行政院國家科學委員會專題研究計畫 成果報告
IA,IC,III 類抗心律不整藥物對不同年齡兔子房室結正向
及逆向傳導的影響
計畫類別: 個別型計畫 計畫編號: NSC93-2314-B-006-055- 執行期間: 93 年 08 月 01 日至 94 年 07 月 31 日 執行單位: 國立成功大學醫學系小兒科 計畫主持人: 吳俊明 共同主持人: 林立人,王玠能 報告類型: 精簡報告 處理方式: 本計畫可公開查詢中 華 民 國 94 年 10 月 30 日
Developmental electrophysiologic effects of propafenone, procaine, and sotalol drugs on the rabbit atrioventricular nodal conduction
Introduction
The cardiac electrical system is designed to ensure the appropriate rate and time of contraction in all regions of the heart, which are essential for effective cardiac function. Well-controlled cardiac electrical activity depends on specialized properties of variable components of the cardiac conduction system, including the sinoatrial node, atria, atrioventricular node, His-Purkinje system, and ventricles. Recently, it is much clear that the specific cardiac electrical function of each conduction component is determined by its differential distribution of cardiac ion channels expression.1
The immature mammalian heart had different electrophysiologic features from that of adult heart due to delay maturation and different distribution of cardiac ionic channels on the conduction system.2-7 Therefore, the responses to variable
anti-arrhythmic drugs might be different between the immature and the adult heart.4-16 The immature mammalian heart usually has higher intrinsic heart rate, shorter
effective or functional refractory period (ERP & FRP), and prominent effect to the cardiac ionic channel blockers than that of the adult heart. 4-16 From our previous isolated super-infused rabbit heart study also showed the similar results. The neonate rabbit heart (within 7 days) had shorter AHmin, AHmax, and Wenckebach blocking
cycle length intervals of AV node, and shorter ERP and FRP of atrium, perinodal tissue, AV node and its posterior nodal extension than those of the adult rabbits (2-3 months & 6 months). The neonate heart was also difficult to induce AV reentry and AVN reentrant tachycardia.
Isolated superinfused rabbit heart model had been established for cardiac
elctrophysiologic study. By using this model, we can accurately place the recording and pacing catheters at different atrial sites, perinodal transitional tissue, posterior nodal extension (PNE), and His bundle area. There is evidence that the posterior nodal extension may form the slow pathway substrate.17 By using this animal model, we can compare the cardiac electrophysiologic effects of variable anti- arrhythmic drugs (propafenone, procaine, and sotalol) between the immature and adult heart and differential effect on the antegrade or retrograde AV conduction at different drug concentration.
Purposes of this study
To study the developmental effects of class Ic (propafenone), Ia (procaine) and III (sotalol) at different concentration on the antegrade and retrograde dual AV conduction in the rabbit heart.
supraventricular tachycardia, and ventricular tachycardia in adult patients. It is classified as type Ic antiarrhythmic drug with potent fast sodium channel blocking effect, moderate β-blocking activity, and weak Ca2+ channel blocking actions.18 These latter two properties may be unimportant for most arrhythmias in adult; they might cause significant effects on the immature heart.2, 9-13 In children and infants, propafenone has been shown to be uniquely effective in treating junctional automatic tachycardia and reentrant supraventricular tachycardia,19 but there was rare reports discussion about the differential effects between the immature and adult heart.16
Procaine is a fast sodium channel blocker with mild anticholinergic properties, and is classified as type Ia antiarrhythmic drug.20 Whether procainamide similar to quinidine (class Ia drug) also has other ionic blocking effect activity was still unproven?5 Procainamide has been used to treat supraventricular tachycardia in children. There were little reports discussing the difference effect of procainamide upon the conduction tissues especially the dual antegrade and retrograde conduction.20
Sotalol posses class II (noncardioselectiveβ-blocking) and class III
antiarrhythmic properties (mainly blocking the fast-activating potassium Ikr ionic
channel that leads to prolong the action potential duration) electrophysiologic effects.21 The concentration-response curves of these 2 action differ, however, with β-blockade beginning and reaching maximum effect at lower concentrations than the class III effect. 21 Sotalol has proved to be very efficacious in the treatment of a variety of ventricular and supraventricular arrhythmias in adult.21-25 Experience with its utility in the treatment of pediatric arrhythmia was not plentiful and maily focued on the supraventricular tachycardia.26 The comparison the electrophysiologic effect of sotalol at different drug concentration between immature and adult heart was limited, and some of the conclusion were still controversial.22-24
Methods
Preparation and Apparatus
The experiments are performed in superfused rabbit heart preparations of male New Zealand white rabbits. Rabbits of two different ages are included, being 7-10 days old and 2 months old. Five rabbits of each age group are included for every drug category. Rabbits are anesthetized with pentobarbital, 20-30 mg/kg (i.v. in adults and i.p. in neonates). The hearts are removed by midsternal thoracotomy. The preparations include right atrium, AV node, and upper part of the interventricular septum and are fixed on a grid mounted in a tissue bath. The tissue is superfused with oxygenated (95%O2-5% CO2) Tyrode’s solution at 37° C and pH 7.34. A 6-liter volume of
solution is continuously re-oxygenated and recirculated at 200 ml/min. The composition of the solution is (mM) 128.2 NaCl, 4.7 KCl, 2 CaCl2, 1 MgCl2, 25
NaHCO3, 0.7 NaH2PO4, and 11.1 dextrose.The unipolar electrograms are recorded,
by using 125-µm platinum-iridium wire (Teflon-coated), at upper atrium (UA), crista terminalis (CT), interatrial septum (IAS), His bundle, transitional cells (E1). Another
125-µm platinum-iridium wire is placed at posterior nodal extension (PNE) with the aid of micromanipulator. A reference electrode is positioned in the bath close to the preparation. Atrial pacing is achieved with a bipolar platinum-iridium stimulating electrode positioned on the crista terminalis near the sinus node. Another two
platinum-iridium electrodes are placed at His bundle to obtain good His signals and then connected to the stimulation ports for His stimulation.
Protocol
Antegrade AV conduction
The effects of various antiarrhythmic agents on the AV nodal recovery curve, obtained in response to a premature stimulation protocol, are assessed at a basic rate of 450-500ms. A test premature impulse is introduced at every 20th basic beat with a decrement of 30, 20, 10, 5 and 1 ms in progressively shorter coupling interval ranges. Wenckebach blocking cycle length is determined by rapid atrial stimulation starting at cycle length slightly shorter than basic drive for 20 beats and repeats with decrement of cycle length by 10 ms until Wenckebach periodicity or 2:1 block occurs.
Retrograde AV conduction
Similar protocols as stated in “antegrade AV conduction” are repeated with stimulation at His bundle.
Baseline AV nodal function
Baseline AV nodal function, antegrade as well as retrograde, is tested to obtain atrial effective refractory period, nodal effective refractory period and Wenckebach blocking cycle length.
Antiarrhythmic drug testing
After having tested the baseline function, the following drugs are tested. The ranges of testing concentrations of every antiarrhythmic drug are listed below. Both antegrade and retrograde protocols are tested for each concentration of antiarrhythmic
CS HIS CT PNE TV LN CN IAS E1 UA
drugs and after the washout. Drugs are perfused at each concentration for 15 minutes before testing the protocols.
Group I. (class Ia) Procaine: 0.1 µM to 10 µM. Group II. (class Ic) Propafenone: 0.1 µM to 10 µM. Group III (class III) Sotalol: 0.1 µM to 10 µM.
After having tested the maximal concentration of drugs, drug-containing solution is removed and recirculated with fresh Tyrode’s solution. Same antegrade and
retrograde protocols are repeated. Interval measurements and Analysis
Electrograms are digitized at 5kHz per channel with the Axoscope program (Axon instruments, Foster City, CA) and analyzed with Data-Pac 2000 program (Run Technologies, Laguna Hills, CA). Activation time at atrio-nodal entrance (A), His bundle (H), transitional cells are determined from both the crista terminalis and interatrial septum inputs. The nodal recovery curve is constructed by plotting the His conduction time (A2H2) against the coupling interval of premature stimulation (A1A2)
for antegrade conduction. Local recovery curves of transitional cells will also be constructed in a similar manner. For each protocol we determine the nodal properties in terms of A2H2min, A2H2max, effective refractory period and functional refractory
period. We also determine corresponding parameters at the transitional cells. Retrograde curve is plotted His-atria conduction time (H2A2) against the coupling
interval of premature stimulation at His bundle (H1H2). Corresponding retrograde
curve is constructed in a similar manner. Definitions
The atrial effective refractory period is the longest S1S2 interval in which the S2
fails to elicit an atrial response. The shortest A1A2 interval that produced an A2
response is defined as the atrial functional refractory period. The AV node effective refractory period is the longest A1A2 interval in which the A2 fails to elicit a response
in the His-bundle. The shortest H1H2 obtained is the functional refractory period of
His bundle. The retrograde AV node effective refractory period is defined as the longest H1H2 in which H2 fails to elicit a response in atrium. The minimal conduction
times (AHmin, HAmin) are defined as the shortest conduction times measured at basic
driving cycle length of antegrade and retrograde conduction. The maximal conduction times (AHmax, HAmax) are the longest conduction times measured during premature
pacing. The differences of minimal or maximal conduction times between different concentrations of every given antiarrhythmic drugs are called ∆AHmin, ∆HAmin,
∆AHmax, ∆HAmax, respectively.
Results
The effects of above-mentioned 3 anti-arrhythmic agents on AV nodal properties was analyzed and presented in several parameters. The abbreviations of these
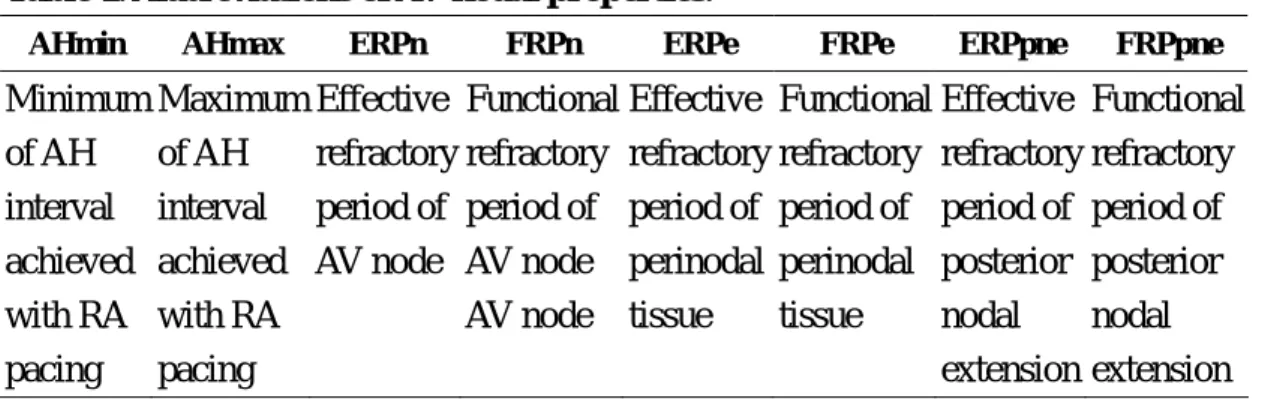
Table 1. Abbreviations of AV nodal properties.
AHmin AHmax ERPn FRPn ERPe FRPe ERPpne FRPpne
Minimum of AH interval achieved with RA pacing Maximum of AH interval achieved with RA pacing Effective refractory period of AV node Functional refractory period of AV node AV node Effective refractory period of perinodal tissue Functional refractory period of perinodal tissue Effective refractory period of posterior nodal extension Functional refractory period of posterior nodal extension Effects of propafenone
The group of propafenone consisted 5 adult rabbit preparations. Two
preparations failed to maintain 1:1 AH conduction with basic pacing cycle length at 5 μM of propafenone. At 10μM, 4 preparations failed. Only 1 preparation kept 1:1 AH conduction at 10μM, which was not shown in Table 2. Various parameters of AV nodal properties were listed in Table 2. As the concentration of propafenone increased, AHmin and AHmax prolonged steadily. Both ERPn and FRPn increased the
concentration of propafenone was getting higher The Figure 1 showed AH conduction curve of one of the preparations. At lower concentration of propafenone (lower than 0.5μM), the curves shifted slightly upward at the right part of the curves. However, left part of the curve merged together without showing any evidence of shifting. As the concentration further increased, the whole AH curve shifted upward and showed marked increment of ERPn.
Table 2. Effects of propafenone on AV nodal properties in adult rabbits.
AHmin AHmax ERPn FRPn ERPe FRPe ERPpne FRPpne Baseline 63±13 141±31 130±25 189±10 111±6 144±13 111±7 169±14 0.1μM 67±15 142±31 133±32 192±17 123±4 144±11 125±21 170±43 0.2μM 78±21 144±28 150±47 207±44 122±7 145±17 128±12 180±29 0.5μM 86±31 146±29 181±92 233±84 139±18 172±56 140±18 201±6 1μM 92±32 165±48 198±108 261±96 151±21 176±37 209±128 258±117 2μM 99±39 163±51 190±23 237±35 203±35 215±41 184±33 232 ±30 5μM 128±76 167±79 207±36 254±38 250±79 246±103 186±50 238±47
All values were in the unit of ms.
Likewise, propafenone affected perinodal transitional tissue and posterior nodal extension in the similar way, with minimal effect at concentration lower than 0.2μM and substantial influence at higher concentration.
AA 50 100 150 200 250 300 350 400 450 AH 60 80 100 120 140 160 180 200 BL 0.1 UM 0.2 UM 0.5 UM 1 UM 2 UM 5 UM
Figure 1. The effect of different concentrations of propafenol on antegrade atrioventricular conduction of adult rabbit heart
Propafenone affected the retrograde AV conduction in the same way as that in antegrade properties. One of the examples was showed in Figure 2. There were marked changes of HA intervals as the dose of propafenone increased.
Figure 2. The effect of differrent propafenol drug concentrations on the retrograde atrioventricular nodal conduction of adult rabbit heart
HH 150 200 250 300 350 400 450 HA 100 120 140 160 180 200 RBL R 0.1 UM R 0.2 UM R 0.5 UM R 1 UM R 2 UM
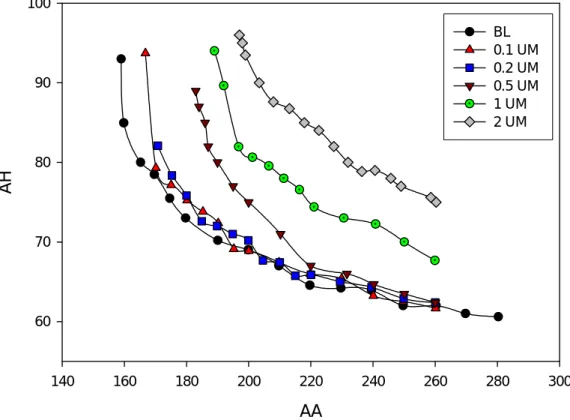
The neonate heart behaved to propafenone in similar way, as did the adult heart preparation (Figure 3). However, the former seemed to be slightly resistant to the inhibitory effect of propafenone, as the curve obviously shifted upward at
concentration higher than 1μM. At 0.5μM, right part of the curve did not change. Left part of the curve tilted to right. This might imply that slow pathway was affected earlier than fast pathway.
AA 140 160 180 200 220 240 260 280 300 AH 60 70 80 90 100 BL 0.1 UM 0.2 UM 0.5 UM 1 UM 2 UM
Figure 3. The effect of differrent propafenol concentrations on the antegrade atrioventricular conduction of neonate rabbit heart
Effects of Sotalol
The group of sotalol consist 5 adult rabbit heart preparations. Various conduction properties were listed in Table 3. Obviously there was no difference in AHmin of various concentration of sotalol. AHmax increased slightly only at concentration of 10 μM, which did not reach a statistical significance. The minimal influence of sotalol on antegrade AV conduction could be seen in Figure 4. The AH conduction curve did not shift either upward of downward in responding to different concentrations of sotalol. Similarly, the ERPn and FRPn showed only slight but insignificant increment at 10μM of sotalol.
Table 3. Effects of sotalol on antegrade AV nodal properties in adult rabbits AHmin AHmax ERPn FRPn ERPe FRPe ERPpne FRPpne
Baseline 63±12 147±28 106±12 175±12 107±17 123±27 106±12 151±13 0.1μM 62±12 149±22 105±8 177±18 102±13 121±24 102±11 150±15 0.2μM 63±12 154±18 107±9 180±21 102±28 126±22 105±7 155±16 0.5μM 61±11 148±23 108±5 177±17 112±18 126±29 110±5 156±22 1μM 63±9 148±14 108±8 180±9 105±23 126±22 108±6 158±24 2μM 63±9 148±11 109±8 178±10 111±19 126±24 109±11 157±22 5μM 64±8 151±11 112±9 178±11 114±14 129±19 112±9 156±22 10μM 63±10 157±18 112±8 186±9 113±15 135±11 113±8 161±22
All values were in the unit of ms.
The effects of sotalol on the perinodal tissue and posterior nodal extension were similarly minimal with slightly increment in terms of FRPe and FRPpne at 10μM. Referring to Figure 4, there were minimal shifts of curves. It was not possible to tell whether fast or slow pathway was more affected by sotalol.
However, in the same preparation, retrograde conduction was more affected by sotalol (Figure 5). As the concentration of sotalol increased, the HA conduction curve shifted upward with left part of the curve shifted to right. This refers to inhibitory effect of sotalol on retrograde AV nodal conduction.
Figure 4. The effect of differrent sotalol concentrations on the antegrade atrioventricular conduction of adult rabbit heart
AA 100 200 300 400 500 AH 80 100 120 140 160 180 200 10 UM 0.1 UM 0.2 UM 0.5 UM 1 UM 2 UM 5 UM BL
Figure 5. The effect of differrent sotalol concentrations on the retrograde atrioventricular conduction of the adult rabbit heart
HH 150 200 250 300 350 400 450 500 HA 60 70 80 90 100 110 120 RBL R 0.1UM R 0.2 UM R 0.5 UM R 1 UM R 2 UM R 5 UM R 10 UM
The effects of sotalol on neonate rabbit heart preparation were shown in Figure 6. Right part of the AH conduction curves showed more substantial upward shift than that in adult rabbit heart preparation. Left part of the curves converged together and only showed right and upward shift at concentration higher than 5μM of sotalol. This implied that sotalol affected fast pathway at lower concentration and started to affect slow pathway at higher concentration.
Figure 6. The effect of differrent sotalol concentration on the antegrade atrioventricular conduction of the neonate rabbit heart
AA 100 200 300 400 500 AH 60 80 100 120 140 BL 0.1 UM 0.2 UM 0.5 UM 1 UM 2 UM 5 UM 10 UM
Effects of procaine
Table 4 listed the AV nodal properties in responding to different concentration of sodium channel blocker (type Ia), procaine. This group consisted 3 adult rabbit preparations. There were some missing ERP values in Table 4, which were limited by early appearance of ERP of atrium.
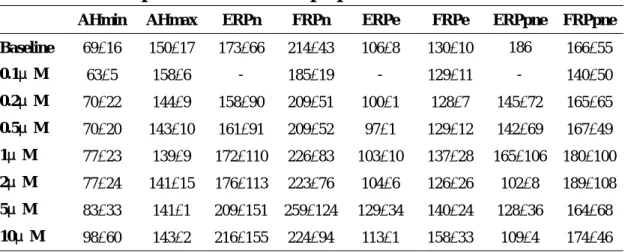
Table 4. Effects of procaine on AV nodal properties in adult rabbits.
AHmin AHmax ERPn FRPn ERPe FRPe ERPpne FRPpne
Baseline 69±16 150±17 173±66 214±43 106±8 130±10 186 166±55 0.1μM 63±5 158±6 - 185±19 - 129±11 - 140±50 0.2μM 70±22 144±9 158±90 209±51 100±1 128±7 145±72 165±65 0.5μM 70±20 143±10 161±91 209±52 97±1 129±12 142±69 167±49 1μM 77±23 139±9 172±110 226±83 103±10 137±28 165±106 180±100 2μM 77±24 141±15 176±113 223±76 104±6 126±26 102±8 189±108 5μM 83±33 141±1 209±151 259±124 129±34 140±24 128±36 164±68 10μM 98±60 143±2 216±155 224±94 113±1 158±33 109±4 174±46
All values were in the unit of ms.
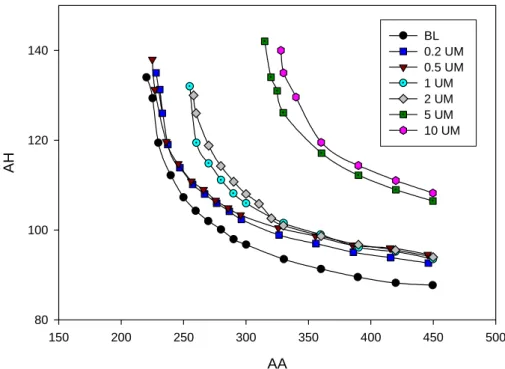
As shown in Figure 7, the AH curves shifted upward tilted to right as the procaine concentration increased. At lower concentrations, right part of the curves shifted upward more than left part did, which refers to that fast pathway was affected more than the slow pathway. As the concentration increased further, left part of the curve tilted to right. ERPn was significantly affected and increased at higher
concentration. However, FRPn, ERPe, ERPpne, FRPe, and FRPpne were not affected. Moreover, the increments of AH corresponding to different procaine concentration were less than that caused by propafenone.
Similar trend was also observed in retrograde conduction as shown in Figure 8. However, the shift was evenly observed in either right or left part of the curve. Consequently, fast and slow pathways were equally affected in terms of retrograde conduction.
The effects of procaine on neonate rabbit heart preparation were shown in Figure 9. There was a slight upward shifting of the nodal conduction curve only at the high concentration of procaine.
Figure 7. The effect of differrent procaine concentrations on the antegrade atrioventricular conduction of the adult rabbit heart
AA 150 200 250 300 350 400 450 500 AH 80 100 120 140 BL 0.2 UM 0.5 UM 1 UM 2 UM 5 UM 10 UM
Figure 8. The effect of differrent procaine concentrations on the retrograde atrioventricular conduction of adult rabbit heart
HH 100 150 200 250 300 350 400 450 500 HA 80 100 120 140 160 180 200 220 RBL R-0.2 UM R-0.5 UM R-1 UM R-2 UM R-5 UM R-10 UM
AA 50 100 150 200 250 300 350 AH 20 40 60 80 100 120 140 160 BL 0.1 UM 0.2 UM 0.5 UM 1 UM 2 UM 5 UM 10 UM
Figure 9. The effect of differrent procaine concentrations on the antegrade atrioventricular conduction of the neonate rabbit heart
Conclusions
Current results demonstrated inhibitory effects of propafenone and procaine on the antegrade and retrograde AV nodal conduction properties. The magnitude of inhibition was more prominent in the setting of propafenone than procaine. However, sotalol did not show significant effects on antegrade conduction. Meanwhile, some inhibitory effects were seen on retrograde properties. Consequently, the inhibitory effect of AV node among these three agents was in the decreasing order of
propafenone, procaine, and sotalol. The response was less substantial in the setting of neonate preparations than in adult preparations.
Both propafenone and procaine are sodium-channel blockers. Type Ic
anti-arrhythmic agents been known to be the most potent sodium-channel blocking agents. It is not surprising to have more substantial effect on AV nodal properties in the group of propafenone. Procaine, a type Ia anti-arrhythmic agent, showed similar but less intensive inhibitory effect.
Surprisingly, sotalol, a combined class II and III agent, showed minimal inhibitory effect at low and moderate concentrations. Even with the highest concentration we tested, the inhibition was quite modest. We speculated the mechanism underlying this phenomenon might be attributed to virtue of the
experimental preparation. Our setup is a superfused preparation, which eliminates all the autonomic influences. In other word, the beta-blocking effect of sotalol might be
obliterated in our denervated heart preparation. As for the weak evidence of inhibition from class III characteristic, we don’t have good explanation at present. Probably, higher concentration may be required in order to achieve an equal inhibition, comparing with other two agents.
The number of neonate preparations is still inadequate to reach a solid conclusion. Therefore, more experiments are needed to disclose the nature. Furthermore, intracellular recording may need needed to clarify the difference between the adult and neonate heart preparations.
References:
1) Schram G, Pourrier M, Melnyk P, Nattel S. Differential distribution of cardiac ion channel expression as a basis for regional specialization in electrical function. Circ Res. 2002; 90: 939-50.
2) Chin TK, Friedman WF, Klitzner TS. Developmental changes in cardiac myocyte calcium regulation. Cir Res 1990; 67: 574-9.
3) Hewett KW, Gaymes CH, Noh CIL, et al. Cellular electrophysiology of neonatal and adult rabbit atrioventricular node. Am J Physiol 1991; 260: H1674-84. 4) WU MH, Su MJ, Lue HC. Characterization of sodium inward currents and their
responses to lidocaine in immature and mature rabbit ventricular myocytes. JFMA 1993; 92: 103-109.
5) Wu MH, Su MJ, Lu HC. Age-related quinidine effects on ionic currents of rabbit cardiac myocytes. J Mol Cell Cardiol 1994; 26: 1167-77.
6) Wu MH, Su MJ, Sun ASM. Age-related differences in the direct cardiac effects of cisapride: narrower safty range in the hearts of young rabbits. Pediatr Res 2003; 53: 493-9.
7) Kilbon MJ, Fedida D. A study of the developmental changes in outward currents of the ventricular myocytes. J Physiol 1990; 430: 37-60.
8) Case CL, Le FK, McKay CA, Gillette PC, Hewett KW. Developmental effects of d-sotolol on antegrade and retrograde atrioventricular conduction in the rabbit. J Cardiovasc Electrophysiol 1996; 7: 406-14.
9) Truccone NJ, Spotnitz HM, Gersony WM. Comparative cardiovascular effects of propranolol and practolol in puppies. Proc Soc Exp Bio Med 1975; 151: 351-5. 10) Moak JP, Reder RF, Danilo Jr P, Rosen MR. Developmental changes in the
interactions of cholinergic and β-adrenergic agonists on electrophysiologic properties of canine Purkinje fibers. Pediatr Res 1986; 20: 613-8.
11) Young ML, Fournier A, Stolfi A, Pickoff AS. Electrophysiologic effects of intravenous propanolol in the intact immature mammalian heart. Dev Pharmacol Thera 1988; 11: 125-34.
electrophysiologic properties and the β-adrenergic receptor complex in atrial fibers of the canine coronary sinus. Cir Res 1989; 65: 325-33.
13) Feng ZP, Dryden WF, Gorden T. Postnatal development of adrenergic
responsiveness in the rabbit heart. Can J Physiol Pharmacol 1989; 67: 883-9. 14) Yabek SM, Kato R, Ikeda N, Singh BN. Cellular electrophysiologic reponses of
isolated neonatal and adult cardiac fibers to sotalol. J Am Coll Cardiol 1988; 11: 1094-9.
15) Houyel L, Fournier A, Ducharme G, Chartrand C, Davignon A. Electrophysiologic effects of sotolol on the immature mammalian heart. J Cardiovasc Pharmacol 1992; 19: 134-9.
16) Hewett KW, Gaymes CH, Noh CIL, Holani R, Gillete PC. Developmental cellular electrophysiologic effects of propafenone on the rabbit atrioventricular node. Pediatr Res 1992; 32: 658-63.
17) Medkour D, Becker AE, Khalife K, et al. Anatomical and functional characteristics of a slow posterior AV nodal pathway: role in dual pathway physiology and reentry. Circulation 1998;98:164-174.
18) Faber TS, Camm AJ. The differentiation of propafenone from other class Ic agents, focusing on the effect on ventricular response rate attributable to its beta-blocking action. Eur J Clin Pharmacol 1996; 51: 199-208.
19) Musto B, Donofrio A, Cavallaro C, Musto A. Electrophysiologic effects and clinical efficacy of propafenone in children with recurrent paroxysmal supraventricular tachycardia. Circulation 1998; 78: 863-9.
20) Shih JY, Gillette PC, Kugler JD, Garson A Jr, Fukushige J, Zinner A, Driscoll DJ. The electrophysiologic effects of procainamide in the immature heart. Pediatr Pharmacol 1982; 2: 65-73.
21) Anderson JL, Prystowsky EN. Sotalol: an important new antiarrhythmic. Am Heart J 1999; 388-409.
22) Houyel L, Fournier A, Ducharme G, Chartrand C, Davignon A. Electrophysiologic effects of sotalol on the immature mammalian heart. J Cardiovasc Pharmacol 1992; 19: 134-9.
23) Singh BN. Historical development of the concept of controlling cardiac
arrhythmias by lengthening repolarization: particular reference to sotalol. Am J Cardiol 1990; 65:3A-11A.
24) Antonaccio MJ, Gomoll A. Pharmacologic basis of the antiarrhythmic and hemodynamic effects of sotalol. Am J Cardio 1993; 72: 27A-37A.
25) Hohnloser SH, Woosley RL. Sotalol. N Engl J Med 1994; 331: 31-38.
26) Maragnes P, Tipple M, Fournier A. Effectiveness of oral sotalol for treatment of pediatric arrhythmias. Am J Cardiol 1992; 69: 751-4.