行政院國家科學委員會專題研究計畫 期中進度報告
於正常與退化性頸椎模式探討椎間植入器植入於去椎間盤
術後之生物力學, 放射學, 與組織病理學上之長期效益(1/3)
計畫類別: 個別型計畫 計畫編號: NSC91-2320-B-006-086-執行期間: 91 年 08 月 01 日至 92 年 07 月 31 日 執行單位: 國立成功大學醫學系外科 計畫主持人: 李宜堅 報告類型: 精簡報告 處理方式: 本計畫可公開查詢中
華
民
國 92 年 5 月 23 日
研究計畫中英文摘要:
請就本計畫要點作一概述,並依本計畫性質自訂關鍵 詞。(計畫中文摘要。(五百字以內) (第一年半)
Keywords: 頸椎去椎間盤術 (cervical discectomy), 前位椎板固定術 (anterior-plate fixation) , 椎間盤骨移植 (intervertebral bone grafting), 椎間盤 cage 移植 (intervertebral cage implant).
本研究設計為一含三年期計劃. 我們將逐年研究探討頸椎前位椎板固定術 與否, 與有無椎間盤骨移植 (intervertebral bone grafting)和椎間盤 cage 移植 (intervertebral cage implant)對於實驗兔去頸椎椎間盤術之生物力學與骨融合之影 響與相關機轉. 近年來 cage 是脊椎手術之一熱門話題. 數個國外知名臨床人體 研究均發現其是一椎間盤骨移植加強或替代物, 並可避免骨移植 donor-site morbidity (such as chronic pain), 是以不論國內國外均有增加使用趨勢. 然而於 human cadaveric spine model, cage 之生物力學特性無法支持其是一椎間盤骨移植 加強或替代物, 是以我們認為 cage 應具有延遲性生物力學特性影響去頸椎椎間 盤術後之力學重整(biomechanical redistribution)與骨融合值得進一步做研究. 於計劃第一年半, 我們將利用大白兔 2-functional units 正常頸椎模式, 以逐步 研究探討有無頸椎去椎間盤術 (cervical discectomy), 前位椎板固定術
(anterior-plate fixation) , 椎間盤骨移植 (intervertebral bone grafting), 椎間盤 cage 移植 (intervertebral cage implant)之遲性生物力學特性去頸椎椎間盤術後之力學
重整(biomechanical redistribution)與骨融合之影響. 於術後半年, 應用放射攝影 與影像處理系統計算 optical bone mineral density 並評估 quality of solid fusion and osteophytes 大小影響. 經由一前導實驗, 我們解決兔子實驗困難之氣管插管. 是 以本模式值得進一步研究探討. 此研究成果將前導後面一年半度一連串於兔子 2-functional unit cervical spines 相關實驗,並提供一本土實體頸椎生物力學與臨床 應用研究前景.
(第二年半)
Keywords: 頸椎去椎間盤術 (cervical discectomy), 前位椎板固定術
(anterior-plate fixation) , 椎間盤骨移植 (intervertebral bone grafting), 椎間盤 cage 移植 (intervertebral cage implant), 退化性頸椎 (degenerative cervical spines). 本研究設計為一含三年期計劃. 我們將逐年研究探討頸椎前位椎板固定術 與否, 與有無椎間盤骨移植 (intervertebral bone grafting)和椎間盤 cage 移植 (intervertebral cage implant)對於實驗兔去頸椎椎間盤術之生物力學與骨融合之影 響與相關機轉. 近年來 cage 是脊椎手術之一熱門話題. 數個國外知名臨床人體 研究均發現其是一椎間盤骨移植加強或替代物, 並可避免骨移植 donor-site morbidity (such as chronic pain), 是以不論國內國外均有增加使用趨勢. 然而於 human cadaveric spine model, cage 之生物力學特性無法支持其是一椎間盤骨移植 加強或替代物, 是以我們認為 cage 應具有延遲性生物力學特性影響去頸椎椎間 盤術後之力學重整(biomechanical redistribution)與骨融合值得進一步做研究, 於
第二, 三年我們將研究這些處置於 degenerative spine model 影響.
於計劃第一年半, 我們將利用大白兔 2-functional units 退化性頸椎模式, 以進 一步研究探討有無頸椎去椎間盤術 (cervical discectomy), 前位椎板固定術 (anterior-plate fixation) , 椎間盤骨移植 (intervertebral bone grafting), 椎間盤 cage 移植 (intervertebral cage implant)之遲性生物力學特性去頸椎椎間盤術後之力學 重整(biomechanical redistribution)與骨融合於 degenerative spines 之影響. 我們將 先行製造 3-functional unit degenerative cervical spines 於術後三個月, 再進行正式 手術, 於正式手術術後半年, 應用放射攝影與影像處理系統計算 optical bone mineral density 並評估 quality of solid fusion and osteophytes 大小影響. 經由一前 導實驗, 我們解決製造 degenerative cervical spines 技術. 是以本模式值得進一步 研究探討. 此研究成果將提供一連串於兔子 2-functional unit degenerative cervical spines 相關實驗,並提供一本土實體頸椎生物力學與臨床應用研究前景.
(一)計畫英文摘要。(五百字以內) (第一年半)
Keywords: Cervical discectomy, anterior-plate fixation, intervertebral bone grafting, intervertebral cage implant.
This study will be conducted to compare the kinematic influence of anterior cervical discectomy with and without bone grafting and anterior-plate fixation and
the role of Cage implant in a condition involving late fusion in the intact cervical spines.
Forty-eight adult New Zealand White rabbits will be included, and eight of which will undergo a sham operation and serves as normal controls (Group A, n=8). Eight animals will receive C3-C4 anterior cervical discectomy alone (Group B, n=8). The other thirty-two animals will receive C3-C4 anterior cervical discectomy plus other stabilization or fusion procedures. Intervertebral autologous iliac bone grafting (Group C, n=8) and complementary stabilization either with the Cage implant (Group D, n =8) or anterior Caspar plate (Group E, n =8) will be immediately performed at the C3-C4 level. The remaining 8 animals will receive C3-C4 anterior cervical discectomy and will be re-stabilized by the use of cage and anterior-plate fixation (Group F, n=8). Postoperatively, the animals will receive radiographic examinations and will be killed six months later. Fresh ligamentous spines (C1-C6) will be subjected to the relevantly applied loads through a loading frame attached to the C1. Each vertebra (from C3 to C5) will be attached with a set of three infrared light-emitting diodes (LEDs) to record their spatial locations relating to each load application using a Selspot II system (Selcom Selective Electronic, Inc., Valdese, NC). The load-deformation data of C3-4 and C4-5 motion segments will be recorded and analyzed for the six groups. In addition, radiographic and histologic
examinations will be employed.
(二)計畫英文摘要。(五百字以內) (第二年半)
Keywords: Cervical discectomy, anterior-plate fixation, intervertebral bone grafting, intervertebral cage implant, degenerative spines.
This study will be conducted to compare the kinematic influence of anterior cervical
discectomy with and without bone grafting and the role of Cage implant in a condition
involving late fusion in degenerative cervical spines.
Six-four adult New Zealand White rabbits will be included, and eight of which will
undergo sham operation and serves as normal controls (Group A, n=8). The other 56 animals
received an induced cervical spinal degenerative injury by multiple incision to the
intervertebral disc at the C2-C3, C3-C4, and C4-C5 levels. Three months later, radiographic
examinations will be performed to verify the presence of relevant degenerative changes. For
the 56 animals subjected to induced degenerative spine injury, eight animals will receive
sham operation which serves as degenerative controls (Group B, n=8). The other forty-eight
animals will further receive C3-C4 anterior cervical discectomy, including the 8 animals
which will receive exclusive discectomy surgery (Group C, n=8). Intervertebral autologous
iliac bone grafting (Group D, n=8) or stand-alone cage (Group E, n=8) will be immediately
either with anterior Caspar plate (Group F, n =8) or Cage implant (Group G, n =8) or the two
in combination (Group H, n=8). Postoperatively, the animals received radiographic
examinations and were killed six months later. Fresh ligamentous spines (C1-C6) will be
subjected to the relevantly applied loads through a loading frame attached to the C1. Each
vertebra (from C3 to C5) will be attached with a set of three infrared light-emitting diodes
(LEDs) to record their spatial locations relating to each load application using a Selspot II
system (Selcom Selective Electronic, Inc., Valdese, NC). The load-deformation data of C3-4
and C4-5 motion segments will be recorded and analyzed for the eight groups. Additionally, radiographic and histologic examinations will be employed.
前言
Anterior cervical fusion was firstly described, by Robinson and Smith in 1955, to treat cervical disc disease, and has been widely accepted to treat degenerative cervical disc disease, acute cervical disc protrusion, and fracture-dislocation of the cervical spine. In the past two decades, numerous implant systems have been developed to treat unstable cervical spine disease arising from trauma, a tumor, or surgical
treatment. Choosing an appropriate approach by which a satisfactory stability can be obtained has therefore become an important issue for the clinical practice of spinal surgeons. Among various surgical approaches, anterior spinal fixation can obtain favorable immediate stability of the whole anterior column and a part of middle column and, thus, has been considered as an excellent treatment modality to achieve satisfactory fusion results in the treatment of unstable cervical spine disorder. For cervical disc disease, the anterior-plate fixation has also been suggested for those patient s at risk to develop soft tissue fusion, although most authors agree that an independent use of bone bulk across the discectomied space is enough for achieving solid bone fusion and maintaining disc height. On the other hand, a great deal of researchers emphasize that facets’ immobilization is essential for consolidation of bone grafting of the functional unit to be fused during a course of healing. This
concept, combined with the anatomic favorable condition for posterior fusion, has also led to the development of various posterior fixation techniques. However, posterior sublaminar wiring, combined with various techniques of structural bone grafting, may need the dangerous passage of sublaminar wires. Additionally, the posterolateral fixation technique is technically demanding and has a potential risk of injury to the vertebral artery. Moreover, this procedure cannot be used in the presence of fixed subluxation and in the case with an aberrant path of the vertebral artery. These problems have resulted in the prevalence of anterior fusion with and without complementary fixation for various cervical spine disorders.
Anterior cervical interbody fusion, however, may lead to the clinical morbidity and complications in the donor site in up to 25% cases with autologous bone grafting. These problems have led neurosurgeon to seek alternative methods for obtaining spinal fusion without potential risks of donor site morbidity. In the past several years, a proliferation in the use of stand-alone interbody fusion cages has been seen for surgical treatment of degenerative disc disease in the lumbar spine. Also, these interbody fusion cage devices have been developed and used in degenerative disc disease of the cervical spine. These implants, filled with cancellous bone tissues, are intended to decrease graft site complication and to promote solid interbody
ossification.
Sophisticated knowledge of kinematic and biomechanical data is important. It not only provides valuable information for determining the optimal surgical approach but also may be helpful to predict the late complication due to biomechanical stress redistribution following surgery. Although numerous studies have been dedicated to evaluate the biomechanical properties with regards to various surgical procedures in the cadaveric spines (with and without surgical disruptions to anatomical contour). Rare, if ever to date, has been aimed to evaluate the influence of these procedures over time in animal models that were designed to evaluate the late fusion results in a condition with degenerative spines.
Using a sheep cervical spine model involving late fusion, we have previously shown that anterior cervical fusion did not completely eliminate the intervertebral motion of the functional unit, presumably as a result of movements at the facet joints. In that study, C2-C3 cervical discectomy without bone grafting formed a dense soft tissue response with irregular and noncontinuing bone bridges across the discectomied space that could oppose the lateral bending but not the axial rotation loads. This biomechanical redistribution in rotation load occurred not only at the functional unit with discectomy (C2-C3) but also at the adjacent functional unit (C3-C4). Following the insertion of intervertebral bone grafting, the discectomy-relevant increases in the motion ranges of rotation loads much improved over time. This finding was explained
by that C2-C3 anterior discectomy redistributed the motility of both the C2-C3 and the C3-C4 functional units toward relative hypermotility in rotation over time, which could be attenuated by the consolidation of the bone grafting masses across the discectomied space.
However, C2-C3 cervical discectomy was also noted to associate with an
increased motion range of flexion load at the C3-C4 functional unit, probably due to a mechanically related mechanism over time acting to compensate for decreased stress absorption in flexion caused by the loss of the C2-C3 disc. Solid fusion achieved by the intervertebral grafting, however, could not reverse this biomechanical change over time. It has been known that mechanical implant fixation may possess a load-sharing or shielding biomechanical character and, thus, may have potential to oppose the undesirable excess of physiological loads over time, either caused by discectomy or the loss of functional disc, onto the adjacent levels of the cervical spines. We therefore supposed that perhaps using an implant fixation bridging across the space of
discectomy and bone grafting, the excessive transfer of flexion load onto contiguous functional units might be much diminished and this kinematic change improved.
An ideal stabilization method, therefore, should include dual biomechanical properties not only providing immediate stabilization for the functional unit to be fixed but also allowing an appropriate amount of physiological stresses transferring onto the bone graft and the adjacent functional unit. Thus, solid bony fusion can be obtained without the occurrence of deleterious biomechanical effects. Certainly, either anterior-plate or posterior-wired fixation can not completely fit both the two criteria, and, thus, should not be recommended as an optimal procedure in dealing with all the cases of unstable cervical spine disorder and/or degenerative spine disease.
Expectation, however, has arisen with the development of cage devices for the management of degenerative cervical spine disorders.
In a recent research in human cadaveric spines of Shimamoto et al., they concluded that the anterior plate showed significantly lower range of motion in flexion/extension loads for the reconstructed functional unit than did the cage and the autograft. The cage-implanted spines indicated significantly higher range of motion in
flexion/extension loads for the reconstructed functional unit than the intact spines. Thus, avoiding the potential donor-site morbidity seemed to be the only benefit of cage treatment. These in vitro biomechanical data also did not favor a routine use of cage for those patients with degenerative spine disorder or at risk for developing soft tissue fusion although the two conditions have been widely considered as relative surgical indications for the use of cage implant in clinical practice. One unsolved problem in the study of Shimamoto et al. was that these kinematic data of cadaveric spines could not represent a condition that might occur in degenerative spines, a state
that has been suggested for the application of cage implant in clinical scenario. Curiously, there have also been several satisfactory clinical reports of stand-alone cervical interbody cage fusion for the surgical management of degenerative disc disease. Thus, it is reasonably to suppose that cage may lead to delayed
biomechanical redistribution during healing, and the event may further influence the bone-remodeling process and, thus, results in satisfactory late fusion results observed in clinical reports. Undoubtedly, these influencing factors can only be investigated through a well-designed experimental degenerative spinal model in animals.
In order to extend our original findings and in line with current treatment
modalities suggested fro degenerative cervical spine disorders, we herein investigate the kinematics of late fusion results following cervical discectomy and intervertebral bone grafting plus an anterior plate or cage fixation in both the intact and degenerative cervical spine models. Although we have developed a one-level degenerative cervical spine model in sheep, we consider that a well-designed degenerative spine model may need to include at least three functional units so as to simulate the clinical scenario mostly involved in degenerative cervical spine disease in human beings. In the study, we, therefore, plan to use a three-level degenerative cervical spine model in rabbits because the sheep have a strong longus colli musculature not easily to performed induced degeneration of multiple functional units of the cervical spines.
研究目的
1. In the clinical spine study, stand-alone cage implant ahs been shown an excellent fusion rate that is slightly better than those previously reported using autologous interbody bone grafts. However, the biomechanical data of cadaveric spine failed to provide a consistent biomechanical data. This discrepancy indicates a need for biomechanical study focusing on late fusion results in experimental cervical spine model.
2. In a 2-functional-unit cervical spine model in New Zealand White rabbits, we plan to evaluate the potentially beneficial effect of stand-alone interbody cage implant in cervical disc disease.
3. We will evaluate whether the cage implant can reverse the rotational hypermotility of the functional unit adjacent ot the level with cervical discectomy.
4. We will also compare the kinematic differences between the cage treatment and the other treatment modalities, including discectomy alone, discectomy with bone grafting, and discectomy with bone grafting plus anterior-plate fixation. 5. We will compare the late results of intervertebral fusion among different groups
following a prolonged recovery period.
6. By simultaneous measurements of the functional unit adjacent to discectomy, we will further decipher whether cage implant is a load-sharing or –shielding
property for the functional unit to be fused. 結果與討論(含結論與建議)
Sixteen adult New Zealand White male rabbits, each weighing 4-5 kg, were involved in this experiment in the past months. Anesthesia was induced by 4% halothane and be maintained by 100% O2. These animals were intubated and
mechanically ventilated with a respirator. With the animals in the supine position and its head in normal cervical lordosis, a right vertical incision was done along the anterior border of the sternocleidomastoid muscle. With the carotid sheath laterally retracted, the deep cervical fascia overlying the longus colli muscles and the anterior longitudinal ligament were incised in the midline and dissected from the vertebral bodies and from the adherent annulus fibrosus of the disc. The level of exposed vertebrae was verified by a lateral radiograph of cervical spine initially, but now we could palpate the anterior prominence of the atlas to ensure the disc space of C3-C4. C3-C4 discectomy was employed through incising the annulus and then removing the nucleus and the remaining cartilaginous end plates. The harvest and the insertion of autologous iliac crest graft were performed according to the Smith-Robinson technique. C3-C4 discectomy without bone grafting were performed in six animals and another four animals were received the insertions of autologous iliac crest
grafting after C3-C4 cervical discectomy. Six rabbits were included in the sham group as intact controls. The sternocleidomastoid muscle EMG was done during operation and repeated radiographs were performed in the duration of 3 months after operation to ensure the spine stability and bone fusion. As for the groups which will undergo C3-C4 discectomy and insertion of stand-alone cage with/without Caspar plate and screws instrumentation were under proceeding due to mini-instruments required and technique difficulty.
The preliminary data showed mild kyphotic deformity change in the group which underwent C3-C4 discectomy alone and well bone fusion in the group of C3-C4 discectomy with insertion of autologous bone graft in radiological studies. The EMG data demonstrated that no obvious amplitude decrease or duration prolonged
happened during operation. We had previously demonstrated that anterior cervical discectomy without bone graft lost the disc space and increased the chance of kyphosis and posterior osteophytes formation in sheep model.
Fig. 1 Intraoperative picture showed anterior surface of the C2, C3, and C4
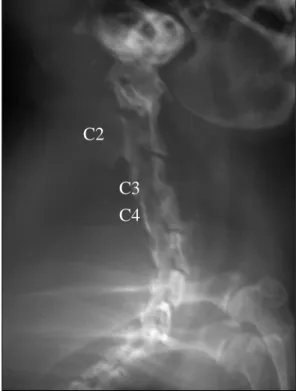
Fig2. C3-C4 discectomy without bone graft C2 C3 C4
Fig. 3: C3-C4 discectomy with interbody bone fusion