行政院國家科學委員會專題研究計畫 成果報告
大動脈完全轉位術後左右肺動脈成長之研究
計畫類別: 個別型計畫 計畫編號: NSC93-2314-B-002-238- 執行期間: 93 年 08 月 01 日至 94 年 12 月 31 日 執行單位: 國立臺灣大學醫學院外科 計畫主持人: 邱英世 共同主持人: 王主科 報告類型: 精簡報告 處理方式: 本計畫可公開查詢中 華 民 國 95 年 1 月 27 日
行政院國家科學委員會專題研究計畫成果報告
計畫名稱:大動脈完全轉位術後左右肺動脈成長之研究
計畫編號:NSC 93-2314-B-002-238
執行期限:93 年 8 月 1 日至 94 年 12 月 31 日
計畫主持人:邱英世 國立台灣大學醫學院 外科
共同主持人:王主科 國立台灣大學醫學院 小兒科
一、中英文摘要 大動脈轉位手術已成為大動脈完全轉位病例之常規手術及選擇術式。但術後併發瓣 膜上性肺動脈狹窄仍為目前存在之問題。有些左右肺動脈形成不良在大動脈轉位手術之 前即已存在。我們比較大動脈完全轉位病例術前和術後之肺動脈血管攝影擬找出發生左 右肺動脈形成不良之機轉。並比較兩種分期性手術(分流手術或加上肺動脈幹束紮)及 兩種治本性手術後(心房轉位手術與大動脈轉換手術)之成長情形。我們發現只做分流 手術之病例(n=3)肺動脈會變小,如加上肺動脈幹束紮(n=2),使心舒期也有左至右 分流才能讓肺動脈生長。心房轉位手術(n=4)使肺動脈幹仍居後位,比大動脈轉換手 術(n=14)術後肺動脈生長情形差。此術後病史與我們之前發表自然病史發病之機轉雷 同。簡言之,大動脈完全轉位發生左右肺動脈形成不良之機轉為存開性動脈導管或外科 分流術造成右至左分流形成血行力學性飢餓有關,以及後位性肺動脈幹(肺動脈幹後緣 與左右肺動脈前緣角度較小)所造成,我們認為針對此病理發生之術式才能避免瓣膜上 性肺動脈狹窄。 關鍵詞:左右肺動脈形成不良,Senning 手術,大動脈轉換手術,大動脈完全轉位,瓣 膜上性肺動脈狹窄,Lecompte 手法。 AbstractIn the present era of arterial switch operation, supravalvular pulmonary stenosis remains a problem. First branch pulmonary arterial hypoplasia in transposition of the great arteries was documented prior to and after palliative or corrective surgery. We sought to determine the morphological features of the pulmonary trunk (PT) and its branches susceptible to first branch pulmonary arterial (PA) hypoplasia in transposition of the great arteries (TGA). All available angiograms between 1981 and 2003 were reviewed and polaroid photos were taken at end-systolic phase. The diameters of the right PA (RPA), the left PA (LPA) and the PT before their first branch, and the angle between the RPA and right border of the PT were measured in frontal view. In addition, the angle between both PA and posterior border of the PT, and the diameter of the ascending aorta were measured in lateral view. The diameter ratio of PA to PT was compared before and after two palliative operations (shunt with or without concomitant PT banding) and two corrective operations (Senning or Jatene). We found that shunt alone (n=3) had regression of PA size. Whereas those who had concomitant PT banding (n=2) to abolish hemodynamic starvation had PA growth. Those who underwent Senning operation (n=4) had PA growth, but the growth was not as good and rapid as Jatene group with Lecompte maneuver (n=14).Thus the natural and second natural history of PA hypoplasia in TGA is about the same, namely, hemodynamic starvation and posterior inclination of PT
would lead to PA hypoplasia in TGA both before and after surgical intervention. We conclude that the surgical options that eliminate the-above-mentioned pathogenesis of PA hypoplasia like shunt with PT banding or Jatene with Lecompte (or had better with Pacifico or spiral reconstruction) could facilitate PA growth in TGA.
Keywords: First branch pulmonary arterial hypoplasia, Senning operation, Arterial switch
operation, Transposition of the great arteries, Supravalvular pulmonary stenosis, Lecompte maneuver.
二、Introduction
At present, arterial switch operation has become the repair of choice for transposition of the great arteries (TGA) with or without ventricular septal defect.1-2However, this operation is not complication-free. In addition to neoaortic regurgitation,3coronary insufficiency4and arterial suture line stenosis,5supravalvular pulmonary stenosis remains one of the most
worrisome problems.5-11Some maintain that it is not related to the Lecompte maneuver7while others suspect that it is.5,6A larger pericardial patch, advocated to eliminate this
morbidity,6,7,12 has not been effective for others.10
The appearance of gross dilatation of the pulmonary trunk with hypoplastic first branch pulmonary arteries(PA)lookslike“two armsfrom theshoulder”.13
Paillole documented the existence of first branch PA hypoplasia before surgery and its persistence until after arterial switch operation.7Itisdocumented that“arms from the shoulder”picturecan also beseen in
congenitally corrected TGA.14To restore the proximal PT to its natural position in congenitally or acquired corrected transposition for better PA growth is another justified reason for double switch operation.15,16
The operation of choice should be decided upon the pathogenesis, so that the best result with least complication could be obtained. First branch PA hypoplasia existed before surgical correction and persisted postoperatively7,13. Recognition of the pathogenesis of first branch PA hypoplasia in TGA and the influence of various surgical options is the cornerstone of the successful surgery and perfect correction.
In this communication, we sought to determine the influence of the surgical procedures on first branch PA hypoplasia before and after surgical treatment for TGA.
三、Patients and Methods
Study patients
The hospital records of all patients with complete TGA who were referred to our hospitals between 1981 and 2003 were reviewed; patients without clear delineation of pulmonary trunk (PT) and PA on angiograms were excluded from this study. Only patients with situs solitus of the viscera and atria, atrioventricular concordance and ventriculoarterial discordance, two patent atrioventricular valves and two patent semilunar valves were included. The systolic pressures in the pulmonary artery and the left ventricle were collected if entered during cardiac catheterization.
Polaroid photos (Polaroid, Cat. No. 617798, Hertfordshire, UK) were taken at end-systolic phase for each case from biplane cineangiograms. The diameters of the right pulmonary artery (RPA), left pulmonary artery (LPA) and PT before their first branch were measured in frontal view. The diameter of the LPA was compared with that of the RPA. If LPA was obscured by PT in frontal projection, another view such as oblique or lateral was selected for comparison. The diameter of the ascending aorta before the branchiocephalic
artery, the angle between posterior border of the PT and both PAs were evaluated on lateral view.
Patients were categorized into four groups according to PA to PT diameter ratio (PA/PT). A ratio above 0.71 was defined as normal. Ratios of 0.70 to 0.50, 0.49 to 0.41, and below 0.40 were defined as mild, moderate and severe hypoplasia, respectively. The flow through a branch is in proportion to its cross-sectional area, hence the flow ratio is equal to the square of the diameter ratio, i.e. >1/2, 1/2-1/4, 1/4-1/6, <1/6 in each group, respectively. The follow-up angiograms were analyzed as mentioned above and compared with the initial examination.
Data Analysis
Numerical data are expressed as mean±SD, except when otherwise noted. Differences between the means of angiographic measurements at initial and follow-up studies were compared by paired Student’sttest;unpaired t-test was used to compare the two groups. The differences among the four groups were tested by one-way analysis of variance (ANOVA). Data analysis was performed on an IBM personal computer with a commercially available statistical package (SPSS version 3.0, SPSS Inc. Chicago, Illinois, USA). For all tests, a value of p<0.05 was considered significant.
.
四、Results
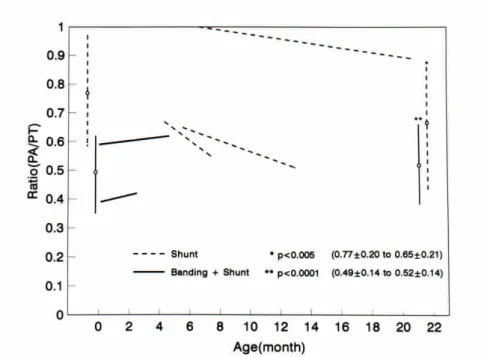
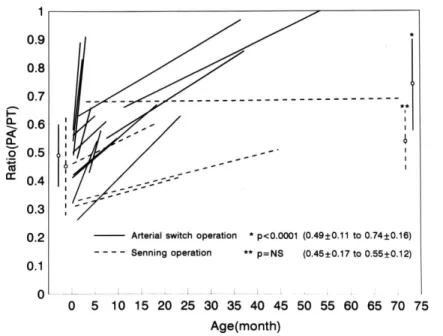
Three patients with simple transposition of the great arteries, who underwent a modified Blalock-Taussig shunt at age 7.5±2.3 months for left ventricular preparation,17had regression of PA size (Fig. 1). The direction of blood flow through the shunt was toward the aorta during early systole and toward the PA from late systole to diastole. In contrast, those who had PT banding in addition to a Blalock-Taussig shunt (n=2, age 1.9±0.6 months) had PA growth. The direction of blood flow across the shunt was toward the PA throughout the cardiac cycle. Fourteen patients who underwent arterial switch operations with the Lecompte maneuver (age 2.5±3.4 months) had follow-up angiogram (Fig. 2). All had evidence of good PA growth (PA/PT from 0.49±0.11 to 0.74±0.16, p<0.0001) (Figs. 2-4). Four patients who underwent the Senning procedure (age 8.0±5.1 months) had PA growth (PA/PT from 0.45±0.17 to 0.55±0.12, P=NS), but the growth was not as good (Fig. 3) or as rapid (the rate of growth was defined as increase of PA/PT divided by the time interval, 0.004±0.003 vs 0.053±0.062, p<0.02) as that in the arterial switch group (Fig. 4). At follow-up, the PA/PT angle in degrees as measured in the lateral view was significantly wider in the arterial-switch (right, 70±14 to 96±14; left, 82±14 to 108±8, p<0.0001) than in the Senning group (right, 59±6 to 60±11; left, 78±11 to 80±4; p=NS). The follow-up duration (from the date of operation to angiographic restudy) between the arterial-switch and Senning groups (13.1±14.0 vs. 30.9±23.5 months) did not reveal any significant difference. Table 1 and Table 2 listed the number of cases in each category before and after operation. In the Senning and shunt group PA growth is not evident as in the ASO and shunt + PTB group, respectively.
Fig. 1 ↑A surgical shunt alone (bold-dashed line) retards pulmonary arterial growth significantly, whereas banding plus shunt (solid) increases the pulmonary arterial growth significantly.
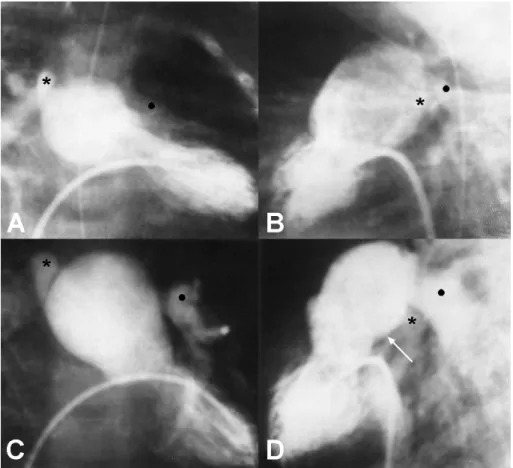
Fig. 2 ↑Angiograms before (A and B) and after (C and D) arterial switch operation. The smooth direction of blood flow and anteriorly inclined pulmonary trunk (white arrow)
after operation (C and D) permitted satisfactory pulmonary arterial growth from a typical “arms from the shoulder”appearance in A. Please note the acute angle
between the posterior border of the pulmonary trunk (PT) and the right pulmonary artery (star) or left pulmonary artery (dot) in B.
Fig. 3 ↑Angiograms before (A and B) and after (C and D) Senning operation. The unsmooth direction of blood flow and posteriorly inclined pulmonary trunk (white arrow) persisted after operation (D) did not permit satisfactory pulmonary arterial growth from a typical “arms from the shoulder”appearance in A. Please note the acute angle
between the posterior border of the pulmonary trunk (PT) and the right pulmonary artery (star) or left pulmonary artery (dot) in B and D.
Fig. 4 ↑There was significantly better growth in the arterial switch group (solid line) than in the Senning group (bold-dashed line). The rate of growth as shown by the slope of each line is significantly faster in the arterial switch group than the Senning group (p<0.02).
Table 1 No of cases before and after corrective operation Group ASO* (n=14) Senning (n=4)
Normal (≧0.71) 0→6 0→0
Borderline (0.70-0.50)
hypoplasia 8→8 1→3
Significant (≦0.49)
hypoplasia 6→0 3→1
*ASO=Arterial Switch Operation.
Table 2 No of cases before and after palliative operation
Group Shunt + PTB* (n=2) Shunt (n=3) Normal (≧0.71) 0→0 1→1 Borderline (0.70-0.50) hypoplasia 1→1 2→2 Significant (≦0.49) hypoplasia 1→1 0→0
*PTB=Pulmonary Trunk Banding.
五、Discussion
Supravalvular pulmonary stenosis has been reported to be more common when arterial switch operation was performed in the neonatal period.18,19Furthermore, apparent branch PA narrowing was present in 59% of those corrected as neonates compared with 9% of the
remaining patients.19The Lecompte maneuver was reported to aggravate the branch PA stenosis either near the point of LPA or RPA origin, or at both.20,21Hemolysis or lethal sepsis from LPA stenosis has been reported.22,23
Preferential flow to the RPA has been well recognized in complete transposition of the great arteries, especially where there was a wide angle between the right border of the PT and the RPA.24,25However, this disparity in perfusion between the lungs is not present in
newborns with transposition. Once right lung flow increases, the right vascular bed grows more and there is a relative increase in vascular resistance and reduced compliance in the left lung, which further reduces left lung flow in diastole.24The apparent narrowing at the origin of the LPA is frequently seen and usually disappears during systole.26It has been mentioned that preferential flow has no significant effect on the natural history of untreated TGA.26
We propose modified arterial switch operation by spiral reconstruction.27,28We have even proved the functional implications of the spiral relationship of the great arteries by computational fluid dynamics.29The flow inside the spiral model is more streamlined than is the Lecompte model.
六、Self-Evaluation
The result of this one-year project revealed consistent with the original proposal. Investigators have demonstrated that the natural and second natural history of PA hypoplasia in TGA is about the same, namely, hemodynamic starvation and posterior inclination of PT would lead to PA hypoplasia in TGA both before and after surgical intervention. The surgical options that eliminate the-above-mentioned pathogenesis of PA hypoplasia like shunt with PT banding or Jatene with Lecompte (or had better with Pacifico or spiral reconstruction)
hopefully could facilitate PA growth in TGA.
七、References
1. Kirklin JW, Blackstone EH, Tchervenkov CI, Castaneda AR. Clinical outcomes after the arterial switch operation for transposition. Patient, support, procedural, and institutional risk factors. Circulation 1992;86:1501-15.
2. Serraf A, Lacour-Gayet F, Bruniaux J, Touchot A, Losay J, Comas J, Uva MS, Planche C. Anatomic correction of transposition of the great arteries in neonates. J Am Coll Cardiol 1993;22:193-200.
3. Kovalchin JP, Allen HD, Cassidy SC, Lev M, Bharatis. Pulmonary valve eccentricity in d-transposition of the great arteries and implication for the arterial switch operation. Am J Cardiol 1994;73:186-90.
4. Tanel RE, Wernovsky G, Landzberg MJ, Perry SB, Burke RP. Coronary artery
abnormalities detected at cardiac catheterization following the arterial switch operation for transposition of the great arteries. Am J Cardiol 1995;76:153-7.
5. Salzer-Muhar U, Proll E, Marx M, Salzer HR, Wimmer M. Two-dimensional and Doppler echocardiographic follow-up after the arterial switch operation for transposition of the great arteries. Thorac Cardiovasc Surg 1991;39:180-4.
6. Norwood WI, Dobell AR, Freed MD, Kirklin JW, Blackstone EH. Intermediate results of the arterial switch repair. A 20-institution study. J Thorac Cardiovasc Surg
7. Paillole C, Sidi D, Kachaner J, Planche C, Belot JP, Villain E, Le Bidois J, Piechaud JF, Pedroni E. Fate of pulmonary artery after anatomic correction of simple transposition of great arteries in newborn infants. Circulation 1988;78:870-6.
8. Yasui H, Yonenaga K, Kado H, Nakamura Y, Fusazaki N, Tsuruhara Y, Nakashima A, Tominaga R, Kawachi Y, Tokunaga K. Arterial switch operation for transposition of the great arteries: Surgical techniques to avoid complications. J Cardiovasc Surg
1992;33:511-7.
9. Krian A, Kramer HH, Quaegebeur J, Ostermeyer J. Korbmacher B, Godehardt E, Bircks W. The arterial switch-operation: Early and midterm (6 years) results with particular reference to technical problems. Thorac Cardiovasc Surg 1991;39:160-5.
10. Elkins RC, Knott-Craig CJ, Ahn JH. Ventricular function after the arterial switch operation for transposition of the great arteries. Ann Thorac Surg 1994;57:826-31. 11. AlexanderJA,KnaufDG,GreeneMA,van Mierop LHS,O‘Brien DJ.The changing
strategies in operation for transposition of the great vessels. Ann Thorac Surg 1994;58:1278-81.
12. Lupinetti FM, Bove EL, Minich LL, Snider AR, Callow LB, Meliones JN, Crowley DC, Beekman RH, Serwer G, Dick II M, Vermilion R, Rosenthal A. Intermediate-term survival and functional results after arterial repair for transposition of the great arteries. J Thorac Cardiovasc Surg 1992;103:421-7.
13. Aziz KU, Nanton MA, Kidd L, Moes CAF, Rowe RD. Variation in the size and distensibility of the pulmonary arteries in d-transposition of the great arteries. Am J Cardiol 1976;38:452-7.
14. Ruttenberg HD. Corrected transposition of the great arteries and splenic syndromes. In: Adams FH, Emmanouilides GC, Riemenschneider TA, editors. Heart disease in infants, children, and adolescents. Baltimore: Williams & Wilkins; 1989, p.424-42.
15. Imai Y. Double-switch operation for congenitally corrected transposition. Adv Cardiac Surg 1997;9:65-86.
16. Cochrane AD, Karl TR, Mee RB. Staged conversion to arterial switch for late failure of the systemic right ventricle. Ann Thorac Surg 1993;56:854-62.
17. Nakano H, Ueda K, Saito A. Beneficial preparatory aortopulmonary shunt for anatomical repair of transposition of the great arteries with intact ventricular septum. Ann Thorac Surg 1985;40:512-5.
18. Yacoub MH, Bernhard A, Radley-Smith R, Lange P, Sievers H, Heintzen P.
Supravalvular pulmonary stenosis after anatomic correction of transposition of the great arteries: Causes and prevention. Circulation 1982;66(suppl I):I-193-I-7.
19. Martin RP, Ladusans EJ, Parsons JM, Keck E, radley-Smith R, Yacoub MH. Incidence and site of pulmonary stenosis after anatomical correction of transposition of the great arteries. Br Heart J 1988;59:122-3.
20. Beek FJA, Beekman RP, Dillon EH, Mali WPTM, Meiners LC, Kramer PPG, Meyboom EJ. MRI of the pulmonary artery after arterial switch operation for transposition of the great arteries. Pediatr Radiol 1993;23:335-40.
21. Hardy CE, Helton GJ, Kondo C, Higgins SS, Young NJ, Higgins CB. Usefulness of magnetic resonance imaging for evaluating great-vessel anatomy after arterial switch operation for D-transposition of the great arteries. Am Heart J 1994;128:326-32. 22. Parsons MJ, Martin RP, Smith RR. Infective endarteritis affecting the left pulmonary
artery after anatomical correction of complete transposition of the great arteries. Br Hear J 1988;60:78-80.
23. Schroeder J, Albert J, Clarke D, Schaffer M, Wolfe R, Hays T. Hemolysis due to branch pulmonary stenosis after the arterial switch procedure. Ann Thorac Surg 1991;51:491-2. 24. Muster AJ, Paul MH, van Grondelle A, Conway JJ. Asymmetric distribution of the
pulmonary blood flow between the right and left lungs in d-transposition of the great arteries. Am J Cardiol 1976;38:352-361.
25. Vidne BA, Duszynski D, Subramanian S. Pulmonary blood flow distribution in transposition of the great arteries. Am J Cardiol 1976;38:62-6.
26. Kirklin JW, Barratt-Boyes BG. Complete transposition of the great arteries. In: Kirklin JW, Barratt-Boyes BG, eds. Cardiac Surgery. New York: Churchill Livingstone, 2nd ed, p1406.
27. Chiu IS, Wu SJ, Chen MR, Lee ML, Wu MH, Wang JK, Lue HC. Modified arterial switch operation by spiral reconstruction of the great arteries in transposition. Ann Thorac Surg 2000;69:1887-92.
28. Chiu IS, Wang JK, Wu MH. Spiral arterial switch operation in transposition of the great arteries. J Thorac Cardiovasc Surg 2002;124:1050-2.
29. Tang T, Chiu IS, Chen HC, Cheng KY, Chen SJ. Comparison of pulmonary arterial flow phenomena in spiral and Lecompte models by computational fluid dynamics. J Thorac Cardiovasc Surg 2001;122:529-34
八、Acknowledgement
This study was supported by a grant from the National Science Council
NSC93-2314-B-002-238. We are indebted to Misses Chang-Ying Lin and Ju-Hsiu Cheng for secretarial assistance.