國立臺灣大學公共衛生學院流行病學與預防醫學研究所 碩士論文
Graduate Institute of Epidemiology and Preventive Medicine College of Public Health
National Taiwan University Master Thesis
以系統性回顧與網絡統合分析比較阻力訓練、
耐力訓練與全身震動系統於治療老年人肌少症之成效 Comparative Effectiveness Analysis of
Resistance Training, Endurance Training and Whole Body Vibration in Treating Sarcopenia in Elderly:
Systematic Review and Network Meta-Analysis
賴芝錦 Chih-Chin Lai
指導教授:簡國龍 博士 Advisor: Kuo-Liong Chien, Ph.D.
中華民國 105 年 7 月 July, 2016
國立臺灣大學碩士學位論文
口試委員會審定書
論文中文題目:以系統性回顧與網絡統合分析比 較阻力訓練、耐力訓練與全身震動系統於治療老 年人肌少症之成效
論文英文題目:Comparative Effectiveness Analysis of Resistance Training, Endurance Training and Whole Body Vibration in Treating Sarcopenia in Elderly: Systematic Review and Network Meta-Analysis
本論文係賴芝錦君(R03849040)在國立臺灣大學流行病
學與預防醫學研究所完成之碩士學位論文,於民國 105 年 6 月
24 日承下列考試委員審查通過及口試及格,特此證明
誌謝
首先誠摯的感謝指導教授簡國龍博士,老師悉心的教導使我得以了解流行病學與 預防醫學領域的深奧,不時的討論並指點我正確的方向,使我在這兩年中獲益匪 淺。在簡老師的課堂與group meeting中,我不只累積學問知識,更深深感受到老 師對做學問的熱情,老師對研究的嚴謹更是我學習的典範。本論文的完成亦得感 謝台大醫院復健部王亭貴主任,在過程中給我中肯的建議,使得本論文能夠更完 整與嚴謹。而在撰寫論文時遇到研究方法上的困難,我很感謝杜裕康老師不厭其 煩的給我統計分析方法上的協助與指導,還有從碩一就很關心我的程蘊菁老師,
雖然兩位都不是我的指導老師,但老師們卻從不吝惜給我幫助。也非常感謝擔任 口試委員的簡盟月老師,謝謝老師不吝賜教,幫助我的論文更臻完善。感謝台大 醫院物理治療技術科的同事們,在我請公假念書期間,在工作上給予協助。感謝 實驗室的學長姊們,在研讀期間,給予諸多意見,提供熱心的幫助與經驗分享。
在台大流預所求學的這兩年,一路上受到所有老師們的照顧,學生我將會永銘於 心,謝謝季瑋珠老師、李永凌老師、林先和老師、張淑惠老師、方啟泰老師,還 有上述已提到的簡國龍老師、程蘊菁老師、杜裕康老師,在老師們的課堂中除了 知識的積累,更獲得做研究的動力,激發我去學習那些完全陌生的學問,謝謝老 師們對我的關愛與照顧。我所上過所有課的老師們,雖然因篇幅有限並未一一提 及,但我同樣感謝。
最後,謹以此文獻給我摯愛的雙親。
中文摘要
背景與目標:肌少症是因年齡增加導致的肌肉質量減少、肌肉力量衰退與身體活
動功能限制的疾病。若特別針對肌少症的三項診斷指標:肌肉質量、肌力與身體
活動功能表現,目前仍缺乏各種運動療效之間的比較文獻。本篇研究的目的即採
用系統性回顧與網絡統合分析,比較阻力訓練、耐力訓練與全身震動系統於治療
老年人肌少症之成效。
方法:收集並分析阻力訓練、耐力訓練與全身震動系統的隨機對照試驗,摘錄其
中訓練前與訓練後之肌肉質量、肌力與身體活動功能之數據,對象為六十歲以上
的老人。以廣義線性混合模型進行網絡統合分析,並以直接證據與間接證據呈現
混合治療型比較之結果。
結果:共收錄 31 篇隨機對照試驗,1405 名六十歲以上老人被收錄(年齡介於 60
歲與 92 歲)。肌力在阻力訓練組與無運動介入組之間達到顯著差異,經由阻力訓
練後的肌力較無運動組別增加 12.8 公斤 (95% 信賴區間 8.54 至 17.0 公斤)。身
體活動功能則在阻力訓練組與無運動介入組、全身震動系統與無運動介入組達到
顯著差異[平均值分別是 2.63 次 (95% 信賴區間 1.34 至 3.93 次) 與 2.07 次
(95% 信賴區間 0.49 至 3.65 次)]。但肌肉質量在各組的直接比較或間接比較皆無
顯著差異。
結論:若使用肌少症的診斷指標來評估老人的運動效益,阻力訓練可顯著增加老
人的肌力與身體活動功能,而全身震動系統可顯著改善老人的身體活動功能。但
研究結果卻顯示三種運動介入方式無法顯著增加肌肉質量。
關鍵字:肌少症、阻力訓練、耐力訓練、全身震動系統、系統性回顧、網絡統合
分析。
英文摘要
Background and Objectives: Sarcopenia is an age-related loss of muscle mass,
muscle strength, and physical performance. Few studies have examined the relative
benefits of resistance training, endurance training, and whole-body vibration through
the simultaneous consideration of three diagnostic criteria: muscle mass, muscle
strength, and physical performance. The purpose of this systemic review and network
meta-analysis was to analyze the effects of resistance training, endurance training, and
whole-body vibration on changes in muscle mass, muscle strength, and physical
performance through the evaluation of lean body mass, leg extension strength, and
chair-stand tests in elderly people.
Methods: We combined evidence from all randomized controlled trials comparing
resistance training, endurance training, and whole-body vibration with usual care
among adults aged at least 60 years. The effects of exercises and usual care on muscle
mass, muscle strength, and physical performance were examined. We performed a
mixed treatment comparison by using generalized linear mixed models for the
network meta-analysis.
Results: Thirty-one randomized controlled trials involving 1405 participants were
included (age range, 60–92 years). Muscle strength enhancement was greater for
resistance training compared with usual care [12.8 (95% CI 8.54 to 17.0)]. Physical
performance enhancement was greater for resistance training compared with usual
care, and whole-body vibration was greater compared with usual care [2.63 (95% CI
1.34 to 3.93), and 2.07 (95% CI 0.49 to 3.65)]. No significant difference was observed
regarding changes in lean body mass.
Conclusion: Resistance training is beneficial for elderly people with outcome
indicators of sarcopenia; specifically, it enhances muscle strength and physical
performance. Resistance training and whole-body vibration were the two most
effective exercise interventions in terms of physical performance. However, no
statistically significant results were observed for resistance training, endurance
training, and whole-body vibration concerning increases in muscle mass.
Keywords: sarcopenia, resistance training, endurance training, whole body vibration,
systemic review, network meta-analysis.
目 錄 Table of Contents
口試委員會審定書 ... II
誌謝 ... III
中文摘要 ... IV
英文摘要 ... VI
INTRODUCTION ... 1
1.1 Sarcopenia ... 1
1.1.1 Definition, prevalence and causes of sarcopenia ... 1
1.1.2 Consequences of sarcopenia ... 3
1.1.3 Interventions of sarcopenia ... 4
1.2 Resistance training ... 5
1.3 Endurance training ... 6
1.4 Whole body vibration... 7
1.5 Review of three exercises ... 9
1.5.1 Resistance training ... 9
1.5.2 Endurance training ... 10
1.5.3 Whole body vibration... 11
STUDY GAP ... 13
MATERIALS AND METHODS ... 14
3.1 Identification of studies ... 14
3.2 Selection of sample studies ... 14
3.3 Data extraction and bias assessment ... 16
3.4 Data synthesis and analysis ... 17
3.4.1 Relative treatment effects... 17
3.4.2 Methods for direct and indirect comparisons ... 18
3.4.3 Relative treatment ranking ... 19
3.4.4 Statistical heterogeneity and inconsistency ... 20
RESULTS ... 21
4.1 Muscle mass: Lean body mass ... 23
4.2 Muscle strength: Leg extension strength ... 24
4.3 Physical performance: chair-stand test ... 25
4.4 Publication bias ... 26
4.5 Statistical heterogeneity and Inconsistency ... 27
DISCUSSION ... 28
5.1 Comparison with previous studies ... 28
5.1.1 Muscle mass ... 28
5.1.2 Muscle strength ... 29
5.1.3 Physical performance ... 30
5.2 Preservation of muscle mass and improvement of muscle strength ... 31
5.3 Improvement of muscle strength and physical performance .. 31
5.4 Improvement of muscle strength in the elderly with heart disease ... 32
5.5 Estimation the benefits of endurance training on physical performance ... 33
5.6 Public health issue and clinical implication ... 34
5.7 Strength and limitation ... 35
5.8 Direction of future research ... 35
CONCLUSION ... 37
REFERENCES ... 38
Figures
Figure 1. Scheme of the different etiological sarcopenia mechanism and their
consequences [1, 10] ... 52
Figure 2. Flowchart of network meta-analysis ... 55
Figure 3. Risk of bias summary: assessments for studies in a Cochrane review of resistance training, endurance training and whole body vibration ... 56
Figure 4. Risk of bias graph: assessments for studies in a Cochrane review of
resistance training, endurance training and whole body vibration ... 57
Figure 5 Traditional meta-analysis of the effects of the effects of resistance training (RT) and usual care (CON) on muscle mass (A), muscle strength (B) and
physical performance (C) ... 65
Figure 6. Summary of network geometry of muscle mass (A), muscle strength (B) and physical performance (C) ... 66
Figure 7. Network meta-analysis of the effects of usual care (CON), resistance
training (RT), endurance training (ET) and whole body vibration (WBV) on lean body mass... 67
Figure 8. Network meta-analysis of the effects of usual care (CON), resistance training (RT), endurance training (ET) and whole body vibration (WBV) on leg extension strength ... 68
Figure 9. Network meta-analysis of the effects of usual care (CON), resistance
training (RT), endurance training (ET) and whole body vibration (WBV) on chair stand test... 69
Figure 10. Begg's funnel plots of the effects of usual care (CON), resistance training (RT), endurance training (ET) and whole body vibration (WBV) on lean body mass, leg extension strength, and chair-stand test among older adults ... 70
(A) Lean body mass, (B) leg extension strength, (C) chair-stand test ... 70
Figure 11. Egger's regression of the effects of usual care (CON), resistance training (RT), endurance training (ET) and whole body vibration (WBV) on lean body mass (A), leg extension strength (B), and chair-stand test (C) among older adults ... 71
Figure 12. Rankogram of the effects of usual care (CON), resistance training (RT), endurance training (ET) and whole body vibration (WBV) on lean body mass (A), leg extension strength (B), and chair-stand test (C) among older adults... 72
Figure 13. Histogram with percentage bins of the relative ranking probabilities for usual care (CON), resistance training (RT), endurance training (ET) and whole body vibration (WBV) on muscle mass(A), muscle strength (B), and physical performance (C) among older adults ... 73
Tables
Table 1. Summary of meta-analysis of studies on muscle mass, muscle strength and physical performance ... 53
Table 2. Description of the study participants and the interventions of resistance training ... 58
Table 3. Description of the study participants and the interventions of resistance training and endurance training ... 63
Table 4. Description of the study participants and the interventions of whole body vibration training (WBV) ... 64
Table 5. Network meta-analysis of pairwise comparisons: mean change from baseline in lean body mass, leg extension strength and chair-stand test ... 74
Table 6. Subgroup analysis: network meta-analysis of pairwise comparisons of leg extension strength for knee extension machines and leg press machine ... 75
Table 7. Network meta-analysis of pairwise comparisons: mean change from baseline in chair-stand test with Davidson’s study [106] ... 76
Introduction
1.1 Sarcopenia
1.1.1 Definition, prevalence and causes of sarcopenia
According to the clinical definition and consensus on diagnostic criteria for
sarcopenia specified by the European Working Group on Sarcopenia in Older People
(EWGSOP), sarcopenia is defined as an aging-associated condition involving a
progressive decline in skeletal muscle mass, resulting in the deterioration of muscle
function (muscle strength and physical activity) [1].
The prevalence of sarcopenia has increased with the rapid growth in the number and
proportion of elderly people. According to the United Nations World Population
Aging 2013, the proportion of the world population aged at least 60 years is projected
to increase from 12% in 2013 to 21% in 2050. People aged at least 60 years in the
2010–2015 period are expected to live an additional 20 years [2]. The overall
prevalence of sarcopenia was estimated to be 5%–13% for elderly people aged 60–70
years in Europe and the United States [3]. The prevalence of sarcopenia in Taiwan
was found to be 18.6% for elderly women and 23.6% for elderly men [4].
Sarcopenia is an age-related condition that leads to a 1%–2% reduction in skeletal
muscle mass for both men and women over the age of 50 [5]. A reduction in muscle
mass and strength in elderly people is caused by the etiologies of sarcopenia. As
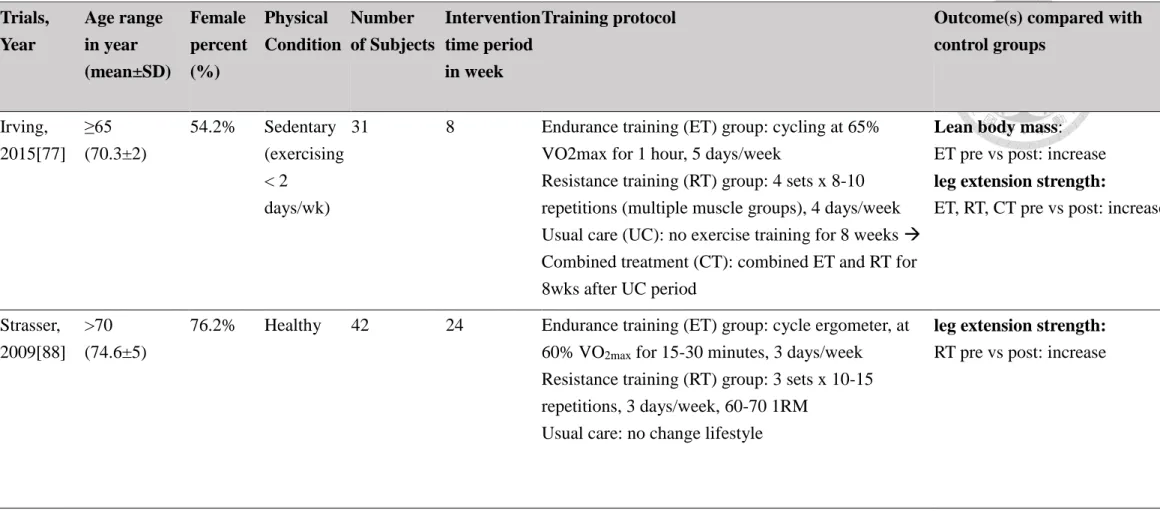
shown in Figure 1, sarcopenia is a multifactorial process in which aging is the major
cause [6]. Primary sarcopenia is caused only by age-related factors such as a reduction
in sex hormones, apoptosis, mitochondrial dysfunction, satellite cell dysfunction, and
motor neuron loss. Cachexia and vitamin D deficiency contribute to sarcopenia. In
addition, sarcopenia is associated with disease states such as neurodegenerative
diseases, advanced organ failure, inflammation diseases, malignancies, and endocrine
diseases.
Most endocrine diseases, such as diabetes, hypogonadism, and hypercortisolism, as
well as obesity and chronic kidney disease are associated with age-related muscle loss
[7, 8]. Seven factors are related to loss of muscle mass and strength: humoral, genetic,
nervous system, hormonal, nutritional, insulin resistance, and lifestyle. Lifestyle
factors consist of sedentary lifestyles, high-fat diets, obesity, smoking, and
immobility. Lifestyle factors are more controllable than the other six factors;
therefore, they have attracted public attention for the prevention of sarcopenia [1, 9,
10].
1.1.2 Consequences of sarcopenia
Public health concerns of sarcopenia include higher healthcare costs, diminished
quality of life, and mortality [11]. Age- and disease-related muscle loss and
comorbidities among elderly people lead to poorer health conditions, suggesting
longer periods of hospitalization. Comorbidities of sarcopenia include cognitive
decline, cerebrovascular disease, insulin resistance, chronic kidney disease stage
three, and osteoporosis at the femur neck in elderly men [7, 12]. Regarding medical
procedures, sarcopenia is associated with high costs and poor outcomes after major
surgery [13]. Higher mortality is strongly correlated with sarcopenia after liver
transplantation [14]. Sarcopenia in an overweight or obese patient is an adverse
prognostic factor in pancreatic cancer [15].
Muscle weakness in the lower extremities (quadriceps, iliopsoas, tibialis anterior or
posterior peroneus, and hip or knee) increases the risk for falling in elderly people
[16]. A study reported that among elderly women who had fallen in the past year,
women who exhibited prolonged chair-rise time (time to stand up from a sitting
position) were three times as likely to have a serious injury as were those with shorter
chair-rise time [17]. Compared with those without sarcopenia, participants with
sarcopenia had a significantly higher number of falls and fractures [18]. Falls threaten
the independence of elderly people and account for many hospital and nursing home
admissions. Functional ability is significantly reduced at 1 year after initial
presentation to the emergency department because of a fall [19].
Lower muscle mass, greater fat infiltration into the muscle, and lower knee extensor
muscle strength are associated with increased risk of mobility loss in elderly men and
women [20]. Severe sarcopenia is a risk factor for the development of physical
disabilities, and consequently, disability is associated with increased hospitalization,
nursing home placement, home health care, and health care expenditure [11, 21]. In
the United States, the estimated direct health care cost attributable to sarcopenia in
2000 was $18.5 billion ($11.8 - $26.2 billion) [22].
1.1.3 Interventions of sarcopenia
Resistance training is a form of physical activity that is designed to improve muscular
fitness by exercising a muscle or a muscle group against external resistance [23].
Pharmacological interventions have shown limited efficacy in counteracting skeletal
muscle wasting resulting from sarcopenia; therefore, exercise interventions represent
a critical approach for preventing and treating sarcopenia [24, 25].
1.2 Resistance training
Resistance training is a form of physical activity that is designed to improve muscular
fitness by exercising a muscle or a muscle group against external resistance [26]. The
American College of Sports Medicine (ACSM) recommends that resistance training
should be performed a minimum of 2–3 days per week. The resistance training
intensity and number of repetitions performed in each set are inversely related.
Elderly and deconditioned people who are susceptible to musculotendinous injury
should begin a resistance training program by conducting a high number of repetitions
at moderate and light intensities. Moderate intensity signifies a 60%–70% repetition
maximum (1-RM). Light intensity signifies 40%–50% of 1-RM. When 1-RM is not
measured, moderate (5–6) and vigorous (7–8) intensity can be distinguished
according to a 10-point scale for rating perceived exertion (RPE). With 1-RM and
RPE measurements, people can calculate quantitative volume while maintaining an
appropriate lifting technique. Repetitions of resistance training can be defined as
follows: one set of 8–12 repetitions for healthy adults or 10–15 repetitions for middle-
aged and elderly people. No specific duration of training has been identified for
effectiveness. For general muscular fitness, a person should perform resistance
training for each major muscle group (i.e., chest, shoulders, upper and lower back,
abdomen, hips, and legs). A total of 8–10 exercises targeting the major muscle groups
should be performed. Typical resistance exercises for major muscle groups can be
performed using body weight or a variety of exercise equipment such as sand bags
and resistance bands. Resistance training causes neural adaptation because of an
increase in motor unit synchronization, concentric contraction of synergist muscles,
and increased inhibition of antagonist muscles.
1.3 Endurance training
Endurance training has been called aerobic training and cardiorespiratory endurance
exercise [26]. Rhythmic, aerobic exercise of at least moderate intensity involving
large muscle groups and requiring little skill to perform is recommended for all adults.
For example, walking, leisurely cycling, aqua-aerobics, and slow dancing are
recommended modes of endurance training for all adults. The ACSM recommends
any modality that does not impose excessive orthopedic stress, such as walking,
which is the most common type of activity. For elderly people with a limited tolerance
for weight-bearing activities, aquatic exercise and stationary cycle exercise may be
advantageous. The ACSM recommends an endurance training intensity of 40%–60%
heart rate reserve (%HRR), 3–6 metabolic equivalents (MET), and a 5–6 rating of
perceived exertion (RPE) to moderate intensity for elderly people. Moderate aerobic
exercise is recommended for most adults, and light to moderate intensity aerobic
exercise can be beneficial for deconditioned people. Endurance training is
recommended 3–5 days per week for most adults, with the frequency varying with the
intensity of exercises. For moderate-intensity exercises, an accumulated 30–60 min
per day in periods of at least 10 min each for a total of 150–300 min per week is
recommended.
Endurance training can enhance maximal voluntary contraction in isometric knee
extension in elderly people. For elderly people, endurance training increases the
cross-sectional area of both type I and type II muscle fibers by 12% and 10%,
respectively. When the number of capillaries in contact with each fiber increases,
endurance training programs result in a 23% increase in maximal O2 consumption
[27].
1.4 Whole body vibration
Whole-body vibration has recently been proposed as a mild approach to improve
neuromuscular performance. Whole-body vibration is an oscillatory motion delivered
to the entire body from a platform. Oscillatory motion is a mechanical stimulus
characterized by a lineal pivotal platform, depending on the type of equipment. The
intensity of oscillation is set at biomechanical variables of frequency and amplitude.
The extent of the oscillatory motion reflects the amplitude (measured in millimeters)
of the vibration. The repetition rate of the cycles of vibration per second reflects the
frequency of the vibration (measured in hertz) [28]. The frequencies of vibration
studied in elderly people have varied from 12.6 to 60 Hz, with reported amplitudes
varying from 55 μm to 8 mm [29]. In elderly people with fragile musculoskeletal
systems, amplitudes >0.5 mm have been reported to have greater effects on the body,
causing discomfort [30]. A review of Rittweger [31] revealed that vibration
frequencies ranging between 20 and 45 Hz shows adaptive neuromuscular effects.
However, Rittweger reported that at frequencies above 50 Hz, severe muscle soreness
and hematoma may emerge in untrained subjects [32]. Low-intensity whole-body
vibration can induce muscle activity as effectively as higher-intensity protocols do,
and it may thus be the preferred choice for frail elderly people [33].
Vibration-induced enhancements in muscular performance have been suggested to be
similar to those after several weeks of power training [34]. Standing on oscillating
platforms induces an enhanced refectory response of the leg and postural muscles
through the so-called “tonic vibration reflex” [35]. Tonic vibration reflex is a
mechanical vibration that induces the stretch reflex of muscle spindles and activates I-
α afferents, which initiates impulses in the polysynaptic excitatory pathway, causing
tonic contraction of the muscle. Skin mechanoreceptors such as Pacinian corpuscles
activate muscle spindles and induce a flexion reflex during vibration stimulation. This
causes wider spreading effects compared with those of the tonic vibration reflex and
evoked muscle contractions [36].
1.5 Review of three exercises
1.5.1 Resistance training
Recent studies have suggested that physical activity and exercises such as resistance
training can be used to slow down the progression of sarcopenia effectively [37-39].
Charette reported an increase in the cross-sectional area of type II muscle fibers, but
not type I fibers, after a 12-week resistance training program. High-intensity exercises
are necessary for the development of type II muscle fibers. However, elderly people
typically have a reduced frequency of high-intensity activities, which leads to type II
muscle fiber-selective atrophy, but the preservation of type I muscle fibers. Therefore,
high-intensity exercise (e.g., resistance training) can increase muscle mass [40]. In
Peterson’s meta-analysis on resistance training designed for elderly people [41], 49
randomized and nonrandomized controlled trials were analyzed. Trials were included
if the mean age of participants was over 50 years. Results revealed that muscle mass
was effectively increased because of the resistance training protocol. The weighted
pooled estimate of the mean change in lean body mass was 1.1 kg (95%CI 0.9–1.2).
Kelley’s meta-analysis involved two randomized controlled trials and six
nonrandomized controlled trials to determine the effects of resistance training in 225
men aged 18–70 [42]. Compared with the control group, lean body mass increase was
reported to be statistically significant in men conducting resistance training (weighted
mean difference 0.3 kg (95%CI -0.2–0.6). However, three randomized controlled
trials involving 143 premenopausal women aged 18–47 were included in another
meta-analysis by Kelley [43]. Results showed no statistically significant difference in
muscle mass within or between the resistance training groups and control groups. In a
meta-analysis by Silva [44], 15 randomized controlled trials involving 528
participants aged 66 years or older were conducted. Muscle strength was significantly
enhanced in the resistance training group compared with the control group (weighted
mean difference 23.1%, 95% CI 15.4–30.8).
1.5.2 Endurance training
Endurance training has been considered minimally effective on muscle mass and
muscle strength, but moderately effective on aerobic capacity. However, a review by
Konopka indicated that endurance training increased muscle hypertrophy by
improving muscle molecular regulation and protein metabolism. In sedentary men and
women, muscle and myofiber size increased after endurance training [45]. Endurance
training changed the muscle fiber distribution. In patients with chronic heart failure, a
regular bicycle exercise improved exercise tolerance, which was associated with a
shift in fiber type distribution from fast-twitch type II fibers to slow-twitch type I
fibers [46].
1.5.3 Whole body vibration
Osawa conducted a meta-analysis comprising 10 studies to determine the effects of
whole-body vibration on knee extension muscle strength. Data collected from four
trials that included elderly people showed a significant increase in knee extensor
muscle strength for exercises in the whole-body vibration group [47]. Sitjà-Rabert
performed a meta-analysis to evaluate the efficacy of whole-body vibration in an
elderly population compared with conventional exercise in control groups. A total of
16 randomized controlled trials were pooled, which indicated that whole-body
vibration significantly enhanced muscle strength (weighted mean difference 18.3
newton meters [95%CI 8.0-28.6])[48].
Recent evidence from systemic reviews and meta-analyses shows that resistance
training, endurance training, and whole-body vibration are crucial for increasing
muscle mass and muscle strength and improving physical performance. However,
because of limitations in traditional meta-analysis, evidence regarding comparisons of
different types of exercise intervention is insufficient. Recent studies have not
identified the most effective option for mitigating the indicators of sarcopenia.
Study gap
When considering the diagnostic criteria of sarcopenia (muscle mass, muscle strength,
and physical performance), it is difficult to conduct a well-designed randomized
controlled trial for all competing exercise interventions. Furthermore, traditional
meta-analysis was used in the comparison of two arms (i.e., one intervention group
compared with one control group). The disadvantage of traditional meta-analysis is
that multiple interventions are tested according to difficulties; traditional analysis does
not enable adequate assessment of the comparative effectiveness of all exercise
interventions. To mitigate the multi-arm analysis problem, a network meta-analysis
was conducted to compare direct and indirect evidence.
In this study, we conducted a network meta-analysis to synthesize direct and indirect
evidence and estimate the relative efficacy between a pair of exercise interventions.
After the rank and the effect of interventions are determined, the exercise can become
a nonpharmacological intervention strategy for preventing sarcopenia in elderly
people.
Materials and methods
3.1 Identification of studies
We searched the databases in MEDLINE, EMBASE, Cochrane Central Register of
Controlled Trials (CENTRAL), the Physiotherapy Evidence Database (PEDro) using
the keywords including sarcopenia, physical activity, muscle atrophy, resistance
training, endurance training, whole body vibration, lean body mass, body
composition, body fat distribution , and muscle strength or physical performance or
other related terms. We limited the search to English language studies. We conducted
a literature search to identify relevant studies published from 1989 until 15 February
2016. The term 'sarcopenia' was proposed by Irwin Rosenberg in 1989 [49].
3.2 Selection of sample studies
Systemic reviews and meta-analyses were followed by the PRISMA (Preferred
Reporting Items for Systemic Reviews and Meta-analyses) guidelines, and used a
predetermined protocol. To be included in this study for higher quality, the studies
should be designed as randomized control trials involving the comparison between the
intervention of resistance training, endurance training, whole body vibration and the
usual-care control group in elderly people (average age ≥ 60 years). In addition, the
inclusion criteria should be met by including at least one of the three following data
results: muscle mass, muscle strength and physical performance. The muscle mass,
muscle strength and physical performance refer to lean body mass, leg extension
strength, chair-stand test, respectively.
The intervention protocols of resistance trainings are classified in accordance with the
American College of Sports Medicine (ACSM). The resistance trainings for the
elderly is a dynamic exercise performed by multi-joint use. In the resistance training
protocol for the elderly to perform a complete movement of a given exercise, the
duration of each exercise is set as a range of approximately 20–45 minutes per session
and no less than 20 minutes, the intensity is at least 60% one-repetition maximum
(1RM), and the repetition requires at least 10 times[26].
The National Institute on Aging (NIA) recommend older adult’s progress to at least 30
minutes of moderate to vigorous endurance exercises. The 30-minute goal can
accomplished by accumulating time in shortening sessions of at least 10 minutes
each[50]. ACSM recommends accumulating 20-60 minutes at that level three to five
days a week[26].
Whole body vibration system was characterized oscillatory motion delivered to the
entire body from a platform. The biomechanical variables that determine its intensity
are the frequency and amplitude. The extent of the oscillatory motion determines the
amplitude (peak to peak displacement, in mm) of the vibration. The repetition rate of
the cycles of oscillation determines the frequency of the vibration (measured in
Hz)[28].
The usual-care control group was used in comparison with the resistance trainings
group, endurance training group and whole body vibration group. In the usual-care
control group, the trials incorporating a placebo-based intervention are also included
(education, stretching, etc.).
3.3 Data extraction and bias assessment
The muscle mass is categorized as the primary outcome while the muscle strength and
physical performance are secondary outcome. The primary outcome is the change of
lean body mass that can be assessed by the imaging techniques (CT, MRI, dual energy
x-ray absorptiometry (DXA)), bio-impedance analysis and anthropometric
measurement. The secondary outcomes are the evaluation of the muscle strength by
the leg extension strength [51], and the physical performance on the chair-stand test
[52]. Maximal concentric leg extension strength is assessed by one-repetition
maximum test (1RM) [51]. Chair-stand test was chosen to evaluate the physical
performance for the muscular strength and endurance in the elderly’s legs [52]. The
participants were instructed to perform a sit-to-stand by rising to a full stand from a
complete sitting position, repeated as many times as possible within 30 seconds, and
the total number of times was counted.
The data are extracted from the same independent extractor from full-text articles. The
publication bias is assessed with funnel plots and egger’s test of effect size (mean
difference) against its standard error. The risk of potential bias assessments is
conducted by Cochrane Collaboration's tool[53]. By using the Cochrane Risk of Bias
Tool, studies were classified as being at low risk, at high risk or unclear. This study is
not funded or sponsored by any special interest.
3.4 Data synthesis and analysis
3.4.1 Relative treatment effects
The primary and secondary outcomes are represented as the mean change from
baseline in lean body mass (kilogram), leg extension strength (kilogram) and chair-
stand performance (frequency), respectively. All the outcomes are continuous
variables. Because of not only different sample of participants but differences in the
way studies were conducted, random effect model was conducted for pairwise meta-
analysis comparisons from trials with the same interventions (i.e. resistance training
vs. usual care, resistance training vs. endurance training, endurance training vs. whole
body vibration and so on). We estimated the pairwise relative treatment effects of the
competing interventions using weighted mean differences for outcomes (lean body
mass, leg extension strength and chair stand test) and the mean difference with 95%
confidential intervals (CI). Change of standard deviation was calculated using the
formula [54, 55]:
𝐶ℎ𝑎𝑛𝑔𝑒 𝑜𝑓 𝑠𝑡𝑎𝑛𝑑𝑎𝑟𝑑 𝑑𝑒𝑣𝑖𝑎𝑡𝑖𝑜𝑛 (𝑆𝐷)
= √𝑆𝐷𝑝𝑟𝑒2+ 𝑆𝐷𝑝𝑜𝑠𝑡2 − 2 × 𝐶𝑜𝑟𝑟(𝑝𝑟𝑒, 𝑝𝑜𝑠𝑡) × 𝑆𝐷𝑝𝑟𝑒 × 𝑆𝐷𝑝𝑜𝑠𝑡
Within-participant correlation was imputed 0.5 if correlation was not reported. All
tests were two-tailed and a p value of less than 0.05 was determined statistically
significant. The heterogeneity was estimated by restricted maximum likelihood. The
data were analyzed with Stata version 14 (StataCorp LP, Texas, USA).
3.4.2 Methods for direct and indirect comparisons
We performed a mixed treatment comparison using generalized linear mixed models
for network meta-analysis to analyze direct and indirect comparisons of different
exercise interventions. For example, for conducting the direct comparison of
resistance training and endurance training, direct evidence is provided by trials
directly comparing these two exercise training. For conducting the indirect
comparisons of resistance training and endurance training, each has been compared
with a common comparator, say usual care, indirect evidence is based on the direct
comparison of resistance training and usual care and the direct comparison of
endurance training and usual care. We performed network meta-analysis in Stata
using the mvmeta command and self-programmed. The between-study variance can
be estimated using restricted maximum likelihood method and DerSimonian-Laird
method [56].
3.4.3 Relative treatment ranking
The relative ranking probabilities for four arms were estimated by using “network
rank max” command. Rankogram of the effects of usual care, resistance training,
endurance training and whole body vibration on lean body mass, leg extension
strength and chair-stand test were used for showing the hierarchy of the competing
interventions. The surface under the cumulative ranking curve (SUCRA) is a
percentage of the mean rank of each treatment relative to an imaginary treatment that
is the best without uncertainty. The larger area under the curve, the better the rank of
the exercise intervention [57].
3.4.4 Statistical heterogeneity and inconsistency
Heterogeneity refers to between-study variance within a comparison[58]. For the
pairwise comparisons (i.e. direct comparisons), statistical heterogeneity was assessing
by the forest plot, I-squared and its 95% confidence interval.
Inconsistency refers to differences between direct and indirect evidence in the
network [58]. For the network comparison, loop-specific approach and“node-
splitting” method were conducted to assess inconsistency locally. Design-by-
treatment model was conducted to evaluate inconsistency globally
Results
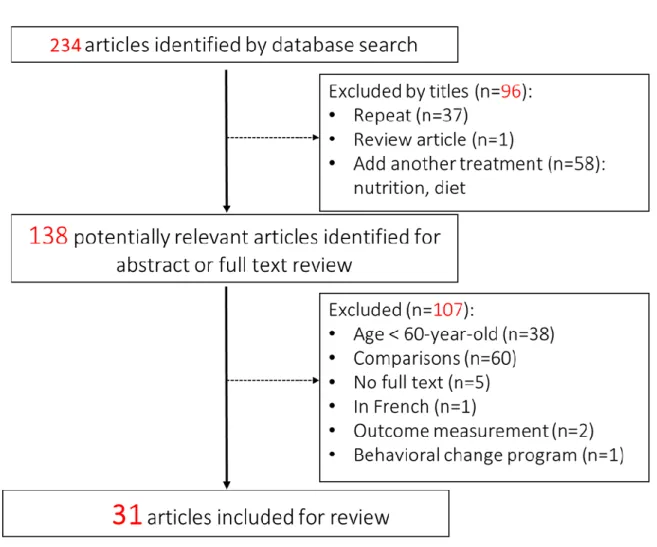
The PRISMA flow chart of the included trials and the assessment of the risk of bias of
the included randomized control trials are given in figure 2, 3 and 4. Figure 2 outlines
the searching strategy, identifying 234 publications. The titles and abstracts were
screened for inclusion. The full texts of 138 articles were retrieved, of which 31 met
the inclusion criteria. One-hundred seven were excluded: 38 studies were participants
for the age only 60 years or younger, 1 was not written in English, 2 did not
incorporate the primary and secondary outcomes, and 60 did not use usual-care
control group or other exercise interventions for comparison.
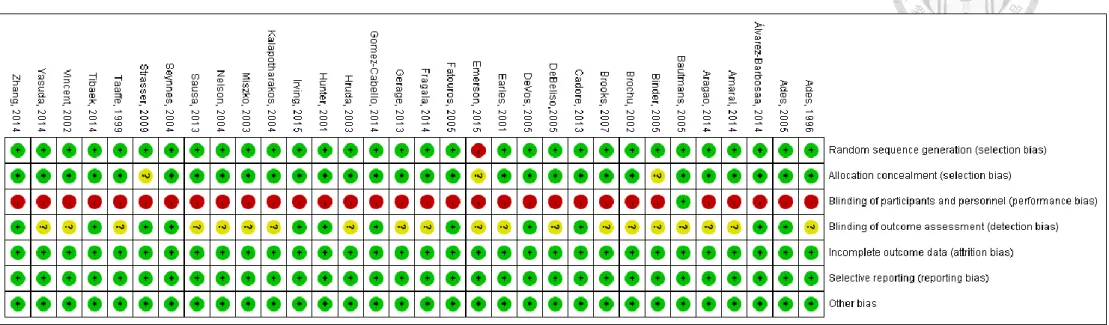
The findings with respect to random sequence generation, allocation concealment,
blinding of participants, personnel and outcome measurement, completeness of
outcome data and slective reporting were demonstreated on figure 3 and 4. Most
studies were low risk of concealment of allocation, blinding of particants and
personnel, incomplete outcomes data and selective reporting. All studies were rated
low risk of bias of random seqence generation exept for Emerson’s study [59], in
which group randomization was based upon the participant's availability and
willingness to attend the training sessions. Many trials did not address insufficient
information of blinding of outcome assessment were rated “unclear risk of bias”.
Because of the characteristics of intervention study, no study blinded participants and
personnels to the intervention exept for Bautmans’ study [60], in this study usual care
group standed on identical whole body system with intervention group but with
switched-off plates.
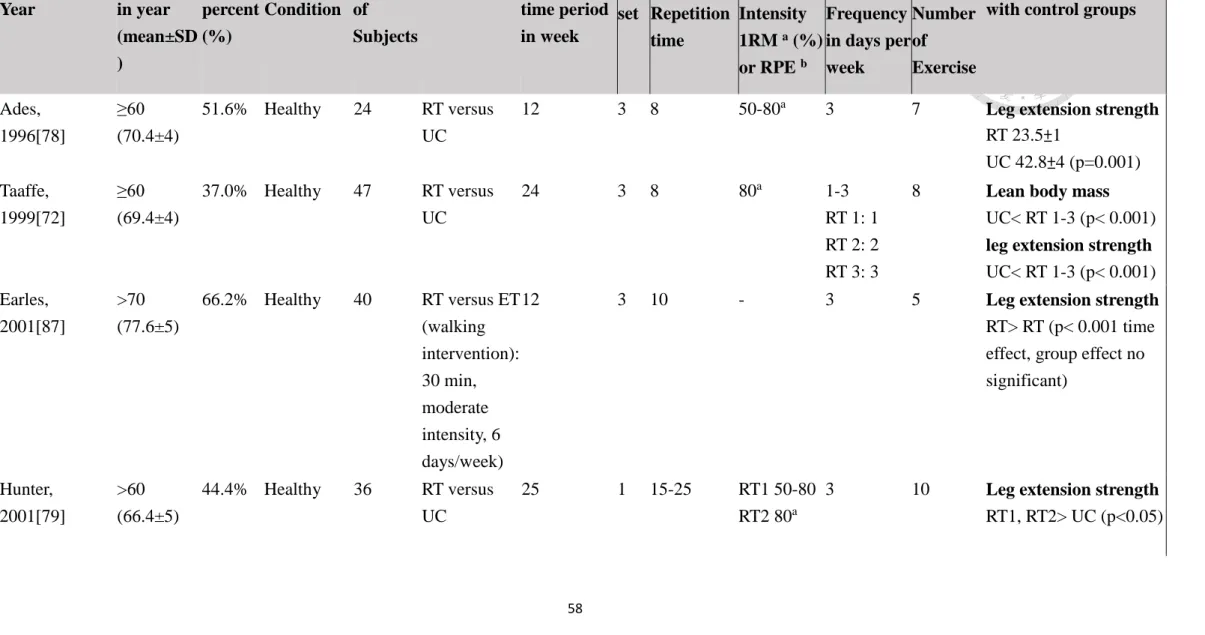
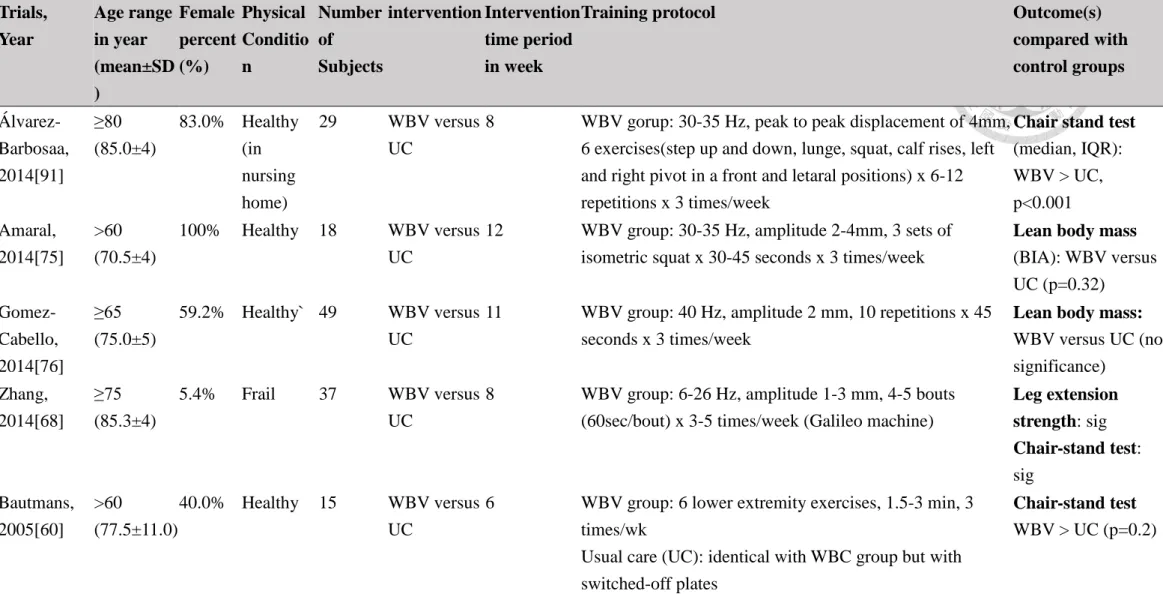
Table 2, 3 and 4 showed the selected characteristics of the 31 studies that met the
inclusion criteria. All studies involved comparisons on at least of two or three of four
arms (usual care, resistance training, endurance training and whole body vibration).
The studies recruited 1405 participants, of which female accounts for 58.5% while
four studies did not provide detailed information for the female percentage[59, 61-
63]. The age for the 31 randomized control trials was 60 to 92 years. The physical
conditions of participants in 23 studies were healthy older adults, while those physical
conditions of participants in 8 studies were type 2 diabetes[64], coronary artery
disease[65, 66], frailty[67, 68], and lower extremity weakness [69, 70],
hospitalized[71], respectively. The time period of 31 studies was 6 weeks to 48 weeks.
4.1 Muscle mass: Lean body mass
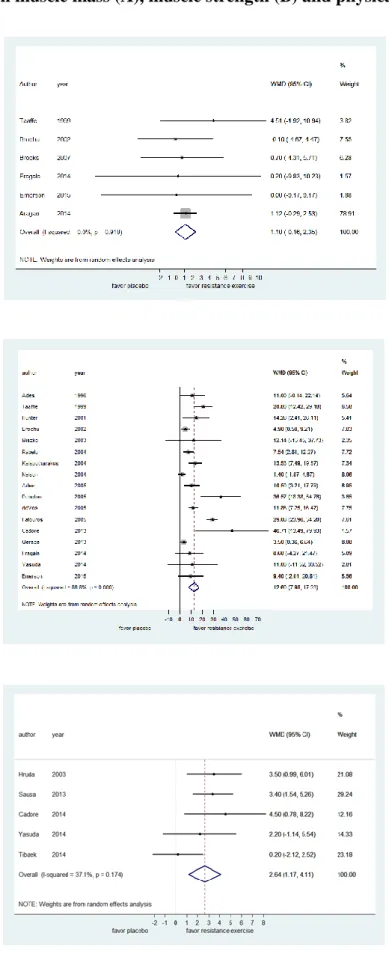
The results of traditional meta-analysis on the primary outcome in terms of lean body
mass was shown in figure 5A. Six trials compared resistance training with usual care
were included in our studies [59, 64, 65, 72-74], the result showed no significant
difference in the change of lean body mass, it still showed a difference by an increase
of 1.12 kg of lean body mass in comparison between resistance training and the
control group (95%CI -2.53–0.29).
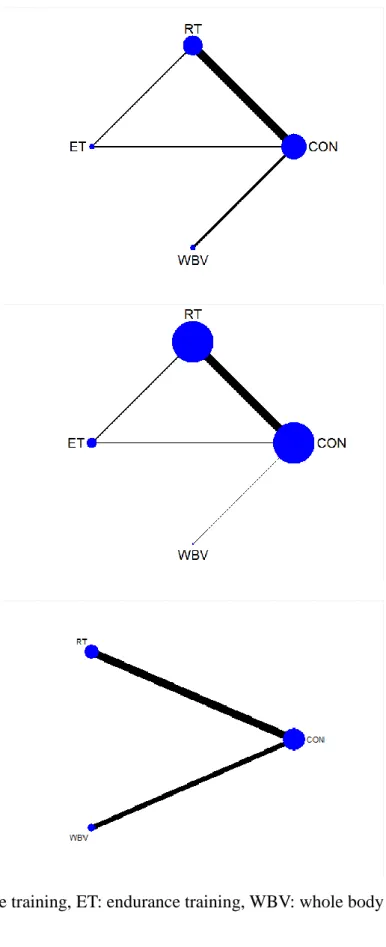
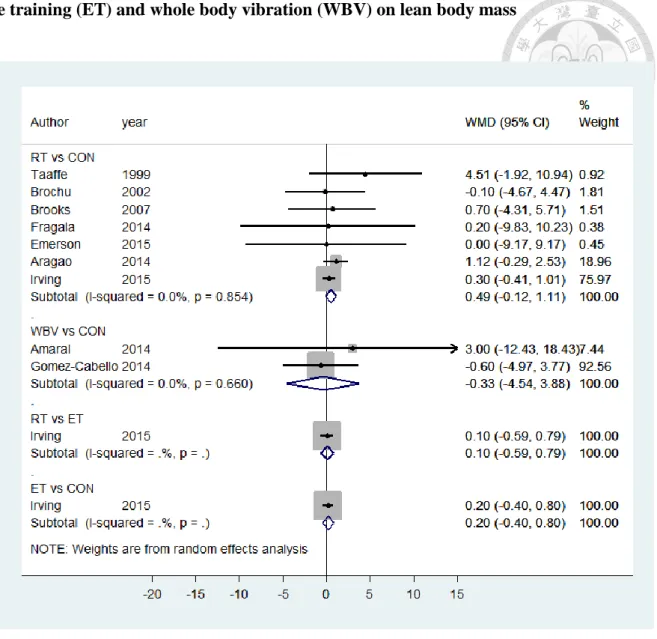
Eight studies of the 31 studies reported the outcome of lean body mass [64, 65, 72-
77], as shown in figure 6A. One of the eight trials was multi-arm. As shown in table 5
and figure 7, no significant difference was observed regarding changes in lean body
mass. Table 5 showed a greater difference by an increase of 0.82 kg of lean body mass
of comparison between resistance training versus whole body vibration (95%CI -3.43
to 5.08). And the difference of resistance training versus usual care (mean 0.49
[95%CI, -0.12–1.11]) is slight lower than that of endurance training versus whole
body vibration (mean 0.60 [95%CI -3.64 to 4.85]). However it showed a trend of a
slightly decrease in whole body vibration versus usual care (mean change-0.33
[95%CI -4.54–3.88]).
Figure 12A and 13A showed a rank from high to low, there is a 38% probability that
resistance training ranked 1st, 42% that endurance training ranked 2nd, 49% that
usual care ranked 3rd and 55% whole body vibration ranked 4th.
4.2 Muscle strength: Leg extension strength
Figure 5B displayed the results of the traditional meta-analysis on the assessment of
the secondary outcome based on the leg extension strength. Seventeen trials reported
outcome of leg extension strength were included in this meta-analysis [59, 62, 65, 66,
69, 70, 72, 73, 78-86]. We reported significant effect of resistance training on leg
extension strength. The comparison between resistance training and usual care
regarding leg extension strength was 12.6 kg (95%CI 7.98–17.2).
Twenty-one studies of the 31 studies reported the outcome of leg extension strength,
as shown in figure 6B [59, 60, 62, 65, 66, 69, 70, 72, 73, 77-88]. Two of the 21 trials
were multi-arms. As shown in table 5 and figure 8, no significant difference was
observed regarding changes in lean body mass. Compared with usual care, leg
extension strength was significantly increased with resistance training, with mean
difference 12.75 kg (95%CI 8.54–16.97). There were no statistically significance
between other pairwise comparisons.
Resistance training was ranked first according to the estimated surface under the
cumulative ranking curve values. Endurance training was more effective than were
usual care and whole body vibration (figure 12B and 13B)
Subgroup analyses were undertaken to investigate whether there was evidence of a
differential effect of measurement of 1-RM test in predefined subgroups of the
elderly. We analyzed data based on data collected from knee extension machine (7
trials) and leg press machine (15 trials) separately, as shown in table 6. The leg
extension strength assessed by knee extension machine and leg press machine were
both significantly increased in resistance training compared with usual care, with
mean difference 10.05 kg (95%CI 5.68–14.41) and 18.45 kg (95%CI 9.63–27.28),
separately.
4.3 Physical performance: chair-stand test
Figure 5C showed the results of the traditional meta-analysis on the assessment of the
secondary outcome based on the chair-stand test. Five studies reported outcome of
chair-stand test were included in this meta-analysis [62, 71, 86, 89, 90]. We reported
significant effect of resistance training on chair-stand test. The comparison between
resistance training and usual care regarding chair stand test was 2.64 times (95%CI
1.17–4.11).
As shown in table 5 and figure 9, the results of the network meta-analysis on the
assessment of outcome based on chair-stand test. Eight studies reported outcome of
chair-stand test were included in this analysis [60, 62, 68, 71, 86, 89-91]. Chair-stand
test was significantly improved with resistance training and whole body vibration,
comparing with usual care, with mean difference of 2.63 times (95% CI 1.34–3.93)
and 2.07 times (95%CI 0.49–3.65), respectively.
The result of ranking probability showed the most effective exercise intervention for
the elderly endpoint was resistance training. The second choice was whole body
vibration (figure 12C and 13C).
4.4 Publication bias
Examination of the Begg’s funnel plot of lean body mass (fig. 10A) and chair-stand
test (fig. 10C) were demonstrated considerable symmetry, suggesting that there was
no significant publication bias. However, funnel plot of leg extension strength (fig.
10B) showed asymmetry in a sample of 21 trials.
The Egger’s regression plot of lean body mass (fig. 11A) of leg extension strength
(fig. 11B) and chair stand test (fig. 11C) was graphically demonstrated. More the
intercept deviates from zero, the more pronounced the asymmetry. If the p-value of
the intercept is smaller than 0.05, the asymmetry is considered to be statistically
significant. The coefficient of bias of lean body mass and chair stand test were -0.27
and -0.48 (95%CI, -0.76–0.22 and -5.28–4.32, p = 0.25 and 0.82, separately). The
Egger’s test showed there were small study effects in leg extension strength
(coefficient of bias: -1.84, 95% CI-3.42–-0.26, p=0.024)
4.5 Statistical heterogeneity and Inconsistency
For muscle mass and physical performance, there were no statistically significance of
I squared between pair-wise comparison. But for muscle strength, there were
statistically significance of resistance training versus usual care (I squared=86.0%,
p=0.00). (Figure 7, 8 and 9)
For assessing inconsistency locally, we conducted loop-specific approach and“node-
splitting” method. We did not note any inconsistencies between evidence derived
from direct and indirect comparisons in these two methods. For assessing
inconsistency globally, we applied the design-by-treatment inconsistency model, we
did not find significant differences in relative effects.
Discussion
This systemic review and network meta-analysis provides evidence of an overall
benefit of resistance training for muscle strength and physical performance among
elderly people. The pair-wise comparison suggested benefits of whole-body vibration
on physical performance. However, three exercise interventions showed a
nonsignificant increase of muscle mass.
5.1 Comparison with previous studies
5.1.1 Muscle mass
Two meta-analyses have considered the effectiveness of resistance training in
nonelderly participants [42, 43]; however, one meta-analysis was published
concerning the benefits of resistance exercises in lean body mass among elderly
people [41]. A total of 49 randomized and nonrandomized controlled trails and 81
cohorts were included; the analysis revealed that after 20.5 weeks of resistance
training, a significant increase in lean body mass of 1.1 kg was recorded among
elderly people (95%CI 0.9–1.2kg, p<0.001). The average age in our study is much
higher than that of Peterson’s study (age range of our study: 64.8 to 91.9 years vs.
65.5±7 years); this difference between the two meta-analyses imply that exercise
effects among elderly people may attenuate, although no statistically significance
results were found in our study.
Among functionally limited elderly people, lower extremity muscle mass was a
critical determinant of physical performance, and a strong association was also
observed between lower extremity lean mass and muscle strength [92].
5.1.2 Muscle strength
Studies included in our network meta-analysis have indicated a significant
enhancement in leg extension strength. In a meta-analysis by Silva [44], 15 studies
(84 effect-sizes) were included, the pooled data of which revealed that resistance
training causes strength gains in adults over 55 years old (standard mean difference
2.00, 95%CI 1.76–2.23). However, our meta-regression analysis showed that strength
increases only if the training duration is sufficient. Compared with meta-analysis by
Osawa[47], four studies were included, the pooled data of which showed significant
enhancements in muscle strength of the knee extensor in the whole-body vibration
group. Our pooled effect also showed significant strength enhancements in the
resistance training group, but no significant enhancements were observed among the
endurance training, whole-body vibration, and usual care groups. Resistance loading
inhibits myostatin, which inhibits myoblast proliferation and differentiation in
developing muscle. By performing a muscle biopsy before and 24-hour after a series
of resistance training exercises, our study revealed that resistance training
downregulates myostatin expression and alters genes that are key to cell cycle
progression [93]. Through the increase in myofibrillar and mitochondrial protein
synthesis rates, resistance training improves the expression of myosin-heavy chains
and increases the quantity and improves the quality of muscle protein [94].
A recent Cochrane review included 121 trials with 6700 participants who received
progressive resistance training and were assessed according to physical functionality.
A modest improvement in gait speed and a moderate to large effect in chair-rise time
were observed [95].
5.1.3 Physical performance
The present study reports significant enhancement in physical performance in whole-
body vibration and resistance training. However, in a meta-analysis by Tschopp [96],
which comprised 11 trials and 377 elderly people, a small advantage over strength
training was observed for various functional outcomes (Short Physical Performance
Battery, chair-stand test, 5-time chair rise, box stepping). The difference between this
and our study is the different function tests applied.
5.2 Preservation of muscle mass and improvement of muscle strength
In a cross-sectional study, changes in muscle mass and strength during a 3-year period
were examined in 1880 elderly people. The knee extensor strength decline was much
more rapid than the concomitant loss of muscle mass, suggesting a decline in muscle
quality [97]. Why did muscle strength improve significantly in the resistance training
group, but not muscle mass? Additionally, why was physical performance in the
resistance training group and whole-body vibration group significantly improved?
Resistance training strengthens muscles that are involved in the exercise, but the
enhancement in strength may reflect an increase in fiber tissue or an improved
synchronization of contractions, rather than an increase in lean muscle mass [98].
Mechanisms of resistance exercise training appear to enhance muscle strength without
necessarily increasing muscle mass [99]. Furthermore, a Framingham Heart Study
revealed that total body and lower extremity muscle mass were not associated with
physical functionality in either men or women [100].
5.3 Improvement of muscle strength and physical performance
Resistance training significantly enhanced both muscle strength and physical
performance. These results imply that the performance in the chair stand test was
similar to that of the leg extension exercise. In Hardy’s study, improved leg extensor
power was correlated with improved chair-rise performance among 174 people aged
53 years [101]. However, improved performance in the chair-rise test was not
correlated with favorable performance in the muscle strength test. The improved
chair-rise performance was associated with improved standing balance performance
[101]. Furthermore, whole-body vibration was effective in improving balance ability
according to the Tinetti total score [102], Tinetti body balance score, and timed up-
and-go test. Our study also reveals that whole-body vibration significantly improved
performance in the chair-stand test, compared with the usual care group.
5.4 Improvement of muscle strength in the elderly with heart disease
In the healthy control group (aged older than 60 years), a significant reduction in leg
extensors strength in cardiac patients was observed [103], despite the fact that cardiac
diseases lead to calcium leak mechanisms in skeletal muscles, causing age-related loss
of muscle function and muscle weakness [104, 105]. In our study, the muscle strength
in elderly people with coronary heart disease was no poorer than that of the healthy
elderly participants [65, 66]. This can be explained by two possible reasons: 1.
Resistance training may delay this adverse mechanism. 2. In the two trials,
participants with stable angina, coronary heart disease, post revascularization status,
and myocardial infarction were included; participants with severe conditions (e.g.,
uncontrolled hypertension, very low threshold angina (<3 METs workload), and
hospitalization for an acute coronary syndrome within 6 months) were excluded.
5.5 Estimation the benefits of endurance training on physical performance
No scientific evidence exists to support that improvement in the chair-stand test
because of endurance training is a measure of physical performance. However, we
extracted data from Davidson’s study for a similar comparison [106]. A total of 136
sedentary, abdominally obese elderly men and women were recruited and randomized
to 1 of the following 4 groups for 6 months: resistance training, endurance training,
combined exercise, and nonexercise control. This study was excluded from our
network meta-analysis because all participants received dietary intervention.
However, when we extracted data from the resistance training group and the
endurance training group to pool with our network meta-analysis of physical
performance, the results indicate that endurance training was the most effective
exercise intervention. Resistance training was considered the second most effective
option, and whole-body vibration was the third treatment option for the obese
participants, as shown in table 7. The trend in physical performance implies that
endurance training is an acceptable exercise intervention for elderly people.
5.6 Public health issue and clinical implication
In the current systemic review and network meta-analysis, we present available
evidence regarding the effectiveness of the three exercise interventions on the
indicators of sarcopenia and as treatment for sarcopenia. The roles of the three
indicators of sarcopenia prevention after exercise training are also presented in our
study. Muscle mass (lean body mass) was considered as an indicator. By examining
muscle mass, we observed that the participants who accepted exercise intervention did
not lose muscle mass with age. Muscle strength and physical performance were the
two appropriate indicators for preventing sarcopenia. The improvements after exercise
intervention were easily measured according to muscle strength and physical
performance.
Building muscle as a result of exercise intervention is crucial for successful aging.
Performing appropriate exercises to prevent and treat sarcopenia can considerably
benefit the prevention of the consequences attributed to falling and immobility, help
avoid hospitalization, and contribute to healthy aging. Our study reveals how key
indicators change after exercising, which may influence recommendations for elderly
people.
5.7 Strength and limitation
The strengths of this study are as follows: (1) This study is the first network meta-
analysis to investigate the relative efficacy between a pair of exercise interventions (2)
It possesses more restrictive inclusion criteria than those of other randomized
controlled trials; (3) It exhibits more robust outcomes and reveals relevant indicators
of sarcopenia; and (4) It has higher generalizability, including not only the healthy
elderly population, but also elderly people with frailty, type 2 DM, and cardiovascular
disease. The study limitations are variability in training characteristics and outcome
measurements.
5.8 Direction of future research
Translating research into clinical practice is challenging. With regard to the clinical
practice of resistance training, endurance training, and whole-body vibration, more
research must be conducted to create a structured guideline. This guideline would
provide practical information on increasing muscle mass and enhancing strength and
physical performance. To effectively enhance muscle attributes, the benefits of
exercises combined with other remedies (i.e., nutrition interventions, behavioral
modification technique, medicine) may be investigated in future research. Because
many elderly people are unwilling or simply unable to engage in exercise training,
future research is necessary to develop structural programs for preventing sarcopenia.
Conclusion
Resistance training is beneficial for elderly people with outcome indicators of
sarcopenia; specifically, it enhances muscle strength and physical performance.
Resistance training and whole-body vibration were the two most effective exercise
interventions in terms of physical performance. However, no statistically significant
results were observed for resistance training, endurance training, and whole-body
vibration concerning increases in muscle mass.
References
1. Cruz-Jentoft, A.J., J.P. Baeyens, J.M. Bauer, Y. Boirie, T. Cederholm, F. Landi, F.C. Martin, J.P. Michel, Y. Rolland, S.M. Schneider, E. Topinkova, M.
Vandewoude, M. Zamboni, and P. European Working Group on Sarcopenia in Older, Sarcopenia: European consensus on definition and diagnosis: Report of the European Working Group on Sarcopenia in Older People. Age Ageing, 2010. 39(4): p. 412-23.
2. World Population Ageing, 2013. 2013.
3. von Haehling, S., J.E. Morley, and S.D. Anker, An overview of sarcopenia:
facts and numbers on prevalence and clinical impact. Journal of cachexia, sarcopenia and muscle, 2010. 1(2): p. 129-133.
4. Chen, L.-K., L.-K. Liu, J. Woo, P. Assantachai, T.-W. Auyeung, K.S. Bahyah, M.-Y. Chou, L.-Y. Chen, P.-S. Hsu, and O. Krairit, Sarcopenia in Asia:
consensus report of the Asian working group for sarcopenia. Journal of the American Medical Directors Association, 2014. 15(2): p. 95-101.
5. Berger, M.J. and T.J. Doherty, Sarcopenia: prevalence, mechanisms, and functional consequences. 2010.
6. Wakabayashi, H. and K. Sakuma, Comprehensive approach to sarcopenia treatment. Current clinical pharmacology, 2014. 9(2): p. 171-180.
7. Kim, J., Y.-h. Lee, J. Huh, D. Kang, Y. Rhee, and S.-K. Lim, Early-stage chronic kidney disease, insulin resistance, and osteoporosis as risk factors of sarcopenia in aged population: the fourth Korea National Health and
Nutrition Examination Survey (KNHANES IV), 2008–2009. Osteoporosis International, 2014. 25(9): p. 2189-2198.
8. Kalyani, R.R., M. Corriere, and L. Ferrucci, Age-related and disease-related muscle loss: the effect of diabetes, obesity, and other diseases. The Lancet Diabetes & Endocrinology, 2014. 2(10): p. 819-829.
9. Cederholm, T.E., J.M. Bauer, Y. Boirie, S.M. Schneider, C.C. Sieber, and Y.
Rolland, Toward a definition of sarcopenia. Clinics in geriatric medicine, 2011. 27(3): p. 341-353.
10. Jiménez, J.B., G.L. Lluch, I.S. Martínez, A. Muro-Jiménez, E.R. Bies, and P.
Navas, Sarcopenia: implications of physical exercise in its pathophysiology, prevention and treatment. Revista andaluza de medicina del deporte, 2011(4):
p. 158-166.
11. Beaudart, C., R. Rizzoli, O. Bruyère, J.-Y. Reginster, and E. Biver, Sarcopenia: burden and challenges for public health. Archives of Public Health, 2014. 72(1): p. 1-8.
12. Maeda, K. and J. Akagi, MON-PP026: Cognitive Decline is an Independent Comorbidity Associated with Sarcopenia in Geriatric Hospital Patients.
Clinical Nutrition, 2015. 34: p. S137.
13. Sheetz, K.H., S.A. Waits, M.N. Terjimanian, J. Sullivan, D.A. Campbell, S.C.
Wang, and M.J. Englesbe, Cost of major surgery in the sarcopenic patient.
Journal of the American College of Surgeons, 2013. 217(5): p. 813-818.
14. Englesbe, M.J., S.P. Patel, K. He, R.J. Lynch, D.E. Schaubel, C. Harbaugh, S.A. Holcombe, S.C. Wang, D.L. Segev, and C.J. Sonnenday, Sarcopenia and mortality after liver transplantation. Journal of the American College of Surgeons, 2010. 211(2): p. 271-278.
15. Tan, B.H., L.A. Birdsell, L. Martin, V.E. Baracos, and K.C. Fearon,
Sarcopenia in an overweight or obese patient is an adverse prognostic factor in pancreatic cancer. Clinical cancer research, 2009. 15(22): p. 6973-6979.
16. Horlings, C.G., B.G. van Engelen, J.H. Allum, and B.R. Bloem, A weak balance: the contribution of muscle weakness to postural instability and falls.
Nature Clinical Practice Neurology, 2008. 4(9): p. 504-515.
17. Davis, J.W., P.D. Ross, M.C. Nevitt, and R.D. Wasnich, Risk factors for falls and for serious injuries on falling among older Japanese women in Hawaii.
Journal of the American Geriatrics Society, 1999. 47(7): p. 792-798.
18. Clynes, M., M. Edwards, B. Buehring, E. Dennison, N. Binkley, and C.
Cooper, Definitions of sarcopenia: associations with previous falls and fracture in a population sample. Calcified tissue international, 2015. 97(5): p.
445-452.
19. Tan, M.P., S.B. Kamaruzzaman, M.I. Zakaria, A.V. Chin, and P.J.H. Poi, Ten‐
year mortality in older patients attending the emergency department after a fall. Geriatrics & gerontology international, 2016. 16(1): p. 111-117.
20. Visser, M., B.H. Goodpaster, S.B. Kritchevsky, A.B. Newman, M. Nevitt, S.M. Rubin, E.M. Simonsick, and T.B. Harris, Muscle mass, muscle strength, and muscle fat infiltration as predictors of incident mobility limitations in well-functioning older persons. The Journals of Gerontology Series A:
Biological Sciences and Medical Sciences, 2005. 60(3): p. 324-333.
21. Janssen, I., Influence of sarcopenia on the development of physical disability:
the Cardiovascular Health Study. Journal of the American Geriatrics Society, 2006. 54(1): p. 56-62.
22. Janssen, I., D.S. Shepard, P.T. Katzmarzyk, and R. Roubenoff, The healthcare costs of sarcopenia in the United States. Journal of the American Geriatrics Society, 2004. 52(1): p. 80-85.
23. Szulc, P., F. Duboeuf, F. Marchand, and P.D. Delmas, Hormonal and lifestyle determinants of appendicular skeletal muscle mass in men: the MINOS study.
The American journal of clinical nutrition, 2004. 80(2): p. 496-503.
24. Montero-Fernandez, N. and J. Serra-Rexach, Role of exercise on sarcopenia in the elderly. European journal of physical and rehabilitation medicine, 2013.
49(1): p. 131-143.
25. Burton, L.A. and D. Sumukadas, Optimal management of sarcopenia. Clin Interv Aging, 2010. 5(452): p. 217-28.
26. Medicine, A.C.o.S., ACSM's guidelines for exercise testing and prescription.
2013: Lippincott Williams & Wilkins.
27. Coggan, A.R., R.J. Spina, D.S. King, M.A. Rogers, M. Brown, P. Nemeth, and J. Holloszy, Skeletal muscle adaptations to endurance training in 60-to 70-yr- old men and women. Journal of Applied Physiology, 1992. 72(5): p. 1780- 1786.
28. Cardinale, M. and J. Wakeling, Whole body vibration exercise: are vibrations good for you? British journal of sports medicine, 2005. 39(9): p. 585-589.
29. Prisby, R.D., M.-H. Lafage-Proust, L. Malaval, A. Belli, and L. Vico, Effects of whole body vibration on the skeleton and other organ systems in man and animal models: what we know and what we need to know. Ageing research reviews, 2008. 7(4): p. 319-329.
30. Kiiski, J., A. Heinonen, T.L. Järvinen, P. Kannus, and H. Sievänen,
Transmission of vertical whole body vibration to the human body. Journal of bone and mineral research, 2008. 23(8): p. 1318-1325.
31. Rittweger, J., Vibration as an exercise modality: how it may work, and what its potential might be. European journal of applied physiology, 2010. 108(5): p.
877-904.
32. Rittweger, J., M. Mutschelknauss, and D. Felsenberg, Acute changes in neuromuscular excitability after exhaustive whole body vibration exercise as compared to exhaustion by squatting exercise. Clinical physiology and functional imaging, 2003. 23(2): p. 81-86.
33. Lam, F.M., L. Liao, T.C. Kwok, and M.Y. Pang, The effect of vertical whole- body vibration on lower limb muscle activation in elderly adults: Influence of vibration frequency, amplitude and exercise. Maturitas, 2016. 88: p. 59-64.
34. Torvinen, S., Effect of whole body vibration on muscular performance, balance, and bone. 2003: Tampere University Press.
![Figure 1. Scheme of the different etiological sarcopenia mechanism and their consequences [1, 10]](https://thumb-ap.123doks.com/thumbv2/9libinfo/9605572.631632/65.1262.108.914.186.697/figure-scheme-different-etiological-sarcopenia-mechanism-consequences.webp)