國立臺灣大學公共衛生學院健康政策與管理研究所 碩士論文
Institute of Health Policy and Management College of Public Health
National Taiwan University Master Thesis
從體感遊戲到正經遊戲- 運用遊戲改善社區老人的健康
From somatosensory games to serious games:
Using games to improve health of the elderly in a community
陳奕翰 I-Han Chen
指導教授:陳端容博士 共同指導教授:陳雅美博士
Advisor: Duan-Rung Chen, Ph.D Co-Advisor: Ya-Mei Chen, Ph.D 中華民國 107 年 6 月
June, 2018
doi:10.6342/NTU201801947
i
Acknowledgements
First of all, I would like to thank my advisor, Director Duan-Rung Chen, for her continuous support of my thesis research. Her insight helped me steer through the writing process smoothly. This thesis would not have been possible without her guidance.
Also, I want to express gratitude to the rest of my thesis committee, Associate Prof.
Ya-Mei Chen and Prof. Kevin C. Tseng, whose participation and comments prompted me to widen my perspectives in my thinking and make my thesis better.
Last but not the least; I must thank my family (my mother: Hui Ying Chen Chan; my sisters: Yih-Yuh Chen, I-Chun Chen, Yi-Shiu Chen; my wife: Man-Ting Chien and my new born baby girl: Ting-Xi Chen) for supporting me spiritually throughout writing this thesis and my life in general. My family is the best thing happened to me in life and I am grateful for it.
doi:10.6342/NTU201801947
iii
Chinese Abstract
聯合國的報告顯示超過 60 歲的族群,人口成長率是最高的,而老年人因為缺乏 肌力,通常運動量會比較少.這個研究想要調查體感遊戲 是否可以增進社區老 人的健康 (體適能,生活品質,以及社交的網絡). 總共有 70 位老人家加入這 個實驗研究,其中 35 位是實驗組,另外 35 位是控制組.實驗組的參與者 每週 兩次在健康中心裡面玩微軟的 Xbox Kinect 體感遊戲,為期六個月. 計劃結束 後,實驗組的體適能以及社交的網絡,有顯著進步,還有 SF8 健康問卷也顯示 出實驗組在生活品質上的 PCS (physical component summary),特別是 bodily pain 有所改善.我們使用 RE-AIM 模式 來為評估這次介入的成果,並對於未來類似 的計劃提出了建議.針對 Kinect 停產,我們延伸出從體感遊戲到正經遊戲的概 念,最後我們討論了可能的商業模式,來擴展整個計劃的成長與持續影響力.
關鍵詞:體感遊戲,正經遊戲,老人健康,商業模式
Abstract
The United Nation report shows that the growth rate of population aged 60 or over is highest among all age groups. Due to lack of muscle strength, older adults tend to exercise less. This study aims to explore whether playing somatosensory games may improve the physical health, quality of life and social network of the elderly. 70 seniors (35 as experimental group, 35 as control) were recruited. The experimental group played Microsoft Xbox Kinect games twice per week in a local health center.
After 6 months, the physical fitness (body composition analysis, muscular analysis, flexibility) and social network of experimental group members showed improvement.
Also, SF8 health survey revealed that experimental group perceived quality of life enhancement in the PCS (physical component summary), particularly bodily pain. We used RE-AIM model to evaluate the intervention program and made suggestions for future replication. In response to the phase-out of Kinect, we expand to serious game concept and discuss potential business model patterns for scale-up.
Key words: somatosensory game, serious game, health of the elderly, business model
doi:10.6342/NTU201801947
v
Table of Contents
Acknowledgements ... ii
Chinese Abstract ... iii
Abstract ... iv
Table of Contents ... v
List of tables ... vi
List of figures ... vii
1. Introduction ... 1
1.1 Background ... 1
1.2 Purpose of the study ... 2
2. Literature Review... 3
2.1 Value proposition ... 3
2.2 Value Creation... 5
2.3 Value Delivery ... 7
2.4 Value Capture ... 8
3. Methods... 9
3.1 Scope ... 9
3.2 Procedures ... 10
3.3 Xbox Kinect Games ... 11
3.4 Test Subjects ... 16
4. Results ... 17
4.1 Physical Fitness ... 18
4.2 Quality of Life ... 20
4.3 Social Network ... 21
5. Discussion ... 22
6. Limitations and suggestions ... 25
7. Conclusions ... 27
References ... 31
List of tables
Table 4-1. Participant demographic statistics ... 17 Table 4-2. Physical Fitness Test: Pretest vs Posttest ... 18 Table 4-3. Experimental group physical fitness trend analysis ... 19 Table 4-4. Quality of Life SF8 Health Survey: Pretest vs Posttest (The lower the
number, the better the quality of life.) ... 20 Table 4-5. Number of acquaintances... 21
doi:10.6342/NTU201801947
vii
List of figures
Fig 3-1. Fruit Ninj ... 11
Fig 3-2. Kinect Sports-FIFA ... 12
Fig 3-3. ShapeUp" – Skiing ... 12
Fig 3-4. ShapeUp - Wrestling ... 13
Fig 3-5. Squid Hero... 13
Fig 3-6. Boom Ball 2 ... 14
Fig 3-7. Rabbids Invasion ... 14
Fig 3-8. Dance Central Spotlight ... 15
Fig 4-1. Experimental group 6 month + baseline physical fitness statistics chart .... 19
Fig 4-2. Cluster Analysis Chart ... 21
1. Introduction 1.1 Background
According to the 2017 world population prospects published by United Nations(United Nations, 2017), aged 60 or over is the fastest growing group among all age groups. The trend is expected to persist over the next few decades, so the increase of older persons' population will continue. Actually aged 80 or over is projected to triple by 2050. In Taiwan, the ageing challenge is even more serious. The ageing rate of Taiwan is more than twice that of the USA and EU countries, due to low fertility rate and high life expectancy(Lin & Huang, 2016). Ageing populations will have significant effects on societies and it is critical to help elderly to stay healthy.
One of the important health factors for the elderly is to exercise regularly. Regular physical activity is good for physical and mental health of older adults. Physical activity can increase life expectancy, improve cardiovascular capacity, build muscle mass, reduce depression, and prevent hypertension. WHO recommends adults aged 65 or older do 150 minutes of moderate-intensity aerobic physical activity per week or do 75 minutes of high-intensity aerobic physical activity per week. However, generally speaking, older adults are less physically active than their younger counterparts.
While many children play games growing up because it is fun, they often stop playing when they reach middle age or golden age. But game could hold the key to encourage the elderly actively participate in physical activities. In addition to providing entertainment, well designed serious games have shown creating benefits in many other domains such as education, health, advertisement and communications.
Playing games may serve as a new way to enhance the physical activity of senior citizens and be part of their healthcare solutions because the fun elements of games can motivate seniors to exercise.
doi:10.6342/NTU201801947
2
1.2 Purpose of the study
So we piloted a 6 month somatosensory game program, inviting elderly to play Microsoft Xbox Kinect games and study whether games can bring benefits to the older adults. Specifically, can playing games improve physical fitness, quality of life or social engagement of the elderly?
2. Literature Review
We search past literatures from business model perspective. A business model is a story about value proposition; and how to create, deliver and capture value. So we look at games from 4 perspectives: value proposition, value creation, value delivery and value capture.
2.1 Value proposition
Many games are originally created for the entertainment purpose. But it is not the only value that games can bring to us.
Training: School teachers today are looking for new ways to educate students.
Allowing students to actively participate in classroom can help them more engaged and open to learning. Chang et al. (2017)(Chang et al., 2017) reported a Kinect based learning system is used to help students learn more about zoo animals with positive results. Students demonstrated enhanced learning outcomes and efficiency by using this Kinect- and game-based interactive learning system. Not only students gained more knowledge of zoo animals, but also they had fun and were motivated while learning.
Quality of life enhancement: As the world population is getting older, there is interest of using game for health promotion of older adults. Chen (2012)(Chen et al., 2012) reported a 4 week training plan video game was applied to help elderly with disabilities. After the intervention, general health, physical function, role physical, and body pain in physical component summary and social functioning in mental component summary of the participants showed significant improvement. The study revealed that video games could be an effective tool for enhancing both physical and social functions of the elderly.
Assessment: There is always need for affordable and accurate measurement tools for physical assessment. Eltoukhy et al. (2018)(Eltoukhy et al., 2018) reported that Microsoft Kinect was used for static and dynamic balance assessment. The study found that Kinect provided valid measurements in assessing center of mass (CoM)
doi:10.6342/NTU201801947
4
excursion and velocity during single leg balance and voluntary ankle sway tasks among young and elderly populations. The findings revealed a low cost technology for assessment of balance parameters in the clinical, research or home environments.
Balance Rehabilitation: To patients that require extended period of rehab, it could be a challenge to stay motivated and actually follow the exercise program throughout the whole process. Betker et al. (2006)(Betker et al., 2006) reported that coupling foot center of pressure (COP) controlled video game is used for balance rehabilitation. The result showed that graded, dynamic balance exercises coupling to video game play can create a fun and effective rehab therapy program.
Compared with conventional exercises that are often repetitive, coupling video game to balance exercises are random, interactive and may be tailored to individual needs. Thus, the practice was more enjoyable and subjects were more motivated to practice during training.
2.2 Value Creation
There are many commercially available games in the market today. Consumers can choose from several brands such as Nintendo Wii, Sony Play Station, and Microsoft Xbox Kinect. These commercially available games can be used to serve intended purposes with appropriate adjustments. But there are times we want to create games from scratch to customize the experience and get the effect we want. In these situations, new games may need to be developed from ground up to tailored to specific needs.
Fall prevention game
Elderly who experience fall can face serious damage to their motion capability, thus having negative impact to their quality of life. Past studies have shown that fall prevention exercises, such as dancing and walking, can improve balance and endurance for older adults, thus reducing falls. Lange et al. (2011)(Lange et al., 2011) reported that a system with step-based exercise and dance video games was developed for elderly. The system consists of a PC, 2 web cameras and 2 LED devices. The game-based interaction was developed using Microsoft Visual Studio 2008 and Ogre3D, an open source gaming engine. The game prototype was initially tested on physical therapists and young participants with positive outcomes. All participants said they enjoyed the experience. Many smiles and laughter were observed while participants playing with the device and software
Whyatt et al. (2015)(Whyatt et al., 2015) reported that Wii was modified and a range of games were developed to deliver effective balance assessment and training for the older population. Unlike commercially available games, balance training games were tailored to the needs of elderly and sensitive to older adults’ movement capabilities. By coupling commercially available hardware with custom-made software programs, they have designed a portable balance training and assessment tool.
Healthy gaming design principles
More and more games are designed for health promotion purpose. Yet it remains to be a challenge to produce games that can be both entertaining and persuasive.
doi:10.6342/NTU201801947
6
Brox et al. (2011)(Brox et al., 2011) reviewed current literature about available health games and broke them into 3 categories: educational games, exergames and persuasive games. They were not able to conclude with certainty what kind of design principles work for what purposes. In other words, they could not find generally applicable game design principles and techniques that may be used to make health games. But they did point out that children may like “rich” games with many contents and information as well as playing together, while older adults may prefer simple games.
Playing somatosensory games using smartwatches
Playing somatosensory game usually require devices from name brand such as Kinect/XBOX or Wii. Also, sizable space is often needed for the comfort of playing games. Pan et al. (2017)(Pan et al., 2017) reported that a newly designed somatosensory game (fighting), which can be played using smartwatches and smart handheld devices. This eliminates the needs of finding a large space and carrying specific devices to play games.
2.3 Value Delivery
For an organization to build a successful business model, it is important to have the proper channels and relationship with its target audiences.
Perceived usefulness, perceived ease of use and usage attitude
Tsai et al. (2013)(Tsai et al., 2013) reported that a fitness testing platform (iFit) was installed in an assisted living community (Chang Gung Health and Culture Village) for fitness promotion and monitoring. Results showed that perceived usefulness, perceived ease of use and usage attitude positively impact behavioral intention to use the platform.
Acceptance of square dancers on a somatosensory game
Yu et al. (2015)(Yu & Rau, 2015) demonstrated the indoor somatosensory games can attract people who usually dance in the park (square dancers) as long as the interface of the game is simple and easy to follow.
Viewing versus Experiencing
Teh et al. (2014)(Teh et al., 2014) reported that when somatosensory technology is viewed, its perceived usefulness is weighed with perceived complexity. However, when somatosensory technology is experienced, the effect of perceived complexity disappears.
doi:10.6342/NTU201801947
8
2.4 Value Capture
For a serious game pilot program to be scalable, an organization needs to build a profitable business model. No papers found discussing the revenue streams or cost structure of using games for elderly health promotion in the organization level.
In our intervention experiment, we will focus on value proposition, i.e. the benefits the elderly gain from playing games. We want to find out whether games can help the elderly improve their physical health, quality of life and enhance their social networking.
3. Methods 3.1 Scope
The study has been approved by Internal Review Board. It was a 6 month program playing Microsoft Xbox One Kinect games on the 2nd floor of Wanhua district health center, Taipei, Taiwan. On the 1st floor, its occupant is an outpatient clinic of Taipei City Hospital, Heping Branch. There were 18 medical staff station for medical service.
This enhances the safety of the elderly participating in the pilot program. From 2017/4/18 to 2017/9/29, 35 participants in experimental group played pre-selected games every Tuesdays and Fridays.
This research adopts quasi-experimental design. The independent variable of this research is playing games. The dependent variables are the elderly's physical health, quality if life and social networking. The data is analyzed using SPSS18.0. The purpose of this project was two folded. On the individual level, we explore whether playing somatosensory games contribute to physical health and quality of life of the elderly. On the group level, we assess if participants may form friendship and thus build stronger social network through playing games together.
doi:10.6342/NTU201801947
10
3.2 Procedures
The start and finish of the 6 month program:
At the beginning and end of the program, all participants need to fill out questionnaire which include:
1. Quality of life
2. Health condition and hospital visit 3. Food and nutrition
4. Community participation 5. Physical activity current status 6. Personal Info
7. Fragility evaluation (Study of Osteoporotic Fractures SOF frail index is used)
Monthly follow-up:
Every month the participants of experimental group would take physical fitness test including
1. Body composition analysis (BCA) 2. Grip strength (hand muscle) 3. 30 second chair rise
4. 2 min leg lifting steps
Every visit (twice per week):
There were 8 time slots (8:45、10:30、14:00、15:45 Tuesdays and Fridays) for experimental group to choose from. The subjects selected one time slot from Tuesdays and another from Fridays. In average, 8 to 9 elderly would come in per time slot. During each visit, the blood pressure of participants will be measured after checking in. The exercises started with warm up exercise, participants would then proceed to play somatosensory games. The total duration for every visit was 90 minutes. Actual exercise game time was 30 to 40 minutes. There were 3 assistants present to help guide elderly playing games and make sure the equipment working properly.
Month
Progra
m
3.3 Xbox Kinect Games
The games were carefully selected for the elderly. The criteria are safe and fun.
Seven Xbox Kinect game pieces (Fruit Ninja, ShapeUp, Kinect Sports-FIFA, Boom Ball 2, Squid Hero, Rabbids Invasion, Dance Central Spotlight) were elected.
The games can be broken down into 3 categories:
1. Double games (for upper limb and lower limb): These games were picked for upper and lower limb exercise purpose. Two subjects played the game together to compete against each other. For example, "Fruit Ninja" was used for upper limb exercise while "Kinect Sports-FIFA" game was chosen for lower limb exercise.
Fig 3-1. Fruit Ninj
doi:10.6342/NTU201801947
12
Fig 3-2. Kinect Sports-FIFA
2. Single games (for aerobic exercise and muscle training): These were single player games for aerobic exercise and muscle training purpose. For instance,
"ShapeUp" was used for aerobic exercise and muscle training.
Fig 3-3. ShapeUp" – Skiing
Fig 3-4. ShapeUp - Wrestling
3. Puzzle games (for collaboration and group dynamics): They were multiple player games that encourage collaboration and group dynamics. For example, "Squid Hero" and "Boom Ball 2" were chosen for enhancing collaboration while "Rabbids Invasion" and "Dance Central Spotlight" were selected for improving group dynamics.
Fig 3-5. Squid Hero
doi:10.6342/NTU201801947
14
Fig 3-6. Boom Ball 2
Fig 3-7. Rabbids Invasion
Fig 3-8. Dance Central Spotlight
doi:10.6342/NTU201801947
16
3.4 Test Subjects
The inclusion criteria for participants of experimental group are 1. Aged 60 or older;
2. Having issue in blood sugar, blood lipid or blood pressure (hyperglycemia, hyperlipidemia or hypertension)
3. BMI (Body Mass Index) greater than 25.
Subjects could join experimental group if he or she meet criterion 1 and one of criterion 2&3.
To ensure the safety of participants, they will be excluded if they have one of the following conditions:
1. Need walkers or canes for mobility
2. Have joined other clinic tests in the past 20 days
3. Expect to move to a new place to live permanently during the 6 month experiment
4. Have severe dementia, neurological disease, cardiovascular disease, recent stroke, or psychosis
The availability of this program was promoted via 1. hospitals referral or
2. distribution of flyers to clinics, hospitals and health centers or 3. Facebook, LINE groups.
Some participants of experimental group were referrals from local clinics in Wanhua district and NTUH (National Taiwan University Hospital) Bei-Hu Branch. Others simply expressed that they had hyperglycemia, hyperlipidemia or hypertension or their BMI was greater than 25 in pre test survey. Eventually 70 qualified citizens were selected: 35 experimental group members and 35 control group members.
4. Results
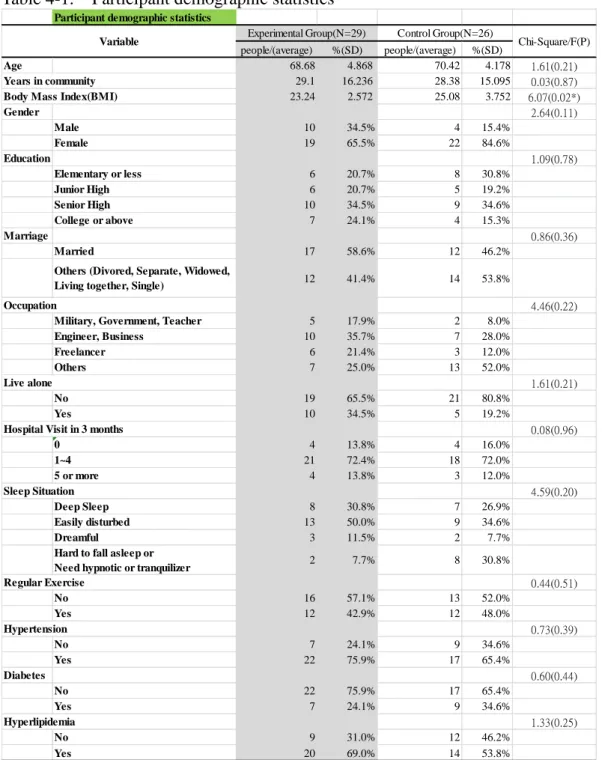
After 6 month period, 29 experimental group members and 26 control group members stay throughout the program. The participant demographic statistics is listed below.
The body mass index (BMI) of experimental group is lower than that of control group is the beginning. Other than BMI, all other factors are the similar between 2 groups.
Table 4-1. Participant demographic statistics
Participant demographic statistics
people/(average) %(SD) people/(average) %(SD)
Age 68.68 4.868 70.42 4.178 1.61(0.21)
Years in community 29.1 16.236 28.38 15.095 0.03(0.87)
Body Mass Index(BMI) 23.24 2.572 25.08 3.752 6.07(0.02*)
Gender 2.64(0.11)
Male 10 34.5% 4 15.4%
Female 19 65.5% 22 84.6%
Education 1.09(0.78)
Elementary or less 6 20.7% 8 30.8%
Junior High 6 20.7% 5 19.2%
Senior High 10 34.5% 9 34.6%
College or above 7 24.1% 4 15.3%
Marriage 0.86(0.36)
Married 17 58.6% 12 46.2%
Others (Divored, Separate, Widowed,
Living together, Single) 12 41.4% 14 53.8%
Occupation 4.46(0.22)
Military, Government, Teacher 5 17.9% 2 8.0%
Engineer, Business 10 35.7% 7 28.0%
Freelancer 6 21.4% 3 12.0%
Others 7 25.0% 13 52.0%
Live alone 1.61(0.21)
No 19 65.5% 21 80.8%
Yes 10 34.5% 5 19.2%
Hospital Visit in 3 months 0.08(0.96)
0 4 13.8% 4 16.0%
1~4 21 72.4% 18 72.0%
5 or more 4 13.8% 3 12.0%
Sleep Situation 4.59(0.20)
Deep Sleep 8 30.8% 7 26.9%
Easily disturbed 13 50.0% 9 34.6%
Dreamful 3 11.5% 2 7.7%
Hard to fall asleep or
Need hypnotic or tranquilizer 2 7.7% 8 30.8%
Regular Exercise 0.44(0.51)
No 16 57.1% 13 52.0%
Yes 12 42.9% 12 48.0%
Hypertension 0.73(0.39)
No 7 24.1% 9 34.6%
Yes 22 75.9% 17 65.4%
Diabetes 0.60(0.44)
No 22 75.9% 17 65.4%
Yes 7 24.1% 9 34.6%
Hyperlipidemia 1.33(0.25)
No 9 31.0% 12 46.2%
Yes 20 69.0% 14 53.8%
Experimental Group(N=29) Control Group(N=26)
Chi-Square/F(P) Variable
doi:10.6342/NTU201801947
18
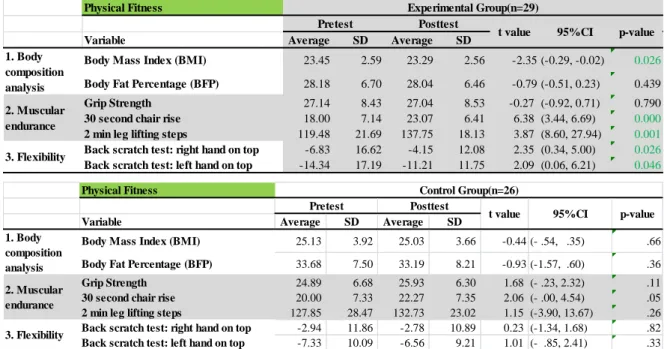
4.1 Physical Fitness
We conducted the physical fitness focusing on 3 dimensions: body composition analysis, muscular endurance and flexibility. By looking at the pretest and posttest data in experimental group, we noticed some improvements. In the body composition analysis category, body mass index (BMI) went from 23.45 to 23.29. In muscular endurance category, 30 second chair rise jumped from 18 to 23.07. 2 min leg lifting increased from 119.48 to 137.75. In the flexibility category, back scratch test: right hand on top went from -6.83 to -4.15 while back scratch test: left hand on top also improved from -14.34 to -11.21. On the other hand, there is no statistically significant improvement in the control group in all categories.
Table 4-2. Physical Fitness Test: Pretest vs Posttest
Physical Fitness
Variable Average SD Average SD
Body Mass Index (BMI) 23.45 2.59 23.29 2.56 -2.35 (-0.29, -0.02) 0.026
Body Fat Percentage (BFP) 28.18 6.70 28.04 6.46 -0.79 (-0.51, 0.23) 0.439
Grip Strength 27.14 8.43 27.04 8.53 -0.27 (-0.92, 0.71) 0.790
30 second chair rise 18.00 7.14 23.07 6.41 6.38 (3.44, 6.69) 0.000
2 min leg lifting steps 119.48 21.69 137.75 18.13 3.87 (8.60, 27.94) 0.001 Back scratch test: right hand on top -6.83 16.62 -4.15 12.08 2.35 (0.34, 5.00) 0.026 Back scratch test: left hand on top -14.34 17.19 -11.21 11.75 2.09 (0.06, 6.21) 0.046 1. Body
composition analysis 2. Muscular endurance
3. Flexibility
Experimental Group(n=29)
Pretest Posttest
t value 95%CI p-value
Physical Fitness
Variable Average SD Average SD
Body Mass Index (BMI) 25.13 3.92 25.03 3.66 -0.44 (- .54, .35) .66
Body Fat Percentage (BFP) 33.68 7.50 33.19 8.21 -0.93 (-1.57, .60) .36
Grip Strength 24.89 6.68 25.93 6.30 1.68 (- .23, 2.32) .11
30 second chair rise 20.00 7.33 22.27 7.35 2.06 (- .00, 4.54) .05
2 min leg lifting steps 127.85 28.47 132.73 23.02 1.15 (-3.90, 13.67) .26 Back scratch test: right hand on top -2.94 11.86 -2.78 10.89 0.23 (-1.34, 1.68) .82 Back scratch test: left hand on top -7.33 10.09 -6.56 9.21 1.01 (- .85, 2.41) .33 1. Body
composition analysis 2. Muscular endurance
3. Flexibility
Control Group(n=26) Posttest
t value 95%CI p-value Pretest
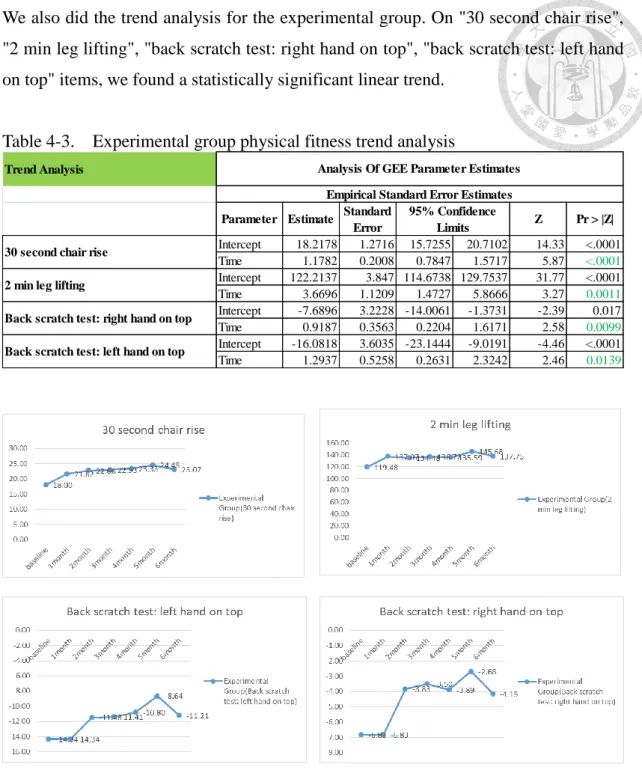
We also did the trend analysis for the experimental group. On "30 second chair rise",
"2 min leg lifting", "back scratch test: right hand on top", "back scratch test: left hand on top" items, we found a statistically significant linear trend.
Table 4-3. Experimental group physical fitness trend analysis
Fig 4-1. Experimental group 6 month + baseline physical fitness statistics chart
Trend Analysis
Parameter Estimate Standard
Error Z Pr > |Z|
Intercept 18.2178 1.2716 15.7255 20.7102 14.33 <.0001 Time 1.1782 0.2008 0.7847 1.5717 5.87 <.0001 Intercept 122.2137 3.847 114.6738 129.7537 31.77 <.0001
Time 3.6696 1.1209 1.4727 5.8666 3.27 0.0011
Intercept -7.6896 3.2228 -14.0061 -1.3731 -2.39 0.017
Time 0.9187 0.3563 0.2204 1.6171 2.58 0.0099
Intercept -16.0818 3.6035 -23.1444 -9.0191 -4.46 <.0001
Time 1.2937 0.5258 0.2631 2.3242 2.46 0.0139
Back scratch test: right hand on top
Back scratch test: left hand on top
Analysis Of GEE Parameter Estimates Empirical Standard Error Estimates
95% Confidence Limits 30 second chair rise
2 min leg lifting
doi:10.6342/NTU201801947
20
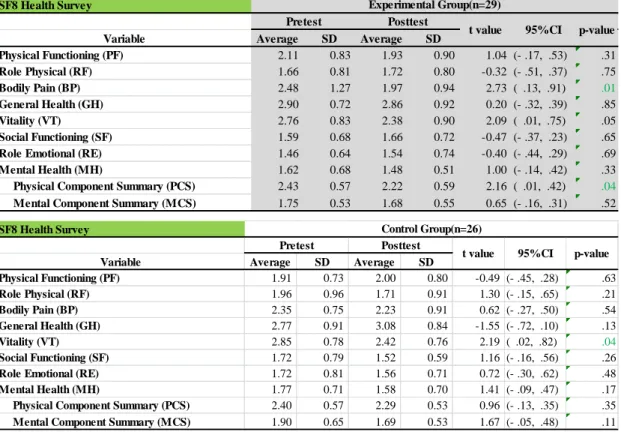
4.2 Quality of Life
We used SF8 health survey to measure the perceived quality of life. The lower the score in the survey, the better the perceived quality of life. In the experimental group, physical component summary (PCS) showed improvement, particularly on bodily pain domain. In the control group, neither physical component summary (PCS) nor mental component summary (MCS) demonstrate changes statistically. Only vitality domain improved but not enough to lead to overall MCS change.
Table 4-4. Quality of Life SF8 Health Survey: Pretest vs Posttest (The lower the number, the better the quality of life.)
SF8 Health Survey
Variable Average SD Average SD
Physical Functioning (PF) 2.11 0.83 1.93 0.90 1.04 (- .17, .53) .31
Role Physical (RF) 1.66 0.81 1.72 0.80 -0.32 (- .51, .37) .75
Bodily Pain (BP) 2.48 1.27 1.97 0.94 2.73 ( .13, .91) .01
General Health (GH) 2.90 0.72 2.86 0.92 0.20 (- .32, .39) .85
Vitality (VT) 2.76 0.83 2.38 0.90 2.09 ( .01, .75) .05
Social Functioning (SF) 1.59 0.68 1.66 0.72 -0.47 (- .37, .23) .65
Role Emotional (RE) 1.46 0.64 1.54 0.74 -0.40 (- .44, .29) .69
Mental Health (MH) 1.62 0.68 1.48 0.51 1.00 (- .14, .42) .33
Physical Component Summary (PCS) 2.43 0.57 2.22 0.59 2.16 ( .01, .42) .04 Mental Component Summary (MCS) 1.75 0.53 1.68 0.55 0.65 (- .16, .31) .52
Experimental Group(n=29)
Pretest Posttest
t value 95%CI p-value
SF8 Health Survey
Variable Average SD Average SD
Physical Functioning (PF) 1.91 0.73 2.00 0.80 -0.49 (- .45, .28) .63
Role Physical (RF) 1.96 0.96 1.71 0.91 1.30 (- .15, .65) .21
Bodily Pain (BP) 2.35 0.75 2.23 0.91 0.62 (- .27, .50) .54
General Health (GH) 2.77 0.91 3.08 0.84 -1.55 (- .72, .10) .13
Vitality (VT) 2.85 0.78 2.42 0.76 2.19 ( .02, .82) .04
Social Functioning (SF) 1.72 0.79 1.52 0.59 1.16 (- .16, .56) .26
Role Emotional (RE) 1.72 0.81 1.56 0.71 0.72 (- .30, .62) .48
Mental Health (MH) 1.77 0.71 1.58 0.70 1.41 (- .09, .47) .17
Physical Component Summary (PCS) 2.40 0.57 2.29 0.53 0.96 (- .13, .35) .35 Mental Component Summary (MCS) 1.90 0.65 1.69 0.53 1.67 (- .05, .48) .11
Control Group(n=26) Posttest
t value 95%CI p-value Pretest
4.3 Social Network
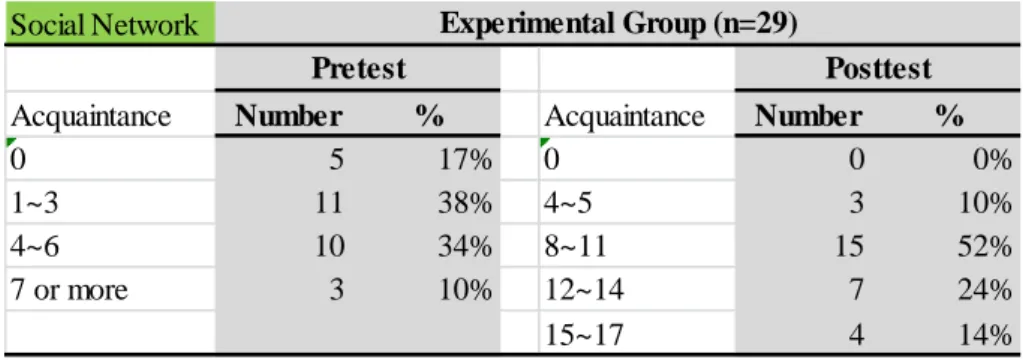
We ask the experimental group whether they know one another before and after the 6 month intervention. Before the program started, 5 participants knew no one in the group and most of them know 1 to 6 people. Only 3 participants knew 7 or more people. After 6 month intervention, the survey revealed that all of the participants have at least 4 friends and 11 in average. Most of them have 8 to 14 friends. Some (4 people) even got to know 15 to 17 friends.
Table 4-5. Number of acquaintances
Moreover, the cluster analysis chart also showed the participants' network increased noticeably after the 6 month test.
Fig 4-2. Cluster Analysis Chart
Social Network
Acquaintance Number % Acquaintance Number %
0 5 17% 0 0 0%
1~3 11 38% 4~5 3 10%
4~6 10 34% 8~11 15 52%
7 or more 3 10% 12~14 7 24%
15~17 4 14%
Experimental Group (n=29)
Pretest Posttest
After Before
doi:10.6342/NTU201801947
22
5. Discussion
RE-AIM model is commonly used for evaluating health intervention to general public(李蘭 et al., 2010). We apply RE-AIM as our discussion framework to assess the impact of our 6 month program.
5.1 Reach: How do we reach our target population?
35 experimental group and 35 control group members were recruited. Some experimental group participants were referrals from local clinics in Wanhua district and NTUH (National Taiwan University Hospital) Bei-Hu Branch while some control group members were volunteers from Wanhua district health center. This may compromise the randomness of the samples. If budget and time allows, we may improve on advertising and outreach. For example, we may show up in local events to promote our program. Recruit seniors as our program team members. Utilize radio, use display in the elderly hang-out locations, such as senior community centers.
Also, when we pick seniors to join experimental group, we simply ask them to get the answers without verifying it. We were not 100% certain that they were really our target population (for example, having hyperglycemia, hyperlipidemia or hypertension). Additional efforts could be added for ensuring that the right population are selected.
Plus, at the end of 6 month period, only 29 experimental group (83%) and 26 control group members (74%) still stayed with the program. This showed that we have room for improvement in terms of participant retention. The attrition (churn) rate is especially high in control group. This might have something to do with the fact that the program lasted 6 long months. If we could also conduct regular monthly physical test on control group, it might potentially reduce the churn rate.
5.2 Effectiveness or Efficacy: How do we know our intervention is effective?
Firstly, the physical condition of participants did improve. All categories (body composition analysis, muscular endurance, and flexibility) in the physical fitness test of experimental group showed improvement comparing posttest and pretest data. To
be specific, several variables such as body mass index (BMI), 30 second chair rise, 2 min leg lifting, and back scratch test were statistically better. On the other hand, none of variables in control group improved between pretest and posttest statistics. The trend analysis of the experimental group in 30 second chair rise, 2 min leg lifting, and back scratch test confirms that the improvement trend is linear.
Secondly, the quality of life SF8 survey showed that experimental group did feel improvement on their physical component, particularly bodily pain. However, their mental component remained unchanged. On control group, there was slight enhancement on vitality. Neither physical nor mental component summary in control group statistically improved.
Thirdly, participants' social network did strengthen. We observe more interactions onsite among participants, more friendship made among seniors and cluster network analysis also confirms that.
5.3 Adoption: How do we develop the institutional support for the intervention?
Our intervention was fully supported by the head of Wanhua district health center throughout the program. With the positive health influence, our intervention may be spread to other health centers. Plus, the demonstrated health results already convinced a vice president of Taiwanese cement company, Hsing Ta Cement Company, to implement a similar program in I-Lan to help local community senior citizens and consider launching a similar program inside the company for the betterment of employees' health in the future. Moreover, MacKay Memorial Hospital Tamsui Branch also expressed interest in applying the gaming program into their volunteer network.
5.4 Implementation: How do we ensure the intervention is delivered properly?
XBox games were carefully previewed and test played to find the most appropriate game sets for the elderly. Assistants from National Taiwan University were onsite when the games were played to ensure the proper procedures were followed and machinery was functioning adequately. Also, we had integrated logistics support, meaning snack, tea, water and chairs were provided to keep the energy up.
doi:10.6342/NTU201801947
24
5.5 Maintenance: How do we incorporate intervention so it is delivered over the long term?
Even though the 6 month program ended on a success, Wanhua district health center could not find additional funding to sustain the program. The ability to secure monetary resource from the government is crucial to sustain the program, particularly in the early stage. Also, we may ask private companies with corporate social responsibility (CSR) program to sponsor. In the long run, it is best a viable business model can be developed.
6. Limitations and suggestions
The intervention proved to be working. There are some limitations learned and suggestions for future program implementation.
6.1 Program Design
1. 3 XBox machines were used and may accommodate up to 10 players. The recommended numbers of players is six for maximum comfort.
2. We only used 7 game set for the duration of 6 month program. More variety of games will be helpful in attracting the interests of the elderly.
3. During each visit, the elderly played roughly 30 to 40 minutes of games. To fully benefit from the experience, the play game can be extended to 60 minutes.
4. 6 month program time length was too long for some seniors. It can be shortened to 3 months.
6.2 Program Execution
1. Since the participants are old, it is advised to insure for all the activities in the program.
2. The playing environment should be kept safe. Pay attention to participants' clothes and physical condition for safety reason.
3. In our program, some restrictions on who might join were imposed for research purpose. These limits can be lifted to include people from all walks of life.
4. We only gave out physical test results to participants at the of 6 month intervention. More frequent (e.g. monthly) health report update can boost the morale and encourage seniors to stay with the program.
6.3 Program Expansion
1. The budget for the program include three set of 60 inch LCD TV (NTD 50k to 60k each) and three Xbox+Kinect (NTD 10k each), and 7 game sets (NTD 500 to 2000 each). The total adds up to 200k NTD. This may pose problems to small community centers with little budget.
2. Xbox games are not designed for the elderly. So the number of game
doi:10.6342/NTU201801947
26
selection suited for older adults is limited.
3. It takes some getting used to for the elderly to master XBox games so assistants' onsite presence is needed. Recruiting and training volunteers is important.
4. Microsoft announced Xbox Kinect to be discontinued, starting from Oct 2017. Without Kinect, it may pose challenges to run the somatosensory game based intervention program once all Kinect devices are sold out in the market. There are a few alternatives:
I. Switch to controller based games such as Microsoft Xbox, Sony PS4, or Nintendo Wii Switch. The downside is that seniors may have difficulty in handling controllers.
II. If we still prefer to play without controller, we may buy systems from somatosensory game based vendors such as LongGood. But the price could be much higher. Or buy other depth sensors in the market, such as Orbbec.
III. Expand on playing serious games. We will discuss more on this in Conclusion.
7. Conclusions
7.1 Somatosensory game for physical health and social engagement
The statistics collected from the 6 month program indicated that playing game regularly may help elderly physically and socially.
The physical fitness test of experimental group between posttest and pretest data showed statistically significant improvement. The trend analysis also confirms the improvement is linear throughout the 6 month intervention. On the other hand, none of the variables in control group become better.
On the quality of life issue, SF8 health survey revealed that the physical component summary(PCS) of experimental group was enhanced. The mental component summary(MCS) of experimental group did not change.
The cluster analysis of seniors' social network confirms that the elderly make more friends while playing games.
7.2 Serious game for easier adoption
Even with the successful outcome, the promotion of the program still face uphill challenge with constraints like funding, playing space, gaming equipment and onsite assistants. For future applications, researchers and practitioners may consider developing new or utilizing existing serious games for health. Serious game is a game designed for purposes other than fun. It was first proposed by Clark Abt in 1970.
There are a few reasons that we favor the term, serious game. First of all, by definition, our intervention program is one kind of serious games. With the end of Kinect product line, the low cost somatosensory games in the market have become hard to come by. Rather than sticking to somatosensory games, organizations may choose serious games that may come in more variety of formats as they see fit. This mindset shift may help facilitate the organizations' adoption in application of games for health.
doi:10.6342/NTU201801947
28
Secondly, when extending to the serious game concept, organizations may add learning (education) element into game program design. This may generate additional flavor for the program and could potentially attract more seniors to join and stick with the program.
Last but not the least, in additional to health promotion purpose of our intervention, serious games can be tailored for different stages of disease such as health monitoring, health detection, treatment/therapy, and rehabilitation. This provides added tools for healthcare professionals.
So a mindset shift from somatosensory game to serious game can open up broader health applications to larger target audience. This could help spread the similar program implementation.
7.3 Business model innovation for sustainable scale-up
For organizations that want to expand on this senior health gaming concept and scale-up, a viable business model would need to be tested and proven in the marketplace. There are high expectations for the growing silver economy; yet the seniors are more reluctant to pay for product or service that they don't deem essential.
This wreaks havoc for companies that target their products/services on the elderly.
By applying Osterwalder et al. (2010)(Osterwalder & Pigneur, 2010) business model tool, five patterns are worthy of exploring:
Unbundling business models:
Organizations should focus on one of three business types: product innovation, customer relationship or infrastructure. In 2008 Asus ComputerTek unbundled its OEM division and created a separate company, Pegatron. Asus focuses on branded computer while Pegatron stays with OEM manufacturing root. By doing so, both Asus and Pegatron blossom. By the same token, the health gaming business unit in a large company can be considered unbundling into individual entity to prevent conflicts.
Long tail:
Internet allows companies to sell niche products to large number customers, a phenomenon called long tail. For example, Twitch creates a platform connecting game players and viewers. If a company can build a platform allowing elderly broadcasting their gaming activities, it might establish a profitable business with long tail of user generated games for seniors.
Multiple-sided platforms:
The Eslite is a thriving bookstore chain in Taiwan. It does not make profit on selling books but on the rent and profit sharing from contracted restaurants and design shops surrounding its book stores. Consumers are attracted to Eslite for its cozy reading environment, and often end up buying stuff other than books.
Likewise, a serious game for health business model may not make profit from the older adults playing games, but from the store selling other products or services (e.g. nutritional supplement, cosmetic product for the elderly).
FREE as a business model
All the sports centers run by Taipei City offer the "get the basic for free, pay for more" model. Some facilities in sports centers are free to senior citizens for a certain hours of the day. Older adults are attracted to visit sports centers during free hours. Sometimes they pay to stay longer or invite younger family members who pay. Following the same logic, a company may offer free basic services to the elderly with paid premium services.
Open business models
Lots of health statistics of the elderly are collected in the program that may be used by doctors for health prevention, rehabilitation or disease treatment. A health gaming company may partner with hospitals and research institutions by providing the statistics and in return getting feedback on designing better exercise games or medical treatment for the elderly. Or they could become a market research company by understanding the elderly's behaviors and preferences. If they could paint the detailed picture of the world of the elderly, they may sell the insights to companies serving senior market.
doi:10.6342/NTU201801947
30
All these business models above are just ideas that have to be tested in the market for its validity. Prototyping and piloting are needed to gain more insights. The more organizations try out innovative business models, the closer we will be getting to bring active ageing into reality.
References
Betker, A. L., Szturm, T., Moussavi, Z. K., & Nett, C. (2006). Video game–based exercises for balance rehabilitation: a single-subject design. Archives of physical medicine and rehabilitation, 87(8), 1141-1149.
Brox, E., Fernandez-Luque, L., & Tøllefsen, T. (2011). Healthy gaming–video game design to promote health. Applied clinical informatics, 2(02), 128-142.
Chang, Y.-H., Hwang, J.-H., Fang, R.-J., Lu, Y.-T., & Lin, Y.-K. (2017). A Kinect-and Game-Based Interactive Learning System. Eurasia Journal of Mathematics, Science and Technology Education, 13(8), 4897-4914.
Chen, S.-T., Huang, Y.-G. L., & Chiang, I.-T. (2012). Using somatosensory video games to promote quality of life for the elderly with disabilities. Paper presented at the Digital Game and Intelligent Toy Enhanced Learning (DIGITEL), 2012 IEEE Fourth International Conference on.
Eltoukhy, M. A., Kuenze, C., Oh, J., & Signorile, J. F. (2018). Validation of static and dynamic balance assessment using Microsoft Kinect for young and elderly populations. IEEE journal of biomedical and health informatics, 22(1), 147-153.
Lange, B., Flynn, S., Chang, C.-Y., Liang, W., Si, Y., Nanavati, C., & Chieng, C.-L.
(2011). Development of an interactive stepping game to reduce falls in older adults. International Journal on Disability and Human Development, 10(4), 331-335.
Lin, Y. Y., & Huang, C. S. (2016). Aging in Taiwan: Building a Society for Active Aging and Aging in Place. Gerontologist, 56(2), 176-183.
Osterwalder, A., & Pigneur, Y. (2010). Business model generation: a handbook for visionaries, game changers, and challengers: John Wiley & Sons.
Pan, M.-S., Hsu, W.-C., Liu, C.-H., Huang, K.-C., & Cheng, C.-F. (2017).
InstantGaming: Playing somatosensory games using smartwatches and portable devices. Paper presented at the Applied System Innovation (ICASI), 2017 International Conference on.
Teh, P.-L., Ahmed, P. K., Goonetilleke, R. S., Au, E. Y. L., Cheong, S.-N., & Yap, W.-J.
(2014). Viewing versus experiencing in adopting somatosensory technology for smart applications. Pacific Asia Journal of the Association for Information Systems, 6(3).
Tsai, T.-H., Wong, A. M.-K., Hsu, C.-L., & Tseng, K. C. (2013). Research on a community-based platform for promoting health and physical fitness in the elderly community. PloS one, 8(2), e57452.
United Nations. (2017). 2017 Revision of World Population Prospects Retrieved June 1, 2018, from https://esa.un.org/unpd/wpp/
Whyatt, C., Merriman, N. A., Young, W. R., Newell, F. N., & Craig, C. (2015). A Wii bit of fun: a novel platform to deliver effective balance training to older adults.
Games for health journal, 4(6), 423-433.
Yu, C.-W., & Rau, P.-L. P. (2015). Studying the acceptance of somatosensory game for Chinese square dancers. Procedia Manufacturing, 3, 2213-2218.
李蘭, 晏涵文, 陳富莉, 陸玓玲, 吳文琪, & 江宜珍. (2010). 健康行為與健康教 育: 臺北: 巨流圖書, 2010.