https://doi.org/10.1007/s12012-018-9484-9
Risk of Myocardial Infarction After Carbon Monoxide Poisoning:
A Nationwide Population-Based Cohort Study
Chien‑Cheng Huang1,2,3,4,5 · Chung‑Han Ho6,7 · Yi‑Chen Chen6 · Hung‑Jung Lin1,8,9 · Chien‑Chin Hsu1,8 · Jhi‑Joung Wang6 · Shih‑Bin Su5,10,11 · How‑Ran Guo2,12
Published online: 22 September 2018
© Springer Science+Business Media, LLC, part of Springer Nature 2018
Abstract
Carbon monoxide poisoning (COP) may lead to ischemic changes in organs, and heart is one of the most susceptible targets to ischemic condition. The objective of this study is to evaluate the risk of myocardial infarction following COP. Using a nationwide database of insurance claims in Taiwan, we conducted a population-based cohort study to identify COP patients diagnosed between 1999 and 2012. At a ratio of 3:1, we identified non-COP patients who were matched by the index date and age and compared the risk of myocardial infarction between the two cohorts by time after the index dates of the COP patients, until 2013. We identified 22,258 COP patients and 66,774 non-COP patients. COP patients had an increased risk of myocardial infarction, with an incidence rate ratio of 1.45 (95% confidence interval 1.06–1.98) in comparison with the non-COP patients after adjusting for other independent predictors, including older age, male sex, and underlying comorbid- ity of hypertension, diabetes, and renal disease. Stratified analyses showed that the increased risk was more prominent in patients with a young age (< 34 years), female sex, and liver disease, and occurred only in the first month of follow-up. We concluded that COP increased the risk of myocardial infarction, but the increased risk was only observed in the first month after COP, which indicated that the impact of COP on the heart was mainly acute. Patients who were younger than 34 years, female, and with liver diseases were more prone to myocardial infarction after COP.
Keywords Carbon monoxide · Heart · Myocardial infarction · Myocardial injury · Poisoning Abbreviations
COP Carbon monoxide poisoning CO Carbon monoxide
NPD Nationwide Poisoning Database
LHID2000 Longitudinal Health Insurance Database CAD 2000 Coronary artery disease
ICD-9 International Classification of Diseases-9 HIV Human immunodeficiency virus
NTD New Taiwan Dollars IRR Incidence rate ratios CI Confidence interval AHR Adjusted hazard ratio HBOT Hyperbaric oxygen therapy
Introduction
Carbon monoxide (CO) comes from an incomplete combus- tion of organic matter and is known as a “silent killer” due to its 200- to 240-fold affinity for hemoglobin compared with oxygen [1, 2]. In the United States, carbon monoxide poison- ing (COP) contributes to 50,000 emergency department vis- its and 2700 deaths annually [2, 3]. In Taiwan, COP occurs not only from unintentional causes such as malfunctioning heating appliances, but also frequently from suicide attempts [4]. Because CO is odorless and fatal, COP by charcoal burning became a popular method for suicide in Chinese society since the first case was reported in Hong Kong [5].
A study in Taiwan reported that charcoal burning became the second most-favored method for suicide and accounted for 33.5% of total suicide deaths in Taiwan in 2006 [4]. The incidence of charcoal-burning suicide was 0.22 per 100,000 in 1999 but increased to 6.48 per 100,000 in 2006 [4].
Hypoxia due to CO’s competitive binding with hemo- globin is the major mechanism for the toxicity of COP [1, 2, 6]. The heart and brain have the highest oxygen demands and
Handling Editor: Gen Suzuki.
* How-Ran Guo
Extended author information available on the last page of the article
therefore are the organs most commonly damaged by COP [1, 2, 6–8]. Myocardial infarction has been found to occur in patients with acute COP [9, 10]. In addition, COP induces inflammatory and immunological reactions in the heart [1, 2, 11–21], which may also increase the risk of subsequent myo- cardial infarction. However, the long-term effects of COP on myocardial infarction are rarely evaluated, and subgroup analyses by age, sex, and co-morbidities have seldom been carried out. To fill the data gaps, we conducted a retrospec- tive nationwide population-based cohort study.
Methods
Data SourcesWe conducted this study using two sub-databases from the National Health Insurance Database: the Nationwide Poison- ing Database (NPD) and the Longitudinal Health Insurance Database 2000 (LHID2000). The NPD contains data on all patients of poisoning (including COP) in Taiwan between 1999 and 2013. The LHID2000 contains the registration and claim data of 1,000,000 individuals randomly selected from the original National Health Insurance Research Database [22]. Large, computerized databases derived from this sys- tem by the National Health Insurance Administration (the former Bureau of National Health Insurance), Ministry of Health and Welfare (the former Department of Health), Taiwan, and maintained by the National Health Research Institutes, Taiwan, are provided to scientists in Taiwan for research purposes [22].
Definitions, Variables, and Outcomes
We identified COP patients using the International Classi- fication of Diseases-9 (ICD-9) codes 986, E868, E952, and E982 either during admission or ambulance care, listed in the NPD between 1999 and 2012 (Fig. 1). Non-COP patients were identified from the LHID2000 by matching the index date and age with COP patients at a ratio of 3:1. The index date was defined as the date of admission or ambulatory care for COP patients. We excluded patients who had coronary artery disease (CAD) (ICD-9: 410–414) before the index date and stratified the age as < 20, 20–34, 35–49, 50–64, and
≥ 65 years. The underlying co-morbidities included in this study were hypertension (ICD-9: 401–405), diabetes (ICD- 9: 250), hyperlipidemia (ICD-9: 272), malignancy (ICD-9:
140–208), stroke (ICD-9: 436–438), dementia (ICD-9: 290), congestive heart failure (ICD-9: 428), chronic obstructive pulmonary disease (ICD-9: 496), liver disease (ICD-9:
570–576), renal disease (ICD-9: 580–593), connective tis- sue disease (ICD-9: 710), HIV infection (ICD-9: 042, 07953, V08), drug abuse (ICD-9: 303–305), and mental disorder
(ICD-9: 290–302, 306–319). Monthly income was classi- fied as < 19,999, 20,000–39,999, and ≥ 40,000 New Taiwan Dollars (NTD). Myocardial infarction was defined as ICD-9 410.
Comparison of the Risk of Myocardial Infarction Between COP and Non‑COP Patients
Following up the two cohorts until 2013, we compared the risk of myocardial infarction between them. We performed both overall analyses and stratified analyses according to age, sex, underlying co-morbidities, and follow-up period (Fig. 1). In addition, we tried to identify the independent pre- dictors for myocardial infarction and evaluate their effects.
Statistical Analyses
We used the two-sample t test and the Chi square test to evaluate the differences in continuous variables and cat- egorical variables, respectively. Estimated incidence rate ratios (IRRs) were obtained using Poisson regression with adjustment for sex, underlying co-morbidities (hypertension, diabetes, hyperlipidemia, malignancy, stroke, dementia, chronic obstructive pulmonary disease, liver disease, renal disease, connective tissue disease, and mental disorder), and monthly income. Kaplan–Meier analysis and the log-rank test were used to compare the risks of myocardial infarction
NPD All patients with COP between 1999 and 2012
LHID2000
Patients without COP randomly selected between 1999 and 2012 Patients with coronary artery disease before index date were excluded
Matching COP vs. non-COP (1:3) by the index date and age
Study cohort COP patients n = 22,258
Comparison cohort Non-COP patients
n = 66,774 Follow up until 2013
Compare the risk of myocardial infarction between COP and non-COP patients
Investigate the independent predictors of myocardial infarction by Cox proportional hazard regression analysis
Fig. 1 Flowchart of this study. NPD Nationwide Poisoning Database, LHID Longitudinal Health Insurance Database, COP carbon monox- ide poisoning
between the two cohorts during the follow-up period. Strati- fied analyses by age, sex, underlying co-morbidities, and fol- low-up periods were performed to investigate potential effect modifications. In addition, we used Cox proportional hazard regressions to identify independent predictors of myocar- dial infarction and estimate their effects. Specifically, we constructed a “full model” which included all the variables with p values < 0.05 in the univariate analyses, and then a
“reduced model” in which all the variables were statistically significant. All the analyses were performed using SAS 9.4 for Windows (SAS Institute, Cary, NC, USA) at a two-tailed significance level of 0.05.
Results
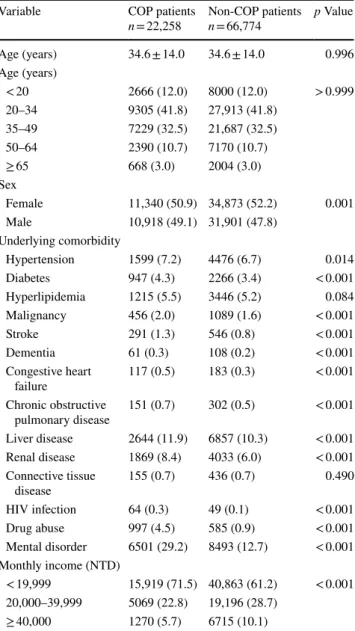
The mean age of the COP cohort was 34.6 years, with a standard deviation of 14.0 years (Table 1). The majority of COP patients were in the age group 20–34 years (41.81%), followed by 35–49 years (32.48%). In the COP patients, 51.0% were females. In comparison with the non-COP patients, the COP patients had higher prevalence rates of hypertension, diabetes, malignancy, stroke, dementia, con- gestive heart failure, chronic obstructive pulmonary dis- ease, liver disease, renal disease, HIV infection, drug abuse, and mental disorder, and had lower monthly incomes (all p < 0.05).
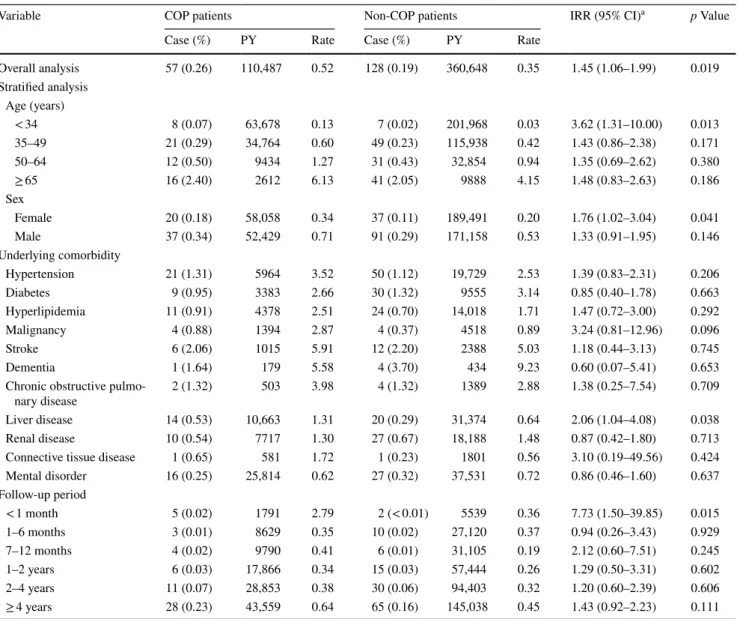
We observed a higher risk of myocardial infarction in COP patients during the follow-up, with an IRR of 1.45 after adjustment for sex; the underlying co-morbidities of hypertension, diabetes, hyperlipidemia, malignancy, stroke, dementia, chronic obstructive pulmonary disease, liver dis- ease, renal disease, connective tissue disease, and mental disorder; and monthly income (95% confidence interval [CI]
1.06–1.99) (Table 2). We did not adjust for HIV infection and drug abuse because there were zero cases of myocardial infarction in the COP patients who had HIV infection or drug abuse. Both the Kaplan–Meier analysis and the log- rank test showed a significant difference between the two cohorts (p = 0.0175) (Fig. 2). In stratified analyses, we found the increased risk was more prominent in young (< 34 years old) patients (IRR 3.62; 95% CI 1.31–10.00), female patients (IRR 1.76; 95% CI 1.02–3.04), patients with liver disease (IRR 2.06; 95% CI 1.04–4.08), and the first month of follow- up (IRR 7.73; 95% CI 1.50–39.85), which indicated that these variables were effect modifiers. No significant differ- ences in the risk of myocardial infarction were observed after 1 month of follow-up between COP and non-COP cohorts.
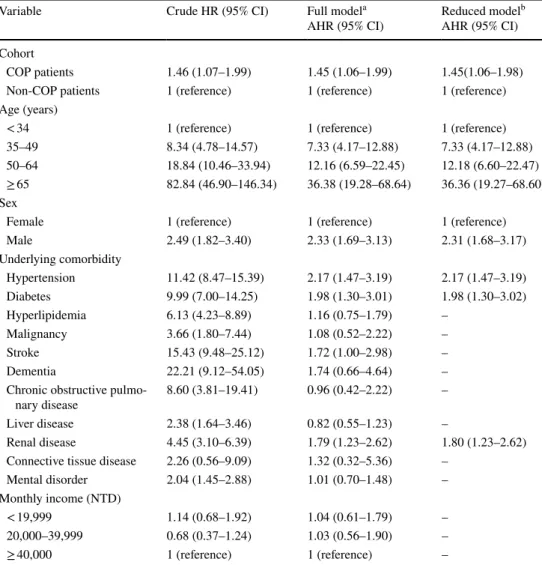
Cox proportional hazard regression analyses showed that independent predictors of myocardial infarction included COP (adjusted hazard ratio [AHR] 1.45; 95%
CI 1.06–1.98), older age, male sex (AHR 2.31; 95% CI
1.68–3.17), hypertension (AHR 2.17; 95% CI 1.47–3.19), diabetes (AHR 1.98; 95% CI 1.30–3.02), and renal disease (AHR 1.80; 95% CI 1.23–2.62) (Table 3). There were no remarkable differences in the AHR estimates between the full and the reduced models.
Discussion
This retrospective nationwide population-based cohort study showed that the risk of myocardial infarction increased after COP. Stratified analysis showed that the increased risk was more prominent in patients with a young (< 34 years)
Table 1 Comparison of age, sex, underlying co-morbidities, and monthly income between COP and non-COP patients
COP carbon monoxide poisoning, NTD New Taiwan Dollars. Data are expressed as means ± SD or n (%)
Variable COP patients
n = 22,258 Non-COP patients
n = 66,774 p Value
Age (years) 34.6 ± 14.0 34.6 ± 14.0 0.996
Age (years)
< 20 2666 (12.0) 8000 (12.0) > 0.999
20–34 9305 (41.8) 27,913 (41.8)
35–49 7229 (32.5) 21,687 (32.5)
50–64 2390 (10.7) 7170 (10.7)
≥ 65 668 (3.0) 2004 (3.0)
Sex
Female 11,340 (50.9) 34,873 (52.2) 0.001
Male 10,918 (49.1) 31,901 (47.8)
Underlying comorbidity
Hypertension 1599 (7.2) 4476 (6.7) 0.014
Diabetes 947 (4.3) 2266 (3.4) < 0.001
Hyperlipidemia 1215 (5.5) 3446 (5.2) 0.084 Malignancy 456 (2.0) 1089 (1.6) < 0.001
Stroke 291 (1.3) 546 (0.8) < 0.001
Dementia 61 (0.3) 108 (0.2) < 0.001
Congestive heart
failure 117 (0.5) 183 (0.3) < 0.001
Chronic obstructive
pulmonary disease 151 (0.7) 302 (0.5) < 0.001 Liver disease 2644 (11.9) 6857 (10.3) < 0.001 Renal disease 1869 (8.4) 4033 (6.0) < 0.001 Connective tissue
disease 155 (0.7) 436 (0.7) 0.490
HIV infection 64 (0.3) 49 (0.1) < 0.001
Drug abuse 997 (4.5) 585 (0.9) < 0.001
Mental disorder 6501 (29.2) 8493 (12.7) < 0.001 Monthly income (NTD)
< 19,999 15,919 (71.5) 40,863 (61.2) < 0.001 20,000–39,999 5069 (22.8) 19,196 (28.7)
≥ 40,000 1270 (5.7) 6715 (10.1)
age, female sex, and liver disease, and occurred in the first month of follow-up only. After the acute poisoning period (< 1 month), changes in the risk of myocardial infarction in COP patients did not reach statistical significance. The independent predictors of myocardial infarction identified in our study were COP, older age, male sex, hypertension, diabetes, and renal disease.
This study showed that the effect of COP on myocar- dial infarction was acute and occurred mainly in the first month after the exposure to CO. In other words, COP did not increase the long-term risk of myocardial infarction, and this finding is compatible with a previous study [9]. Some studies that used cardiac biomarkers or electrocardiography for defining myocardial infarction reported that 37% of the
patients with moderate to severe COP had a concomitant myocardial infarction [10, 23]. In these patients, the in-hos- pital mortality was 5%, and the long-term all-cause mortality was 38% after a median follow-up of 7.6 years; both were higher than those in the COP patients without myocardial infarction [10, 23]. Another study reported that all COP patients with myocardial infarction were found to have nor- mal coronary arteries without evidence of vasospasm shown by coronary angiogram [9]. The systolic function of the left ventricle may be normal or mildly to severely impaired, but most of the myocardial dysfunction disappeared within 1 day [9], suggesting that the mechanism of COP-related myocar- dial infarction is not via the coronary artery, but via other processes such as tissue hypoxia and myocardial stunning
Table 2 Comparison of the risk of myocardial infarction Between COP and non-COP patients by estimating the IRR with Poisson regression
COP carbon monoxide poisoning, IRR incidence rate ratio, PY person-year, CI confidence interval.
a Adjusted for sex, underlying comorbidities (hypertension, diabetes, hyperlipidemia, malignancy, stroke, dementia, chronic obstructive pulmo- nary disease, liver disease, renal disease, connective tissue disease, and mental disorder), and monthly income
Variable COP patients Non-COP patients IRR (95% CI)a p Value
Case (%) PY Rate Case (%) PY Rate
Overall analysis 57 (0.26) 110,487 0.52 128 (0.19) 360,648 0.35 1.45 (1.06–1.99) 0.019
Stratified analysis Age (years)
< 34 8 (0.07) 63,678 0.13 7 (0.02) 201,968 0.03 3.62 (1.31–10.00) 0.013
35–49 21 (0.29) 34,764 0.60 49 (0.23) 115,938 0.42 1.43 (0.86–2.38) 0.171
50–64 12 (0.50) 9434 1.27 31 (0.43) 32,854 0.94 1.35 (0.69–2.62) 0.380
≥ 65 16 (2.40) 2612 6.13 41 (2.05) 9888 4.15 1.48 (0.83–2.63) 0.186
Sex
Female 20 (0.18) 58,058 0.34 37 (0.11) 189,491 0.20 1.76 (1.02–3.04) 0.041
Male 37 (0.34) 52,429 0.71 91 (0.29) 171,158 0.53 1.33 (0.91–1.95) 0.146
Underlying comorbidity
Hypertension 21 (1.31) 5964 3.52 50 (1.12) 19,729 2.53 1.39 (0.83–2.31) 0.206
Diabetes 9 (0.95) 3383 2.66 30 (1.32) 9555 3.14 0.85 (0.40–1.78) 0.663
Hyperlipidemia 11 (0.91) 4378 2.51 24 (0.70) 14,018 1.71 1.47 (0.72–3.00) 0.292
Malignancy 4 (0.88) 1394 2.87 4 (0.37) 4518 0.89 3.24 (0.81–12.96) 0.096
Stroke 6 (2.06) 1015 5.91 12 (2.20) 2388 5.03 1.18 (0.44–3.13) 0.745
Dementia 1 (1.64) 179 5.58 4 (3.70) 434 9.23 0.60 (0.07–5.41) 0.653
Chronic obstructive pulmo-
nary disease 2 (1.32) 503 3.98 4 (1.32) 1389 2.88 1.38 (0.25–7.54) 0.709
Liver disease 14 (0.53) 10,663 1.31 20 (0.29) 31,374 0.64 2.06 (1.04–4.08) 0.038
Renal disease 10 (0.54) 7717 1.30 27 (0.67) 18,188 1.48 0.87 (0.42–1.80) 0.713
Connective tissue disease 1 (0.65) 581 1.72 1 (0.23) 1801 0.56 3.10 (0.19–49.56) 0.424
Mental disorder 16 (0.25) 25,814 0.62 27 (0.32) 37,531 0.72 0.86 (0.46–1.60) 0.637
Follow-up period
< 1 month 5 (0.02) 1791 2.79 2 (< 0.01) 5539 0.36 7.73 (1.50–39.85) 0.015
1–6 months 3 (0.01) 8629 0.35 10 (0.02) 27,120 0.37 0.94 (0.26–3.43) 0.929
7–12 months 4 (0.02) 9790 0.41 6 (0.01) 31,105 0.19 2.12 (0.60–7.51) 0.245
1–2 years 6 (0.03) 17,866 0.34 15 (0.03) 57,444 0.26 1.29 (0.50–3.31) 0.602
2–4 years 11 (0.07) 28,853 0.38 30 (0.06) 94,403 0.32 1.20 (0.60–2.39) 0.606
≥ 4 years 28 (0.23) 43,559 0.64 65 (0.16) 145,038 0.45 1.43 (0.92–2.23) 0.111
[9, 10, 24]. In some case reports, coronary artery occlu- sion was found in COP patients, but these reports could not determine a causal relationship between COP and coronary artery occlusion [25–27]. In addition to acute intoxication as we studied, CO is an important air pollutant, and a meta- analysis showed that CO increased the risk for myocardial infarction (relative risk 1.048; 95% CI 1.026–1.070) [28], which support the conclusion of an association between COP and myocardial infarction in our study. In addition to hypoxia, COP may induce immunological and inflammatory damages to the heart via reactive oxygen species production by the following mechanisms: (1) binding to intracellular proteins, (2) nitric oxide generation and peroxynitrite pro- duction, (3) lipid peroxidation by neutrophils, (4) mitochon- drial oxidative stress, (5) apoptosis (programmed cell death), (6) immune-mediated injury, and (7) delayed inflammation [1, 2, 11–21].
In this study, age was matched between COP and non- COP patients, and therefore we could not identify the high risk age of COP. However, through stratified analyses, we found that age was an effect modifier of COP, with young (< 34 years) being more vulnerable to COP-associated myocardial infarction. We also found that sex is an effect modifier of COP, with the female sex being more vulner- able. These results are compatible with those in a pre- vious nationwide cohort study which reported that COP increased mortality especially in the younger (< 30 years) and female patients [29]. Previous studies on risk factors for myocardial infarction also revealed that females were more sensitive than males to the harmful effects of smok- ing, diabetes, elevated triglycerides, and left ventricular hypertrophy [30, 31]. Interactions between the risk factors (including smoking) and hormonal factors (including oral contraceptive use and hormone replacement therapy) may
be involved in the development of myocardial infarction [30, 31]. This may also be true in the case of COP. While we found that liver disease was also an effect modifier like age and sex, we could not find any previous reports by using “liver disease,” “myocardial injury,” “myocardial infarction,” and “carbon monoxide” to search literature indexed by the PubMed. Therefore, this is very likely to be a novel finding. In addition, our study also showed that older age, male sex, hypertension, diabetes, and renal dis- ease were independent predictors for myocardial infarc- tion, which are known as conventional risk factors for myocardial ischemia reported in the literature [29, 32, 33].
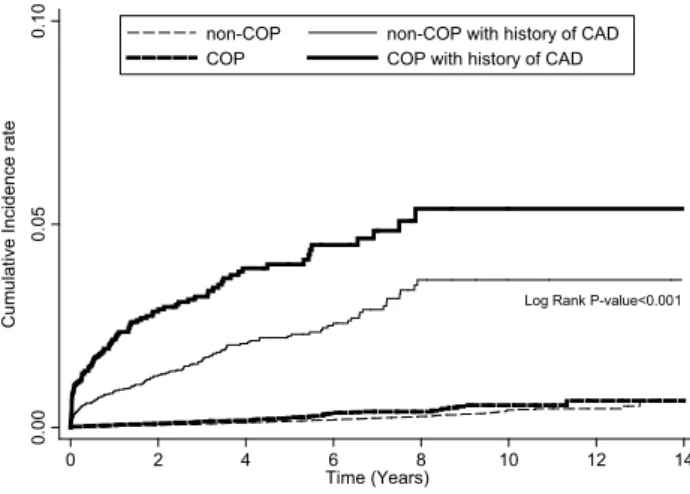
In order to evaluate the effect of CAD, which was excluded in the initial analysis, we performed a compari- son between COP patients with history of CAD and non- COP patients with history of CAD and found that COP patients with history of CAD were more vulnerable to myocardial injury than non-COP patients with history of CAD (IRR 2.00; 95% CI 1.52–2.63 and Fig. 3). The cur- rent result is compatible with previous human and envi- ronmental studies. Some prospective studies on males with CAD revealed that low levels of carboxyhemoglobin exac- erbate myocardial ischemia during graded exercise [34, 35]. A multicenter cohort study in European also showed that ambient CO increased risk of hospital cardiac read- missions in patients with CAD [36]. Another multicenter study in the United States reported a positive association between short-term exposure to ambient CO and the risk of hospitalizations for cardiovascular disease [37]. A recent meta-analysis revealed that myocardial infarction can be triggered by air pollution, physical exertion, alco- hol, and coffee; however, these estimates did not account for the contribution of CO [38]. The current study found that COP is a triggering factor for myocardial infarction and suggested that in addition to particular matters, CO may be another air pollutant that may contribute to the occurrence of myocardial infarction.
Various methods have been suggested for diagnosing myocardial infarction caused by COP, including electrocar- diogram, echocardiography, scintiscanning, coronarography, single photon emission computed tomography, and levels of troponin I, B-type natriuretic peptide, creatine kinase, and creatine kinase-MB [9, 39–41]. Further studies are warranted to identify the ones that are best for screening and monitoring after COP, the standard treatment for COP is administration of oxygen via non-rebreathing mask or endotracheal intubation in order to provide nearly 100% of oxygen, which shortens the half-life of CO from 320 min on normal air to 80 min [1]. Hyperbaric oxygen therapy (HBOT) is also suggested for patients with COP, espe- cially for those with severe poisoning, to reduce neurologi- cal sequelae, which are the most common and concerning complication [1]. However, the benefit of HBOT in limiting
Log Rank P-value=0.0175
0.000.01250.025
Cumulative Incidence rate
66749 53611 40449 28168 14936 6720 2043 non-COP COP 21912 16537 12231 8425 4475 1990 615 Number at risk
0 2 4 6 8 10 12 14
Time (Years)
COP non-COP
Fig. 2 Comparison of the risk of myocardial injury between COP and non-COP patients by Kaplan–Meier analysis and log-rank test. COP carbon monoxide poisoning
or reversing myocardial infarction is still unknown [41, 42], and further studies are needed to address this issue.
Although our study has a large sample size and thus is able to perform stratified analyses and evaluate the effects of multiple risk factors for myocardial infarction at the same time, it has some limitations. First, using ICD-9 codes to identify patients with myocardial infarction may underes- timate the incidence. Despite there is a good sensitivity of 88% using ICD-9 code 410 to identify myocardial infarction or injury [43], some patients might be missed. However, this is not expected to cause remarkable bias because both COP and non-COP cohorts had the same issue of misclassifica- tion. Second, the impact of HBOT was not evaluated. But, as we discussed earlier, the effect of HBOT in such cases is still unknown [42], and thus further studies are warranted
to address this issue. Third, we did not have information on smoking, which is an important risk factor for myocardial infarction. Because the prevalence of smoking in Taiwanese females is very low (4.4% in 2011 [44]), the effects of smok- ing on the results have been minimized when the analyses were adjusted for sex.
Conclusion
This study showed that COP increased the acute risk of myocardial infarction within 1 month, especially in patients who are < 34 years, females, or with liver disease. The independent predictors of myocardial infarction after COP include older age, male sex, and underlying comorbidity of
Table 3 Predictors of myocardial infarction in all patients by Cox proportional hazard regression analysis
COP carbon monoxide poisoning, HR hazard ratio, AHR adjusted hazard ratio, CI confidence interval, NTD New Taiwan Dollars
a Adjusted for age, sex, underlying comorbidities (hypertension, diabetes, hyperlipidemia, malignancy, stroke, dementia, chronic obstructive pulmonary disease, liver disease, renal disease, connective tissue dis- ease, and mental disorder), and monthly income
b Adjusted for age, sex, and the underlying comorbidities of hypertension, diabetes, and renal disease
Variable Crude HR (95% CI) Full modela
AHR (95% CI) Reduced modelb AHR (95% CI) Cohort
COP patients 1.46 (1.07–1.99) 1.45 (1.06–1.99) 1.45(1.06–1.98)
Non-COP patients 1 (reference) 1 (reference) 1 (reference)
Age (years)
< 34 1 (reference) 1 (reference) 1 (reference)
35–49 8.34 (4.78–14.57) 7.33 (4.17–12.88) 7.33 (4.17–12.88)
50–64 18.84 (10.46–33.94) 12.16 (6.59–22.45) 12.18 (6.60–22.47)
≥ 65 82.84 (46.90–146.34) 36.38 (19.28–68.64) 36.36 (19.27–68.60)
Sex
Female 1 (reference) 1 (reference) 1 (reference)
Male 2.49 (1.82–3.40) 2.33 (1.69–3.13) 2.31 (1.68–3.17)
Underlying comorbidity
Hypertension 11.42 (8.47–15.39) 2.17 (1.47–3.19) 2.17 (1.47–3.19)
Diabetes 9.99 (7.00–14.25) 1.98 (1.30–3.01) 1.98 (1.30–3.02)
Hyperlipidemia 6.13 (4.23–8.89) 1.16 (0.75–1.79) –
Malignancy 3.66 (1.80–7.44) 1.08 (0.52–2.22) –
Stroke 15.43 (9.48–25.12) 1.72 (1.00–2.98) –
Dementia 22.21 (9.12–54.05) 1.74 (0.66–4.64) –
Chronic obstructive pulmo-
nary disease 8.60 (3.81–19.41) 0.96 (0.42–2.22) –
Liver disease 2.38 (1.64–3.46) 0.82 (0.55–1.23) –
Renal disease 4.45 (3.10–6.39) 1.79 (1.23–2.62) 1.80 (1.23–2.62) Connective tissue disease 2.26 (0.56–9.09) 1.32 (0.32–5.36) –
Mental disorder 2.04 (1.45–2.88) 1.01 (0.70–1.48) –
Monthly income (NTD)
< 19,999 1.14 (0.68–1.92) 1.04 (0.61–1.79) –
20,000–39,999 0.68 (0.37–1.24) 1.03 (0.56–1.90) –
≥ 40,000 1 (reference) 1 (reference) –
hypertension, diabetes, or renal disease. While the results have casted some light on the risk of myocardial infarction after COP, further studies are needed to identify the best methods for screening and monitoring myocardial infarction after COP, as well as the effect of HBOT.
Author contributions C-C Huang and H-RG designed and conceived this study and wrote the manuscript. H-CH and Y-CC performed the statistical analysis and wrote the manuscript. H-JL, C-C Hsu, J-JW, and S-BS provided professional suggestions and wrote the manuscript. All the authors have read and approved the final manuscript.
Funding This study was supported by Grants CMFHR10677 and CMFHR10734 from the Chi-Mei Medical Center.
Compliance with Ethical Standards
Conflict of interest The authors declare no potential conflicts of inter- est.
Ethical Approval This study involved human data and was conducted in strict accordance with the Declaration of Helsinki. The study protocol was approved by the Institutional Review Board (IRB) at the Chi-Mei Medical Center.
Informed Consent The two databases consisted of depersonalized information, and so the requirement of informed consent was waived by the IRB as the study did not affect the welfare of the participants.
References
1. Weaver, L. K. (2009). Clinical practice. Carbon monoxide poison- ing. New England Journal of Medicine 360, 1217–1225.
2. Hampson, N. B., & Weaver, L. K. (2007). Carbon monoxide poi- soning: A new incidence for an old disease. Undersea & Hyper- baric Medicine, 34, 163–168.
3. Lee, F. Y., Chen, W. K., Lin, C. L., et al. (2015). Carbon monoxide poisoning and subsequent cardiovascular disease risk: A nation- wide population-based cohort study. Medicine (Baltimore), 94, e624.
4. Pan, Y. J., Liao, S. C., & Lee, M. B. (2010). Suicide by charcoal burning in Taiwan, 1995–2006. Journal of Affective Disorders, 120, 254–257.
5. Lee, D. T., Chan, K. P., Lee, S., et al. (2002). Burning charcoal:
A novel and contagious method of suicide in Asia. Archives of General Psychiatry, 59, 293–294.
6. Ernst, A., & Zibrak, J. D. (1998). Carbon monoxide poisoning.
New England Journal of Medicine, 339, 1603–1608.
7. Zou, J. F., Guo, Q., Shao, H., et al. (2015). Lack of pupil reflex and loss of consciousness predict 30-day neurological sequelae in patients with carbon monoxide poisoning. PLoS ONE, 10, e0119126.
8. Zou, J. F., Guo, Q., Shao, H., et al. (2014). A positive Babinski reflex predicts delayed neuropsychiatric sequelae in Chinese patients with carbon monoxide poisoning. BioMed Research International, 2014, 814736.
9. Kalay, N., Ozdogru, I., Cetinkaya, Y., et al. (2007). Cardiovascular effects of carbon monoxide poisoning. The American Journal of Cardiology, 99, 322–324.
10. Satran, D., Henry, C. R., Adkinson, C., et al. (2005). Cardio- vascular manifestations of moderate to severe carbon monoxide poisoning. Journal of the American College of Cardiology, 45, 1513–1516.
11. Hampson, N. B., Piantadosi, C. A., Thom, S. R., et al. (2012).
Practice recommendations in the diagnosis, management, and prevention of carbon monoxide poisoning. American Journal of Respiratory and Critical Care Medicine, 186, 1095–1101.
12. Brown, S. D., & Piantadosi, C. A. (1989). Reversal of carbon monoxide–cytochrome c oxidase binding by hyperbaric oxygen in vivo. Advances in Experimental Medicine and Biology, 248, 747–754.
13. Brown, S. D., & Piantadosi, C. A. (1990). In vivo binding of carbon monoxide to cytochrome c oxidase in rat brain. Journal of Applied Physiology, 68, 604–610.
14. Brown, S. D., & Piantadosi, C. A. (1992). Recovery of energy metabolism in rat brain after carbon monoxide hypoxia. Journal of Clinical Investigation, 89, 666–672.
15. Piantadosi, C. A., Zhang, J., Levin, E. D., et al. (1997). Apoptosis and delayed neuronal damage after carbon monoxide poisoning in the rat. Experimental Neurology, 147, 103–114.
16. Thom, S. R. (1990). Antagonism of carbon monoxide–mediated brain lipid peroxidation by hyperbaric oxygen. Toxicology and Applied Pharmacology, 105, 340–344.
17. Thom, S. R., Bhopale, V. M., Fisher, D., et al. (2004). Delayed neuropathology after carbon monoxide poisoning is immune- mediated. Proceedings of the National Academy of Sciences of the USA, 101, 13660–13665.
18. Thom, S. R., Bhopale, V. M., & Fisher, D. (2006). Hyperbaric oxygen reduces delayed immune-mediated neuropathology in experimental carbon monoxide toxicity. Toxicology and Applied Pharmacology, 213, 152–159.
19. Thom, S. R., Bhopale, V. M., Han, S. T., et al. (2006). Intravas- cular neutrophil activation due to carbon monoxide poisoning.
American Journal of Respiratory and Critical Care Medicine, 74, 1239–1248.
20. Thom, S. R. (2008). Carbon monoxide pathophysiology and treat- ment. In T. S. Neuman & S. R. Thom (Eds.), Physiology and medicine of hyperbaric oxygen therapy (pp. 321–347). Philadel- phia: Saunders Elsevier.
21. Thom, S. R., Bhopale, V. M., Milovanova, T. M., et al. (2010).
Plasma biomarkers in carbon monoxide poisoning. Clinical Toxi- cology (Philadelphia), 48, 47–56.
Log Rank P-value<0.001
0.000.050.10Cumulative Incidence rate
0 2 4 6 8 10 12 14
Time (Years)
non-COP non-COP with history of CAD
COP COP with history of CAD
Fig. 3 Comparison of the risk of myocardial injury between COP patients with history of CAD and non-COP patients with history of CAD and between COP and non-COP patients (i.e., without history of CAD in the Fig. 2) by Kaplan–Meier analysis and log-rank test.
COP carbon monoxide poisoning, CAD coronary artery disease
22. National Health Insurance Administration, Ministry of Health and Welfare, Taiwan, R.O.C. (2014). National Health Insurance Annual Report 2014–2015.
23. Henry, C. R., Satran, D., Lindgren, B., et al. (2006). Myocardial injury and long-term mortality following moderate to severe car- bon monoxide poisoning. JAMA, 295, 398–402.
24. Tritapepe, L., Macchiarelli, G., Rocco, M., et al. (1998). Func- tional and ultrastructural evidence of myocardial stunning after acute carbon monoxide poisoning. Critical Care Medicine, 26, 797–801.
25. Dziewierz, A., Ciszowski, K., Gawlikowski, T., et al. (2013). Pri- mary angioplasty in patient with ST-segment elevation myocardial infarction in the setting of intentional carbon monoxide poisoning.
The Journal of Emergency Medicine, 45, 831–834.
26. Sward, D. G., Sethuraman, K. N., Wong, J. S., et al. (2016).
Carbon monoxide and ST-elevation myocardial infarction: case reports. Undersea & Hyperbaric Medicine, 43, 63–69.
27. Unlu, M., Ozturk, C., Demirkol, S., et al. (2016). Thrombolytic therapy in a patient with inferolateral myocardial infarction after carbon monoxide poisoning. Human & Experimental Toxicology, 35, 101–105.
28. Mustafic, H., Jabre, P., Caussin, C., et al. (2012). Main air pol- lutants and myocardial infarction: A systematic review and meta- analysis. JAMA, 307, 713–721.
29. Huang, C. C., Chung, M. H., Weng, S. F., et al. (2014). Long- term prognosis of patients with carbon monoxide poisoning: A nationwide cohort study. PLoS ONE, 9, e105503.
30. Jónsdóttir, L. S., Sigfússon, N., Gudnason, V., et al. (2002). Do lipids, blood pressure, diabetes, and smoking confer equal risk of myocardial infarction in women as in men? The Reykjavik Study.
Journal of Cardiovascular Risk, 9, 67–76.
31. Anand, S. S., Islam, S., Rosengren, A., et al. (2008). Risk factors for myocardial infarction in women and men: Insights from the INTERHEART study. European Heart Journal, 29, 932–940.
32. Prescott, E., Hippe, M., Schnohr, P., et al. (1998). Smoking and risk of myocardial infarction in women and men: Longitudinal population study. BMJ, 316, 1043–1047.
33. Sarnak, M. J., Levey, A. S., Schoolwerth, A. C., et al. (2003).
Kidney disease as a risk factor for development of cardiovascu- lar disease: a statement from the American Heart Association Councils on kidney in cardiovascular disease, high blood pressure research, clinical cardiology, and epidemiology and prevention.
Circulation, 108, 2154–2169.
34. Allred, E. N., Bleecker, E. R., Chaitman, B. R., et al. (1989).
Short-term effects of carbon monoxide exposure on the exercise performance of subjects with coronary artery disease. New Eng- land Journal of Medicine, 321, 1426–1432.
35. Kleinman, M. T., Davidson, D. M., Vandagriff, R. B., et al. (1989).
Effects of short-term exposure to carbon monoxide in subjects with coronary artery disease. Archives of Environmental Health, 44, 361–369.
36. von Klot, S., Peters, A., Aalto, P., et al. (2005). Ambient air pollu- tion is associated with increased risk of hospital cardiac readmis- sions of myocardial infarction survivors in five European cities.
Circulation, 112, 3073–3079.
37. Bell, M. L., Peng, R. D., Dominici, F., et al. (2009). Emergency hospital admissions for cardiovascular diseases and ambient levels of carbon monoxide: Results for 126 United States urban counties, 1999–2005. Circulation, 120, 949–955.
38. Nawrot, T. S., Perez, L., Künzli, N., Munters, E., & Nemery, B.
(2011). Public health importance of triggers of myocardial infarc- tion: A comparative risk assessment. Lancet, 377, 732–740.
39. Yücel, M., Avsarogullari, L., Durukan, P., et al. (2016). BNP shows myocardial injury earlier than Troponin-I in experimental carbon monoxide poisoning. European Review for Medical and Pharmacological Sciences, 20, 1149–1154.
40. Szponar, J., Kołodziej, M., Majewska, M., et al. (2012). Myocar- dial injury in the course of carbon monoxide poisoning. Przegl Lek, 69, 528–534.
41. Lippi, G., Rastelli, G., Meschi, T., et al. (2012). Pathophysiology, clinics, diagnosis and treatment of heart involvement in carbon monoxide poisoning. Clinical Biochemistry, 45, 1278–1285.
42. Garg, J., Krishnamoorthy, P., Palaniswamy, C., et al. (2014). Car- diovascular abnormalities in carbon monoxide poisoning. Ameri- can Journal of Therapeutics. https ://doi.org/10.1097/MJT.00000 00000 00001 6.
43. Cheng, C. L., Lee, C. H., Chen, P. S., et al. (2014). Validation of acute myocardial infarction cases in the national health insur- ance research database in taiwan. Journal of Epidemiology, 24, 500–507.
44. Health Promotion Adminstration, Ministry of Health and Welfare, Taiwan. Health indicators 123. Retrieved from https ://olap.hpa.
gov.tw/en_US/Index .aspx?menu=-1&vid=1.
Affiliations
Chien‑Cheng Huang1,2,3,4,5 · Chung‑Han Ho6,7 · Yi‑Chen Chen6 · Hung‑Jung Lin1,8,9 · Chien‑Chin Hsu1,8 · Jhi‑Joung Wang6 · Shih‑Bin Su5,10,11 · How‑Ran Guo2,12
Chien-Cheng Huang
[email protected] Chung-Han Ho
[email protected] Yi-Chen Chen
[email protected] Hung-Jung Lin
[email protected] Chien-Chin Hsu [email protected] Jhi-Joung Wang
Shih-Bin Su
1 Department of Emergency Medicine, Chi-Mei Medical Center, Tainan, Taiwan
2 Department of Environmental and Occupational Health, College of Medicine, National Cheng Kung University, 1 Daxue Road, East District, Tainan City 701, Tainan, Taiwan
3 Department of Senior Services, Southern Taiwan University of Science and Technology, Tainan, Taiwan
4 Department of Geriatrics and Gerontology, Chi-Mei Medical Center, Tainan, Taiwan
5 Department of Occupational Medicine, Chi-Mei Medical Center, Tainan, Taiwan
6 Department of Medical Research, Chi Mei Medical Center, Tainan, Taiwan
7 Department of Pharmacy, Chia Nan University of Pharmacy and Science, Tainan, Taiwan
8 Department of Biotechnology, Southern Taiwan University of Science and Technology, Tainan, Taiwan
9 Department of Emergency Medicine, Taipei Medical University, Taipei, Taiwan
10 Department of Leisure, Recreation and Tourism Management, Southern Taiwan University of Science and Technology, Tainan, Taiwan
11 Department of Medical Research, Chi-Mei Medical Center, Liouying, Tainan, Taiwan
12 Department of Occupational and Environmental Medicine, National Cheng Kung University Hospital, Tainan, Taiwan