) 1,855(10.7) 0.99 36-50 16,608(24.0) 4,152(24.0) 51-65 20,256(29.2) 5,064(29.2) 65+ 25,044(36.1) 6,261(36.1) Comorbidity Diabetes 8,108(11.7) 3,046(17.6) <0.0001 Hypertension 7,063(10.2) 4,598(26.5) <0.0001 Hyperlipidemia 1,680(2.42) 1,507(8.69) <0.0001 Congestive heart failure 2,891(4.31) 1,909(11.0) <0.0001 Coronary artery disease 3,682(5.31) 2,078(12.0) <0.0001 Atrial fibrillation 651(0.94) 316(1.82) <0.0001
COPD 1929(2.78) 1251(7.22) <0.0001
Asthma 1291(1.86) 899(5.19) <0.0001
Table 2 The risk of ischemic stroke compared to study subjects without helicobactor pylori infection in Cox proportional hazard regression
Helicobactor pylori infection
Compared to non-HPI
No Yes
Variables Stroke Stroke Stroke Stroke Crude HR *
(95% CI)
Adjusted HR† (95% CI) Event Rate# Event Rate#
All 2,103 8.45 837 14.8 1.76(1.68, 1.83)*** 1.52(1.40, 1.65)*** Subtype Embolic ischemic stroke 35 0.14 10 0.18 1.26(1.18, 1.35)*** 0.93(0.45, 1.91) Non-embolic ischemic stroke 2,068 8.31 827 14.7 1.76(1.69, 1.84)*** 1.53(1.41, 1.67)*** Sex Male 1381 8.75 506 14.2 1.63(1.54, 1.72)*** 1.45(1.31, 1.61)*** Female 722 7.94 331 15.9 2.00(1.87, 2.14)*** 1.65(1.44, 1.89)***
Rate#, incidence rate, per 1000 person-years; Crude hazard ratio (HR)*: relative hazard ratio; Adjusted HR†: multivariable analysis including age, sex, and
comorbidities of diabetes, hypertension, hyperlipidemia, congestive heart failure, coronary artery disease, atrial fibrillation, COPD and asthma; *p<0.05, **p<0.01, ***p<0.001
Table 3. Cox model estimated hazard ratios of stroke in relation to number of admissions visits due to helicobactor pylori infection
Stroke Compared to non-HPI
No. of Cases Crude HR
* (95% CI) Adjusted HR† (95% CI) Ischemic stoke Number of admissions
0 (Non-infected H. pylori) 2,103 1(Reference) 1(Reference)
1 785 1.72(1.58, 1.86)*** 1.49(1.37, 1.62)***
≥2 52 2.65(2.01, 3.49)*** 2.26(1.71, 2.98)***
P for trend p < 0.0001
Embolic ischemic stroke Number of admissions
0 (Non-infected H. pylori) 35 1(Reference) 1(Reference)
1 10 1.30(0.65, 2.63) 0.97(0.47, 2.00)
≥2 0 -
-P for trend p =0.72
Non-embolic ischemic stroke Number of admissions
0 (Non-infected H. pylori) 2,068 1(Reference) 1(Reference)
1 775 1.72(1.59, 1.87)*** 1.50(1.38, 1.64)***
≥2 52 2.69(2.05, 3.55)*** 2.31(1.75, 3.05)***
P for trend p < 0.0001
Crude hazard ratio (HR)*: relative hazard ratio; Adjusted HRs†: adjusted for age, sex, and comorbidities of diabetes, hypertension, hyperlipidemia, congestive heart failure, coronary artery disease, atrial fibrillation, COPD and asthma; *p<0.05, **p<0.01, ***p<0.001
Table 4. Cox model with hazard ratios and 95% confidence intervals of non-embolic ischemic stroke associated with helicobactor pylori infection and covariates
Crude* Adjusted†
Variable HR (95%CI) HR (95%CI)
Stratify age ≤35 1.00 (Reference) 1.00 (Reference) 36-50 4.45 (2.57, 7.71)*** 4.27 (2.47, 7.39)*** 51-65 13.0 (7.66, 22.2)*** 11.3 (6.62, 19.2)*** 65+ 52.0 (30.8, 87.9)*** 37.4 (22.1, 63.4)*** Sex Male 1.04 (0.97, 1.13) -
-Female 1.00 (Reference) 1.00 (Reference)
Baseline co-morbidities (yes vs no) Helicobactor pylori infection 1.76 (1.63, 1.91)*** 1.48 (1.37, 1.61)*** Diabetes 2.82 (2.59, 3.06)*** 1.54 (1.41, 1.68)*** Hypertension 4.18 (3.88, 4.52)*** 1.63 (1.48, 1.80)*** Hyperlipidemia 2.33 (2.02, 2.68)*** 1.03 (0.89, 1.20)
Congestive heart failure 4.33 (3.93, 4.77)*** 1.20 (1.06, 1.35)**
Coronary artery disease 3.43 (3.12, 3.78)*** 1.15 (1.02, 1.28)*
Atrial fibrillation 4.33 (3.54, 5.30)*** 1.36 (1.10, 1.67)** COPD 3.90 (3.46, 4.39)*** 1.44 (1.26, 1.64)*** Asthma 2.74 (2.34, 3.21)*** 1.05 (0.89, 1.24)
Crude hazard ratio (HR)*: relative hazard ratio;
†Adjusted HR: multivariable analysis including for Stratify age, and comorbidities of diabetes, hypertension, hyperlipidemia, congestive heart failure, coronary artery disease, atrial fibrillation, COPD and asthma