1
中 國 醫 藥 大 學
1專題研究計畫成果報告
2 3計畫名稱:以調控缺氧誘發因子(HIF-1α)的觀點探討
4低能雷射治療慢性發炎及疼痛的分生機
5制
6 已經發表於 7Hsieh YL, Chou LW, Chang PL, Yang CC, Kao MJ, Hong CZ. Low-level laser therapy alleviates 8
neuropathic pain and promotes function recovery in rats with chronic constriction injury-possible 9
involvements in hypoxia-inducible factor 1α (HIF-1α). J Comp Neurol. 2012 Feb 20. doi: 10
10.1002/cne.23072. [Epub ahead of print] 11
計畫編號:CMU99-TC-23
12 13執行期限:100 年 04 月 01 日至 101 年 03 月 31 日
14單位名稱:物理治療學系
15主持人:謝悅齡
16 17中 華 民 國
101 年 04 月 14 日
182
Abstract
19
Background. Nerve inflammation plays an important role in the development and progression 20
of neuropathic pain after chronic constrictive injury (CCI). Recent studies explored 21
hypoxia-inducible factor 1α (HIF-1α) in the process of inflammation. Low-level laser therapy 22
(LLLT) has been suggested to benefit treatment of pain disorders, but few data directly support 23
LLLT for neuropathic pain. Objective. We investigated the effect of LLLT on accumulation of 24
hypoxia-inducible factor-1 alpha (HIF-1α), proinflammatory cytokines tumor necrosis factor-α 25
(TNF-α), and interleukin-1β (IL-1β) for controlling neuropathic pain, as well as on activation 26
of vascular endothelial growth factor (VEGF) and nerve growth factor for promoting 27
functional recovery in rat model of CCI. Methods. CCI was induced by placing four loose 28
ligatures around the sciatic nerve of rats. LLLT (660 nm, 9 J/cm2) at CCI sites was performed 29
after 7 days of CCI. Effects of LLLT in CCI animals were determined by measuring 30
mechanical paw withdrawal threshold (MPWT), sciatic, tibial and peroneal function indexes 31
(SFI, TFI and PFI), and histopathological and immunoassay analyses. Results. Our results 32
demonstrated that LLLT significantly improved MPWT, SFI, TFI and PFI after CCI. LLLT 33
also significantly reduced overexpressions of HIF-1α, TNF-α and IL-1β and increased the 34
amounts of VEGF, NGF and Schwann cells. Conclusions. LLLT can modulate HIF-1α activity 35
and may represent a novel, clinically applicable therapeutic approach for improvement of 36
tissue hypoxia/ischemia and inflammation in nerve entrapment neuropathy as well as for 37
promotion of nerve regeneration, which may lead to sufficient morphologic and functional 38
recovery of the peripheral nerve. 39
40
Key Words: Chronic constrictive injury-Low-level laser therapy-Hypoxia-inducible factor
41
1α-Neuropathic pain-Functional recovery
3
Introduction
43
Neuropathic pain is a common sequela initiated by a primary lesion of the peripheral or 44
central nervous system (Baron, 2000, Zimmermann, 2001). In previous studies, the relationship 45
between proinflammatory cytokines, such as tumor necrosis factor-α (TNF-α), interleukin 1 46
(IL-1) released by inflammatory cells on their activation and the development of hyperalgesia 47
and allodynia in neuropathic pain has been identified (Sommer and Kress, 2004, Sommer and 48
Schäfers, 2004, Li et al., 2011, Liou et al., 2011). These results support the notion that nerve 49
inflammation plays an important contributory role in the development and progression of 50
neuropathic pain. Experimentally, various animal models of peripheral neuropathy have been 51
developed. Chronic constriction injury (CCI) of the sciatic nerve with loose ligatures is the 52
most widely used model for peripheral neuropathy and neuropathic pain (Bennett and Xie, 53
1988, Kingery et al., 1993), simulating the clinical condition of chronic nerve compression as 54
occurs in nerve entrapment neuropathy or spinal root irritation by a lumbar disk herniation 55
(Zimmermann, 2001). 56
Hypoxia-inducible factor-1α (HIF-1α) is a transcription factor that is increased in 57
conditions of hypoxia, ischemia and inflammation (Fraisl et al., 2009). HIF-1α is also thought 58
to be essential in maintaining inflammatory processes by promoting the production of 59
proinflammatory cytokines, including TNF-α and IL-1β (Takeda et al., 2009). HIF-1α has been 60
identified as a pivotal transcription factor linking the inflammatory pathways (Dehne and 61
Brune, 2009). Inhibition and/or down-regulation of these molecules may exert anti-hypoxic 62
and anti-inflammatory effects. Therefore, inhibiting HIF-1α accumulation may be a novel 63
therapeutic strategy for neuropathic inflammation. 64
Many experimental and clinical studies have also reported positive effects of low-level 65
laser therapy (LLLT) for promoting the repair processes of peripheral nerve by increasing 66
vascular endothelial growth factor (VEGF) and nerve growth factor (NGF) secretions (Byrnes 67
et al., 2005, Gigo-Benato et al., 2005, Hou et al., 2008, Rochkind, 2009, Rochkind et al., 2009, 68
Gigo-Benato et al., 2010), and by inhibiting the inflammation through reduction of 69
pro-inflammatory cytokines (Albertini et al., 2007). However, to date, there is little evidence 70
directly supporting the anti-allodynia effects of LLLT in neuropathic pain. In this study, 71
therefore, the effects of LLLT on management of neuropathic pain after CCI in sciatic nerve of 72
rat were investigated and possible biological mechanisms through which LLLT may exert its 73
action on functional recovery of peripheral nerve were analyzed. We hypothesized that LLLT 74
can decrease pro-inflammatory cytokines, reduce HIF-1α accumulation, and then promote 75
expressions of VEGF and NGF in the sciatic nerve proximal to the site of CCI on improvement 76
of neuropathic pain and functional recovery. 77
78
MATERIALS AND METHODS
7980
General Design
81Neuropathy was induced in all animals by CCI surgery. After surgery, animals (n=40) 82
were divided randomly into four groups (Figure 1) based on the nerve surgery and treatment 83
administration: (1) the CL group (n=10), which consisted of CCI animals that received LLLT; 84
(2) CsL group (n=10), which consisted of CCI animals that received sham-irradiated LLLT; (3) 85
sCL group (n=10), which consisted of sham-operated CCI animals that received LLLT; and (4) 86
sCsL group (n=10), which consisted of sham-operated CCI animals that received 87
sham-irradiated LLLT. Treatments of LLLT or sham-irradiation were given for consecutive 7 88
days. The evaluation instruments were mechanical paw withdrawal threshold (MPWT), sciatic 89
functional index (SFI), tibial functional index (TFI), peroneal functional index (PFI), histology, 90
4 immunohistochemistry and immunoassays. Pain and functional assessments were performed 91
the day before (pre-op, at day 0), immediately after operation (post-op, at day 1), at 7 days (7d 92
post-op, at day 7) after surgery and after the 7-day treatment (post-tr, at day 14). Animals were 93
sacrificed for assessments of histopathology and immunoassays the day after completing the 94
treatments. A flow diagram of the experimental design is presented in Figure 1. 95
96
Animals
97Experiments were performed on adult male Sprague–Dawley rats (SD, 250 to 300 g, 98
purchased from BioLASCO Co., Ltd, Taiwan). Ambient temperature was maintained at 22 to 99
24 °C and the animals were kept on an artificial 12-h light–dark cycle in the Animal Center of 100
China Medical University. The light period began at 7:00 a.m. with food and water available 101
ad libitum up to the time of testing. Efforts were made to minimize discomfort and reduce the 102
number of animals used. The ethical guidelines of the International Association for Study of 103
Pain in Animals were followed (Zimmermann, 1983). All experimental procedures were 104
approved by the China Medical University Committee on Animal Care and Use. 105
106
Chronic Constriction Injury of Sciatic Nerve
107Following the procedure originally proposed by Bennet and Xie (Bennett and Xie, 1988) 108
adapted for mice, CCI of sciatic nerve was used as the model of peripheral nerve injury for 109
evoking neuropathic pain symptoms. Surgery was performed under anesthesia with 4% 110
isoflurane in liquid form for inhalation (AErrane, Baxter Healthcare of Puerto Rico, PR). Using 111
a double-headed operating microscope, the sciatic nerve on one randomly selected side was 112
exposed by skin incision along the femur and separation of biceps femoris and superficial 113
gluteal muscles. At the middle third of the sciatic nerve, four ligatures with 4-0 chromic gut 114
thread (Ethicon, USA) were tied loosely around the nerve with inter-ligation spacing of about 1 115
mm. The wound of muscle layers (with 4/0 reabsorbable suture, Ethicon, USA) and skin (with 116
3/0 non-reabsorbable suture, Ethicon, USA) were then sutured and closed to allow recovery. 117
Sham-operated CCI animals underwent the same procedures. Branches were dissociated and 118
without any lesion for comparison 119
. 120
Low-Level Laser Irradiation
121Seven days after surgery, a continuous 660-nm Ga-Al-As diode laser (Aculas-Am series, 122
Multi-channel LLLT system; Konftec Corporation, Taipei, Taiwan) was used in this study. 123
After sterilization, the hand-held delivery probe was placed lightly on the skin surface directly 124
above the loose ligation sciatic nerve at 4 spots / per area. The spot size was approximately 0.2 125
cm2. The output power of the laser irradiation was 30 mW per session for 60 sec/ per spot for 7 126
consecutive days. The energy density was 9 J/cm2. The output of the equipment was routinely 127
checked by the Laser Check Power Meter (Coherent, Santa Clara, CA, USA). A similar 128
procedure was applied to the control group with sham-irradiated LLLT with the output power 129
of laser irradiation adjusted to 0. 130
131
Mechanical Allodynia
132The assessment of mechanical allodynia was performed by a MPWT which was measured 133
by nociceptive thresholds to stimulate von Frey filaments at pre-op, post-op, 7d post-op and 134
post-tr. The test consisted of evoking a hind paw flexion reflex with a handheld force 135
transducer (electronic von Frey anesthesiometer, IITC Inc., CA, USA) adapted with a 0.5 mm2 136
5 polypropylene tip. In a quiet room, the rats were placed in acrylic cages (32 × 22 × 27 cm high) 137
with a wire grid floor for 15-30 min habituation prior to testing. The polypropylene tip was 138
perpendicularly applied to the central area of the hind paw with sufficient force to bend the 139
filaments into an “S” shape for 3-4 sec. The test consisted of poking a hind paw to provoke a 140
flexion reflex followed by a clear flinch response after paw withdrawal. Testing was initiated 141
with the filament corresponding to 20 log of force (g). The filaments were applied with a 142
gradual increase in pressure until a withdrawal reflex response was finally detected from the 143
animal. The response to this filament was defined if a series of weaker or stronger filaments 144
would be tested. The weakest filament able to elicit a response was taken to be the MPWT (g). 145
The intensity of the pressure was recorded and the final value for the response was obtained by 146
averaging five measurements. 147
148
Assessments of Functional Recovery
149The degree of recovery was monitored by evaluating the rats’ walking patterns in order to 150
obtain SFI, TFI, and PFI according to the method described by Bain et al. (Bain et al., 1989). 151
Before the recording, a few conditioning trials were performed to accustom the animals to the 152
track. All animals underwent preoperative walking-track analysis. Briefly, the plantar surfaces 153
of both hind paws were wetted with red ink in order to obtain clear footprints, and they were 154
allowed to walk along a specially designed alley (84 cm length × 8.5 cm width) lined with 155
scaled paper. Recordings continued until five measurable footprints had been collected. The 156
data used for calculations were taken from the footprint as follows: (1) distance from the heel 157
to the third toe, the print length (PL); (2) distance from the first to fifth toe, the toe spread (TS); 158
and, (3) distance from the second to the fourth toe, the intermediary toe spread (ITS). All three 159
measurements were taken from the experimental (E) and normal (N) sides. Prints were then 160
calculated using the following formulae (Bain et al., 1989): (1) SFI = -38.3 ([EPL−NPL]/NPL) + 161
109.5 ([ETS−NTS]/NTS) + 13.3 ([EIT−NIT]/NIT) - 8.8; (2) TFI = -37.2 ([EPL−NPL]/NPL) + 104.4
162
([ETS−NTS]/NTS) + 45.6 ([EIT−NIT]/NIT) - 8.8; (3) PFI = 174.9 ([EPL−NPL]/NPL) + 80.3 163
([ETS−NTS]/NTS) - 13.4. Values of these tests equal to -100 indicated total impairment of the 164
sciatic, posterior tibial and peroneal nerves, whereas SFI, TFI and PFI oscillating around 0 165
were considered to reflect normal function (Bain et al., 1989). 166
167
Sciatic Nerve Obtainment and Tissue Preparations
168After completing the treatments at day 14, rats were sacrificed after being deeply 169
anaesthetized with saturated KCl (300 g/ml, i.p.), then sciatic nerve segment was harvested, 170
which included the four ligatures as well as 1 cm of sciatic nerve proximal to the site of CCI. 171
The biopsied nerve specimens were divided into two portions for histopathology and 172
immunoassays. For histopathological assessments, nerve specimens randomly selected from 5 173
animals of each group were fixed in 10% neutral formalin, and embedded in paraffin for 12 h 174
at room temperature. All of the biopsied nerve specimens obtained from each animal for 175
immunoassays were immediately frozen in liquid nitrogen and stored at −80℃ for later 176
homogenization and subsequent assay of cytokine and protein expression. The homogenization 177
buffer was freshly prepared by adding protease inhibitor (P8340 cocktail Sigma, NY, USA) to 178
T-PER™ Tissue Protein Extraction Reagent (Pierce Chemical Co., USA) and centrifuged for 179
40 min. The supernatant was extracted and stored at −80 °C. 180
181
Histopathological, Immunohistochemical and Immunofluorescent Stainings
182The specimens were submitted to diafanization with xylene, then dehydrated by graded 183
ethanol, embedded in paraffin and cut in 4-μm-thick sections longitudinally using a microtome. 184
6 Ten consecutive longitudinal resections contiguous to a maximum diameter were chosen for 185
data collection and subsequent comparisons. Histopathologic changes were evaluated on 186
sections stained with hematoxylin and eosin (H&E, Muto Pure Chemicals Co., Ltd., Tokyo, Japan) to 187
determine infiltration of inflamed cells in nerves. Slides were examined by a light microscope 188
and photographed using the Automatic Photomicrographic System PM10SP (Olympus, PA, 189
USA). The area of inflamed cell and nerve nuclei was measured in a 200× magnification field 190
by an ImageScope program (Aperio, Vista, CA, USA). 191
For immunohistochemical staining, the slides of sciatic nerve sections were first incubated 192
overnight at 4℃ with the monoclonal mouse antibodies, including anti-HIF-1α (1:200, 193
Thermo, CA, USA), anti-monocytes/macrophages (ED1, 1:200, Millipore, CA, USA) primary 194
antibodies, with the polyclonal rabbit antibodies, including anti-Schwann cells (S100, 1:400, 195
DakoCytomation, Denmark) and anti-VEGF (1:200, Abbiotec, CA, USA) primary antibodies, 196
as well as with rabbit monoclonal anti-NGF-β (1:2500, Millipore, CA. USA) primary antibody. 197
After washing three times in PBS, the nerve sections were then incubated with biotinylated 198
goat anti-mouse and goat anti-rabbit IgG secondary antibody (Jackson ImmunoResearch 199
Laboratories, Inc., West Grove, PA, USA) for 1 hour at room temperature. Following washing 200
with phosphate buffer three times, sections were incubated with a streptavidin-horseradish 201
peroxidase conjugate (Jackson ImmunoResearch Laboratories, Inc., West Grove, PA, USA). 202
Finally, sections were visualized as brown precipitates yields using 3,3′-diaminobenzidine 203
(DAB, 0.2 mg/ml, Pierce, Rockford, IL, USA) as a substrate and then counterstained with 204
hematoxylin. Negative control sections received the same treatment without the addition of 205
primary antibody. Slides were examined at a minimum of five sections in the more 206
representative fields using a light microscope and then photographed. The area sizes of positive 207
nuclear and cytoplasmic staining cells for HIF-1α, ED1, S100, VEGF and NGF were measured 208
in a 200× magnification field using the ImageScope program (Aperio, Vista, CA, USA). Ten 209
fields of each slide were calculated and repeated three times for statistical analysis. Results are 210
expressed as the proportion (%) of positive immunoreactive area per total stained area. 211
To observe coexpression of HIF-1α with infiltrated inflammatory cells in the injured nerve, 212
we incubated the sections with rabbit polyclonal anti-HIF-1α (1:200, Santa Cruz Biotechnology, 213
CA, USA) and mouse monoclonal anti-monocytes/macrophages (ED1) (1:200, Millipore, CA, 214
USA) overnight at 4°C under gentle agitation. Sections were then incubated with the respective 215
secondary antibodies (Jackson ImmunoResearch Laboratories, Inc., West Grove, PA, USA), 216
goat anti-rabbit IgG fluorescein-conjugated (FITC, 1:1000) and goat anti-mouse IgG 217
rhodamine-conjugated (TRITC, 1:1000) secondary antibodies for 2 hours at room temperature. 218
Following washing with phosphate buffer three times, sections were incubated with a 219
streptavidin-horseradish peroxidase conjugate (Jackson ImmunoResearch Laboratories, Inc., 220
West Grove, PA, USA). Finally, the sections were washed three times in PBS and then 221
counterstained with 4′,6-diamidino-2-phenylindole (DAPI, Molecular Probes, Invitrogen 222
Corporation, Carlsbad, CA, USA) to reveal cell nuclei. Images were obtained using a 223
conventional fluorescence microscope (Fluoview X; Olympus, Tokyo, Japan). All of 224
quantitative image analyses were assessed by two independent observers who were blinded to 225
the origin of the sections to avoid bias from interobserver variability. 226
227
Enzyme-Linked Immunosorbent Assay
228The amounts of TNF-α, IL-1β and BDNF concentrations in the supernatants were 229
determined using the DuoSet® ELISA Development kit (R&D Systems, Minneapolis, MN, 230
USA). Nerve extracts were incubated in 96-well plates coated with mouse anti-rat TNF-α and 231
goat anti-rat IL-1β. After washing at each step, biotinylated anti-rat TNF-α and anti-rat IL-1β 232
7 and then streptavidin-HRP were added and incubated in accordance with the manufacturer's 233
instructions. After washing, a NeA-Blue (Tetramethylbenzidine) Substrate solution (Clinical 234
Science Products, Inc., Mansfield, MA, USA) was added to each well. The enzyme reaction 235
was terminated by adding stop solution (2N H2SO4). The levels of TNF-α and IL-1β were
236
assessed by a reader (Thermo Scientific Multiskan EX, Finland) using a 450 nm filter and 237
normalized with an abundance of standard solution. Data were then analyzed using Ascent 238
Software (Thermo Scientific Ascent Software, Finland) and a four-parameter logistics curve-fit. 239
Data are expressed in pg/mg protein of duplicate samples. 240
241
Western Blot Analysis
242Protein determination was performed by modified Lowry protein assays. Equal amounts 243
of protein were loaded and separated in 10% Tris-Tricine SDS-PAGE gels. The resolved 244
proteins were transferred onto PVDF membranes ((Millipore, Bedford, MA, USA). The 245
membranes were blocked in 5% non-fat milk for 1 hour at room temperature, and incubated 246
overnight at 4 °C with mouse monoclonal anti-HIF-1α (1:500, Novus Biologicals, CA, USA), 247
rabbit polyclonal anti-VEGF antibody (1:2500, Abbiotec, CA, USA), and rabbit monoclonal 248
anti-NGF-β (1:2500, Millipore, CA. USA) primary antibody. The blots were then incubated 249
with the horseradish peroxidase-conjugated goat anti-mouse and anti-rabbit IgG secondary 250
antibody (1:20000, Jackson ImmunoResearch Laboratories, Inc., West Grove, PA, USA) for 1 251
hour at room temperature. Signals were finally visualized using enhanced chemiluminescence 252
detection system (Fujifilm LAS-3000 Imager, Tokyo, Japan) and the blots were exposed to 253
X-ray films. All Western blot analyses were performed at least three times, and consistent 254
results were obtained. Immunoreactive bands were analysed using a computer-based 255
densitometry Gel-Pro Analyzer (version 6.0, Media Cybernetics, Inc. USA). Grey levels, 256
obtained by densitometric analysis of immunoreactive bands, were normalized on β-actin. 257
258
Statistical Analysis
259Results were averaged for each group and values were expressed as mean ± S.E.M. The 260
data obtained from MPWT, SFI, TFI and PFI were analyzed using mixed-design, two-way 261
repeated-measures ANOVA performed with group as a between-subjects factor and time as a 262
within-subjects factor. The Bonferroni adjustment was examined post hoc for multiple 263
comparisons at individual time points between groups. One-way ANOVA was performed for 264
comparison of individual group means for assessing parametric results of histopathology and 265
immunoassay. The Dunnett test was performed for multiple comparisons between experimental 266
and control groups at the post-tr time point. A P value of < .05 was considered statistically 267
significant. All data were analyzed using SPSS version 10.0 for Windows (SPSS Inc., IL, 268 USA). 269 270
RESULTS
271 272Effects of Low-Level Laser Therapy on Mechanical Allodynia
273After surgery, there were significant differences in MPWT among time points in each 274
group (P < .0001). MPWT was significantly decreased at post-op and 7d post-op conditions in 275
animals that received CCI when compared with that of the pre-op condition (both were P < 276
0.001). In animals that received sham-operated CCI, MPWT of post-op compared to that of 277
pre-op condition was significantly decreased (P < 0.0001), whereas there was no significant 278
difference between the 7d post-op and pre-op condition (P=0.36). There were also significant 279
8 differences among the four groups at each time point (all were P < 0.0001, Figure 2A).
280
At the post-tr time point, there was a significant difference in MPWT compared with that 281
of the 7d post-op condition in CL group (P < .0001), but there were no significant differences 282
compared with values obtained in the CsL (P=0.59), sCL (P=0.22) and sCsL (P=0.98) groups. 283
The significant differences in MPWT were shown among CL, CsL, sCL and sCsL groups after 284
treatments (P < .0001). Significantly higher MPWT existed after LLLT treatment in CL group 285
compared with those in CsL groups after sham-irradiated LLLT treatment (P < .0001). 286
However, no significant difference was observed between sCL and sCsL groups (P=0.98). 287
288
Effects of Low-Level Laser Therapy on Functional Recovery
289After surgery, there were significant differences in SFI, TFI and PFI among time points in 290
each group. SFI, TFI and PFI values were around 0 at pre-op condition and decreased 291
significantly after surgery in all groups (P < .001). SFI and TFI were still significantly 292
decreased at 7d post-op condition in animals that received CCI when compared with those of 293
post-op (SFI: P=0.83; TFI: P=0.99), but PFI showed significant recovery (P < .0001). 294
However, in sham-operated CCI animals at 7d post-op condition, PFI values significantly 295
recovered and approached that of the pre-surgery condition (P = 0.99), and SFI and TFI were 296
significant increased compared with those of post-op conditions (both were P < .0001, Figure 297
2B-D). 298
At the post-tr time point, SFI, TFI and PFI values were significantly higher when 299
compared with those of 7d post-op in CL group (SFI: P=0.001; TFI: P=0.003; PFI=0.03), but 300
no significant differences were found in CsL (SFI: P=1.0; TFI: P=0.73; PFI: P=1.0). SFI, TFI 301
and PFI values in sCL and sCsL groups showed no significant difference from pre-op level (all 302
were P > .05). Significant differences in SFI, TFI and PFI were shown among CL, CsL, sCL 303
and sCsL groups (all were P < .0001). Significantly higher values of SFI, TFI and PFI existed 304
after LLLT treatment in CL group compared with those of sham-irradiation treatment in CsL 305
groups (SFI: P=0.001; TFI: P=0.004; PFI: P=0.002). 306
307
Effects of Low-Level Laser Therapy on
Inflammation
and Cytokines
308The results of H&E study showed there was pronounced infiltration of immune cells at 309
the site of CCI injury as compared with the site of sham-operated CCI (Figure 3A, 3B, 3C, 3D). 310
The percentages of nuclei in nerve contents were significantly different among the four groups 311
(P < .0001). The percentage of nuclei was significantly decreased and showed less 312
inflammation and cell infiltration in CL groups when compared with CsL group (Figure 3G). 313
Similar results were found for ED1 immunoreactivity which showed significant increases in 314
CsL group, but was reduced in CL group (Figure 3E, 3F and 3H). 315
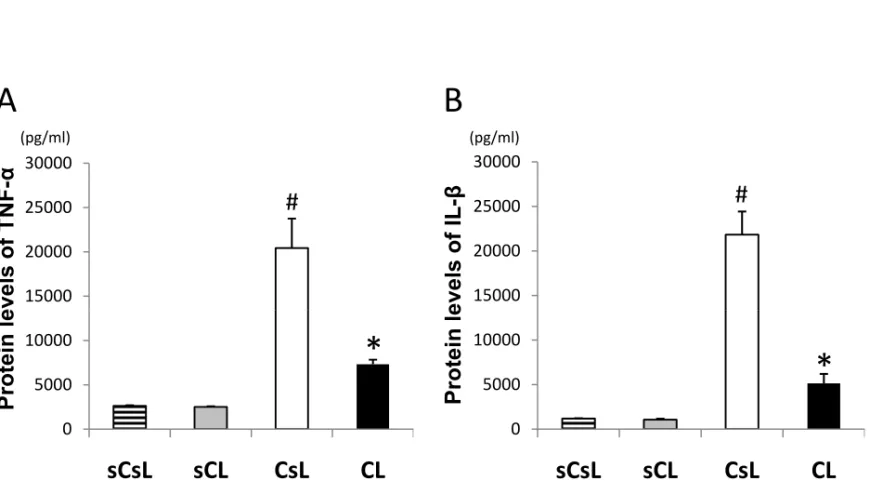
TNF-α and IL-1β of the sciatic nerve contents were significantly different among the four 316
groups (both were P < .0001). There were significantly higher levels of TNF-α and IL-1β in 317
CsL groups in comparison with those of sCsL and sCL groups (both were P < .0001). No 318
significant differences were observed between sCL and sCsL groups (P=1.0). There was a 319
significant reduction of these cytokines in the CL group when compared with CsL groups (P 320
< .0001), but no significant difference was found when compared with those of sCL (TNF-α: 321
P=0.29; IL-1β: P=0.39) or sCsL (TNF-α: P=0.33; IL-1β: P=0.28) groups (Figure 4).
322 323
Effects of Low-Level Laser Therapy on HIF-1
α
324
The expressions of HIF-1α immunoreactivity in sciatic nerves were significantly different 325
among the four groups (P < .0001). The results showed there were sparse HIF-1α-positive cells 326
in sCL and sCsL groups (Figure 5A, 5B) and no significant differences were found among 327
9
these groups (both were P > .05, Figure 5G). In the CsL group, overexpression of HIF-1α 328
immunoreactivity was observed and localized in both the nucleus and cytoplasm of the injured 329
samples at higher-power magnification (Figure 5C). The accumulation of HIF-1α-positive cells 330
was decreased significantly in CL group when compared with CsL group (P=0.006, Figure 5D). 331
Double staining with HIF-1α and ED1 showed the ED1 immunoreactive cells which were 332
morphologically consistent with macrophages, mainly by inflammatory infiltration of the 333
inflamed nerve coexpressed by the specific HIF-1α immunoreactivity. The number of double 334
positive cells was decreased in CL groups when compared with those in CsL group (Figure 5E 335
and 5J). The observed HIF-1α expressions were further supported at the protein level assay by
336
Western blotting. The levels of HIF-1α in sciatic nerve was shown as gray density percentages 337
(normalized on β-actin) in the form of a representative Western blotting (Figure 6H). The 338
protein levels of HIF-1α in sciatic nerve contents were significantly different among the four 339
groups (P < .0001). No significant differences were observed between sCL and sCsL groups (P 340
> .05). Significantly higher levels of HIF-1α level were found in CsL groups in comparison 341
with those of CL, sCsL and sCL groups (all were P < .0001). The protein levels of HIF-1α was 342
significantly decreased in CL group in comparison with CsL groups (P=0.006) and 343
approximated the levels of sCL control group (P=0.064). 344
345
Effects of Low-Level Laser Therapy on VEGF, NGF and Schwann Cells
346At day 14 after CCI, the constitutive expressions of VEGF and NGF in sciatic nerves 347
were significantly different among the four groups (VEGF: P < .0001; NGF: P=0.003). There 348
were no significant differences of VEGF and NGF expression between sCL and sCsL groups
349
(both were P > .05). After CCI, the expressions of these factors in the injured sciatic nerve
350
were slightly increased in CsL group as shown in Figures 6A and 6D, but the difference was of 351
non-significant when compared with those of sCsL groups (NGF: P=0.9; VEGF: P=0.22). As
352
expected, our results demonstrated that there were significant increases of VEGF and NGF in
353
CL groups compared with those in CsL group (VEGF: P=0.009; NGF: P=0.002, Figure 6B, 6C,
354
6E and 6F).Furthermore, as demonstrated in Figure 6I and 6J, the observed VEGF and NGF
355
immunoreactive expressions could be further supported at the protein level by Western blotting.
356
The protein levels of VEGF and NGF in sciatic nerve contents were also significantly different 357
among the four groups (VEGF: P < .0001; NGF: P < .0001). No significant differences were 358
observed between sCL and sCsL groups (both were P=1.0). The protein levels of VEGF and 359
NGF in CsL group also showed a slight elevation over 14 days after CCI surgery but the 360
calculation was not significant when compared with those of sCsL groups (NGF: P=0.18; 361
VEGF: P=0.07). There were significant increases of levels of VEGF and NGF in CL group 362
when compared with those of CsL groups (VEGF: P=0.009; NGF: P=0.002). Using S100 363
immunohistochemistry for Schwann cells, the S100 expression was decreased in injured nerve 364
in CsL group (Figure 6G), but increased in CL group (Figure 6H). The S100 immunoreactivity 365
in sciatic nerve contents was also significantly different among the four groups (P < .0001). 366
There was a significant decrease in S100 expression in CsL group when compared with values 367
seen in CL (P=0.005), sCL (P=0.035) and sCsL (P=0.027) groups (Figure 6I). 368
369
DISCUSSION
370371
In the current study, we demonstrated that 660nm-GaAlAs-LLLT at a dose of 9 J/cm2 372
significantly reduced neuropathic allodynia in CCI rats. Our results are similar to those of 373
previous reports demonstrating that Nd: YAG laser-applied rats that received soft tissue surgery 374
had significantly higher nociceptive thresholds of the hind paw compared with the controls on 375
10 the 7th postoperative day (Kara et al., 2010) and 830 nm-wavelength LLLT at doses of 4 and 8 376
J/cm2 over the surgical incision on the 3rd postoperative day was effective in reducing pain in 377
rats with sciatic nerve compression using catgut thread (Bertolini et al., 2011). In clinical 378
studies of carpal tunnel syndrome, there was a significant improvement in neuropathy-induced 379
pain and delay of nerve conduction in patients undergoing LLLT over the carpal tunnel area 380
(Elwakil et al., 2007) (Shooshtari et al., 2008). 381
Pain due to inflammation is characteristic of neuropathy (Sommer and Kress, 2004, 382
Sommer and Schäfers, 2004, Li et al., 2011, Liou et al., 2011). As previously described,
383
mediators released from infiltrated cells, such as TNF-α and IL-1, have been implicated
384
directly in neuropathic pain, chronic hyperalgesia, and allodynia (Wagner and Myers, 1996,
385
DeLeo et al., 1997). Based on our observations from CCI rats in this study, the infiltration cells 386
and the protein levels of TNF-α and IL-1β in damaged nerves were significantly increased in
387
the control group. It seems that the contribution of inflammation and pro-inflammatory
388
cytokines to neuropathic pain were predominantly observed in the late postinjury phases.Our
389
results are further supported by a recent study with CCI rat model which showed reduction of 390
MPWT was correlated with increases of TNF-α and IL-1β gene expression in sciatic nerve 391
(Okamoto et al., 2001). Our results also demonstrated the infiltration of inflamed cells and the
392
release of proinflammatory cytokines were significantly reduced after LLLT in comparison 393
with the sham-irradiated controls. This result is similar to findings of previous studies with a 394
rat model of carrageenan-induced inflammation (Albertini et al., 2008, Boschi et al., 2008). 395
Therefore, the alleviation of neuropathic pain treated with LLLT in this study was probably
396
due to the reduction of inflammation and pro-inflammatory cytokines of injured nerve tissue.
397
SFI, TFI and PFI described by Bain et al. (Bain et al., 1989) are well-established and are 398
useful techniques for quantitatively assessing a rat’s lower limb deficits and determining 399
lesion-induced changes in function in sciatic nerve and its muscular branches in the rat. 400
Therefore, footprints were obtained after CCI for evaluation of functional locomotor recovery 401
by means of the SFI, TFI and PFI in this study. Our results showed that the SFI, TFI and PFI 402
were significantly affected by CCI at proximal stump of sciatic nerve. Probably owing to 403
impairment of sciatic nerve function and pain induced by CCI, prints were found to be 404
abnormal with evidence of toe dragging and a more “slurred” print. The use of LLLT 405
significantly promoted functional recovery as evidenced by increases in the SFI, TFI and PFI. 406
These results are consistent with the findings of a previous study that demonstrated LLLT was 407
effective in promoting early functional recovery as indicated by the SFI (Barbosa et al., 2010). 408
A nerve constriction injury produces histopathologic changes similar to the manner in 409
which a ischemic nerve injury can produce hyperesthesia when it causes Wallerian 410
degeneration (Myers et al., 1993). These data suggest that the nerve ischemia itself may play 411
an important role in the development of the hyperesthesia and allodynia induced by nerve CCI 412
(Myers et al., 1993). In response to ischemic damage in nerve, involvement of the 413
ischemia-related gene HIF-1 has been reported (Goldenberg-Cohen et al., 2009). HIF-1 has 414
dual effects and can induce either cell survival or cell death (Semenza, 2000). Accumulation of 415
HIF-1α protein and increase of HIF-1 activity have been found to exist following inflammation, 416
probably induced by pro-inflammatory cytokines, i.e., IL-1 and TNF-α (Hellwig-Burgel et al., 417
2005, Dehne and Brune, 2009, Chou et al., 2011). HIF-1 also existed in macrophage to 418
optimize its innate immunity, control pro-inflammatory gene expression and influence cell 419
migration (Dehne and Brune, 2009). Our previous findings showed pain and infiltration of 420
inflamed cells can be reduced by reducing HIF-1α protein accumulation in an arthritic animal 421
model (Chou et al., 2011). An in vitro study demonstrated that impaired neurons can be 422
rescued to promote neurogenesis by stabilizing HIF-1α (Milosevic et al., 2009). Therefore, 423
11 stabilization of HIF-1α protein expression as a regulator of gene expression in tissues is
424
required for the establishment of normal physiological systems (Semenza, 2000). The results of 425
this study demonstrated that the accumulation of HIF-1α in damaged nerve tissues was 426
prominent in response to CCI and were suppressed after LLLT. LLLT also reduced HIF-1α 427
expression in macrophages which coordinate chronic inflammation and immune responses. 428
Our results are consistent with a recent study which employed a mouse infection model to 429
investigate wound healing and demonstrated that untreated lesions showed high 430
immunoreactivity for HIF-1 , whereas little immunoreactivity could be detected in 431
laser-treated lesions (Ferreira et al., 2009). We postulate that this finding may help to explain 432
the ability of laser radiation to eliminate HIF-1α accumulation and then stabilize its activity, 433
thereby stimulating aerobic cell metabolism, accelerating tissue repair and promoting 434
functional recovery. 435
Vascular alterations of peripheral nerves occurring after injury are well described. 436
Angiogenesis is an essential component of nerve re-growth, and regeneration of the endoneural 437
vasculature precedes the outgrowth of axons from the proximal stump (Hoke, 2006, Webber 438
and Zochodne, 2010). It is thought that VEGF, a potent growth factor for angiogenesis, also 439
plays an important role in proliferation of Schwann cells, nerve repair and motor performance 440
(Hobson et al., 2000, Pereira Lopes et al., 2011). Increased angiogenesis primarily takes place 441
in metabolically altered or in injured peripheral nerves (Samii et al., 1999). Moreover, 442
stabilization of HIF-1α in a mouse with diabetes enhances wound healing and increases VEGF 443
production (Mace et al., 2007). Our findings demonstrated that CCI rats with sensory 444
neuropathy expressed VEGF in sciatic nerves. LLLT could further facilitate a prominent 445
increase of VEGF immunoreactivity compared with that obtained by sham-irradiation. This 446
effect was probably achieved through the stabilization of HIF-1α protein activity. In a study 447
which revealed similar findings to those of the present investigation it was shown that LLLI 448
could stimulate proliferation, increase VEGF secretion and facilitate myogenic differentiation 449
of bone marrow-derived mesenchymal stem cells (Hou et al., 2008), indicating that LLLT can 450
accelerate the healing process of tissues by stimulating VEGF. 451
NGF may act positively on the regeneration and growth of axonal processes to promote 452
the survival and integrity of sensory neurons and reverse distinct morphological and sensory 453
deficits and degeneration of myelin (Apfel et al., 1994). NGF also increases the levels of 454
VEGF in normal neural cells (Calza et al., 2001) and stimulates angiogenesis in animal models 455
under ischemic condition (Turrini et al., 2002). Local administration of anti-NGF serum can 456
block sprouting of collateral nerve fiber after sciatic nerve CCI in rats (Ro et al., 1998). 457
Improvement of sensory neuropathy and nerve fiber morphology could also be achieved by 458
application of NGF (Unger et al., 1998). In accordance with these previous findings, our results 459
showed that the elevation of NGF protein by LLLT was greater than that found in animals 460
treated with sham-irradiation. Moreover, in this study, an increase of S100 immunoreactivity 461
was also found after LLLT, indicating an increase in Schwann cells and these changes may be 462
attributed to improvement of functional motor status measured by SFI, TFI and PFI. Therefore, 463
improvement of neural function could also be achieved by application of LLLT which can 464
increase protein levels of NGF and VEGF to repair the myelin sheath in the injured nerve 465 tissues. 466 467
CONCLUSIONS
468 46912 The aim of this study was to analyze the influence of injured nerve irradiation using a 470
660-nm Ga-Al-As diode laser on the neurorehabilitation of CCI sciatic nerves. The behavioral 471
evaluation of rats indicated that LLLT on CCI nerve tissues yielded much better recovery with 472
regard to motor function, pain behavior and histomorphometry than that achieved by 473
sham-irradiation. LLLT also reduced the protein levels of pro-inflammatory cytokines and 474
HIF-1α accumulation, and elevated levels of VEGF and NGF of the nerve tissue. These results 475
support our postulation that LLLT applied transcutaneously to the CCI nerve can suppress 476
inflammation-induced TNF-α, IL-1β and HIF-1α accumulation to control the neuropathic pain 477
and elevate the levels of VEGF and NGF in injured nerve thereby promoting functional 478
recovery and nerve regeneration. These results also indicate that the LLLT can modulate 479
HIF-1α activity and may represent a novel therapeutic approach as a clinically applicable 480
modality for improvement of tissue hypoxia/ischemia in nerve entrapment neuropathy as well 481
as for acceleration of the reinnervation rate of regenerated nerves, which may lead to sufficient 482
morphologic and functional recovery of the peripheral nerve. 483
484
ACKNOWLEDGEMENTS
485
The authors gratefully acknowledge the pathological and technical expertise of Mr. 486
Shih-Chung Chen in this study. This study was supported by a grant from China Medical 487
University (CMU99-TC-23), Taiwan. 488
489 490
13
REFERENCES
491 492
Albertini R, Villaverde AB, Aimbire F, Bjordal J, Brugnera A, Mittmann J, Silva JA, Costa M 493
(Cytokine mRNA expression is decreased in the subplantar muscle of rat paw subjected to 494
carrageenan-induced inflammation after low-level laser therapy. Photomed Laser Surg 495
26:19-24.2008). 496
Albertini R, Villaverde AB, Aimbire F, Salgado MA, Bjordal JM, Alves LP, Munin E, Costa 497
MS (Anti-inflammatory effects of low-level laser therapy (LLLT) with two different red 498
wavelengths (660 nm and 684 nm) in carrageenan-induced rat paw edema. J Photochem 499
Photobiol B 89:50-55.2007). 500
Apfel SC, Arezzo JC, Brownlee M, Federoff H, Kessler JA (Nerve growth factor 501
administration protects against experimental diabetic sensory neuropathy. Brain Res 502
634:7-12.1994). 503
Bain JR, Mackinnon SE, Hunter DA (Functional evaluation of complete sciatic, peroneal, and 504
posterior tibial nerve lesions in the rat. Plast Reconstr Surg 83:129-138.1989). 505
Barbosa RI, Marcolino AM, de Jesus Guirro RR, Mazzer N, Barbieri CH, de Cassia Registro 506
Fonseca M (Comparative effects of wavelengths of low-power laser in regeneration of sciatic 507
nerve in rats following crushing lesion. Lasers Med Sci 25:423-430.2010). 508
Baron R (Peripheral neuropathic pain: from mechanisms to symptoms. Clin J Pain 509
16:S12-20.2000). 510
Bennett GJ, Xie YK (A peripheral mononeuropathy in rat that produces disorders of pain 511
sensation like those seen in man. Pain 33:87-107.1988). 512
Bertolini GR, Artifon EL, Silva TS, Cunha DM, Vigo PR (Low-level laser therapy, at 830 nm, 513
for pain reduction in experimental model of rats with sciatica. Arq Neuropsiquiatr 514
69:356-359.2011). 515
Boschi ES, Leite CE, Saciura VC, Caberlon E, Lunardelli A, Bitencourt S, Melo DA, Oliveira 516
JR (Anti-Inflammatory effects of low-level laser therapy (660 nm) in the early phase in 517
carrageenan-induced pleurisy in rat. Lasers Surg Med 40:500-508.2008). 518
Byrnes KR, Wu X, Waynant RW, Ilev IK, Anders JJ (Low power laser irradiation alters gene 519
expression of olfactory ensheathing cells in vitro. Lasers Surg Med 37:161-171.2005). 520
Calza L, Giardino L, Giuliani A, Aloe L, Levi-Montalcini R (Nerve growth factor control of 521
neuronal expression of angiogenetic and vasoactive factors. Proc Natl Acad Sci U S A 522
98:4160-4165.2001). 523
Chou LW, Wang J, Chang PL, Hsieh YL (Hyaluronan modulates accumulation of 524
hypoxia-inducible factor-1 alpha, inducible nitric oxide synthase, and matrix 525
metalloproteinase-3 in the synovium of rat adjuvant-induced arthritis model. Arthritis Res Ther 526
13:R90.2011). 527
Dehne N, Brune B (HIF-1 in the inflammatory microenvironment. Exp Cell Res 528
315:1791-1797.2009). 529
DeLeo JA, Colburn RW, Rickman AJ (Cytokine and growth factor immunohistochemical 530
spinal profiles in two animal models of mononeuropathy. Brain Res 759:50-57.1997). 531
Elwakil TF, Elazzazi A, Shokeir H (Treatment of carpal tunnel syndrome by low-level laser 532
versus open carpal tunnel release. Lasers Med Sci 22:265-270.2007). 533
Ferreira MC, Gameiro J, Nagib PR, Brito VN, Vasconcellos Eda C, Verinaud L (Effect of low 534
intensity helium-neon (HeNe) laser irradiation on experimental paracoccidioidomycotic wound 535
healing dynamics. Photochem Photobiol 85:227-233.2009). 536
Fraisl P, Aragones J, Carmeliet P (Inhibition of oxygen sensors as a therapeutic strategy for 537
ischaemic and inflammatory disease. Nat Rev Drug Discov 8:139-152.2009). 538
14 Gigo-Benato D, Geuna S, Rochkind S (Phototherapy for enhancing peripheral nerve repair: a 539
review of the literature. Muscle Nerve 31:694-701.2005). 540
Gigo-Benato D, Russo TL, Tanaka EH, Assis L, Salvini TF, Parizotto NA (Effects of 660 and 541
780 nm low-level laser therapy on neuromuscular recovery after crush injury in rat sciatic 542
nerve. Lasers Surg Med 42:673-682.2010). 543
Goldenberg-Cohen N, Dadon-Bar-El S, Hasanreisoglu M, Avraham-Lubin BC, 544
Dratviman-Storobinsky O, Cohen Y, Weinberger D (Possible neuroprotective effect of 545
brimonidine in a mouse model of ischaemic optic neuropathy. Clin Experiment Ophthalmol 546
37:718-729.2009). 547
Hellwig-Burgel T, Stiehl DP, Wagner AE, Metzen E, Jelkmann W (Review: hypoxia-inducible 548
factor-1 (HIF-1): a novel transcription factor in immune reactions. J Interferon Cytokine Res 549
25:297-310.2005). 550
Hobson MI, Green CJ, Terenghi G (VEGF enhances intraneural angiogenesis and improves 551
nerve regeneration after axotomy. J Anat 197 Pt 4:591-605.2000). 552
Hoke A (Neuroprotection in the peripheral nervous system: rationale for more effective 553
therapies. Arch Neurol 63:1681-1685.2006). 554
Hou JF, Zhang H, Yuan X, Li J, Wei YJ, Hu SS (In vitro effects of low-level laser irradiation 555
for bone marrow mesenchymal stem cells: proliferation, growth factors secretion and 556
myogenic differentiation. Lasers Surg Med 40:726-733.2008). 557
Kara C, Suleyman H, Tezel A, Orbak R, Cadirci E, Polat B, Kara I (Evaluation of pain levels 558
after Nd: YAG laser and scalpel incisions: an experimental study in rats. Photomed Laser Surg 559
28:635-638.2010). 560
Kingery WS, Castellote JM, Wang EE (A loose ligature-induced mononeuropathy produces 561
hyperalgesias mediated by both the injured sciatic nerve and the adjacent saphenous nerve. 562
Pain 55:297-304.1993). 563
Li F, Fang L, Huang S, Yang Z, Nandi J, Thomas S, Chen C, Camporesi E (Hyperbaric 564
Oxygenation Therapy Alleviates Chronic Constrictive Injury-Induced Neuropathic Pain and 565
Reduces Tumor Necrosis Factor-Alpha Production. Anesth Analg.2011). 566
Liou JT, Liu FC, Mao CC, Lai YS, Day YJ (Inflammation confers dual effects on nociceptive 567
processing in chronic neuropathic pain model. Anesthesiology 114:660-672.2011). 568
Mace KA, Yu DH, Paydar KZ, Boudreau N, Young DM (Sustained expression of Hif-1alpha in 569
the diabetic environment promotes angiogenesis and cutaneous wound repair. Wound Repair 570
Regen 15:636-645.2007). 571
Milosevic J, Adler I, Manaenko A, Schwarz SC, Walkinshaw G, Arend M, Flippin LA, Storch 572
A, Schwarz J (Non-hypoxic stabilization of hypoxia-inducible factor alpha (HIF-alpha): 573
relevance in neural progenitor/stem cells. Neurotox Res 15:367-380.2009). 574
Myers RR, Yamamoto T, Yaksh TL, Powell HC (The role of focal nerve ischemia and 575
Wallerian degeneration in peripheral nerve injury producing hyperesthesia. Anesthesiology 576
78:308-316.1993). 577
Okamoto K, Martin DP, Schmelzer JD, Mitsui Y, Low PA (Pro- and anti-inflammatory 578
cytokine gene expression in rat sciatic nerve chronic constriction injury model of neuropathic 579
pain. Exp Neurol 169:386-391.2001). 580
Pereira Lopes FR, Lisboa BC, Frattini F, Almeida FM, Tomaz MA, Matsumoto PK, Langone F, 581
Lora S, Melo PA, Borojevic R, Han SW, Martinez AM (Enhancement of sciatic-nerve 582
regeneration after VEGF gene therapy. Neuropathol Appl Neurobiol.2011). 583
Ro LS, Chen ST, Tang LM (Extent of collateral sprouting of intact nerve fibers in rats depends 584
on the local availability of nerve growth factor. J Formos Med Assoc 97:247-251.1998). 585
Rochkind S (Phototherapy in peripheral nerve regeneration: From basic science to clinical 586
15 study. Neurosurg Focus 26:E8.2009).
587
Rochkind S, Geuna S, Shainberg A (Chapter 25: Phototherapy in peripheral nerve injury: 588
effects on muscle preservation and nerve regeneration. Int Rev Neurobiol 87:445-464.2009). 589
Samii A, Unger J, Lange W (Vascular endothelial growth factor expression in peripheral nerves 590
and dorsal root ganglia in diabetic neuropathy in rats. Neurosci Lett 262:159-162.1999). 591
Semenza GL (HIF-1: mediator of physiological and pathophysiological responses to hypoxia. J 592
Appl Physiol 88:1474-1480.2000). 593
Shooshtari SM, Badiee V, Taghizadeh SH, Nematollahi AH, Amanollahi AH, Grami MT (The 594
effects of low level laser in clinical outcome and neurophysiological results of carpal tunnel 595
syndrome. Electromyogr Clin Neurophysiol 48:229-231.2008). 596
Sommer C, Kress M (Recent findings on how proinflammatory cytokines cause pain: 597
peripheral mechanisms in inflammatory and neuropathic hyperalgesia. Neurosci Lett 598
361:184-187.2004). 599
Sommer C, Schäfers M (Mechanisms of neuropathic pain: the role of cytokines. Drug 600
Discovery Today: Disease Mechanisms 1:441-448.2004). 601
Takeda K, Ichiki T, Narabayashi E, Inanaga K, Miyazaki R, Hashimoto T, Matsuura H, Ikeda J, 602
Miyata T, Sunagawa K (Inhibition of prolyl hydroxylase domain-containing protein suppressed 603
lipopolysaccharide-induced TNF-alpha expression. Arterioscler Thromb Vasc Biol 604
29:2132-2137.2009). 605
Turrini P, Gaetano C, Antonelli A, Capogrossi MC, Aloe L (Nerve growth factor induces 606
angiogenic activity in a mouse model of hindlimb ischemia. Neurosci Lett 323:109-112.2002). 607
Unger JW, Klitzsch T, Pera S, Reiter R (Nerve growth factor (NGF) and diabetic neuropathy in 608
the rat: morphological investigations of the sural nerve, dorsal root ganglion, and spinal cord. 609
Exp Neurol 153:23-34.1998). 610
Wagner R, Myers RR (Endoneurial injection of TNF-alpha produces neuropathic pain 611
behaviors. Neuroreport 7:2897-2901.1996). 612
Webber C, Zochodne D (The nerve regenerative microenvironment: early behavior and 613
partnership of axons and Schwann cells. Exp Neurol 223:51-59.2010). 614
Zimmermann M (Ethical guidelines for investigations of experimental pain in conscious 615
animals. Pain 16:109-110.1983). 616
Zimmermann M (Pathobiology of neuropathic pain. Eur J Pharmacol 429:23-37.2001). 617
618 619 620
16
Legends of Figures
621
Figure 1. Experimental design of the sequence of events for the entire course of the 622
experiment. Evaluations include measurements of mechanical paw withdrawal threshold 623
(MPWT), sciatic, tibial and peroneal functional indexes (SFI, TFI and PFI) at the periods 624
before surgery (pre-op), immediately after surgery (post-op), 7 days after surgery (7d post-op) 625
and after treatment (post-tr) in the chronic constriction injury (CCI) animals treated with LLLT 626
(CL group) and sham-irradiation (CsL group) as well as in the sham-operated CCI animals 627
treated with LLLT (sCL group) and sham-irradiation (sCsL group). After the final treatment, 628
the animals were sacrificed for histology, immunohistochemistry (IHC), immunofluorescence 629
(IFC), Western blotting (WB) and ELISA assays. Solid and dotted lines denote the CCI and 630
sham-operation on the animals sciatic nerve, respectively. Solid and dotted borders of columns 631
denote the LLLT and sham-irradiation on the animals’ sciatic nerve, respectively. 632
633
Figure 2. Assessments of mechanical allodynia and functional recovery. Data were 634
calculated before surgery (pre-op), immediately after surgery (post-op), 7 days after surgery 635
(7d post-op) and after treatment (post-tr) in the chronic constriction injury (CCI) animals 636
treated with LLLT (CL group) and sham-irradiation (CsL group) as well as in the 637
sham-operated CCI animals treated with LLLT (sCL group) and sham-irradiation (sCsL group). 638
Each value represents the mean ± SEM in mechanical paw withdrawal threshold (MPWT) (A), 639
sciatic, tibial and peroneal functional indexes (SFI, TFI and PFI) (B-D). There were no 640
significant differences in any of the data between sCL and sCsL groups. After LLLT, the 641
MPWT, SFI, TFI and PFI were significantly increased when compared with those that received 642
sham-irradiated LLLT. # indicates there were significant differences among the four groups (P 643
< .05). * indicates there was a significant differences between CL and CsL groups (P < .05). 644
645
Figure 3. Assessments of inflammation in sciatic nerves by H&E staining and ED1 646
immunohistochemistry. Representative sections of the sciatic nerves obtained from chronic 647
constriction injury (CCI) animals treated with LLLT (CL group) and sham-irradiation (CsL 648
group) as well as in the sham-operated CCI animals treated with LLLT (sCL group) and 649
sham-irradiation (sCsL group). A-D indicate H&E staining for histopathology of sciatic nerves. 650
In rats of sCL and sCsL groups, the nerve tissues show normal histological appearance (A, B). 651
In rats of CsL group, there was even greater and massive inflammatory cells infiltration in 652
injured nerves (C). However, in rats of CL group, there was less infiltration in the nerves and 653
less accumulation of inflamed cells (D). For ED1 immunohistochemistry, there was more ED1 654
immunoreactivity (DAB-brown) in CsL group (E) than that in CL group (F). The quantitative 655
analysis of H&E and immunostaining for inflamed cells and ED1 are showed in F and G, 656
respectively. # indicates a statistically significant difference (P < .05) when data for CsL group 657
were compared with those of CL, sCsL and sCL groups and * indicates a significant difference 658
(P < .05) when data for CL groups were compared with data from CsL, sCL, sCsL groups. A 659
scale bar indicates 100 μm. Original magnification was ×400. 660
661
Figure 4. Results of TNF-α and IL-1β protein levels in the sciatic nerve. The levels of 662
TNF-α (A) and IL-1β (B) proteins were measured by ELISA in the sciatic nerves removed 663
from the chronic constriction injury (CCI) animals treated with LLLT (CL group) and 664
sham-irradiation (CsL group) as well as in the sham-operated CCI animals treated with LLLT 665
(sCL group) and sham-irradiation (sCsL group). # indicates a statistically significant difference 666
(P < .05) between CsL group and sCsL and sCL groups. # indicates a significant difference (P 667
< .05) between CL groups and CsL groups. 668
17 669
Figure 5. Results of HIF-1α expression in the sciatic nerve. Representative sections of the 670
sciatic nerves obtained from chronic constriction injury (CCI) animals treated with LLLT (CL 671
group) and sham-irradiation (CsL group) as well as in the sham-operated CCI animals treated 672
with LLLT (sCL group) and sham-irradiation (sCsL group). In rats of sCL and sCsL groups, 673
nerve tissue showed low HIF-1α expression (A, B). In rats of CsL group, there was even 674
greater and massive HIF-1α accumulation (DAB-brown) in injured nerves (C). But in rats of 675
CL group, there was less HIF-1α accumulation in nerves (D). Double staining with HIF-1α 676
(FITC-green), ED1 (TRITC-red) and DAPI (blue) by immunofluorescence showed there was 677
more co-expression of HIF-1α and ED1 (light red) in CsL groups (E) than that in CL groups 678
(F). The quantitative analysis of HIF-1α immunoreactivity for positive stained area is shown in 679
G. The protein levels of HIF-1α immunoblotting were significantly increased in CsL and 680
decreased in CL group (H). # indicates a statistically significant difference (P < .05) between 681
CsL group and sCsL and sCL groups. * indicates a significant difference (P < .05) for CL 682
compared with CsL groups. A scale bar indicates 100 μm. Original magnification was ×400. 683
684
Figure 6. Results of NGF, VEGF and S100 expressions in the sciatic nerve. Representative 685
sections of the sciatic nerves obtained from chronic constriction injury (CCI) animals treated 686
with LLLT (CL group) and sham-irradiation (CsL group) as well as in the sham-operated CCI 687
animals treated with LLLT (sCL group) and sham-irradiation (sCsL group). In rats of sCL and 688
sCsL groups, nerve tissue showed low NGF and VEGF expression (data not shown). In rats of 689
CsL group, there was slightly increased NGF (A) and VEGF (B) expression in injured nerves 690
compared with those in sham-operated CCI nerves. But in rats of CL group, the nerves 691
expressed more NGF and VEGF accumulation (D). For coexpression of ED1 and HIF-1α 692
immunofluorescence, there were more coexpressions (shown in light red) in CsL groups (E) 693
than those in CL groups (F). The quantitative analysis of HIF-1α immunoreactivity for positive 694
stained area is shown in G. The protein levels of HIF-1α immunoblotting showed a significant 695
increase in CsL and a decrease in CL group (H). # indicates a statistically significant difference 696
(P < .05) for CsL groups compared with CL, sCsL and sCL groups, and * indicates a 697
significant difference between CL group and CsL, sCsL and sCL groups (P < .05). A scale bar 698
indicates 100 μm. Original magnification was ×400. 699
700 701 702 703
0 1 7 14 CCI / sham-operation Laser / sham-irradiation Sacrificed Day
IHC
IFC
WB
7d post‐op
MPWT
SFI, TFI, PFI
pre‐op
MPWT
SFI, TFI, PFI
post‐op
MPWT
SFI, TFI, PFI
post‐tr
MPWT
SFI, TFI, PFI
0 1 7 14 Day
WB
ELISA
CL
C L
GroupCsL
sCL
sCsL
A
0B
CsLCLsCL sCsL
post‐tr pre‐op post‐op post‐op 7d
0 pre‐op post‐op post‐tr 7d post‐op 5 10 CsL sCsL W T ( g) ‐40 ‐20 sco re
#
#
#
*
15 20 MP W ‐80 ‐60#
#
*
SFI s 25 post‐tr pre‐op post‐op post‐op 7d0
‐100
#
#
#
0 pre‐op post‐op post‐tr 7d post‐op
C
D
‐40 ‐20 re ‐40 ‐20*
re ‐80 ‐60*
TFI sc o r ‐80 ‐60#
#
*
PFI sc o r ‐100#
#
#
*
‐100#
A B
C D
E F
ED 1-po sit iv e s ta in ed a rea (% ) 0 10 20 30sCsL sCL CsL
CL
0 2 4 6 8 10sCsL sCL CsL
CL
A rea o f n uc lei (% )G H
*
#
*
#
30000 30000 α
A B
(pg/ml) (pg/ml) 15000 20000 25000 15000 20000 25000 evels of TNF-α evels of IL-β#
#
0 5000 10000 0 5000 10000 Protein l e Protein l e*
*
sCsL
sCL
CsL
CL
sCsL
sCL
CsL
CL
A B
C D
E F
G H
0 0.1 0.2 0.3 0.4 0.5sCsL
sCL
CSL
CL
0 5 10 15 20 25sCsL
sCL
CsL
CL
Group
HIF-1α β-actinsCsL sCL CsL CL
HI F -1 α / β -a c ti n ( fol d)*
HI F -1 α -pos it iv e st ai n ed area (% )*
#
#
0 5 10 15 20
![HPSH [ 分子間作用力 - 凡得瓦力 ]](data:image/gif;base64,R0lGODlhAQABAIAAAP///wAAACH5BAEAAAAALAAAAAABAAEAAAICRAEAOw==)