國立台灣大學 公共衛生學院 流行病學與預防醫學研究所
碩士論文
Graduate Institute of Epidemiology and Preventive Medicine College of Public Health
National Taiwan University Master Thesis
比較第二型糖尿病患者以 metformin 及 sulfonylurea 治療仍控 制不良時加上 pioglitazone 或 sitagliptin 之療效
Efficacy and safety of adding pioglitazone or sitagliptin to patients with type 2 diabetes insufficiently controlled with
metformin and a sulfonylurea
劉松臻 Sung-Chen, Liu
指導教授:簡國龍 教授 Advisor: Kuo-Liong Chien, Prof.
中華民國 101 年 6 月
致謝
本研究得以完成首先要特別感謝我的指導老師,簡國龍教授的教導。簡教授 對於學術的認真與嚴謹態度,讓我們對於研究有更深入的認識與瞭解。雖然學習 過程中有些挫折與煎熬,但老師往往適時給了我們前進的動力,並提供我們解決 問題的方法,讓我能順利完成本論文。
本班同學大多數都是在職生,雖然平時都有工作要忙,但大家平時上課都互 相鼓勵與合作,讓我們有段難忘的學習歷程,在此也要謝謝每位同學的幫忙。
最後我要向我的太太,姿君,說聲謝謝,感謝妳盡心的照顧好兩個小寶貝並 且忍受我有時的不耐煩,讓我在工作、上課時能夠沒有後顧之憂,你們給我的溫 暖是我最強的支柱。
中文摘要
背景與研究目的:第 2 型糖尿病是一種進行性的慢性疾病,往往需要逐漸增加降血糖藥物才能 有效控制血糖。metformin 及 sulfonylurea 為最常見的治療組合,且是一些治療指 引建議的第一線與第二線口服降血糖藥物。但隨著疾病的進行血糖往往無法達到 治療目標,此時需要加上其他降血糖藥物來控制血糖。pioglitazone(愛妥糖)與 sitagliptin (佳糖維)常被用來當作第三線的治療藥物,但沒有研究直接比較兩種藥 物在治療效果與副作用上的差異。
研究對象與方法:
已經用 metformin(≥1500mg/d)及 sulfonylurea(≥ half maximal dose)治療仍控制 不良(糖化血色素≥7.0 % and <11%)的第 2 型糖尿病患者,隨機分配加上 pioglitazone(每日一錠 30 毫克;59 人) 或 sitagliptin (每日一錠 100 毫克;60 人) 治 療24 周。
結果:
糖化血色素在 pioglitazone 組與 sitagliptin 組分別下降 0.94± 0.12 %與 0.71±
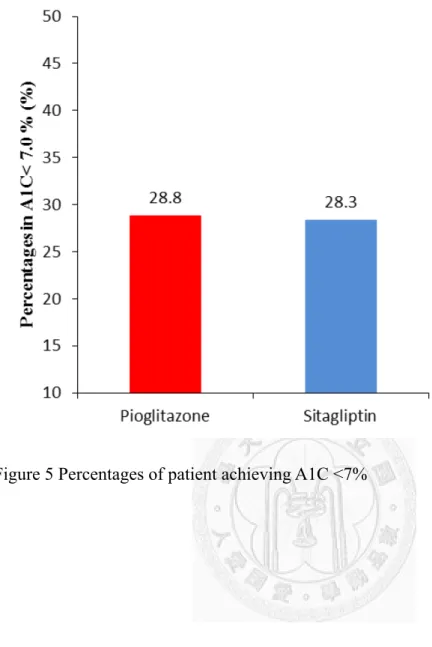
0.12 %,兩組間沒有差異(-0.23±0.16 %;p=0.16)。 pioglitazone 組有 28.8%、
sitagliptin 組有 28.3%的患者達到糖化血色素小於 7.0%的目標。空腹血糖在 pioglitazone 組與 sitagliptin 組分別下降 35.7± 4. 0mg/dl 與 22.8± 4.0mg/dl,兩組 之間有顯著的差異(-12.9±5.7mg/dl;p=0.02)。HOMA-IR、三酸甘油脂與 high sensitive CRP 在 pioglitazone 組顯著比 sitagliptin 組下降較多,而高密度膽固醇在 pioglitazone 組顯著比 sitagliptin 組升高。治療後 pioglitazone 組顯著比 sitagliptin
組體重增加 1.6±0.5 公斤。整體上兩組在副作用與低血糖發生的比率上沒有差
異,但pioglitazone 組周邊水腫發生的機會較高(27% vs. 0%),而 sitagliptin 組腸 胃道副作用發生的機會較高(20%vs.6.8%)。
結論:
糖尿病患者以 metformin 及 sulfonylurea 治療仍控制不良時加上 pioglitazone
或sitagliptin 之療效相當。但兩組在空腹血糖、HOMA-IR、三酸甘油脂、高密度
膽固醇、high sensitive CRP 與體重的變化上有顯著的異。
關鍵字:第2 型糖尿病、愛妥糖、佳糖維、胰島素增敏劑、二肽基酶-4 抑制劑
ABSTRACT
Background: Type 2 diabetes is a progressive illness which most patients experience
a progressive deterioration in glycemic control, dual combination therapy with metformin and a sulfonylurea also may not achieve or maintain glycemic control.Objective: To evaluate the efficacy and safety of add-on pioglitazone vs. sitagliptin in
patients with type 2 diabetes inadequately controlled on dual therapy.Methods: This 24-week, randomized, open-label, randomized, parallel study
compared pioglitazone (30 mg daily, n=59) and sitagliptin (100 mg daily, n=60) inpatients with inadequate glycemic control (glycosylated hemoglobin A1c [A1C] ≥ 7.0% to <11.0%) while receiving a stable dose of metformin (≥1500 mg daily) and a sulfonylureas (≥half maximal dose).
Results: Mean (±s.e.) change in A1C from baseline was -0.94± 0.12 % with
pioglitazone and -0.71± 0.12 % with sitagliptin, for a between groups difference of -0.23±0.16 % (p=0.16). The percentages of patient achieving A1C <7% were 28.8%and 28.3% in the pioglitazone and sitagliptin groups, respectively. Mean change in fasting plasma glucose were -35.7± 4.0mg/dl with pioglitazone and -22.8± 4.0mg/dl with sitagliptin, for a between groups difference of-12.9±5.7mg/dl (p=0.02).
Pioglitazone was associated with significant decrease in HOMA-IR, triglyceride, hs-CRP and increase high-density lipoprotein cholesterol, while sitagliptin did not
induce changes in these parameters. Mean weight gain was higher in the pioglitazone group with a between-group difference of 1.60kg (p<0.01). Overall adverse events and the rate of hypoglycemia were similar in both groups. However, the incident of edema was higher with pioglitazone vs. sitagliptin (27% vs. 0%) and the incident of gastrointestinal adverse events was higher with sitagliptin vs. pioglitazone (20%
vs.6.8%).
Conclusions: Pioglitazone and sitagliptin achieved similar improvements in overall
glycemic control in patients with type 2 diabetes inadequately controlled withmetformin and a sulfonylurea. However there were some differences in terms of FPG, lipids, HOMA-IR, body weight change and adverse events.
Key words: type 2 diabetes, pioglitazone, sitagliptin, thiazolidinedione, DPP4-inhibitors
CONTENTS
口試委員會審定書 ...i
致謝 …...……….……….ii
中文摘要 ... iii
ABSTRACT ... v
CONTENTS ... 1
Chapter 1: Introduction ... 4
Chapter 2: Literature review ... 6
2.1 Pioglitazone ... 6
2.1.1 Mechanism: ... 6
2.1.2 Efficacy ... 6
2.1.3 Safety and tolerability ... 7
2.2 Sitagliptin ... 7
2.2.1 Mechanism: ... 7
2.2.2 Efficacy ... 8
2.2.3 Safety and tolerability ... 8
2.3 Research gap ... 9
Chapter 3: Materials and Methods ... 10
3.1 Patients ... 10
3.1.1 Inclusion criteria ... 10
3.1.2 Execution criteria ... 10
3.2 Study Design ... 10
3.3 Withdrawal Criteria ... 11
3.4 Efficacy and safety assessments ... 12
3.5 Lab data acquisition and analysis ... 12
3.6 Statistical Analyses ... 13
Chapter 4: Results ... 15
4.1 Patient disposition and baseline characteristics ... 15
4.2 Efficacy ... 15
4.2.1 A1C, FPG and HOMA-IR ... 15
4.2.2 Hs-CRP and lipids ... 16
4.3 Safety and tolerability ... 17
4.4 Subgroup analyses ... 18
Chapter 5: Discussion ... 19
5.1 A1C, FPG and HOMA-IR ... 19
5.2 Hs-CRP and lipids ... 20
5.3 Safety, tolerability and body weight change ... 20
5.4 Subgroup analyses ... 21
5.5 Limitation ... 22
5.6 Conclusion ... 23
Chapter 6: References ... 24
List of Figures ... 30
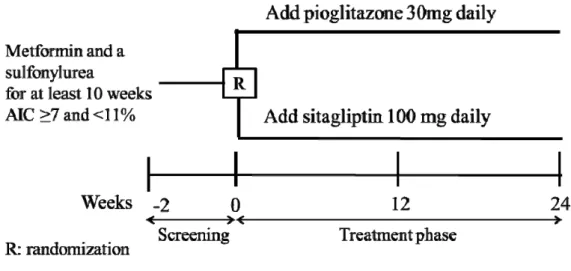
Figure 1 Study Design ... 30
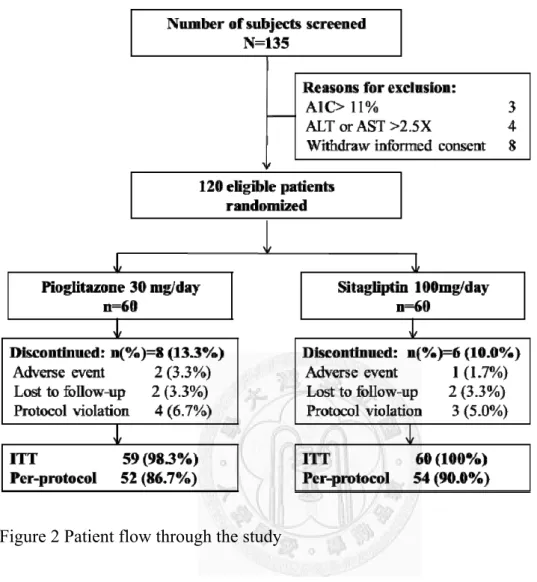
Figure 2 Patient flow through the study ... 31
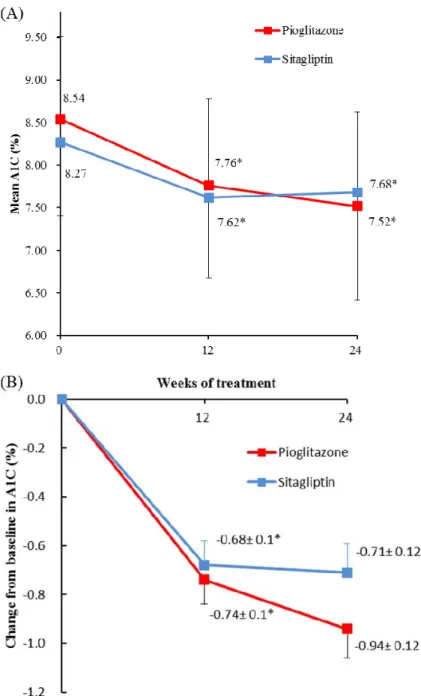
Figure 3 Change in glycosylated hemoglobin (A1C) over 24 weeks ... 32
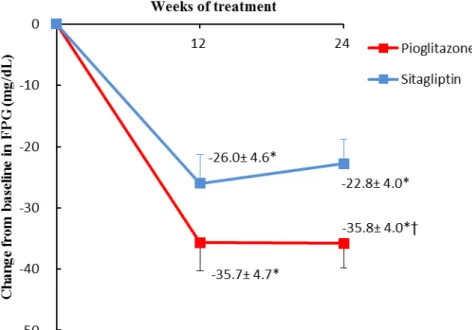
Figure 4 Least squares (LS) mean change from baseline in fasting plasma glucose .. 33
Figure 5 Percentages of patient achieving A1C <7% ... 34
Figure 6 Change in A1C on the subgroups according to baseline characteristics ... 35
Table 1 Literature review: Effect of antidiabetic agents added to metformin ... 36
Table 2 Baseline demographic and clinical characteristics ... 38
Table 3 Least squares (LS) mean change from baseline ... 39
Table 4 Summary of clinical AEs ... 40
Appendix 1: IRB approval ... 41
Appendix 2: ClinicalTrials.gov registration receipt ... 43
Appendix 3: Informed consent ... 44
Chapter 1: Introduction
Effective glycemic control plays an important role in preventing chronic complications of diabetes mellitus1,2. Although diet and exercise can improve
glycemic control early in the course of type 2 diabetes, success rates of such methods in the long-term are generally poor, thus oral antidiabetic drugs (OADs) often become the mainstay of treatment3,4. Metformin and sulfonylurea (SU) is recommended as the first 2 steps of pharmacological therapy in the current treatment algorithm5,6 .Type 2 diabetes is a progressive illness which most patients experience a progressive
deterioration in glycemic control, dual combination therapy with metformin and a SU also may not achieve or maintain glycemic control7,8. In this setting, adding basal insulin to ongoing OADs is often the next step therapy5,6. However, insulin therapy which requires percutaneous administration and additional injection education was undesirable for patients and clinical practice. So adding a third OAD to ongoing dual therapy is still often being used in clinical practice.
Previous studies had demonstrated that adding pioglitazone, a thiazolidinedione oral antidiabetic agent, to ongoing OAD monotherapy or dual therapy with metformin and a SU improves glycemic control9-12. Sitagliptin, potent and highly selective
dipeptidyl peptidase-4 (DPP-4) inhibitor, has been shown to improve glycemic control as add-on therapy to OAD monotherapy or dual therapy13-17.
Pioglitazone and sitagliptin are often using as third-line OADs in clinical practice.
However, lack head to head study to compare the efficacy and side effect between the two agents. This study was conducted to directly compare the glycemic efficacy and safety of pioglitazone with sitagliptin, as add-on therapy, in patients with type 2 diabetes inadequately controlled by dual therapy with metformin and a SU.
Chapter 2: Literature review
2.1 Pioglitazone
Pioglitazone (Actos@) was approved by the FDA in July 1999 for the treatment of type 2 diabetes.
2.1.1 Mechanism:
Pioglitazone is an insulin sensitizing thiazolidinedione that activates peroxisome-proliferator activated receptor-γ (PPAR-γ) found in adipose tissue, pancreatic, β -cells, vascular endothelium and macrophages18. Pioglitazone is a high-affinity ligand for PPAR-γ. Once activated by a ligand, PPAR-γ forms a heterodimer with another nuclear receptor, the retinoid-X receptor. This heterodimer then binds to specific DNA sequences and regulates the transcriptional activity of target genes that play a role in the metabolism of glucose and lipids18.
2.1.2 Efficacy
Previous trial had demonstrated that adding a thiazolidinedione (TZD) to ongoing OAD monotherapy or dual therapy with metformin and a SU improves glycemic control9-12. The magnitude of glycosylated hemoglobin (A1C) reduction was -1.2 to -1.9% as a third-line OADs9-11. Beyond these effects on glucose metabolism, pioglitazone has positive effects on lipid metabolism, blood pressure, endothelial function, adiponectin and high sensitivity CRP levels19.
2.1.3 Safety and tolerability
The main adverse effects reported with pioglitazone are weight gain, peripheral edema, bone loss and precipitation of congestive heart failure in at-risk individuals, without any increase in CVD/all-cause mortality20. Body weight increased from 1.4 to 4.1 kg and the incident of edema was 29 to 30% when pioglitazone was added on to metformin and a SU9,10,21,22.
2.2 Sitagliptin
Sitagliptin (Januvia@) was approved by the FDA in October 2006 for the treatment of type 2 diabetes, and it was the first DPP-4 inhibitor approved by the FDA.
2.2.1 Mechanism:
Antidiabetic agents targeting the incretin hormones have been developed in recent years. The incretin hormones that attribute to this effect are glucagon-like peptide-1 (GLP-1) and glucose-dependent insulinotropic peptide (GIP). GLP-1 and GIP stimulate insulin output from pancreatic β-cells in a glucose-dependent manner, with GLP-1 also suppressing pancreatic α-cell secretion of glucagon. However, endogenous GLP-1 and GIP are rapidly degraded by the enzyme DPP-4, resulting in half-lives in the range of minutes for these hormones.DPP-4 inhibitors are a class of agents that inhibit the inactivation of incretin hormones by inhibiting the ubiquitously
expressed DPP-4 enzyme, thereby enhancing and prolonging the activity of GLP-1 and GIP and attenuating glucose excursions23.
2.2.2 Efficacy
Previous trials have demonstrated the advantages on glycemic control of sitagliptin monotherapy, in combination with SU, or in combination with metformin in type 2 diabetes poorly controlled on OADs13-17,23. In a subgroup analysis from prior study of adding sitagliptin or placebo to ongoing dual therapy with metformin and a SU, treatment with sitagliptin significantly decreased A1C by 0.59% from baseline17. 2.2.3 Safety and tolerability
Early meta-analysis of DPP4 inhibitors suggest that there was an increased risk of some infections (nasopharyngitis and urinary tract infections) and headache24. However, updated safety analyses of the DPP4 inhibitors clinical studies have been published, showing no increased risk for respiratory or urinary tract infections or headache with the DPP-4 inhibitors compared to placebo or comparator25,26. DPP-4 inhibitors as a class appear to be well tolerated, and rates of adverse effects have been low, and generally not different to placebo or comparator. Retrospective analyses of data do not appear to indicate any increased cardiovascular risk with the DPP-4 inhibitors relative to comparators and large prospective trials, designed specifically to evaluate the effect of DPP-4 inhibitors on cardiovascular outcomes are underway25,26.
2.3
Research gapOur previous review showed that there was no significant difference in A1C reduction and incident of hypoglycemia between pioglitazone and sitagliptin as secondary-line OADs (Table 1)12. Pioglitazone and sitagliptin are often using as third-line OADs in clinical practice. However, lack head to head study to compare the efficacy and side effect between the two agents.
Chapter 3: Materials and Methods
3.1 Patients
3.1.1 Inclusion criteria
Men and women with type 2 diabetes (> 20 years of age) who were taking stable doses of metformin (≥1500mg/d) and a SU (≥half maximal dose; modified release gliclazide 60-120 mg daily or glimepiride 4-8 mg daily ) for at least 10 weeks prior to the screening visit and had inadequate glycemic control (AIC≥7 and <11%) were recruited for the study.
3.1.2 Exclusion criteria
Patients were excluded if they had type 1 diabetes, insulin use within 12 weeks of the screening visit, any contraindications for use of pioglitazone or sitagliptin, impaired renal function (serum creatinine >1.4 mg/dl), alanine aminotransferase (ALT) or aspartate aminotransferase levels (AST)>2.5 times the upper limit of normal (ULN), current or prepare to pregnancy and lactation.
3.2 Study Design
This prospective, randomized, open-label, parallel-group study was performed at the Mackay Memorial Hospital, Taipei, Taiwan between September 2009 and September 2011. Eligible patients were randomized in a 1: 1 ratio to one of the following once-daily treatment groups: pioglitazone 30 mg or sitagliptin 100 mg for
24 weeks (Figure 1). The randomization was performed using an interactive voice-response system that used a permuted-block size of 6. In addition, patients were stratified by A1C (7.0% to 8.5% and >8.5%). During the entire study period, no dose adjustments were made on metformin, SU and lipid-lowering agents. At any time during the study, study medication (pioglitazone or sitagliptin) could be down titrated if hypoglycemia occurs. Throughout the course of the study, patients were instructed to continue the same lifestyle (including diet and exercise) they had maintained prior to study entry. Patients were allowed to continue using antihypertensive and lipid-lowering agents if they had been taking a stable dose for at least 10 weeks before entry into the study, and the same doses maintained during the entire study. It was be conducted in accordance with the Declaration of Helsinki and approved by ethics boards of Mackay Memorial Hospital. All subjects must provide informed consent before enter the trial. This trial is registered with ClinicalTrials.gov, with the number NCT01195090.
3.3 Withdrawal Criteria
Withdrawal criteria included pregnancy, A1C >11.0% after the first 12 weeks of treatment, ALT or AST >3x ULN, serum creatinine female >1.4 mg/dl and male >
1.5mg/dl, any adverse effect unacceptable to the patient, or serious adverse effects, including severe hypoglycemia, heart failure and hepatic failure.
3.4 Efficacy and safety assessments
A1C, fasting plasma glucose (FPG), fasting serum insulin, high sensitive C-reactive protein (hs-CRP), ALT, AST and fasting plasma lipid parameters (total cholesterol (TC), low-density lipoprotein cholesterol (LDL-C), triglycerides (TG) and high-density lipoprotein cholesterol (HDL-C)) were measured at baseline and after 12 and 24 weeks of treatment. Fasting serum C-peptide was measured at baseline. Insulin resistance was assessed by the homeostasis model assessment (HOMA-IR), calculated as (fasting insulin [μU⁄ ml]) x (fasting plasma glucose [mmol⁄ l]) ⁄ 22.527.
Safety and adverse events were assessed and monitored throughout the study.
Physical examinations, vital signs, and safety laboratory measurements, were performed. Safety endpoints of interest included hypoglycemia, edema, gastrointestinal related adverse events, nasopharyngitis, influenza, any serious adverse event and change from baseline in body weight.
3.5 Lab data acquisition and analysis
A1C was analysed using cation ion exchange HPLC method (BIO-RAD VARIANT Ⅱ ). A Beckman automatic analyzer was used to measure FPG (hexokinase method), TC (enzymatic method), TG (enzymatic GPO trinder method), LDL-C (homogeneous method), HDL-C (homogeneous method), ALT (2-amino-2methyl-1-propanl method), AST (Henry method) and creatinine
(colorimetric assay). Hs-CRP was determined using chemiluminescent immunometric assay (Immultitle 2000, Siemens). Insulin was analysed by the coated tube separation radioimmunoassay and C-peptide by solid-phase two site immunoradiometric assay.
3.6 Statistical Analyses
An intent-to-treat (ITT) analysis with last observation carried forward was used to assess efficacy. The ITT population included all patients who had received at least one dose of study medication and had A1C recorded at baseline and at least once after baseline. Treatment groups were compared at baseline using the Student t test for continuous variables and the Chi-square test for categorical variables. The change from baseline in continuous parameters were determined using an analysis of co-variance (ANCOVA) model with the factor ‘treatment’ and baseline value as covariate. The chi-square test or Fisher’s exact test were used for dichotomous parameters. A repeated measure, mixed model analysis was used to compare the primary outcomes of change in A1C between groups and over time. All patients who had taken at least one dose of study medication were included in the safety analysis.
Subgroup analyses for the primary efficacy endpoint (A1C) were performed by including an interaction term in the ANCOVA model to explore whether treatment effects were consistent within subgroups. For subgroup analyses, baseline variables were treated as binary variables, dichotomized at the median value. Results were
presented as mean (±SD or ±standard error) or 95% CI for continuous parameters, and numbers or percentages for dichotomous parameters.
One hundred twenty patients were planned for randomization to 1 of 2 groups with 60 patients each, accounting for a 10% early discontinuation rate. Therefore, 120 patients would provide 80% power to detect a treatment difference of 0.5% for A1C using a 2-sided test with a 0.05 significance level. An estimated 0.9% SD of intra-subject difference was expected. The treatment difference and standard deviation was based on the previous trials9-11, 17. All analyses were done using SAS version 9.2.
Chapter 4: Results
4.1 Patient disposition and baseline characteristics
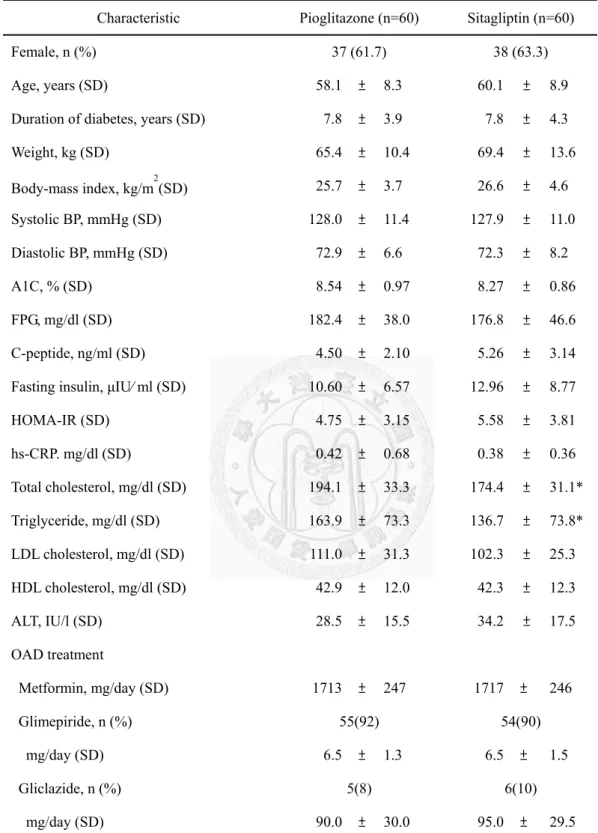
Figure 2 summarizes patients flow through the study. A total of 120 patients were randomized and similarly number of patients in each treatment group completed the 24-week treatment. The reasons for premature withdrawal included being lost to follow-up (2 in pioglitazone group and 2 in sitagliptin group), protocol violation (4 in pioglitazone group and 3 in sitagliptin group), peripheral edema (1 in pioglitazone group), ALT >3 times ULN (1 in pioglitazone group) and gastrointestinal events (1 in sitagliptin group). There were no statistically significant differences between the treatment groups in respect to baseline demographics, clinical characteristics, and laboratory measurements with the exception of total cholesterol and triglycerides levels, which were higher in patients randomly assigned to pioglitazone (Table 2).
4.2 Efficacy
4.2.1 A1C, FPG and HOMA-IR
Both pioglitazone and sitagliptin significantly decreased A1C from baseline to endpoint (-0.94±0.12%, p< 0.001 and -0.71±0.12%, p <0.001; respectively), but no statistically significant difference between treatment groups was observed (Table 3 and Figure 3). No significant differences were observed between groups in reductions in A1C after adjusting for the dose of sulfonylurea (P=0.17) or analyzed using the
mixed model with repeated time measures (p=0.12). Mean changes in FPG were -35.7± 4.0mg/dl with pioglitazone and -22.8± 4.0mg/dl with sitagliptin, for a between groups difference of -12.9±5.7mg/dl (p=0.024). The difference in FPG between the two groups was still significant after adjusting for the dose of sulfonylurea (p=0.025).
Figure 3 and Figure 4 show changes during the course of the study for A1C and FPG levels. The maximum decrease in A1C was reached at 12 weeks in the sitagliptin group and 24 weeks in the pioglitazone group. The percentages of patient achieving an A1C <7% was similar in both groups (28.8% in the pioglitazone and 28.3% in sitagliptin) (Figure 5).
HOMA-IR significantly changed from baseline in the pioglitazone group (-1.56± 0.35, p < 0.001), and a non-significant changed in the sitagliptin group (-0.00± 0.35, p=0.993), resulting in a significant difference between groups (-1.56±0.50, p=0.002) (Table 3).
4.2.2 Hs-CRP and lipids
Hs-CRP significantly changed from baseline in the pioglitazone group (-0.19± 0.04 mg/dL, p < 0.001), and a non-significant changed in the sitagliptin group (-0.07±
0.04mg/dL, p=0.069), resulting in a significant difference between groups (-0.12±0.05, p=0.030). Treatment with pioglitazone significantly increased TC, HDL-C, and decreased TG, while sitagliptin did not induce changes in these parameters (Table 3).
At end point, there were significant differences between the groups for TG and HDL-C in favour of pioglitazone (-30.2± 13.3mg/dL, p=0.025 and 5.0± 1.6, p=0.003;
respectively). No significant change from baseline in the LDL-C was observed in either group, resulting in no significant difference between groups (Table 3). No differences between groups were observed with regard to systolic blood pressure and diastolic blood pressure.
4.3 Safety and tolerability
Overall adverse events were similar between treatment groups (Table 4). Among the reported adverse events, peripheral edema was more common in the pioglitazone group than sitagliptin group (27.1% vs. 0.0%, respectively), whereas gastrointestinal adverse was more common in the sitagliptin group than pioglitazone group (20%
vs.6.8%, respectively). All the adverse events were mild to moderate. Hypoglycemic events occurred in 5 patients (8.5%) in the pioglitazone group and in 6 patients (10.0%) in the sitagliptin group. No hypoglycaemia episode required medical assistance or required assistance of another person. One patient discontinued therapy because of mild, but unacceptable to the patient, edema in the pioglitazone group and one patient discontinued therapy because of abdomen pain in the sitagliptin group.
ALT decreased non-significantly by 4.5± 2.4 IU/L (p=0.367) in the pioglitazone group, and remained unchanged in the sitagliptin group (Table 3). One patient withdrew due
to elevated ALT > 3times ULN. On follow-up, the level of ALT reduced to < 3times ULN.
Mean change in body weight from baseline was 1.34± 0.32kg (p<0.001) in the pioglitazone group and -0.26± 0.32kg (p=0.43) in the sitagliptin group (Table 3). The between group difference in the body weight was 1.60±0.46 kg (p < 0.001).
4.4 Subgroup analyses
In an exploratory intention-to-treat analysis that was not prespecified in the study protocol, we assessed the consistency of between-group differences regarding the change from baseline in A1C in subgroups (Figure 6). There was only significant interaction between patients with different gender (P = 0.006), although we found that female patients and patients with higher BMI or higher HOMA-IR at baseline appeared to have a greater reduction in A1C in pioglitazone group.
Chapter 5: Discussion
5.1 A1C, FPG and HOMA-IR
Metformin and SU are recommended as the first 2 steps of therapy in current treatment algorithms5,6. However, there is no widely agreed consensus on how to intensify therapy in patients with secondary oral agent failure. Our study demonstrated that intensifying an existing dual oral therapy by adding pioglitazone or sitagliptin resulted in a significant and similar improvement in A1C.
Our changes in A1C results of pioglitazone and sitagliptin were similar to previous meta-analysis evaluating antidiabetic drug additions to metformin12. The magnitude of A1C reduction of pioglitazone in our study was somewhat lower than previous reports combining metformin and a SU with pioglitazone9-11,21. This could be due to that we only used pioglitazone 30mg daily lower than previous studies (34.5mg to 45mg daily).
Our results demonstrated superior FPG reductions with pioglitazone verses sitagliptin, despite similar effect on A1C, were consistent with prior studies which pioglitazone or vildagliptin (another brand of DPP-4 inhibitors) were added to patients with metformin monotherapy28. This could be probably due to the different mechanisms of action of the two add-on drugs. Pioglitazone decreases fasting and postprandial plasma glucose by improving hepatic and peripheral insulin sensitivity, whereas
sitagliptin stimulate insulin secretion and inhibit glucagon secretion in a glucose-dependent manner which was considered to be mainly a postprandial treatment18,23,29. Future studies are needed to compare the 24-h glucose profiles with treatment with both drugs.
In agreement with the established effects of pioglitazone on insulin resistance, pioglitazone was associated with significant decrease in HOMA-IR18,19. In contrast, HOMA-IR was not significantly change with sitagliptin, consistent with the observation that DPP4 inhibitors target insulin secretion and do not alter insulin resistance15-17.
5.2 Hs-CRP and lipids
The favourable influence of pioglitazone on TG, HDL-C and hs-CRP is well established18,19. Our results extended the findings and showed that similar lipid and hs-CRP changes can be expected when pioglitazone is added to dual therapy with metformin and a SU. Consistent with previous studies, in which sitagliptin has generally demonstrated a neutral effect on lipid and hs-CRP15,16,23. Whether these differences in lipid and hs-CRP effects translate into differences for the risk of CVD is not clear.
5.3 Safety, tolerability and body weight change
Both combination therapies were general well tolerated, with no difference in the
incidence of overall adverse events. There was a significantly higher incidence of edema in the pioglitazone group compared with the sitagliptin group, consistent with previous results of an increased incidence of edema with pioglitazone9,22. Gastrointestinal adverse events was more common in the sitagliptin and was higher than reports of previous sitagliptin studies (20% vs. 4.3 -12%)13-17. However, most of the events were mild and resolved while patients continued to receive therapy.
Hypoglycemia is always a concern with the antidiabetic drugs. The incidence of hypoglycemia was similar in both groups and none of the episodes was considered to be severe by the investigators and most were associated with precipitating factors, such as delay eating, skipped meals or increased activity.
Another concern with antidiabetic drugs is weight gain. In this study, the mean weight gain was higher in the pioglitazone group compared with the sitagliptin group. Weight gain is a well-known consequence of pioglitazone treatment, while weight neutrality has been observed in sitagliptin studies both in monotherapy and add-on settings13-17,23.
5.4 Subgroup analyses
The treatment effects on A1C were consistent across most subgroups, with only significant interaction noted with regard to gender. Magnitudes of the A1C reduction with sitagliptin were generally consistent across the subgroups in previous clinical
studies (e.g. age, gender, duration of diabetes, BMI, and HOMA-IR)15,17. The efficacy of pioglitazone was different in gender has not been reported in clinical studies, but according to the FDA review, the decrease in AlC was greater in women than in men30. The reasons for sex difference are possibly due to the pharmacological mechanisms based on differences in body fat distribution and in sex hormones and due to the different pharmacokinetic mechanism31-33.
5.5 Limitation
There were some limitations to this study. First, the period of treatment was too short to evaluate long-term glycemic control and adverse event. Second, we may underestimate the efficacy of pioglitazone, as the maximum dose pioglitazone was not used. However, the cost of pioglitazone 30mg is similar to sitagliptin 100mg, so we don’t need to consider cost-effectiveness. Third, our study did not record or measure some potential adverse events including anemia, osteoporosis and urinary tract infection. Finally, Subgroup analyses indicated a slight favour for adding pioglitazone compared with sitagliptin in patients with higher BMI or higher HOMA-IR at baseline, however, our study was not designed with sufficient power to draw statistical conclusions about individual subgroups. Thus, one should be cautious in interpreting the results of subgroup analyses.
5.6 Conclusion
Pioglitazone and sitagliptin achieved similar improvements in overall glycemic control in patients with type 2 diabetes inadequately controlled with metformin and a sulfonylurea. However there were some differences in terms of FPG, lipids, HOMA-IR, body weight change and adverse events. Long term randomized control trials will be required to provide the reference when choosing OAD as combination therapy in patients with type 2 diabetes who had inadequate glycemic control on dual therapy with metformin and a SU.
Chapter 6: References
1. Group UPDSU. Intensive blood-glucose control with sulphonylureas or insulin compared with conventional treatment and risk of complications in patients with type 2 diabetes (UKPDS 33). The Lancet 1998;352:837-53.
2. Holman RR, Paul SK, Bethel MA, Matthews DR, Neil HAW. 10-Year Follow-up of Intensive Glucose Control in Type 2 Diabetes. New England Journal of Medicine 2008;359:1577-89.
3. Wing RR, Venditti E, Jakicic JM, Polley BA, Lang W. Lifestyle intervention in overweight individuals with a family history of diabetes. Diabetes Care
1998;21:350-9.
4. Tuomilehto J, Lindström J, Eriksson JG, et al. Prevention of Type 2 Diabetes Mellitus by Changes in Lifestyle among Subjects with Impaired Glucose Tolerance.
New England Journal of Medicine 2001;344:1343-50.
5. Nathan DM, Buse JB, Davidson MB, et al. Medical Management of
Hyperglycemia in Type 2 Diabetes: A Consensus Algorithm for the Initiation and Adjustment of Therapy. Diabetes Care 2009;32:193-203.
6. National Collaborating Centre for Chronic Conditions. Type 2 diabetes: National clinical guideline for management in primary and secondary care (update). London:
Royal College of Physicians 2008.
7. Turner RC, Cull CA, Frighi V, Holman RR, Group ftUPDS. Glycemic Control With Diet, Sulfonylurea, Metformin, or Insulin in Patients With Type 2 Diabetes Mellitus. JAMA 1999;281:2005-12.
8. Cook MN, Girman CJ, Stein PP, Alexander CM, Holman RR. Glycemic Control Continues to Deteriorate After Sulfonylureas Are Added to Metformin Among Patients With Type 2 Diabetes. Diabetes Care 2005;28:995-1000.
9. Aljabri K, Kozak S, Thompson D. Addition of pioglitazone or bedtime insulin to maximal doses of sulfonylurea and metformin in type 2 diabetes patients with poor glucose control: a prospective, randomized trial. Am J Med 2004;116:230-5.
10. Dorkhan M, Frid A, Groop L. Differences in effects of insulin glargine or
pioglitazone added to oral anti-diabetic therapy in patients with type 2 diabetes: What to add--Insulin glargine or pioglitazone? Diabetes Research and Clinical Practice 2008;82:340-5.
11. Hartemann-Heurtier A, Halbron M, Golmard J-L, et al. Effects of bed-time insulin versus pioglitazone on abdominal fat accumulation, inflammation and gene expression in adipose tissue in patients with type 2 diabetes. Diabetes Research and Clinical Practice 2009;86:37-43.
12. Liu SC, Tu YK, Chien MN, Chien KL. Effect of antidiabetic agents added to metformin on glycaemic control, hypoglycaemia and weight change in patients with
type 2 diabetes: a network meta-analysis. Diabetes, Obesity and Metabolism 2012: in press.
13. Charbonnel B, Karasik A, Liu J, Wu M, Meininger G. Efficacy and Safety of the Dipeptidyl Peptidase-4 Inhibitor Sitagliptin Added to Ongoing Metformin Therapy in Patients With Type 2 Diabetes Inadequately Controlled With Metformin Alone.
Diabetes Care 2006;29:2638-43.
14. Scott R, Loeys T, Davies MJ, Engel SS, for the Sitagliptin Study G. Efficacy and safety of sitagliptin when added to ongoing metformin therapy in patients with type 2 diabetes*. Diabetes, Obesity and Metabolism 2008;10:959-69.
15. Raz I, Chen Y, Wu M, et al. Efficacy and safety of sitagliptin added to ongoing metformin therapy in patients with type 2 diabetes. Curr Med Res Opin
2008;24:537-50.
16. Pratley RE, Nauck M, Bailey T, et al. Liraglutide versus sitagliptin for patients with type 2 diabetes who did not have adequate glycaemic control with metformin: a 26-week, randomised, parallel-group, open-label trial. The Lancet 2010;375:1447-56.
17. Hermansen K, Kipnes M, Luo E, et al. Efficacy and safety of the dipeptidyl peptidase-4 inhibitor, sitagliptin, in patients with type 2 diabetes mellitus inadequately controlled on glimepiride alone or on glimepiride and metformin. Diabetes, Obesity and Metabolism 2007;9:733-45.
18. Waugh J, Keating GM, Plosker GL, Easthope S, Robinson DM. Pioglitazone: A Review of its Use in Type 2 Diabetes Mellitus. Drugs 2006;66:85-109.
19. de Pablos-Velasco P. Pioglitazone: beyond glucose control. Expert Review of Cardiovascular Therapy 2010;8:1057-67.
20. Shah P, Mudaliar S. Pioglitazone: side effect and safety profile. Expert Opinion on Drug Safety 2010;9:347-54.
21. Derosa G, Mereu R, D’Angelo A, et al. Effect of pioglitazone and acarbose on endothelial inflammation biomarkers during oral glucose tolerance test in diabetic patients treated with sulphonylureas and metformin. J Clin Pharm Ther
2010;35:565-79.
22. Scheen AJ, Tan MH, Betteridge DJ, et al. Long-term glycaemic control with metformin–sulphonylurea–pioglitazone triple therapy in PROactive (PROactive 17).
Diabetic Medicine 2009;26:1033-9.
23. Dhillon S. Sitagliptin: a review of its use in the management of type 2 diabetes mellitus. Drugs 2010;70:489-512.
24. Amori RE, Lau J, Pittas AG. Efficacy and Safety of Incretin Therapy in Type 2 Diabetes. JAMA: The Journal of the American Medical Association
2007;298:194-206.
25. Deacon CF. Dipeptidyl peptidase-4 inhibitors in the treatment of type 2 diabetes:
a comparative review. Diabetes, Obesity and Metabolism 2011;13:7-18.
26. Gooβen K, Gräber S. Longer-term safety of DPP-4 inhibitors in patients with type 2 diabetes mellitus: systematic review and meta-analysis. Diabetes, Obesity and Metabolism 2012:in press.
27. Matthews D, Hosker J, Rudenski A, Naylor B, Treacher D, Turner R.
Homeostasis model assessment: insulin resistance and β-cell function from fasting plasma glucose and insulin concentrations in man. Diabetologia 1985;28:412-9.
28. Bolli G, Dotta F, Rochotte E, Cohen SE. Efficacy and tolerability of vildagliptin vs. pioglitazone when added to metformin: a 24-week, randomized, double-blind study*. Diabetes, Obesity and Metabolism 2008;10:82-90.
29. Natali A, Ferrannini E. Effects of metformin and thiazolidinediones on
suppression of hepatic glucose production and stimulation of glucose uptake in type 2 diabetes: a systematic review. Diabetologia 2006;49:434-41.
30. U.S. Food and Drug Administration. Drug Approvals and Databases. Label and Approval History;NDA021073:Available at:
http://www.accessdata.fda.gov/scripts/cder/drugsatfda/index.cfm?fuseaction=Search.
Label_ApprovalHistory#labelinfo.
31. Adams M, Montague CT, Prins JB, et al. Activators of peroxisome proliferator-activated receptor gamma have depot-specific effects on human
preadipocyte differentiation. J Clin Invest 1997;100:3149-53.
32. Kadowaki K, Fukino K, Negishi E, Ueno K. Sex differences in PPARgamma expressions in rat adipose tissues. Biol Pharm Bull 2007;30:818-20.
33. Fujita Y, Yamada Y, Kusama M, et al. Sex differences in the pharmacokinetics of pioglitazone in rats. Comparative Biochemistry and Physiology Part C: Toxicology
& Pharmacology 2003;136:85-94.
List of Figures
Figure 1 Study Design
Figure 2 Patient flow through the study
Figure 3 Change in glycosylated hemoglobin (A1C) over 24 weeks (A) Mean A1C by weeks during the study. Data are mean ± SD;
(B) Least squares (LS) mean change from baseline (last-observation-carried-forward analysis) in A1C by weeks during the study. Data are mean ± se;
*P < 0.001 versus baseline.
Figure 4 Least squares (LS) mean change from baseline in fasting plasma glucose (FPG) by weeks during the study. Data are mean ± se;
*P < 0.001 versus baseline † <0.05 between group
Figure 5 Percentages of patient achieving A1C <7%
Figure 6 Change in A1C on the subgroups according to baseline characteristics A1C=glycosylated hemoglobin; FPG= Fasting plasma glucose; LDL-C= LDL cholesterol; HDL-C=HDL cholesterol; hs-CRP=high sensitive C-reactive protein;HOMA-IR= homoeostasis model assessment of insulin resistance
List of Tables
Table 1 Literature review: Effect of antidiabetic agents added to metformin on glycemic control, hypoglycemia and weight change in patients with type 2 diabetes- a network meta-analysis
12Mean change from baseline in A1C level (95% CI), %
Placebo-0.82 (-0.95, -0.70) Sulfonylureas
-0.71 (-1.01, -0.43) 0.11 (-0.17,0.38) Glinides
-0.82 (-0.98, -0.66) -0.00 (-0.16,0.16) -0.11 (-0.42,0.21) Pioglitazone
-0.66 (-0.90, -0.42) 0.16 (-011, 0.43) 0.05 (-0.31,0.44) 0.16 (-0.12, 0.45) AGI
-0.69 (-0.79, -0.61) 0.12 (0.03, 0.23) 0.01 (-0.26,0.31) 0.12 (-0.03,0.28) -0.03 (-0.29,0.22) DPP4-inhibitors
-1.02 (-1.17, -0.86) -0.20 (-0.34,-0.04) -0.31 (-0.61,-0.02) -0.20 (-0.38,-0.00) -0.36 (-0.64,-0.07) -0.32 (-0.47,-0.17) GLP−1
-0.88 (-1.21, -0.56) -0.07 (-0.38, 0.26) -0.17 (-0.58, 0.25) -0.06 (-0.40,0.28) -0.22 (-0.63,0.18) -0.19 (-0.51,0.13) 0.13 (-0.16,0.42) Basal insulin
-1.07 (-1.46, -0.69) -0.26 (-0.63,0.12) -0.36 (-0.82, -0.11) -0.25 (-0.65, 0.15) -0.41 (-0.87,0.04) -0.38 (-0.76,0.00) -0.06 (-0.44,0.33) -0.19 (-0.56,0.18) Biphasic insulin
At least one event of overall hypoglycemia (95% CI), odds ratio
Placebo
8.86 (4.63,17.83) Sulfonylureas
10.51 (3.59,38.32) 1.19 (0.43,3.85) Glinides
0.45 (0.15,1.34) 0.05 (0.02,0.13) 0.04 (0.01,0.17) Pioglitazone
0.40 (0.01,6.57) 0.04 (0.00,0.79) 0.04 (0.00,0.77) 0.87 (0.01,18.08) AGIs
1.13 (0.62,2.17) 0.13 (0.08,0.21) 0.11 (0.03,0.32) 2.50 (0.93,7.43) 2.85 (0.17,163.1) DPP4-inhibitors
0.92 (0.42,2.07) 0.10 (0.05,0.21) 0.09 (0.02,0.29) 2.03 (0.66,6.51) 2.32 (0.13,132.7) 0.81 (0.38,1.63) GLP−1
4.77 (1.35,18.3) 0.54 (0.17,1.85) 0.45 (0.09,2.17) 10.57 (2.41,51.26) 12.33 (0.55,774.0) 4.22 (1.24,14.87) 5.20 (1.77,16.45) Basal insulin
17.78 (4.84,69.98) 2.00 (0.62,6.68) 1.67 (0.32,8.06) 39.38 (8.84,189.6) 45.74 (2.01,2889) 15.67 (4.45,55.92) 19.36 (5.73,68.648) 3.72 (1.16,11.80) Biphasic insulin
Mean change from baseline in body weight (95% CI), kg
Placebo
2.17 (1.70,2.65) Sulfonylureas
1.40 (0.59, 2.26) -0.77 (-1.65,0.15) Glinides
2.46 (1.88,3.06) 0.29 (-0.31,0.90) 1.07 (0.05,2.03) Pioglitazone
-1.01 (-1.88,-0.13) -3.18 (-4.17,-2.17) -2.41 (-3.63,-1.22) -3.47 (-4.52,-2.41) AGIs
0.23 (-0.13,0.60) -1.93 (-2.35,-1.53) -1.16 (-2.07,-0.30) -2.23 (-2.81,-1.66) 1.24 (0.29,2.19) DPP4-inhibitors
-1.66 (-2.26,-1.09) -3.81 (-4.44,-3.24) -3.06 (-4.08,-2.11) -4.12 (-4.84,-3.44) -0.65 (-1.72,0.39) -1.89 (-2.46,-1.35) GLP−1
1.38 (0.18,2.60) -0.79 (-1.95,0.38) 0.02 (-1.47,1.40) -1.08 (-2.34,0.19) 2.39 (0.91,3.88) 1.15 (-0.03,2.34) 3.04 (1.97,4.15) Basal insulin
3.41 (2.04,4.77) 1.24 (-0.08,2.54) 2.01 (0.41,3.56) 0.94 (-0.48,2.35) 4.41 (2.79,6.05) 3.17 (1.82,4.52) 5.06 (3.74,6.41) 2.02 (0.69,3.35) Biphasic insulin
A1C: glycosylated hemoglobin, CI: confidence interval, AGIs: α-glucosidase inhibitors, DPP4-inhibitors: dipeptidyl peptidase-IV inhibitors,
GLP-1: glucagon-like peptide-1 analogues
Table 2 Baseline demographic and clinical characteristics
Characteristic Pioglitazone (n=60) Sitagliptin (n=60)
Female, n (%) 37 (61.7) 38 (63.3)
Age, years (SD) 58.1 ± 8.3 60.1 ± 8.9
Duration of diabetes, years (SD) 7.8 ± 3.9 7.8 ± 4.3
Weight, kg (SD) 65.4 ± 10.4 69.4 ± 13.6
Body-mass index, kg/m
2(SD) 25.7 ± 3.7 26.6 ± 4.6
Systolic BP, mmHg (SD) 128.0 ± 11.4 127.9 ± 11.0
Diastolic BP, mmHg (SD) 72.9 ± 6.6 72.3 ± 8.2
A1C, % (SD) 8.54 ± 0.97 8.27 ± 0.86
FPG, mg/dl (SD) 182.4 ± 38.0 176.8 ± 46.6
C-peptide, ng/ml (SD) 4.50 ± 2.10 5.26 ± 3.14
Fasting insulin, μIU⁄ ml (SD) 10.60 ± 6.57 12.96 ± 8.77
HOMA-IR (SD) 4.75 ± 3.15 5.58 ± 3.81
hs-CRP. mg/dl (SD) 0.42 ± 0.68 0.38 ± 0.36
Total cholesterol, mg/dl (SD) 194.1 ± 33.3 174.4 ± 31.1*
Triglyceride, mg/dl (SD) 163.9 ± 73.3 136.7 ± 73.8*
LDL cholesterol, mg/dl (SD) 111.0 ± 31.3 102.3 ± 25.3
HDL cholesterol, mg/dl (SD) 42.9 ± 12.0 42.3 ± 12.3
ALT, IU/l (SD) 28.5 ± 15.5 34.2 ± 17.5
OAD treatment
Metformin, mg/day (SD) 1713 ± 247 1717 ± 246
Glimepiride, n (%) 55(92) 54(90)
mg/day (SD) 6.5 ± 1.3 6.5 ± 1.5
Gliclazide, n (%) 5(8) 6(10)
mg/day (SD) 90.0 ± 30.0 95.0 ± 29.5
BP=blood pressure; A1C=glycosylated hemoglobin; FPG= Fasting plasma glucose;
HOMA-IR= homoeostasis model assessment of insulin resistance; hs-CRP=high sensitive C-reactive protein; ALT= Alanine-aminotransferase; OAD= oral antidiabetic drugs; * p<0.05
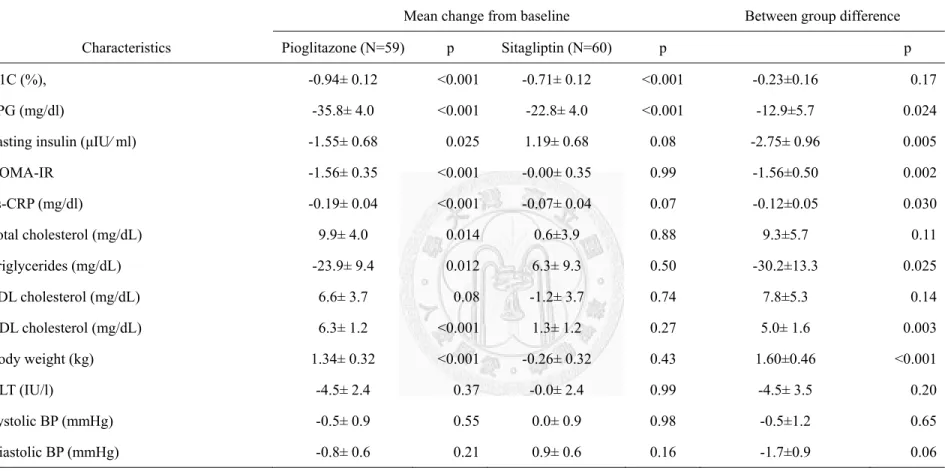
Table 3 Least squares (LS) mean change from baseline in primary and secondary outcomes for the intent-to-treat population
Mean change from baseline Between group difference
Characteristics Pioglitazone (N=59) p Sitagliptin (N=60) p p
A1C (%), -0.94± 0.12 <0.001 -0.71± 0.12 <0.001 -0.23±0.16 0.17
FPG (mg/dl) -35.8± 4.0 <0.001 -22.8± 4.0 <0.001 -12.9±5.7 0.024
Fasting insulin (μIU⁄ ml) -1.55± 0.68 0.025 1.19± 0.68 0.08 -2.75± 0.96 0.005
HOMA-IR -1.56± 0.35 <0.001 -0.00± 0.35 0.99 -1.56±0.50 0.002
hs-CRP (mg/dl) -0.19± 0.04 <0.001 -0.07± 0.04 0.07 -0.12±0.05 0.030
Total cholesterol (mg/dL) 9.9± 4.0 0.014 0.6±3.9 0.88 9.3±5.7 0.11
Triglycerides (mg/dL) -23.9± 9.4 0.012 6.3± 9.3 0.50 -30.2±13.3 0.025
LDL cholesterol (mg/dL) 6.6± 3.7 0.08 -1.2± 3.7 0.74 7.8±5.3 0.14
HDL cholesterol (mg/dL) 6.3± 1.2 <0.001 1.3± 1.2 0.27 5.0± 1.6 0.003
Body weight (kg) 1.34± 0.32 <0.001 -0.26± 0.32 0.43 1.60±0.46 <0.001
ALT (IU/l) -4.5± 2.4 0.37 -0.0± 2.4 0.99 -4.5± 3.5 0.20
Systolic BP (mmHg) -0.5± 0.9 0.55 0.0± 0.9 0.98 -0.5±1.2 0.65
Diastolic BP (mmHg) -0.8± 0.6 0.21 0.9± 0.6 0.16 -1.7±0.9 0.06
Data are means ± se
BP=blood pressure; A1C=glycosylated hemoglobin; FPG= Fasting plasma glucose; HOMA-IR= homoeostasis model assessment of insulin
resistance; hs-CRP=high sensitive C-reactive protein; ALT= Alanine-aminotransferase
Table 4 Summary of clinical AEs
Pioglitazone Sitagliptin
N (%) N (%) P value
Any AE
31 (51.7) 26 (43.3) 0.36SAE
0 (0.0) 0 (0.0)Edema
16 (27.1) 0 (0.0) <0.001Nasopharyngitis or Influenza
11 (18.6) 12 (20.0) 0.85
Gastrointestinal AEs
4 (6.8) 12 (20.0) 0.035Diarrhea 0 (0.0) 4 (6.7)
Nausea or Vomiting 2 (3.3) 6 (10.0)
Constipation 1 (1.7) 1 (1.7)
Abdomen pain 3 (5.0) 4 (6.7)
Hypoglycemia
Mild to moderate 5 (8.5) 6 (10.0) 0.77
Severe 0 (0.0) 0 (0.0)
Appendix 1: IRB approval
Appendix 2: ClinicalTrials.gov registration receipt
Appendix 3: Informed consent
96.5.30.衛署藥字第 0960318326 號函公告 本院修正 96.07.
受試者同意書
計畫名稱:
比較第 2 型糖尿病患者以 metformin 及 sulfonylurea 治療仍控制不良 時加上佳糖維(Januvia
®)或愛妥糖(Actos
®)之療效。
執行單位:馬偕紀念醫院內分泌暨新陳代謝科
主要主持人:劉松臻 職稱:主治醫師 電話:0968957754 協同主持人:王朝弘 職稱:主治醫師 電話:25433535-2174 協同主持人:梁清香 職稱:主治醫師 電話:25433535-2173 協同主持人:陳偉哲 職稱:主治醫師 電話:25433535-2173 二十四小時緊急聯絡人電話:
劉松臻醫師 電話:0968957754 受試者姓名:
性別: 出生日期:
年月
日
病歷號碼:
國民身分證統一編號:
通訊地址:
聯絡電話:
法定代理人/有同意權人姓名:
與受試者關係:
性別: 出生日期:
年月
日
國民身分證統一編號:
通訊地址:
聯絡電話:
1.藥品全球上市現況簡介:
佳糖維為美國默沙東藥廠生產之原廠藥物,愛妥糖為日本武田公司 生產之原廠藥物。佳糖維及愛妥糖皆為已上市之合法降血糖藥物。
以前的研究證實若以 metformin 及 sulfonylurea 治療後血糖仍控制不 良時,再加上佳糖維或愛妥糖治療都可以有效的下降血糖。但沒有 研究比較當已使用 metformin 及 sulfonylurea 治療但仍控制不良 時,何種藥物是最適當的選擇。
2.試驗目的:
比較使用 metformin 及 sulfonylurea 治療後,但血糖仍控制不良時加 上佳糖維或愛妥糖之療效。
3.試驗之主要納入與排除條件:
1.第 2 型糖尿病患者以最大劑量一半或一半以上的 metformin 及 sulfonylurea 治療超過 10 週以上,但血糖仍控制不良。
2. 糖化血紅素大於等於 7.0 %但小於 11%。
3. 年齡大於等於 20 歲。
4.試驗方法及相關檢驗:
符合條件者隨機分配為:
1. 愛妥糖組:加上每日一次每次一錠愛妥糖(30 毫克) 2. 佳糖維組:加上每日一次每次一錠佳糖維(100 毫克)
在治療前、治療後第 12 週及第 24 週測量空腹血糖、糖化血色素、
胰島素濃度、C-peptide、總膽固醇、中性脂肪酸、低密度膽固醇、
高密度膽固醇、肌酸酐及肝功能等相關檢驗,以比較及評估治療效 果。每次回診測量體重與進行身體評估。
5.可能產生之不良反應、發生率及處理方法:
使用佳糖維治療時常見的副作用為腹痛(2.3%)、腹瀉(3.0%)與其他 藥物一起使用時可能會造成低血糖(1.2%)。
預防方法為:.每次回診皆進行詳細的身體評估,2.若發生低血糖,
請儘速吃含糖食物,若有嚴重低血糖請儘速送醫院治療。
使用愛妥糖治療時常見的副作用為水腫(6%)、體重增加(2kg)、肝功 能升高(0.34%),與其他藥物一起使用時可能會造成低血糖(1.3%)。
預防方法為:1.每次抽血皆會檢查肝功能,2.每次回診皆進行詳細
的身體評估,3.若發生低血糖,請儘速吃含糖食物,若有嚴重低血
糖請儘速送醫院治療。
6.其他替代療法及說明:
加上其他種類口服降血糖藥物或注射胰島素皆可作為替代的治療方 法,醫師會依據病情選擇最適合的治療方式來控制您的血糖。
7.試驗預期效益:
加上佳糖維或愛妥糖治療皆可以讓血糖的控制得到改善,本研究的 結果可以提供以後糖尿病患者選擇藥物時的參考。
8.試驗進行中受試者之禁忌、限制與應配合之事項:
1. 懷孕或哺乳之婦女不可參加此臨床計劃,若在臨床計劃期間可能 或已經懷孕,請立即通知臨床計劃醫師。
2. 對佳糖維或愛妥糖成分過敏的患者禁用。
9.機密性:
本研究為單純學術性研究,研究結果可能會發表於學術性雜誌,但參與者姓名 及所有個人資料將不會公布,參與者之隱私將會受到妥善保密。
10.損害賠償與保險:
• 如依本研究所訂臨床試驗計劃實施試驗,因而發生不良反應造成損害,
將由馬偕紀念醫院依法負損害賠償責任及所有醫療費用。但本受試者同 意書上已記載之不良反應,將不予賠償或為其他任何補償。
• 本研究使用之藥物皆為已上市之合法降血糖藥物,如依本研究所訂臨床 試驗計劃實施試驗,因而發生不良反應所造成之損害,本醫院會依法協 助與提供專業醫療照顧及醫療諮詢。
• 本研究未投保責任保險,除法定賠償及醫療照顧外,本研究不提供其他 形式之賠償或補償。若您不願意接受這樣的風險,請勿參加試驗。
• 您不會因為簽署本同意書,而喪失在法律上其他的權利。
11.受試者權利:
A. 試驗過程中,與你(妳)的健康或是疾病有關,可能影響你(妳)繼續接受臨 床試驗意願的任何重大發現,都將即時提供給你(妳)。
B. 如果你(妳)在試驗過程中對試驗工作性質產生疑問,對身為患者之權利有 意見或懷疑因參與研究而受害時,可與本院之人體試驗委員會聯絡請求 諮詢,其電話號碼為:02-25433535-3486、3487。
C. 為進行試驗工作,你(妳)必須接受馬偕紀念醫院新陳代謝科醫師的照顧。
如果你(妳)現在或於試驗期間有任何問題或狀況,可與在馬偕紀念醫院新 陳代謝科的劉松臻醫師、王朝弘醫師、梁清香醫師或陳偉哲醫師聯絡。
D. 醫師已將同意書副本交給你(妳),並已完整說明本研究之性質與目的。
醫師已回答您有關藥品與研究的問題。
12.試驗之退出與中止:
您可自由決定是否參加本試驗;試驗過程中也可隨時撤銷同意,退出試驗,
不需任何理由,且不會引起任何不愉快或影響其日後醫師對您的醫療照顧。
試驗主持人或贊助廠商亦可能於必要時中止該試驗之進行。
13.簽章
A. 主要主持人、協同主持人已詳細解釋有關本研究計畫中上述研究方法的 性質與目的,及可能產生的危險與利益。
主要主持人/協同主持人:
日期:
年
月
日
B. 受試者已詳細瞭解上述研究方法及其所可能產生的危險與利益,有關本 試驗計畫的疑問,業經計畫主持人詳細予以解釋。本人同意接受為臨床 試驗計畫的自願受試者。
受試者簽章:
國民身份證統一編號:
法定代理人簽章:
日期:
年
月
日
C. 如您不是受試者或其法定代理人,但因事實需要,受試者或其法定代理 人(暫時)無法簽署本同意書而需由您代簽。請用正楷書寫您的姓名,
並指出您與受試者的關係:
1. 姓名:
關係:
國民身份證統一編號:
聯絡電話:
通訊地址:
簽章: 日期:
年
月
日 2. 見證人(非本人或法定代理人簽章,則須另具見証人一名):
姓名:
國民身份證統一編號:
聯絡電話:
通訊地址:
簽章: 日期: