科技部補助專題研究計畫報告
開發卵巢亮細胞癌精準醫療:以FXYD2為臨床生物標記和藥物治
療靶點-探討FXYD2在臨床卵巢亮細胞癌病人的角色(2/2)
報 告 類 別 : 成果報告 計 畫 類 別 : 整合型計畫
計 畫 編 號 : MOST 108-2314-B-006-003- 執 行 期 間 : 108年08月01日至109年07月31日 執 行 單 位 : 國立成功大學醫學系婦產科
計 畫 主 持 人 : 許耿福
共 同 主 持 人 : 李國賓、陳玉玲、謝興邦、鄭雅敏
計畫參與人員: 碩士級-專任助理:莊媛喆
博士班研究生-兼任助理:白明旭 博士後研究-博士後研究:林長霓
本研究具有政策應用參考價值:■否 □是,建議提供機關
(勾選「是」者,請列舉建議可提供施政參考之業務主管機關)
本研究具影響公共利益之重大發現:□否 □是
中 華 民 國 109 年 10 月 18 日
中 文 摘 要 : 由於近年來液態切片(如循環癌細胞或cell-free DNA; CTC or cfDNA)應用於腫瘤醫學受到大家的重視。相較於傳統組織切片而言
,液態切片較不具侵入性,且可即時檢測。在第一年的研究中,我 們發現在卵巢癌病人的液態切片中可純化cfDNA,經過qPCR分析發現
,漿液型卵巢癌患者與卵巢亮細胞癌患者腹水中的FXYD2量,較良性 患者腹腔灌洗液中的FXYD2分別高出4.8倍與8.7倍; 而
BPR1P0004S0(ouabain),BPR1P0012S0(cymarol),BPR1P0013S0
(oleandrin),BPR1P0014S0(neriifolin)和
BPR1P0015S0(cymarin)等CG衍生物具有高表達FXYD2的OCCC細胞的 治療潛力; 且我們也成功建立卵巢原位癌小鼠模式。第一年結果說 明,偵測FXYD2 cfDNA可成為卵巢亮細胞癌新興的生物標誌,且利用 CG衍生物可成為高表達FXYD2的OCCC病患精準治療的潛在藥物。第二 年,我們進一步量化血漿中FXYD2 cfDNA的水平,經過qPCR偵測 gnomic DNA來推算血漿中FXYD2 cfDNA的濃度,發現31例正常人的血 漿中FXYD2 cfDNA平均濃度為18.10±7.51 ng/ml; 而7例第一期 OCCC患者的血漿中FXYD2 cfDNA平均濃度為29.20±7.85 ng/ml。此部 分結果顯示利用qPCR量測血漿中FXYD2 cfDNA濃度確實可以當作 OCCC早期偵測平台。另外,我們偵測8個CGs衍生物之細胞半致死濃 度後,確認BPR1P0014S0(neriifolin)為最具有治療潛力的 CGs,且在心肌細胞(H9C2)的存活分析中發現,在相同治療濃度下
,BPR1P0014S0(neriifolin)治療後其細胞致死率較Digoxin治療 低。也就是說,BPR1P0014S0(neriifolin)具有高表達FXYD2的 OCCC治療潛力,而且具有較低的心臟毒性。除此之外,我們也成功 地建立OCCC原位癌動物模式。在高表達FXYD2的OCCC細胞株(TOV- 21G)與低表達FXYD2的OCCC細胞株(ES-2)中,分別轉殖GFP螢光載體
,利於活體分子影像系統觀察腫瘤生長情況。在
PR1P0014S0(neriifolin)治療後,相較於ES-2誘發的腫瘤,TOV- 21G誘發的腫瘤生長有消退的情形。顯示
BPR1P0014S0(neriifolin)具有治療高表達FXYD2的OCCC之潛力。
我們的研究指出,偵測血漿中FXYD2 cfDNA的水平可以達到OCCC早期 診斷。儘管CG具有高心臟毒性,但CG類似物
(BPR1P0014S0(neriifolin))仍顯示出具有治療OCCC潛力,而且相 較於Digoxin也具較低的心肌細胞致死率。
中 文 關 鍵 詞 : 卵巢亮細胞癌、FXYD2、液態切片、生物標誌、強心苷
英 文 摘 要 : Over the past recent years, the application of liquid
biopsies (such as circulating tumor cells or cell-free DNA;
CTC or cfDNA) has been attention. Liquid biopsies have less invasive and real-time detection characteristics as
compared with traditional biopsy. In the first year, we validated the FXYD2 cfDNA level from serous ovarian cancer ascites and OCCC ascites were increase 4.8-folds and 8.7- folds respectively as compared with cfDNA from normal
peritoneal lavage. The CGs including BPR1P0004S0 (ouabain), BPR1P0012S0 (cymarol), BPR1P0013S0 (oleandrin), BPR1P0014S0 (neriifolin) and BPR1P0015S0 (cymarin) have therapeutic effect in OCCC with FXYD2 high expression. In addition, we
success established a OCCC orthotopic xenograft model.
Thus, we demonstrated the FXYD2 cfDNA detection can act a novel biomarker in OCCC, and the CGs may have therapeutic effect in OCCC with FXYD2 high expression.
In the second year, we further quantified the level of FXYD2 cfDNA in plasma. We used qPCR to detect the gnomic DNA to estimate the concentration of FXYD2 cfDNA in plasma.
We found that the average concentration of FXYD2 cfDNA in plasma of 31 normal people was 18.10±7.51 ng/ml, and the average concentration of FXYD2 cfDNA in the plasma of the 7 first-stage OCCC patients was 29.20±7.85 ng/ml. This part of the results show that the use qPCR to measure the concentration of FXYD2 cfDNA in plasma can act an early detection platform for OCCC. Moreover, after detecting the IC50 of 8 CGs derivatives, we confirmed that BPR1P0014S0 (neriifolin) is the GCs have most therapeutic potential. In the cell viablity analysis, we found that H9C2 cells death after treated with BPR1P0014S0 (neriifolin) was lower than Digoxin treatment at the same concentration. In other words, BPR1P0014S0 (neriifolin) has the therapeutic
potential of OCCC with FXYD2 high expression, and has low cardiotoxicity.
In the meantime, we also successfully established a OCCC orthotopic xenograft model that situaction of tumor growth can be observed by IVIS image system. We used the
fluorescent vector to transfected into OCCC cell lines, TOV-21G (with high expression of FXYD2) and ES-2 (with low expression of FXYD2). Which is beneficial to the
observation of tumor growth by in vivo molecular imaging system. Compared with ES-2 induced tumors, the TOV-21G induced tumor growth has subsided after BPR1P0014S0
(neriifolin) treatment. The results show that BPR1P0014S0 (neriifolin) has the therapeutic potential in OCCC with high FXYD2 expression.
Our research indicates that detecting the level of FXYD2 cfDNA in plasma can achieve early diagnosis of OCCC.
Despite the high cardiotoxicity of CG, the CG analogue (BPR1P0014S0 (neriifolin)) still has the therapeutic potential in OCCC with high FXYD2 expression, and the BPR1P0014S0 (neriifolin) treatment also has a lower cell death rate of cardiomyocytes than Digoxin treatment.
Therefore, FXYD2 can be regarded as a novel biomarker of OCCC, and the precision medicine can be achieved through the GCs treatment.
英 文 關 鍵 詞 : Ovarian clear cell carcinoma (OCCC), FXYD2, liquid biopsies, biomarker, Cardiac glucosides
I
中文摘要
卵巢亮細胞癌(OCCC)是婦女癌症中最棘手的疾病,主要原因是 OCCC 難以早期診斷與 對於化學治療的抗藥性。目前臨床上並沒有可以信賴的卵巢亮細胞癌腫瘤標記,用以反應病 人在臨床治療成效。故發展一個具有科學信賴的生物標記及精準醫療靶點,對於卵巢亮細胞 癌患者是非常重要的。先前我們的研究團隊發現 Na+/K+ ATPase 的 γ-subunit, FXYD2, 在 OCCC 有高度表現,同時與病人的預後有相關性。使用強心苷(cardiac glycoside, CG),如 Digoxin 可以有效抑制 FXYD2 表現與 Na+/K+ ATPase 活性,並在動物模型中發現低劑量的 Digoxin(0.1 mg/kg)可以抑制 OCCC 的生長。這些結果顯示 FXYD2 是個具有潛力的生物 標誌且可適用低劑量的 CG 治療。
由於近年來液態切片(如循環癌細胞或 cell-free DNA; CTC or cfDNA)應用於腫瘤醫學受 到大家的重視。相較於傳統組織切片而言,液態切片較不具侵入性,且可即時檢測。在第一 年的研究中,我們發現在卵巢癌病人的液態切片中可純化 cfDNA,經過 qPCR 分析發現,漿 液型卵巢癌患者與卵巢亮細胞癌患者腹水中的 FXYD2 量,較良性患者腹腔灌洗液中的 FXYD2 分 別 高 出 4.8 倍 與 8.7 倍 ; 而 BPR1P0004S0 ( ouabain ) , BPR1P0012S0
( cymarol ) , BPR1P0013S0 ( oleandrin ) , BPR1P0014S0 ( neriifolin ) 和 BPR1P0015S0
(cymarin)等 CG 衍生物具有高表達 FXYD2 的 OCCC 細胞的治療潛力; 且我們也成功建立 卵巢原位癌小鼠模式。第一年結果說明,偵測 FXYD2 cfDNA 可成為卵巢亮細胞癌新興的生 物標誌,且利用 CG 衍生物可成為高表達 FXYD2 的 OCCC 病患精準治療的潛在藥物。
第二年,我們進一步量化血漿中 FXYD2 cfDNA 的水平,經過 qPCR 偵測 gnomic DNA 來推算血漿中 FXYD2 cfDNA 的濃度,發現 31 例正常人的血漿中 FXYD2 cfDNA 平均濃度 為 18.10±7.51 ng/ml; 而 7 例第一期 OCCC 患者的血漿中 FXYD2 cfDNA 平均濃度為 29.20±
7.85 ng/ml。此部分結果顯示利用 qPCR 量測血漿中 FXYD2 cfDNA 濃度確實可以當作 OCCC 早期偵測平台。另外,我們偵測 8 個 CGs 衍生物之細胞半致死濃度後,確認 BPR1P0014S0
(neriifolin)為最具有治療潛力的 CGs,且在心肌細胞(H9C2)的存活分析中發現,在相同治 療濃度下,BPR1P0014S0(neriifolin)治療後其細胞致死率較 Digoxin 治療低。也就是說,
BPR1P0014S0(neriifolin)具有高表達 FXYD2 的 OCCC 治療潛力,而且具有較低的心臟毒 性。
除此之外,我們也成功地建立 OCCC 原位癌動物模式。在高表達 FXYD2 的 OCCC 細 胞株(TOV-21G)與低表達 FXYD2 的 OCCC 細胞株(ES-2)中,分別轉殖 GFP 螢光載體,利於 活體分子影像系統觀察腫瘤生長情況。在 BPR1P0014S0(neriifolin)治療後,相較於 ES-2 誘發的腫瘤,TOV-21G 誘發的腫瘤生長有消退的情形。顯示 BPR1P0014S0(neriifolin)具 有治療高表達 FXYD2 的 OCCC 之潛力。
我們的研究指出,偵測血漿中 FXYD2 cfDNA 的水平可以達到 OCCC 早期診斷。儘管 CG 具有高心臟毒性,但 CG 類似物(BPR1P0014S0(neriifolin))仍顯示出具有治療 OCCC 潛力,而且相較於 Digoxin 也具較低的心肌細胞致死率。因此,FXYD2 可視為 OCCC 的生 物標誌,且透過 GC 類似物的治療亦可實現精密醫學的目標。
關鍵字: 卵巢亮細胞癌、FXYD2、液態切片、生物標誌、強心苷
Abstract
Ovarian clear cell carcinoma (OCCC) is the most knotty disease in gynecological cancers. The difficulties of OCCC therapy are including early diagnosis and chemo-resistance. For the moment, no a specific marker could be used in clinical diagnosis for OCCC. It is very urgent to explore the useful clinical tumor marker for the OCCC and develop the precision target therapy for OCCC patients. Our preliminary results shown the gamma subunit of sodium potassium ATPase, FXYD2, is highly expressed in OCCC patients and significantly associated with poor prognosis. Cardiac glucoside (CG), such as Digoxin, could be used to reduce sodium potassium ATPase activities and FXYD2 expression, in the meantime, low dose (0.1 mg/kg) of Digoxin could suppress the OCCC growth in mice xenograft model. These results imply FXYD2 is a potential marker for OCCC early detection, and suitable for low dose CGs therapy.
Over the past recent years, the application of liquid biopsies (such as circulating tumor cells or cell-free DNA; CTC or cfDNA) has been attention. Liquid biopsies have less invasive and real-time detection characteristics as compared with traditional biopsy. In the first year, we validated the FXYD2 cfDNA level from serous ovarian cancer ascites and OCCC ascites were increase 4.8-folds and 8.7-folds respectively as compared with cfDNA from normal peritoneal lavage. The CGs including BPR1P0004S0 (ouabain), BPR1P0012S0 (cymarol), BPR1P0013S0 (oleandrin), BPR1P0014S0 (neriifolin) and BPR1P0015S0 (cymarin) have therapeutic effect in OCCC with FXYD2 high expression. In addition, we success established a OCCC orthotopic xenograft model.
Thus, we demonstrated the FXYD2 cfDNA detection can act a novel biomarker in OCCC, and the CGs may have therapeutic effect in OCCC with FXYD2 high expression.
In the second year, we further quantified the level of FXYD2 cfDNA in plasma. We used qPCR to detect the gnomic DNA to estimate the concentration of FXYD2 cfDNA in plasma. We found that the average concentration of FXYD2 cfDNA in plasma of 31 normal people was 18.10±7.51 ng/ml, and the average concentration of FXYD2 cfDNA in the plasma of the 7 first-stage OCCC patients was 29.20±7.85 ng/ml. This part of the results show that the use qPCR to measure the concentration of FXYD2 cfDNA in plasma can act an early detection platform for OCCC.
Moreover, after detecting the IC50 of 8 CGs derivatives, we confirmed that BPR1P0014S0 (neriifolin) is the GCs have most therapeutic potential. In the cell viablity analysis, we found that H9C2 cells death after treated with BPR1P0014S0 (neriifolin) was lower than Digoxin treatment at the same concentration. In other words, BPR1P0014S0 (neriifolin) has the therapeutic potential of OCCC with FXYD2 high expression, and has low cardiotoxicity.
In the meantime, we also successfully established a OCCC orthotopic xenograft model that situaction of tumor growth can be observed by IVIS image system. We used the fluorescent vector to transfected into OCCC cell lines, TOV-21G (with high expression of FXYD2) and ES-2 (with low expression of FXYD2). Which is beneficial to the observation of tumor growth by in vivo molecular imaging system. Compared with ES-2 induced tumors, the TOV-21G induced tumor growth has subsided after BPR1P0014S0 (neriifolin) treatment. The results show that BPR1P0014S0 (neriifolin) has the therapeutic potential in OCCC with high FXYD2 expression.
Our research indicates that detecting the level of FXYD2 cfDNA in plasma can achieve early diagnosis of OCCC. Despite the high cardiotoxicity of CG, the CG analogue (BPR1P0014S0 (neriifolin)) still has the therapeutic potential in OCCC with high FXYD2 expression, and the BPR1P0014S0 (neriifolin) treatment also has a lower cell death rate of cardiomyocytes than Digoxin treatment. Therefore, FXYD2 can be regarded as a novel biomarker of OCCC, and the precision medicine can be achieved through the GCs treatment.
Keywords: Ovarian clear cell carcinoma (OCCC), FXYD2, liquid biopsies, biomarker, Cardiac glucosides
Contents
Chinese abstract………..………..…I Abstract………...….II
Introduction………..…1
Specific aims………1
Materials and Methods………...2
Results……….….3
Discussion………6
Reference………..7
Tables and Figures……….….…..9
1
Introduction
Epithelial ovarian cancer is classified into four major histological subtypes, including serous, mucinous, endometrioid, and clear cell types [1]. Each subtype is a genetically distinct disease leading different pathogenesis and clinical response. While patients with ovarian clear cell carcinoma (OCCC) have a high rate of recurrence and poor prognosis [2-4]. OCCC usually relatived chemoresistance when the tumor cells spread outside of ovary [5, 6]. Patients with OCCC were only 45% responded to platinum-based chemotherapy versus 81% in other epithelial cell types [7]. Currently, there is no reliable biomarker for OCCC [8]. OCCC has been reported that occur more frequent in Asian women than Western ones (20 % vs. 5 %) [9]. All these findings suggest that OCCC has distinct genetic background and may require individualized treatment modality to improved prognosis, especially in Asian women.
Na+/K+ ATPase, an oligomeric transmembrane protein composed of α, β, and γ subunits, is highly expressed in epithelial cells and plays an important role in the kidney [10, 11]. Na+/K+ ATPase activity is required to maintain membrane potential homeostasis and has been implicated in many cellular functions and the pathogenesis of specific diseases [12]. In this study, we proposed the cardiac glycoside (CG) maybe have potential in OCCC therapy that was because CG induced OCCC cell death is associated with FXYD2 (the γ subunit and enzymatic modulator of the Na+/K+
ATPase) expression. Silence of FXYD2 in OCCC cells (TOV21G, IGROV1) decreased the sensitivity to cardiac glycosides compared with non-OCCC cells with lower FXYD2 expression.
The results suggest that FXYD2 is functionally upregulated in OCCC and may serve as a promising prognostic biomarker and therapeutic target of CGs (digoxin / digitoxin) in OCCC [13]. Therefore, CGs are considered acting novel roles in cancer research and cancer therapy. Here, we aimed to clarify the role of FXYD2 in OCCC patients and assess the possibility of new synthetic CG compounds (provide from Prof. Hsieh, NHRI) act as novel drugs for OCCC accurately therapy.
The circulating tumor cells (CTC) or cell free circulating tumor DNA (cfDNA/ctDNA) have demonstrated the translational potential and may apply clinically and to consider their applications in personalized oncology and in cancer research [14-16]. CTCs are known to be circulating in the body fluids before they metastasize to various parts of the body even in primary stages of the disease [17]. However, they are not easily identified, as they are present in a very small numbers. It is estimated that 5ml of blood might contain just about 5-50 CTCs [18]. On the other hand, cfDNA size has been reported about 150 bp or multiples of 150 bp, they were thought to derive from apoptotic processes originating from the endogenous cleavage of chromatin DNA into inter- nucleosomal fragments [19]. To date, cfDNA origin, mechanisms of release, regulation, clearance, and its physiological role are still unclear. Importantly, the quality of patient’s tissues (including
blood, ascites and tumor tissue) for clinical diagnosis need exacting preservation. In the first year, we established a strict process for clinical specimens collection to future experiments. Some preliminary results show the cfDNA quality within an acceptable margin. Moreover, these CTC/cfDNA were also experimented in microfluidic platforms to assess the clinical usability of early detection (Prof. Lee, NTHU). We are the well-connected team. Next year, experiments will be go ahead to clarify the role of FXYD2 in OCCC patients (cooperation with Prof. Chen, NCKU) and assess the application in clinical early diagnosis. The specific aims were described below:
(1) To establish OCCC tissue bank, and to explore the feasibility of FXYD2 detection in OCCC early diagnosis through liquid biopsies.
(2) To establish the Patient-Derived Xenograft (PDX) mice model and OCCC orthotopic xenograft tumor model.
(3) To explore the possibility of new synthetic CG compounds act as novel drug for OCCC accurately therapy.
Materials and Methods
Isolation of cell-free DNA/circulating tumor cells (CTCs) from plasma
We subjected the Ficoll-paque tubes containing blood (3:5) to centrifugation at 3500 rpm for 15 min at room temperature. We transferred the supernatant to fresh tubes and stored them at −80°C.
We purified cell-free DNA from 1 ml of the plasma using the QIAamp Circulating Nucleic Acid vacuum kit (Qiagen) according to the manufacturer's instructions. The final elution volume was 30 μl, and store at -20℃ until qPCR analysis.
Quantitative real-time polymerase chain reaction (qRT-PCR)
Total RNA was isolated from cell lines or CTC using TRIzol Reagent (Invitrogen) and reverse transcribed to complementary DNA using SuperScript™ III Reverse Transcriptase (Invitrogen) according to the manufacturer's instructions. All amplification reactions were performed using StepOne™ real-time PCR (Applied Biosystems, Foster City, CA). All reactions were performed in triplicate, and relative expression levels of mRNA were calculated using the delta cycle threshold method by subtraction of GAPDH expression.
Human ovarian cancer cell lines
All of the human ovarian cancer cell lines used in our study, including TOV-21G, ES-2, and SKOV3 were obtained from the American Type Culture Collection (ATCC, Manassas, VA). TOV- 21G cells were maintained in MCDB105 and M199 (1:1) supplemented with 10% fetal bovine serum (FBS, Invitrogen, Carlsbad, CA). The ES-2 cell line was maintained in RPMI1640
supplemented with 10% FBS. The SKOV3 cell line was maintained in DMEM/F-12 with 10% FBS.
All of the culture media contained 5 mM L-glutamine and antibiotics. All of the human ovarian cancer cell lines were incubated at 37°C, in a humid 5% CO2 atmosphere.
Cytotoxicity assay
5000 cells per well in 96-well plates were exposed to various concentrations of inhibitors for 48 hours. Cell viability was measured by MTT assay (Sigma) according to the manufacturer’s instructions. The IC50 value resulting from 50% inhibition of cell growth was calculated by CalcuSyn program.
Orthotopic xenograft mice model
Four- to 6-week-old NOD/SCID mice were obtained from the National Laboratory Animal Center. The housing and experimental animal procedures were approved by the Institutional Animal Care and Use Committee of NCKU. Ovarian cancer cells (5 × 104) were orthotopic injected into the mice by 30G needle and anesthetics (50mg/kg ketamine and 10mg/kg xylazine). The xenografts were observed by IVIS for 8 weeks until the mice were sacrificed.
Patient-derived tumor xenograft (PDX) animal model with OCCC
Human OCCC specimens were cut into 2-4mm3. Make a shallow incision in the dorsal region of ASID mouse using a scissor and then implant subcutaneously two pieces of primary tumor into the interscapular fat pad of ASID mouse within 3 hours after collecting primary tumor tissues from a patient. These mice in the engraftment phase were called P0 mice. When the tumor grows and reaches around 1.5 cm (4–10 weeks), prepare the additional transplant. Cut off skin around the tumor area and cut the tumor into even size piece. One piece of tumor will perform NGS study to check the phenotype of tumor. Other tumors will be implanted into the interscapular fat pad of new ASID mice. Mice in this expansion phase are called P1 mice. After 2–4 weeks, the tumors could be visible. According to this protocol, we will have P3 generation mice to test the therapeutic effect of CG and non-CG type inhibitors in animal with OCCC.
Statistical analysis
Data from all three independent experiments were expressed as the mean ± SD and were then analyzed using an unpaired 2-tailed Student’s t test. For all tests, p < 0.05 was used to define statistical significance.
Results
Concentration of plasma FXYD2 cfDNA in stage I OCCC patients is higher than non-tumor control group.
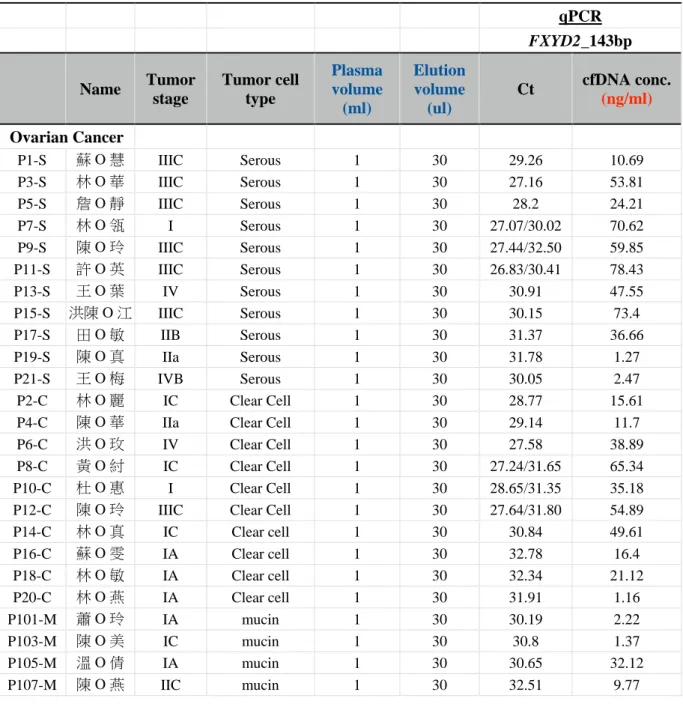
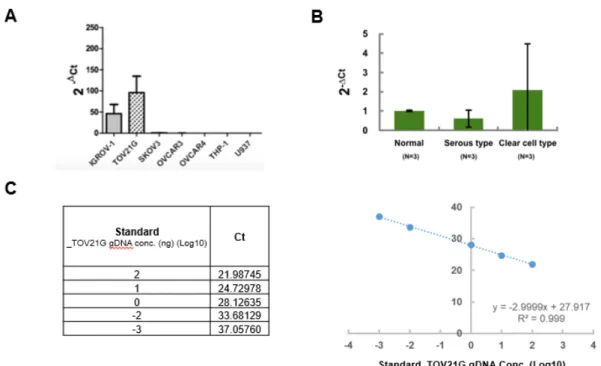
In our preliminary results, FXYD2 gene highly expressed in OCCC cells rather than other cells (Figure 1A). Similarly, FXYD2 gene highly expressed in OCCC clinical specimens as compared with normal control and non-OCCC groups (Figure 1B). This result suggest FXYD2 gene is specific highly expression in OCCC. To explore the cell-free DNA (cfDNA) expression level of FXYD2 in circulation, we used the plasma to execute cfDNA extraction, and quantify the FXYD2 level through pPCR technique. Standard curve is according to the genomic DNA concentration and relevant Ct value from TOV-21G cells (Figure 1C). Sixty-eight samples, including10 OCCC, 11 serous type ovarian cancer, 8 mucinous type ovarian cancer, 5 endometrioid type ovarian cancer, 3 other type and 31 non-tumor control (Table 1), were performed the plasma cfDNA extraction and qPCR analysis. Every plasma sample was used 1ml to perform cfDNA extraction, and used 30μl H2O to elution before stored at -20℃. The rawdata showed in the Table 2. After statistical analyzed, we notice the mean of plasma FXYD2 cfDNA concentration in 31 non-tumor control was 18.78±7.51 ng/ml (mean±SE) and while in 7 clear cell carcinoma with stage I was 29.20±7.85 ng/ml (mean±SE) (Table 3). This data indicated the different of plasma FXYD2 cfDNA in non-tumor control and early OCCC is 10 ng/ml, while detect plasma FXYD2 cfDNA concentration can act a early diagnosis tool in OCCC through qPCR analysis.
A cardiac glycoside (CG) compound, BPR1P0014S0 (neriifolin), have therapeutic effect on the FXYD2 high expression OCCC cell line and no effect on cardiomyocyte.
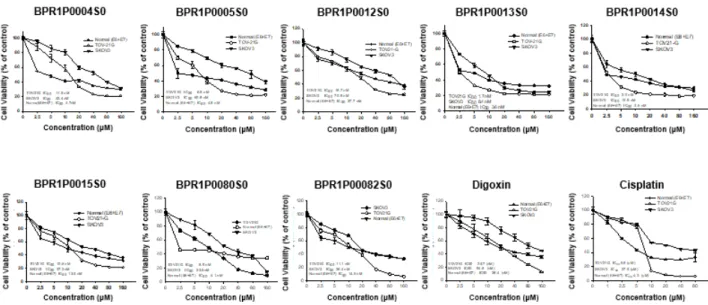
In our periliminary results, 6 CG compounds (BPR1P0004S0, BPR1P0005S0, BPR1P0012S0, BPR1P0013S0, BPR1P0014S0 and BPR1P0015S0) have therapeutic effect on FXYD2 high expression cell lines. Next, we explore the therapeutic effect of GC on ovarian cancer cells whether base on the FXYD2 expression level. We selecte FXYD2 high expression OCCC cell line, TOV- 21G and FXYD2 no expression OCCC cell line, ES-2 to execute experiments. The western blot data showed the protein expression level of FXYD2, and this result imply the expression different of FXYD2 existance in OCCC (Figure 2A). This phenomena is same with the result of IHC stain of clinical specimens that we were reported before. OCCC patients with FXYD2 highly expression has poor outcome. To explore the therapeutic effect of CG compounds, we added a normal epithelium cell line to test the cytotoxicity in CG treatment by MTT assay. Take Digoxin as an example, the IC50 in normal cell and TOV-21G cells were 62.0 nM and 18.7 nM respectively, imply use CG treatment act therapeutic effect in FXYD2 highly expression OCCC and no effect in normal cells (Figure 2B).
Next, we detected the IC50 of 8 CG compounds (BPR1P0004S0, BPR1P0005S0, BPR1P0012S0,
BPR1P0013S0, BPR1P0014S0, and BPR1P0015S0, BPR1P0080S0 and BPR1P0082S0) in normal epithelium, TOV-21G and SKOV3 cell lines through MTT assay to assess dose the cytotoxicity effect presence in normal cell (Figure 3). The data showed that BPR1P0014S0 (neriifolin) is the most potential CG compound in OCCC treatment because the therapeutic window range is largest between normal cells and FXYD2 highly expression OCCC cells. Other words, BPR1P0014S0 (neriifolin) have minimum toxic in normal cells and have most therapeutic effect in FXYD2 highly expression OCCC cells.
We next explore the BPR1P0014S0 (neriifolin) treatment whether influence heart failure or not yet. We used cardiomyocyte, H9C2, to execute cell cytotoxicity assay through MTT assay. The IC50 of BPR1P0014S0 (neriifolin) and Digoxin in H9C2 cells were 132.0 uM and 13.8 uM respectively. The result suggest that BPR1P0014S0 (neriifolin) treatment less likely to cause H9C2 cell death as compare with Digoxin. In this perspective, CG compounds has therapeutic effect for FXYD2 highly expression OCCC while not influence heart function, especially BPR1P0014S0 (neriifolin).
OCCC orthotopic xenograft and patient-derived tumor xenograft (PDX) mice model were successful established.
To evaluate the effect of BPR1P0014S0 (neriifolin) whether achieve the precision target therapy, OCCC orthotopic xenograft and Patient-derived tumor xenograft (PDX) mice model were developed. 5 × 104 TOV-21G GL cells / ES-2 GL cells that has been transfected fluorescence and lucifence (Figure 5A) were execute orthotopic injected into mice by 30G needle under situation of anesthetics (50mg/kg ketamine and 10mg/kg xylazine). In TOV-21G GL orthotopic xenograft mice, 5/5 tumor grew successful at 7-14 days after tumor cell injection. And the BPR1P0014S0 (neriifolin) treatment started at 14 days in 3/5 mice (No. 3, No. 4 and No. 5), others were the no treatment control (No. 1 and No. 2). The IVIS microscopy image was take in the 6th weeks (Figure 5B, left).
In the same conditions, 5/5 tumor grew successful at 3-7 days after tumor cell injection in the ES-2 GL orthotopic xenograft mice. The IVIS microscopy image was take in the 2th weeks (Figure 5B, right) due to the tumor grew faster than TOV-21G GL orthotopic xenograft mice. After BPR1P0014S0 (neriifolin) treatment, the TOV-21G GL orthotopic xenograft tumors size obviously reduce as compare with no treatment, but no therapeutic effect on ES-2 GL orthotopic xenograft tumors (Figure 5C-D). The results imply BPR1P0014S0 (neriifolin) achieve the precision target therapy in FXYD2 highly expression OCCC.
On the other hand, patient-derived tumor xenograft (PDX) mice that executed by NAR Labs were successful established 2 mice with mucinous type ovarian cancer (Table 4). In general, BPR1P0014S0 (neriifolin) act as the FXYD2 highly expression OCCC precision target therapy is
feasible.
Discussion
In Taiwan, the OCCC incidence is almost the same as in Japan (about 20% in ovarian cancer), which is much higher in Western countries (about 5 %). The difficulties of OCCC therapy are including early diagnosis and chemo-resistance. Therefore, search of new treatment modality for OCCC is important. In our preliminary results, FXYD2 highly expression in OCCC tumor and that was associated with patient survival. In the meantime, cardiac glycosides (CGs) successfully treated mice with FXYD2-high expressing tumor [13]. Due to the liquid biopsies has been widely used in early diagnosis, we try to development OCCC early diagnosis method by the liquid biopsies.
cfDNA size has been reported about 150 bp or multiples of 150 bp, they were thought to derive from apoptotic processes originating from the endogenous cleavage of chromatin DNA into inter- nucleosomal fragments [19]. To date, cfDNA origin, mechanisms of release, regulation, clearance, and its physiological role are still unclear. Importantly, the quality of patient’s tissues (including blood, ascites and tumor tissue) for clinical diagnosis need exacting preservation. In the first year, we established a strict process for clinical specimens collection to future experiments. Some preliminary results show the cfDNA quality within an acceptable margin. In the second years, we validate the plasma FXYD2 cfDNA concentration can act a early diagnosis tool in OCCC through qPCR analysis.
In term of target therapy, we known the CGs have therapeutic effect on FXYD2 high expression OCCC mice tumor. In 1st year, we screening 6 new synthetic CG compounds and they maybe have therapeutic feasibility in FXYD2 high expression OCCC. And then in the second years, we confirm the BPR1P0014S0 (neriifolin) can act the precision target therapy in FXYD2 highly expression OCCC via in vitro and in vivo experiments. Simply put, we verify the plasma FXYD2 cfDNA can act a OCCC early prognosis biomarker through qPCR detection. More important, BPR1P0014S0 (neriifolin) therapy may be crucial for FXYD2 high expression OCCC patients in future.
Reference
[1] Reviewed by R Vajpeyi. WHO Classification of Tumours: Pathology and Genetics of Tumours of the Breast and Female Genital Organs. J Clin Pathol. 2005; 58(6): 671–672.
[2] del Carmen MG, Birrer M, Schorge JO. Clear cell carcinoma of the ovary: a review of the literature. Gynecol Oncol. 2012; 126:481–490.
[3] Pectasides D, Pectasides E, Psyrri A, Economopoulos T. Treatment issues in clear cell carcinoma of the ovary: a different entity? Oncologist. 2006; 11:1089–1094.
[4] Sugiyama T, Kamura T, Kigawa J, et al. Clinical characteris- tics of clear cell carcinoma of the ovary: a distinct histologic type with poor prognosis and resistance to platinum-based chemotherapy.
Cancer. 2000; 88:2584–2589.
[5] Itamochi H, Kigawa J, Terakawa N. Mechanisms of chemoresistance and poor prognosis in ovarian clear cell carcinoma. Cancer Sci. 2008; 99: 653-658.
[6] Sugiyama T, Kamura T, Kigawa J, et al. Clinical characteristics of clear cell carcinoma of the ovary: a distinct histologic type with poor prognosis and resistance to platinum-based chemotherapy.
Cancer. 2000; 88: 2584-2589.
[7] Pectasides D, Fountzilas G, Aravantinos G, et al. Advanced stage clear-cell epithelial ovarian cancer: the Hellenic Cooperative Oncology Group experience. Gynecol Oncol,2006; 102: 285-291.
[8] Arakawa N, Kobayashi H, Yonemoto N, et al. Clinical Significance of Tissue Factor Pathway Inhibitor 2, a Serum Biomarker Candidate for Ovarian Clear Cell Carcinoma. PLoS One. 2016;11:
e0165609.
[9] Chan JK, Tech D, Hu JM, Shin JY, Osann K, Kapp DS. Do clear cell ovarian carcinomas have poorer prognosis compared to other epithelial cell types? A study of 1411 clear cell ovarian cancers.
Gynecol Oncol 2008; 109: 370-376.
[10] Kaplan JH. Biochemistry of Na,K-ATPase. Annu Rev Biochem. 2002; 71:511–535.
[11] Jorgensen PL. Structure, function and regulation of Na,K- ATPase in the kidney. Kidney Int.
1986; 29:10–20.
[12] Rose AM, Valdes R Jr. Understanding the sodium pump and its relevance to disease. Clin Chem. 1994; 40:1674–1685.
[13]Hsu IL, Chou CY, Wu YY, et al. Targeting FXYD2 by cardiac glycosides potently blocks tumor growth in ovarian clear cell carcinoma. Oncotarget. 2016;7:62925-62938.
[14]Alix-Panabieres C, Riethdorf S, Pantel K. Circulating tumor cells and bone marrow micrometastasis. Clin Cancer Res 2008;14:5013-21
[15]Fan T, Zhao Q, Chen JJ, Chen WT, Pearl ML. Clinical significance of circulating tumor cells detected by an invasion assay in peripheral blood of patients with ovarian cancer. Gynecol Oncol 2009;112:185-91
[16]Wan JCM, Massie C, Garcia-Corbacho J, Mouliere F, Brenton JD, Caldas C, et al. Liquid biopsies come of age: towards implementation of circulating tumour DNA. Nat Rev Cancer 2017;17:223-38
[17]Yap TA, Lorente D, Omlin A, Olmos D, de Bono JS. Circulating tumour cells: a multifunctional biomarker. Clin Cancer Res 2014;20:2553-68.
[18]Pravin D. Potdar, Navjeet Kaur Lotey. Role of circulating tumor cells in future diagnosis and therapy of cancer. .J Cancer Metastasis Treat. 2015;1:44-56.
[19]Zhivotosky B, Orrenius S. Assessment of apoptosis and necrosis by DNA fragmentation and morphological criteria. Curr. Protoc. Cell Biol. Chapter 18, Unit 18.3 (2001).
Tables and figures
Table 1. List of ovarian cancer tissue bank of NCKU Gynecologic Lab.
Pathology Number
Clear cell type 10
Serous type 11
Mucinous type 8
Endometrioid type 5
Others 3
Non-tumor 31
Table 2. Clinical characteristics and plasma cfDNA concentration of 68 samples.
qPCR
FXYD2_143bp
Name Tumor stage
Tumor cell type
Plasma volume (ml)
Elution volume
(ul)
Ct cfDNA conc.
(ng/ml)
Ovarian Cancer
P1-S 蘇 O 慧 IIIC Serous 1 30 29.26 10.69
P3-S 林 O 華 IIIC Serous 1 30 27.16 53.81
P5-S 詹 O 靜 IIIC Serous 1 30 28.2 24.21
P7-S 林 O 瓴 I Serous 1 30 27.07/30.02 70.62
P9-S 陳 O 玲 IIIC Serous 1 30 27.44/32.50 59.85
P11-S 許 O 英 IIIC Serous 1 30 26.83/30.41 78.43
P13-S 王 O 葉 IV Serous 1 30 30.91 47.55
P15-S 洪陳 O 江 IIIC Serous 1 30 30.15 73.4
P17-S 田 O 敏 IIB Serous 1 30 31.37 36.66
P19-S 陳 O 真 IIa Serous 1 30 31.78 1.27
P21-S 王 O 梅 IVB Serous 1 30 30.05 2.47
P2-C 林 O 麗 IC Clear Cell 1 30 28.77 15.61
P4-C 陳 O 華 IIa Clear Cell 1 30 29.14 11.7
P6-C 洪 O 玫 IV Clear Cell 1 30 27.58 38.89
P8-C 黃 O 紂 IC Clear Cell 1 30 27.24/31.65 65.34
P10-C 杜 O 惠 I Clear Cell 1 30 28.65/31.35 35.18
P12-C 陳 O 玲 IIIC Clear Cell 1 30 27.64/31.80 54.89
P14-C 林 O 真 IC Clear cell 1 30 30.84 49.61
P16-C 蘇 O 雯 IA Clear cell 1 30 32.78 16.4
P18-C 林 O 敏 IA Clear cell 1 30 32.34 21.12
P20-C 林 O 燕 IA Clear cell 1 30 31.91 1.16
P101-M 蕭 O 玲 IA mucin 1 30 30.19 2.22
P103-M 陳 O 美 IC mucin 1 30 30.8 1.37
P105-M 溫 O 倩 IA mucin 1 30 30.65 32.12
P107-M 陳 O 燕 IIC mucin 1 30 32.51 9.77
P109-M 楊 O 鈺 IA mucin 1 30 32.65 3.73
P111-M 柯 O 女勻 IC mucin 1 30 31.18 10.58
P113-M 蔡 O 美 IA mucin 1 30 31.94 6.17
P115-M 饒柯 O 葉 IC mucin 1 30 33.42 2.16
P102-O 李 O 旭 X Granulosa cell 1 30 32.4 0.39
P104-O 黃 O 倫 I Granulosa cell 1 30 31.28 21.39
P106-O 吳 O 紛 IA Ovarian
adenosarcoma 1 30 30.98 12.14
P201-E 郭 O 娟 IB Emdo 1 30 33.35 5.7
P203-E 李石 O 美 IC Emdo 1 30 32.05 13.07
P205-E 楊 O 菁 IIIC Emdo 1 30 33.58 1.92
P207-E 陳 O 嬿 IIA Emdo 1 30 32.35 4.6
P209-E 張 O 萍 IC Emdo 1 30 32.1 5.48
Normal Control
N1 黃 O 琴 1 30 28.41 20.5
N2 林 O 玲 1 30 28.79 15.4
N3 黃 O 蘭 1 30 29.44 9.32
N4 邱 O 心 1 30 27.02/31.14 72.17
N5 蔡 O 燕 1 30 26.74/32.18 81.53
N6 蔡 O 函 1 30 28.90/33.39 31.51
N7 張 O 蓁 1 30 28.41/31.73 39.08
N8 吳 O 岑 1 30 34.3316 6.8
N9 杜 O 綠 1 30 31.8217 28.32
N10 楊 O 婷 1 30 31.7181 30.04
N11 林 O 晴 1 30 33.3013 12.21
N12 吳 O 芬 1 30 34.29 0.22
N13 黛 O 葉 1 30 32.3 0.88
N14 鄭 O 蓁 1 30 31.84 1.23
N15 邱殷 O 玉 1 30 31.23 0.97
N16 曾 O 呤 1 30 31.39 0.86
N17 王陳 O 姬 1 30 30.84 1.33
N18 廖 O 恩 1 30 29.83 2.95
N19 許 O 慧 1 30 32.62 0.32
N20 陳 O 琍 1 30 29.2 4.83
N21 蔡 O 吟 1 30 33.46 5.32
N22 郭 O 伶 1 30 32.81 8.05
N23 林吳 O 麗 1 30 28.9 97.87
N24 沈 O 蓉 1 30 32.3 11.15
N25 劉蘇 O 香 1 30 30.85 28.18
N26 侯 O 萍 1 30 30.95 12.37
N27 方 O 麗 1 30 31.76 6.98
N28 吳 O 琪 1 30 31.06 11.49
N29 楊 O 君 1 30 32.26 4.91
N30 王 O 玉 1 30 31.29 9.78
N31 林 O 雯 1 30 32.9 3.11
Table 3. List for average of plasma FXYD2 cfDNA concentration (ng/ml) in different ovarian cancer types and non-tumor control.
Table 4. The situation of tumor formation in the patient-derived tumor xenograft (PDX) mice model.
Figure 1. Human FXYD2 gene expression in OCCC is higher than non-OCCC. (A) FXYD2 gene expression in human cell lines. (B) Human FXYD2 gene expression in clinical specimens. (C) A standard curve base on the TOV-21G genomic DNA concentration and Ct value can be used to calculat the cell-free DNA concentration.
Figure 2. FXYD2 expression in ovarian cancer cell lines and IC50 of TOV-21G, ES-2, SKOV3, and normal cells treated with Digoxin. (A) Protein expression level of FXYD2 on OCCC and non- OCCC cells. (B) In Digoxin treatment, TOV-21G cells was more senstitive than other cells.
Figure 3. The IC50 of TOV-21G, SKOV3 and normal cells under the 8 CG compounds, Digoxin and cisplatin treatment.
Cell line : H9C2
(M)
0 1 10 50 100 150 200 300
Cell viability of control (%)
20 40 60 80 100 120
Digoxin CG #14
IC50 = 132.0M
IC50 = 13.8M Cell line : H9C2
(M)
0 1 10 50 100 150 200 300
Cll ibilif l (%)
20 40 60 80 100 120
Digoxin CG #14
IC50 = 132.0M
IC50 = 13.8M
Figure 4. The cytotoxicity assay of cardiomyoma cell line. IC50 of H9C2 cells under the Digoxin (132 μM) or BPR1P0014S0 (neriifolin) (13.8 μM) treatment. The H9C2 cells were sentitive in Digoxin treatment more than in BPR1P0014S0 (neriifolin) treatment.
Figure 5. A ovarian cancer orthotopic xenograft model was established to confirm the BPR1P0014S0 (neriifolin) therapeutic effect. (A) 5 x 104 TOV-21G GL cells or ES-2 GL cells were local injected into NOD/SCID mice ovarian (n=5). Tumor formation was observed at 7-14 days after tumor cells injection through IVIS image system, and then start to treated with Digoxin. (B) After treated with Digoxin, tumor grew rate and tumor volume were reduced in TOV-21G GL xenograft mice as compare with ES-2 GL xenograft mice. (C-D) In TOV-21G GL xenograft mice, tumor volume reduced after BPR1P0014S0 (neriifolin) treatment as compare with no treatment. But BPR1P0014S0 (neriifolin) treatment no effect on ES-2 GL xenograft mice.
108年度專題研究計畫成果彙整表
計畫主持人:許耿福 計畫編號:108-2314-B-006-003- 計畫名稱:探討FXYD2在臨床卵巢亮細胞癌病人的角色(2/2)
成果項目 量化 單位
質化
(說明:各成果項目請附佐證資料或細 項說明,如期刊名稱、年份、卷期、起 訖頁數、證號...等)
國
內 學術性論文
期刊論文 0
研討會論文 0 篇
專書 0 本
專書論文 0 章
技術報告 0 篇
其他 0 篇
國
外 學術性論文
期刊論文 0
研討會論文 0 篇
專書 0 本
專書論文 0 章
技術報告 0 篇
其他 0 篇
參 與 計 畫 人 力
本國籍
大專生 0
人次
碩士生 0
博士生 0
博士級研究人員 0
專任人員 1 碩士級專案人員 莊媛喆
非本國籍
大專生 0
碩士生 0
博士生 1 非本國籍博士生-白明旭
博士級研究人員 0
專任人員 0
其他成果
(無法以量化表達之成果如辦理學術活動
、獲得獎項、重要國際合作、研究成果國 際影響力及其他協助產業技術發展之具體 效益事項等,請以文字敘述填列。)
在此計畫中,我們證實了CG compounds可能成為卵巢癌的 治療標靶,而具有治療潛力。除了將此部分研究成果撰寫 學術論文,對未來卵巢癌的治療策略亦有另一個參考價值
。一旦提高卵巢癌的治癒率,不僅可減少病患的焦慮感
,亦可減少健保費用在治療癌症用藥的支出。