Research Express@NCKU - Articles Digest
Research Express@NCKU Volume 21 Issue 10 - March 30, 2012 [ http://research.ncku.edu.tw/re/articles/e/20120330/3.html ]
A Dose-Ranging Study of the Efficacy and Tolerability of Entecavir in Lamivudine-Refractory Chronic
Hepatitis B Patients
Ting-Tsung Chang
Department of Medicine, College of Medicine, National Cheng Kung University [email protected]
Gastroenterology (2005), 129(4), 1198-1209
1. Introduction
Chronic hepatitis B infection affects more than 350 million people worldwide and lead to high morbidity and mortality due to the development of chronic liver disease, cirrhosis and HCC. In Taiwan, the prevalence of CHB is 15%~20% with ablout 3 million chronic HBV carriers. The high prevalence of CHB somehow arise intensive clinical trials of new drugs and therapies in Taiwan.
Two groups of CHB treatment have been practiced by physicians currently: interferons and nucleotide/nucleoside analogues (NAs). Although interferons lead to high HBeAg seroconversion rates, it is poorly tolerated and expensive. Lamivudine (LMV) is the first NA introduced and present high short-term efficacy. However, drug resistance develops after continuous treatment of LMV. It is principally associated with amino acid substitutions in the conserved tyrosine–methionine–aspartate- aspartate (YMDD) motif. LMV resistance occurs with the rebound in viral load, elevation of alanine aminotransferase (ALT) and increases the risk of liver diseases. The strategy toward LMV-resistant patients had been a dilemma. Long-term LMV therapy increased the occurring rate of resistance, but discontinuation of the therapy was associated with a significant increase in viral replication and flare of ALT levels. Thus, LMV therapy was often continued in LMV-refractory patients because viral loads may remain lower than pretreatment levels.
Entecavir (ETV) is a potent and highly selective inhibitor of HBV, and it has been reported to produce less drug resistance among several NAs introduced after LMV. The activity of ETV was initially addressed by animal models of viral hepatitis, and subsequently in NA naïve patients with CHB infection. Two phase II clinical trials showed the superior efficacy of ETV than LMV. In this multicenter and multinational clinical study, we aimed to assess the efficacy and safety of ETV versus continued LMV in patients with CHB who had documented LMV- associated mutations.
2. Results
We conducted a randomized and double-blind phaseII study. It is a dose-ranging trial comparing 3 doses of ETV monotherapy with continued LMV in adult LMV-refractory CHB patients. Patients enrolled in this study received 1.0, 0.5, and 0.1 mg ETV or 100 mg LMV daily for up to 76 weeks. Investigation of virologic and biochemical responses showed that the efficacy of ETV appeared with dose- and time-dependent manner (Fig.1, 2).
1 of 3
Research Express@NCKU - Articles Digest
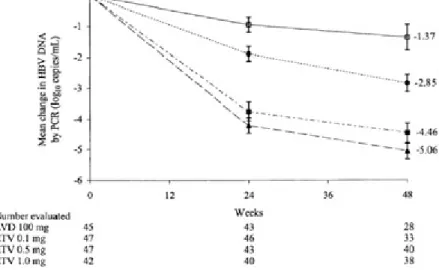
Figure 1. Mean change from baseline in Log10 HBV DNA levels by PCR assay through 48 weeks in patients treated with ETV 0.1 mg (closed circles), 0.5 mg (closed squares), 1.0 mg (closed triangles) or LMV 100 mg (open
squares). Error bars represent the SEM.
Virologic response was determined by bDNA assay after 24 weeks of study treatment (week-24), and a significant greater proportion of patients in the ETV 1.0 mg (79%) and 0.5 mg (51%) groups achieved low HBV DNA level (<0.7 MEq/ml by bDNA assay) compared with the LMV group (13%). At week-48, significant greater proportion of ETV 1.0 mg (26%) and ETV 0.5 mg (26%) groups achieved low HBV DNA by PCR assay (<400 copies/mL) compared with LMV group (4%), but no significant virologic response was observed in ETV 0.1 mg group.
Normalization of ALT levels indicating biochemical response was detected significantly more in all ETV groups than LMV groups by 48 weeks (Fig.2). Serologic response was also observed by determination of serum HBeAg and HBeAg antibody at week 48. However, among patients identified as HBeAg positive at baseline, no more than 11% of the patients in any treatment group lost HBeAg or achieve seroconversion. There were no significant differences in this parameter among all treatment groups.
Figure 2. Normalization of ALT levels through 48 weeks in patients with abnormal ALT levels at baseline treated with ETV 0.1 mg (closed circles), 0.5 mg (closed squares), or 0.1 mg (closed triangles) or LMV 100 mg (open
squares).
A complete response (undetectable HBV DNA levels by bDNA assay, normal ALT levels, and HBeAg negative) was achieved by significantly greater proportions of patients in the ETV 1.0 mg (29%) and 0.5 mg (19%) groups than in the LMV 100 mg (4%) group. Rare viral rebounds and drug resistances were observed in ETV 1.0 mg group through 48 weeks; the treatment was also well tolerated with safety profile similar to that of LMV. Based on
2 of 3
Research Express@NCKU - Articles Digest
these results, ETV treatment with dose of 1.0 mg was select to be used in subsequent phase III study. The efficacy of ETV and the impact of drug resistance over longer period would be investigated in the larger phase III study.
In conclusion, ETV treatment for up to 79 weeks had reduced viral load, normalized serum ALT levels in majority of patients who had previously failed to respond to LMV therapy. Of the three doses used in this trial, ETV 1.0 mg daily showed the most profound and consistent antiviral activity with good tolerability. Therefore, ETV therapy (with dose of 1.0 mg) was then considered as one appropriate therapy for LMV-refractory CHB infection.
3 of 3