國立台灣大學醫學院物理治療學系暨研究所 碩士論文
School and Graduate Institute of Physical Therapy College of Medicine
National Taiwan University Master Thesis
聽覺提示結合跑步機訓練對巴金森氏症患者於大腦皮質興奮 性與步態表現的影響
Effects of Combined Auditory Cues and Treadmill Training on Cortical Excitability and Gait Performance in Parkinson’s Disease
高珮容 Pei-Jung Kao
指導教授:陸哲駒 博士 Advisor: Jer-Junn Luh, Ph.D.
中華民國 107 年 7 月
July 2018
口試委員會審定書
誌謝
回首兩年的研究所生涯,實在感謝許多貴人,有大家的鼓勵支持與幫助,我 的研究生活才能如此充實與順利。
首先,由衷的感謝我的指導教授 陸哲駒老師,不僅鼓勵我思考不同主題的 研究,在研究過程不順遂時,也給予許多支持,從研究架構的形成、實驗過程的 討論到碩士論文的撰寫,每一階段都受到老師很大的幫助與引導,讓我學習用多 方面的角度看事情,從中獲得許多收穫,此外,多虧老師在學術上的提點與生活 上的關心,儘管研究過程辛苦,但是內心很充實,能與陸老師結下師生緣實在太 幸運了!
另外,非常感謝李亞芸老師提供許多寶貴的建議,能接受老師的教導,學習 操作一直以來有興趣的經顱磁刺激並瞭解相關知識,真的很開心,與老師討論的 過程中,每次都是腦力激盪,獲益良多!感謝吳瑞美醫師協助收案與撥空給予意 見,讓我更全面的了解巴金森氏症。也感謝饒紀倫醫師提點在實證醫學領域需要 注意的事項。各位老師們的建議,使論文更臻於完整,十分感謝您們的指導!
能順利的完成研究,還要感謝眾多實驗小幫手們:張綉芸、林昱瑄、李旻 昊、陳雪婷、汪千涵、陳雯柔、許君慈,沒有你們的協助,我的研究就不會如此 順利,謝謝你們!感謝我的學姊張綉芸,謝謝你陪我學習討論、給我打氣與聊天 紓壓,讓我的研究生活增添許多風采!
在此我也要感謝我的家人們、台大老師們、碩士班、大學與高中朋友們,謝 謝你們的關心,給予我心靈支持,讓我陷於失意時推動我向前邁進。也謝謝每一 位受試者熱心的參與,你們是我研究的最大功臣!另外,感謝眾多神明庇佑,讓 我何其有幸身邊充滿貴人!
感謝過去已無法細數的所有協助,期許自己莫忘初衷,繼續在學問洪流中勇 敢向前邁進!
中文摘要
研究背景:巴金森氏症是常見的神經退化性疾病,由於基底核的退化性病變導致巴 金森氏症患者在自動化動作控制上受損,例如:步態失調。臨床上常使用聽覺提示 介入以改善行走步伐變異度高、凍結步態等問題。此外,聽覺提示為基礎的步態訓 練對步態的改善效果可能來自於一系列神經塑性的累積。然而,目前鮮少研究顯示 巴金森氏症患者經過聽覺提示訓練後其神經生理的改變,另外,也少有研究比較聽 覺提示對於有或無步態凍結的巴金森氏症患者之效果。
目的:本研究將探討一次性以聽覺提示為基礎之跑步機訓練對於巴金森氏症患者 神經生理與步態表現的影響,藉由經顱磁刺激評估大腦皮質興奮度來顯示神經生 理之變化。本研究也探討聽覺提示對於有或無步態凍結之巴金森氏症患者是否有 不同影響。
方法:此為隨機交叉試驗,收取 17 位巴金森氏患者(PD),其中 8 位有凍結步態
(FOG),9 位無凍結步態(nFOG),且另收取 9 位健康成年人(Control)作為對照組參
與本試驗,每組皆以隨機順序接受兩種情形之介入,兩次訓練中間會相隔至少一星
期,兩次訓練分別為30 分鐘之以聽覺提示為基礎之跑步機訓練(AC condition)和沒
有聽覺提示之跑步機訓練(NC condition)。每位受試者將接受介入前和介入後的評
估。主要評估指標為大腦皮質興奮度,次要評估指標為舒適與最快行走速度下的走 路表現。
統計分析:使用變異數分析(analysis of variance)檢測組間介入前、後之變化。
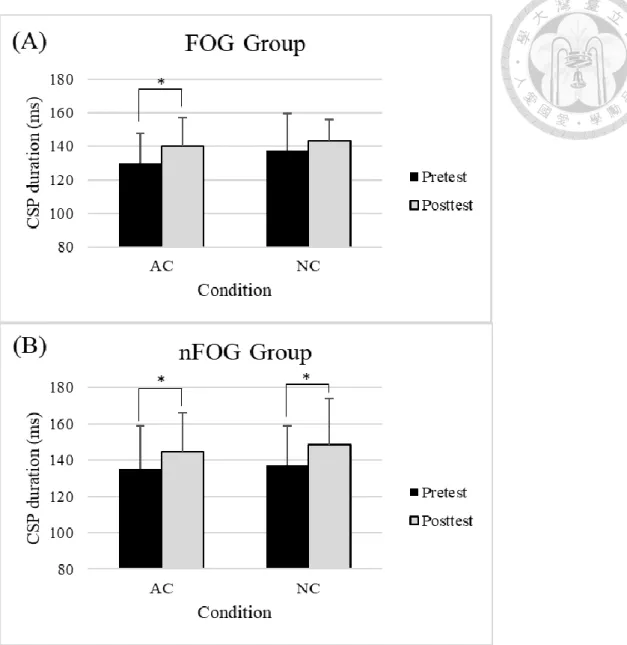
結果: 在大腦皮質興奮度方面,無論有無聽覺提示,巴金森氏症患者相較於健康 人在接受訓練後其皮質寧靜期(cortical silent period, CSP)顯著延長(p<0.001),有凍
結 症 狀 組 只 有 在 合 併 聽 覺 提 示 訓 練 後 有 顯 著 延 長 的 現 象(AC: p=0.032; NC:
p=0.257),而無凍結步態組無論有無聽覺提示介入,其皮質寧靜期都有顯著延長(AC:
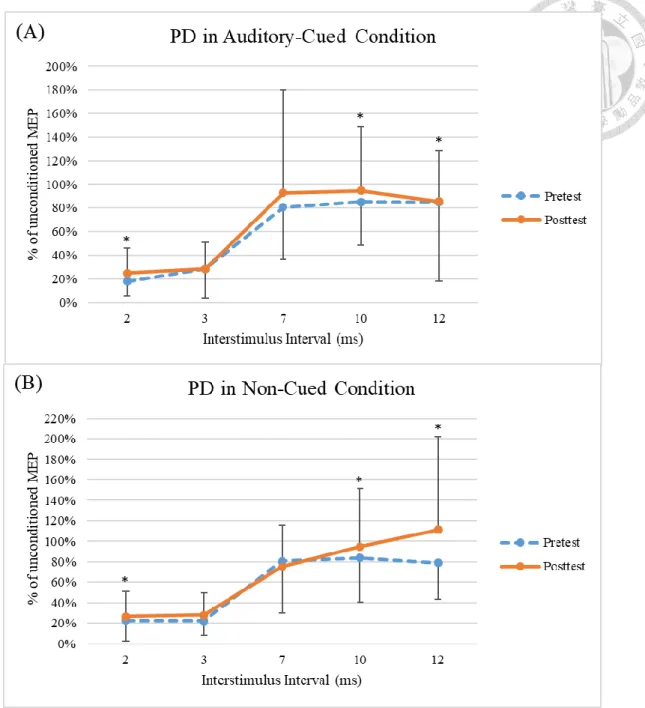
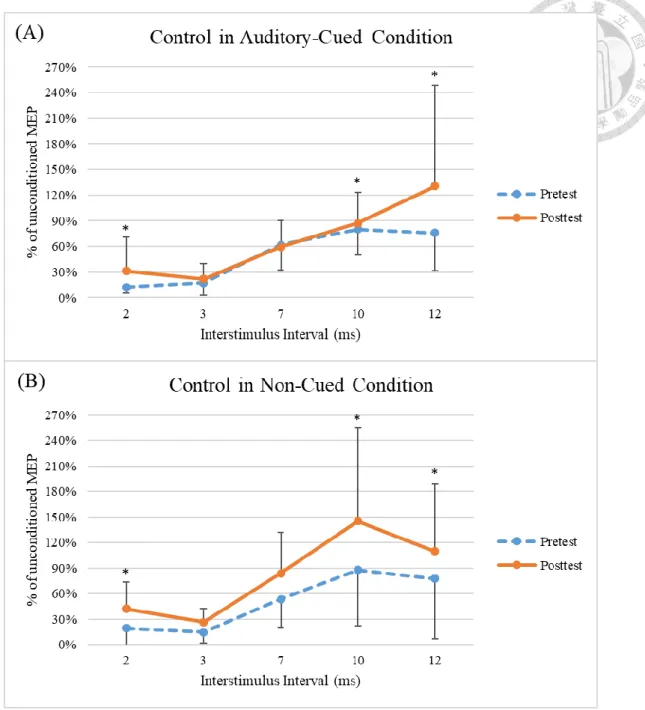
p=0.007; NC: p=0.008)。無論有無聽覺提示,巴金森氏症患者與健康人在經過訓練 後,顯著減少刺激間距兩毫秒的皮質內抑制(short intracortical inhibition, SICI)以及 增加刺激間距十、十二毫秒的皮質內促進(short intracortical facilitation, ICF),然而
有和無凍結步態組在皮質內抑制與促進方面,經過無論有無聽覺提示的訓練後並 無顯著差異。在步態表現方面,無論有無聽覺提示,巴金森氏症患者與健康人在訓 練後顯著增加舒服行走速度(p=0.006)與步長(p<0.001),此外,無論有無聽覺提示,
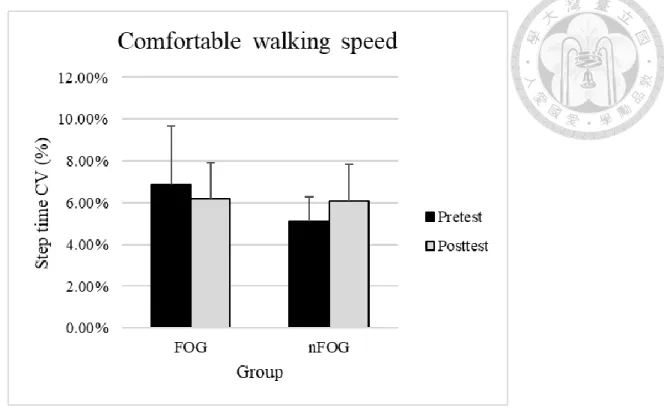
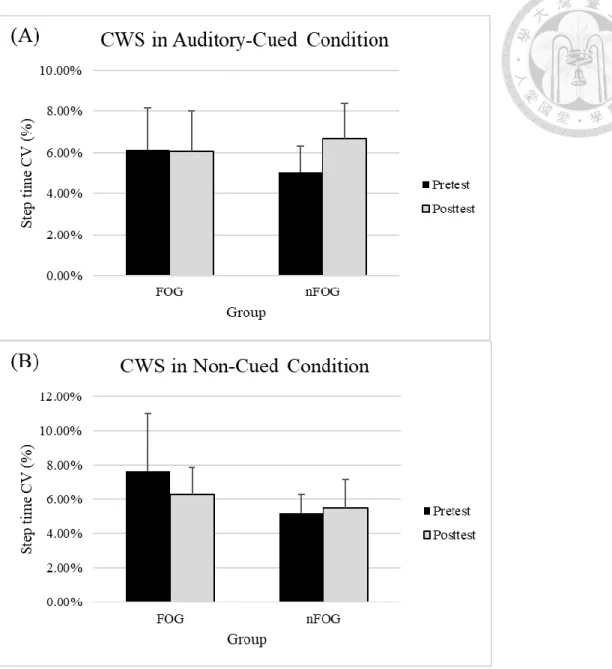
有 凍 結 步 態 組 與 無 凍 結 步 態 組 經 過 訓 練 後 , 皆 顯 著 增 加 其 舒 服 行 走 的 步 長 (p=0.002),在舒服行走步伐變異度方面,無論有無聽覺提示介入,有凍結步態組經
過訓練後,其行走步伐變異度有下降趨勢,而無凍結步態組則呈相反趨勢。
結論: 一次性的跑步機訓練無論有無結合聽覺提示,可以調控巴金森氏症患者之
大腦皮質興奮度並且增加舒服行走時的步長與速度。聽覺提示結合跑步機訓練能 增強有或無凍結步態者的皮質脊髓抑制,然而,有凍結步態者若接受沒有聽覺提示 的跑步機訓練則沒有顯示此效果。
關鍵詞:巴金森氏症、聽覺提示、經顱磁刺激、皮質興奮度、步態、跑步機訓練
Abstract
Background: Parkinson’s disease (PD) is a common neurodegenerative disorder.
Dysfunction of dopaminergic cells in basal ganglia leads to deficits in the automatic execution of movements such as gait disturbances. Auditory cues are often used in clinical setting and revealed benefits in ambulation. Moreover, the effects of cueing-based training on gait pattern might come from the accumulation of a series of neuroplasticity through serial motor training. However, current studies provided little information on the changes of neuroplasticity after the patients with PD carried out the cued-based training.
Furthermore, it is still uncertain whether PD with or without freezing of gait (FOG) can achieve equal favorable effects from auditory cues.
Purpose: The present study is to investigate the effects of auditory-cued treadmill
training for a single session on the neurophysiology and gait performance in patients with PD. Neurophysiology will be evaluated the cortical excitability through transcranial magnetic stimulation (TMS). The study will further explore whether any different effects of auditory cues between freezers and non-freezers.
Methods: This is a crossover study. Freezers (FOG, n=8), non-freezers (nFOG, n=9), and
healthy subjects (control, n=9) were recruited in this study. Each subject randomly carried out training with two condition with at least one-week washout interval. Two conditions were 30-minutes of treadmill training with (AC condition) and without rhythmic auditory
cues (NC condition). All subjects received the baseline and post-treatment assessments.
Primary outcome measures included the cortical excitability and the secondary outcome measures included the gait performance in both comfortable and fast walking speed.
Statistical analysis: Repeated measure analysis of variance (RM-ANOVA) was used to
determine differences of mean scores of the dependent variables between groups under two condition. The statistical significance was set at P<0.05.
Results: PD subjects compared to healthy subjects revealed lengthened CSP duration
after training whether with or without auditory cues (p<0.001 and p=0.392, respectively).
Significantly increased CSP duration in AC condition (p=0.032), but not in NC condition (p=0.257) for the FOG group was found. The nFOG group presented significantly lengthened CSP duration in both AC and NC condition (p=0.007 and p=0.008, respectively). Both PD and control groups reduced SICI(2ms), increased ICF(10ms), and ICF(12ms) after training whether with or without AC (p=0.003, p=0.009, and p=0.009, respectively), but the FOG and nFOG did not show significant differences in SICI and ICF after training. For the gait performance in comfortable speed, PD and control group showed increased speed (p=0.006) and stride length (p<0.001) after training whether with or without AC. Moreover, both the FOG and nFOG group increased stride length (p=0.002) after treadmill training whether with or without auditory cues. The step time
CV in the FOG group presented a downward tendency after training, whereas the non- freezers presented an opposite picture.
Conclusion: One-session treadmill training whether with or without auditory cues played
a major role in modulated cortical excitability, increased step length, and gait velocity in comfortable walking speed for patients with PD. The auditory cues with treadmill training enhanced the corticospinal inhibition in both freezers and non-freezers. However, this phenomenon cannot be found in freezers when they received treadmill training without cues.
Keyword: Parkinson's disease, auditory cueing, transcranial magnetic stimulation, cortical excitability, gait, treadmill training
LIST of ABBREVIATIONS
AC auditory cues
BGTC ganglia-thalamocortical network CNS central nervous system
CSP cortical silent period
CTC cerebellar-thalamocortical network CV coefficient of variation
CWS comfortable walking speed EEG electroencephalography
EMG electromyogram
FOGQ Freezing of gait Questionnaire FWS fast walking speed
GABA γ-aminobutyric acid
GPi internal segments of the globus pallidus GPe external segments of the globus pallidus ICF intracortical facilitation
ISI interstimulus intervals
M1 primary motor cortex
MEPs motor evoked potentials
MMSE Mini-Mental State Examination
MT motor threshold
NMDA N-methyl-D-aspartate
PD Parkinson’s disease
PET positron emission tomography
RM-ANOVA repeated measure analysis of variance rTMS repetitive transcranial magnetic stimulation SICI short intracortical inhibition
SIP stepping-in-place
SMA supplementary motor area SNr substantia nigra pars reticulata TMS transcranial magnetic stimulation
UPDRS Unified Parkinson's Disease Rating Scale
CONTENTS
口試委員會審定書 ... i
誌謝 ... ii
中文摘要 ... iii
Abstract ... v
LIST of ABBREVIATIONS ... viii
FIGURES ... xiii
TABLES ... xiv
APPENDICES ... xv
Chapter 1 Introduction ... 1
1.1 Background ... 1
1.2 Purpose and significance ... 5
1.3 Hypotheses ... 7
Chapter 2 Literature Review ... 9
2.1 Introduction of Parkinson’s disease ... 9
2.3 Treadmill training for patients with Parkinson’s disease ... 19
2.4 Transcranial magnetic stimulation ... 23
2.5 Summary of review ... 28
Chapter 3 Methods ... 31
3.1 Study design ... 31
3.2 Subjects ... 31
3.3 Procedure ... 32
3.4 Interventions ... 33
3.5 Outcome measurements ... 34
3.6 Statistical analysis ... 38
Chapter 4 Results ... 39
4.1 Demographics and baseline characteristics of patients and healthy adults ... 39
4.2 Transcranial magnetic stimulation ... 40
4.3 Gait performance ... 41
Chapter 5 Discussion ... 44
5.1 Effects of auditory-cued treadmill training on cortical excitability ... 44
5.3 Treadmill may act as another external cues ... 49
5.4 Impact of the interventional duration on the effects of the auditory-cued treadmill training ... 50
5.5 Clinical implication ... 52
5.6 Limitation and future study ... 53
Chapter 6 Conclusion ... 55
References ... 56
FIGURES
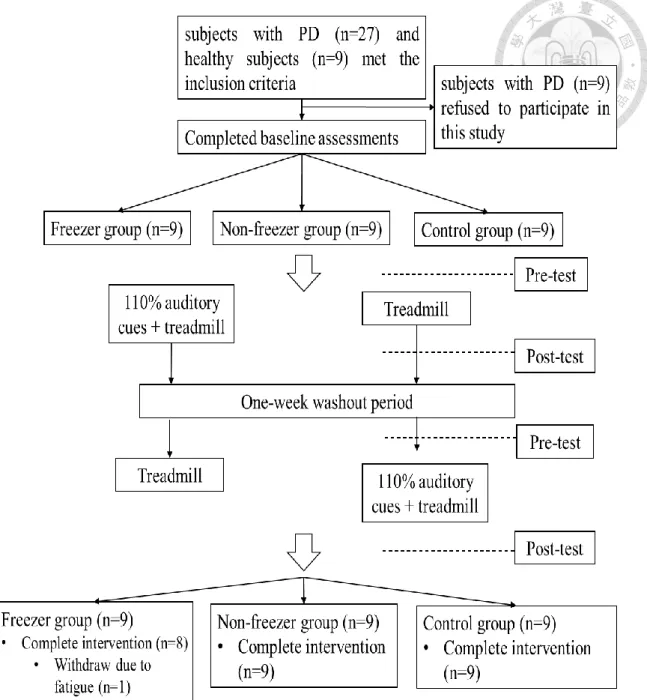
Figure 1. Flowchart of the study ... 70
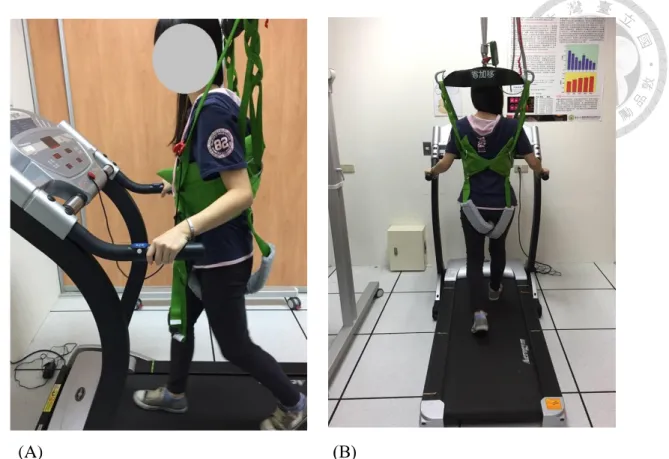
Figure 2. Treadmill training from (A) lateral view, and (B) posterior view ... 71
Figure 3. Transcranial magnetic stimulation (TMS). ... 72
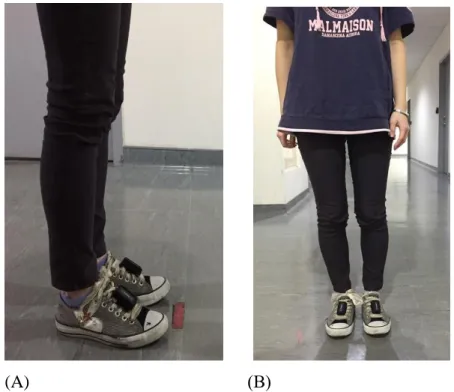
Figure 4. The placement of the inertial sensor system Physilogs® on the subject from (A) lateral view, and (B) anterior view ... 73
Figure 5. Paired-pulse TMS in the PD group (A, B). ... 74
Figure 6. Paired-pulse TMS in the control group (A, B). ... 75
Figure 7. Paired-pulsed TMS in the freezer (A, B) and non-freezer group (C, D). ... 76
Figure 8. CSP duration in the freezer (A) and non-freezer (B) group ... 77
Figure 9. Step time CV of CWS in the freezer and non-freezer group ... 78
Figure 10. Step time CV of CWS in the freezer and non-freezer group under AC (A) and NC (B) condition ... 79
TABLES
Table 1. Summary of the cortical excitability in PD ... 80
Table 2. Demographics and clinical characteristics of healthy subjects and patients with Parkinson’s disease ... 81
Table 3. Single-pulse TMS in PD and control group... 82
Table 4. Single-pulse TMS in freezers and non-freezers group ... 83
Table 5. Paired-pulse TMS in PD and control group... 84
Table 6. Paired-pulse TMS in freezers and non-freezers group ... 85
Table 7. Gait performance with comfortable walking speed in PD and control group .. 86
Table 8. Gait performance with comfortable walking speed in freezers and non-freezers group ... 87
Table 9. Gait performance with fast walking speed in PD and control group ... 88
Table 10. Gait performance with fast walking speed in freezers and non-freezers group ... 89
Table 11. Comparison of PD and control group in cortical excitability and gait performance ... 90
APPENDICES
Appendix A. Clinical trial/research approval ……….91 Appendix B. Informed consent form………...93 Appendix C. Safety questionnaire of Transcranial Magnetic Stimulation (TMS) …...103
Chapter 1 Introduction
1.1 Background
Parkinson’s disease (PD) is a common neurodegenerative disorder due to a dopaminergic deficiency in the basal ganglia.1 The prevalence of PD rises as a growth of aging population. Approximately 0.5-1% of the population ranged from 65 to 69 years of age and rising to 1-3% among people who are older than 80 years of age.2 Dysfunction of dopaminergic cells in basal ganglia leads to deficits in internal timing and automatic execution of movements3,4 such as gait disturbances, which are the hallmark of PD.
Parkinsonian gait is characterized by small stride length, decreased gait speed, increased cadence, increased percentage of double leg support, absence of arm swing, and increased stride-to-stride variability.5-8 Freezing of gait (FOG) is one of the disabling gait disturbances and defined as “brief, episodic absence or marked reduction of forward progression of the feet despite the intention to walk.”9-11 Freezers exhibits more gait instability, which related to stride time variability,12-15 than non-freezers.6
In order to ameliorate the impaired automatic motor performance, the pharmacological management is the primary way and has the capability to relieve certain symptoms; however, motor complications occur after long-term use of medicine, which should not be ignored. Rehabilitation such as physical therapies remains important for
patients with PD to gain function and decrease the rate of functional decline.
So far, overground gait training with external cues and treadmill training are the common interventions to improve gait disturbances attributed to dysfunction of motor automaticity. Auditory cues are widely applied in clinical studies or practice for PD.
Auditory cues provide an external rhythm that bypasses the internal rhythm deficits to prompt more appropriate gait pattern.16,17 Abundant studies revealed the utilization of auditory cues facilitates the normalization of gait performances in PD such as reduced gait variability and increased stride length.18,19 However, according to Willems et al.,7 different effects on improved step length were noted in freezers and non-freezers when they received different frequency of auditory cues. It seems that the freezers and non- freezers may exhibit the different responses in gait to the auditory cues. Insufficient studies investigate that the different responses to the auditory cues in freezers and non- freezers. We are still uncertain whether both types of patients can achieve equal favorable effects on gait performance from auditory cues.
Recently, there has been growing interest in combined auditory cues with treadmill training. Since treadmill training is another common and beneficial intervention to normalize the spatiotemporal gait parameter for PD, cues applied during treadmill walking may potentiate more positive effects on gait in PD compared to traditional intervention.20,21 Despite this, we are still unclear these different effects of cued treadmill
training between freezers and non-freezers due to scarcer studies.
After having realized the effects of cueing-based training on gait pattern, it is necessary to dig into how these effects come from and what is the potential mechanism behind the auditory cues. According to the mechanism of learning-induced cortical plasticity in the primary motor cortex (M1), it hypothesized that synaptic plasticity could be modulated through long-term potentiation (LTP) and long-term depression (LTD) depend on different stimuli.22 An animal study had shown these neurophysiological changes after training is associated with improved motor performance.23 Moreover, training-induced plasticity may be important to the rehabilitation.24Based on the previous research, some neuroplastic changes in the brain might occur before the behavioral changes response to the auditory-cued training. One Positron Emission Tomography (PET) study25 revealed significant metabolic increment in the cerebellum, parietal and temporal lobes after the patients with PD carried out the auditory cueing-based physical rehabilitation program. Nevertheless, gait parameters except for stride time variability after training did not differ from those obtained before training. It seems that neuroplasticity through cueing-based training plays a crucial role to improve gait disturbances for PD.
In order to explore the neuroplastic effects of cueing-based training in patients with PD, the application of the neuronal imaging techniques is needed. The common neuronal
imaging techniques for the human to demonstrate neuroplasticity include positron emission tomography (PET), electroencephalography (EEG), and transcranial magnetic stimulation (TMS). Compared to PET and EEG, TMS parameters can be rapidly acquired and provide close monitoring of relatively short-duration neuroplastic changes following experimental manipulation. TMS explore the neuroplasticity as measured through the cortical excitability. Previous studies indicated the patients with PD exhibited abnormal cortical excitability including the reduced cortical silent period (CSP) and a failure of intracortical inhibition.26 Therefore, it is worth for us to dig into whether auditory cued- based training has an impact on cortical excitability.
Based on our previous laboratory experiment,27 for the cortical excitability, we investigated significantly lengthened CSP duration and reduced short intracortical inhibition (SICI) at 2ms after PD subjects received stepping-in-place (SIP) training with auditory cues (AC) but not without cues. Additionally, the freezers in comparison of the non-freezers achieved more plastic changes in CSP duration and SICI(2ms) after SIP training with AC. Concurrently, the freezers obtained significantly decreased walking step time CV after training. These findings suggested some changes in neuroplasticity and behavioral performance occurred after training with AC and the freezers and non-freezers may have different responses to the AC. Despite this, SIP is unlike walking, which needs to provide the forward propulsion. We cannot draw the firm conclusion that whether the
auditory-cued treadmill training could provide similar effects on the cortical excitability and gait performances in freezers.
In general, gait disturbances that related to the dysfunction of automatic motor execution is a major problem for the patients with PD, especially in freezers. Training- induced plasticity may play a crucial role in gait rehabilitation in PD. Therefore, it is worth for us to investigate whether the cortical excitability can be modulated through auditory-cued treadmill training and explore whether any improvement in gait performance after training.
1.2 Purpose and significance
So far, the majority of studies regarding the utilization of auditory cues in PD have focused on overground walking and long-term training for several weeks. Among these studies, the favorable effects of auditory cues on gait were well documented. Moreover, recently, there has been growing interest in the application of auditory cues combined with treadmill walking due to better gait pattern during treadmill walking compared with overground walking. According to the animal study regarding the mechanism of learning- induced cortical plasticity in the primary motor cortex (M1), we may believe that the improvements in gait performances after cueing-based training come from the accumulation of series of neuroplasticity through serial motor training. Thus,
neuroplasticity through motor training may play a crucial role for the patients with PD to improve their gait performances. However, current studies provide little information on the changes in neuroplasticity after the patients with PD carried out the cued-based training. It is uncertain that if any neurophysiological changes occur following the one- session cueing-based training. To explore the neuroplasticity in the human cortex, transcranial magnetic stimulation (TMS) is applied to demonstrate the cortical plasticity.
The potential mechanism behind auditory cues through observing the neurophysiological and behavioral changes in response to auditory-cued training can be explored in this study.
We can also gain further insight into the different effects of auditory cues in freezers and non-freezers by comparing the results from two types of patients. Therefore, we can choose the appropriate intervention when we apply the auditory cues according to the existence of freezing of gait.
The aims of this study are: (1) to investigate the effects of auditory-cued treadmill training for a single session on cortical excitability in patients with PD; (2) to investigate the effects of auditory-cued treadmill training for a single session on gait performance in patients with PD; (3) to explore whether any different effects of auditory cues on cortical excitability between freezers and non-freezers; (4) to explore whether any different effects of auditory cues on gait performance between freezers and non-freezers
1.3 Hypotheses
Single session training was used in this study. Therefore, it was considered that the changes in the cortical excitability may be more apparent compared with the changes in gait performances. Furthermore, step time variation, which may relate to the gait stability, in freezers is more impaired than that in non-freezers. Thus, freezers might obtain more benefits from auditory-cued training than non-freezers.
Aim 1: Whether the auditory-cued treadmill training could significantly alter the cortical
excitability in PD subjects.
Hypothesis: Compared with treadmill training alone, the auditory-cued treadmill training will significantly alter the cortical excitability in PD subjects than in healthy subjects
Aim 2: Whether the auditory-cued treadmill training could significantly reduce step time
variation and improve gait pattern in PD subjects.
Hypothesis: Compared with treadmill training alone, the auditory-cued treadmill training
will significantly reduce step time variation and improve gait pattern in PD subjects than in healthy subjects
*Gait pattern include walking speed, cadence, and stride length
Aim 3: To determine whether auditory-cued treadmill training has different changes in
cortical excitability between freezers and non-freezers.
Hypothesis: Compared with treadmill training alone, the auditory-cued treadmill training
would have changes in the cortical excitability in both types of patients, and freezers may achieve more alternation than non-freezers.
Aim 4: To determine whether auditory-cued treadmill training has different effects on
step time variation and gait pattern between freezers and non-freezers.
Hypothesis: Compared with treadmill training alone, the auditory-cued treadmill training would have favorable effects on step time variation and gait pattern in both types of patients, and freezers may achieve more benefits than non-freezers.
Chapter 2 Literature Review
2.1 Introduction of Parkinson’s disease
2.1.1 Pathophysiology and symptoms
The basal ganglia are a group of subcortical nuclei and they organized connections with external structures such as the basal ganglia-thalamocortical circuit (BGTC).1 The basal ganglia is considered as a primary substrate for motor learning and controlling behavioral output (e.g., temporal information processing3 and automatic motor control).4
Parkinson’s disease (PD) is the progressive neurological degenerative disorders attributed to dysfunction of dopaminergic neurons in the basal ganglia.28 The cardinal symptoms of Parkinson’s disease are rigidity, bradykinesia, tremor, and postural instability.29 Progressive dopamine deficiency leads to the disturbance of internal rhythmic control and deficits in automatic motor performance such as impaired balance control and gait disturbances, which related to the risks of fall.30 Additionally, since the basal ganglia have connected to widespread cortical areas, other non-motor symptoms will occur as the disease progressing. These non-motor features contain mood, cognitive problems, sleep disorders, pain, and autonomic disorders, which cause a decline in the quality of life.31
2.1.2 Prevalence and incidence
Parkinson's disease is the second common neurodegenerative disorder in the elderly.32 Age is the greatest risk factor for developing PD. The prevalence of Parkinson's disease is approximately 0.5-1% of the population older than 65 years of age and rising to 1-3% among people who are older than 80 years of age.2 Moreover, the prevalence of Parkinson's disease seems higher in Europe and North America compared to Asia and Africa.33 Gender is another risk factor, with the male-to-female ratio being about 3:2.34 In Taiwan, the prevalence of Parkinson's disease is 159.8-299.3 per 100,000 and the incidence is 33.5-36.6 per 100,000 in 2002 to 2009.35 Despite the relatively low prevalence of Parkinson's disease in Asian area, it is still a crucial issue due to the increasing prevalence and incidence in Taiwan.
2.1.3 Freezing of gait
Gait disturbances are the most common complication in patients with PD.
Approximately 7% of patients with recently diagnosed of PD36 and 47% of patients with PD suffer from freezing of gait (FOG).37 FOG is defined as “brief, episodic absence or marked reduction of forward progression of the feet despite the intention to walk.”9-11 There are three different patterns of FOG: (1) trembling in place: alternating tremor of the legs at a frequency of 3–8 Hz;38,39 (2) shuffling forward with small steps; (3) complete
akinesia: no observable motion of the limbs or trunk.11 The third type occurs in low incidence.40 Patients with FOG would feel as if their feet are glued to the floor. This symptom commonly lasts for several seconds, but the episodes may occasionally exceed 30s.40 Furthermore, FOG is most commonly observed in the “off” state.41 It increases the risk of falling.9
The pathophysiology of FOG is multifactorial and still not well understood. Most studies classified freezers and non-freezers based on their subjective descriptions of FOG, such as assessed by the New Freezing of Gait Questionnaire (NFOG-Q).42,43
2.1.4 Gait patterns in freezers and non-freezers
Dysfunction of dopaminergic cells in basal ganglia circuit affects motor automaticity, such as walking.4 The features of Parkinsonian gait include decreased gait speed, increased cadence, small stride length, increased percentage of double leg support, absence of arm swing, and increased stride-to-stride variability.5-8 Among these gait parameters, stride time variability might be considered as the quantitative evaluation of gait instability, since stride time variability is found to be a parameter associated with risk of fall rather than gait speed and stride length.5,6,13,15 Therefore, The larger stride time variability, the more gait instability for patients with Parkinson’s disease.
FOG is a sudden and transient gait disturbance. The cumulative loss of stride length
and increased cadence are showed before FOG starts to occur.44 Chee et al.45 also demonstrated that decreased step length is a precursor of FOG. In this study, freezers who walk on the ground in 100%, 75%, 50%, and 25% of their preferred stride length showed significantly decreased step length and increased step variability compare to non-freezers who walk in the same condition. The gait performance of non-freezers is similar to healthy elders in those conditions. Additionally, between FOG episodes, cadence appears to be similar in freezers and non-freezers whether they are during "on" or "off" medication.
However, there is a significantly increased stride time variability in freezers compared to non-freezers regardless of medication.6 The higher stride time asymmetry in freezers than in non-freezers is also revealed by Plotnik et al.46 According to the aforementioned findings, a capability of regulating stride time variation in freezers is more impaired than that in non-freezers.
2.2 External cueing as rehabilitative strategy
2.2.1 Auditory cues versus visual cues
Despite the positive effects of pharmacological management for Parkinsonian gait, it still has the side effects and limitation that should not be ignored. Behavioral strategies remain important for patients with PD. As we mentioned above, PD has impaired automaticity of motor control. Behavioral strategies may shift patients' automatic motor
control to the goal-directed way.47 External cues, which provide the references for the execution of movement, are the common behavioral strategies for patients to allocate their attention to gait.
External cues contain stimuli of temporal and spatial aspect and they may prompt more appropriate movement timing and amplitude of gait. Auditory cues and visual cues are temporal and spatial stimuli, respectively. A meta-analysis of 25 studies demonstrated auditory cues may provide positive effects in gait speed, cadence, and stride length;
whereas visual cues only improve stride length.48 Although two kinds of stimuli can elicit positive effect in stride length, which is consistently decreased in patients with PD, auditory cues seem more consistent and beneficial in gait performance than visual cues.
This result is the same with the previous review.49 Additionally, comparing the effects of auditory cues to visual cues on gait stability, auditory cues are the effective stimuli to reduce stride time variability, especially for patients in Hoehn and Yahr III to IV.19
2.2.2 Effects of auditory cueing on gait for patients with PD
Auditory cues provide the temporal stimuli to regular the timing of gait and coordination of limbs. It is cost efficient and easy to implement. It can be delivered by verbal counting, musical beats, or metronome. There are abundant studies investigated the effects of auditory cue on gait in patients with PD.
Previous study showed that when patients with PD walked combined with auditory cues, the cadence, step length, and stride time variability are significantly improved than patients walked without cues.19 Furthermore, auditory cues have immediate effect on gait.
Hausdorff et al.18 instructed patients with PD walking with auditory cues at 100% or 110%
of their usual cadence and then immediately evaluated their gait performance without cues. Both frequency of auditory cues improved gait speed and stride length in patients even when cues were removed, but it did not influence gait parameters in healthy elderly.
These effects lasted for 15 minutes.
In terms of interventional studies, they combined auditory cues with ground walking or other physical therapies as training.50,51 The interventional period ranged from one week to eight weeks. All of them demonstrated the beneficial effect on gait in patients with PD after a period of training. However, the frequency of auditory cues applied in these studies did not consistent. Although the therapeutic effects would be influenced by different frequency, insufficient studies demonstrated which frequency is the best.
2.2.3 Different response of auditory cueing in freezers and non-freezers
Although the effects of auditory cues on gait in PD are well documented, the literature assessing the role of auditory cues on FOG are scarcer and controversial. Cubo et al.52 studied the effects of auditory cues at 100% of usual cadence on FOG in PD during
"on" medication. Results demonstrated there was no significant difference in the freezing time, average freezing duration, and numbers of freezes between the freezers walking with and without auditory cues. However, since 1996, Enzensberger and Fischer have found a significant reduction in the number of freezing episodes on straight walking when patients walked with metronome during "on" medicine.53 Another study also showed the presence of auditory cueing at 110% of preferred walking cadence led a significantly reduced number and duration of freezing episodes in freezers during end of dose-period.8 Furthermore, the different response of auditory cueing in freezers and non-freezers might be influenced by different task. Based on our previous laboratory experiment,54 non- freezers revealed improved coefficient of variance in fast tapping after auditory-cued tapping training, but not in freezers
Due to the multifactorial nature of FOG, the freezers and non-freezers may exhibit the different responses on gait to the auditory cues. According to Willems et al.,7 they investigated the effects of auditory cues on gait in the freezers and non-freezers during
“on” period. All patients respectively walked with auditory cues at five different frequencies including 80%, 90%, 100%, 110%, and 120% of preferred walking cadence.
Results revealed there was no difference in gait speed and stride length between the freezers and non-freezers under different cued conditions. However, they further investigated the gait performance across different cued frequency in each group. For the
freezers, although their gait speed improved under higher cued frequencies, they performed decreased stride length in 110% cued condition and had larger stride length in 90% condition. Whereas, for the non-freezers, 110% of usual cadence was suitable for them to increase speed and stride length. Due to the small sample size in this study and fewer studies regarding the auditory cues response between the freezers and non-freezers, more evidence is needed to make a clear conclusion.
From the previous literature, it can be seen that the frequency of cueing seems plays an important role in gait for the freezers and non-freezers. Additionally, lack of study investigates the effect of auditory cues on gait instability in the freezers and non-freezers during "off" medication.
2.2.4 Potential mechanism behind auditory cues
Previous sections have demonstrated the clinical effects of auditory cues. It is now necessary to investigate the possible mechanism underlying this effect of auditory cues.
Brain areas, such as the basal ganglia, cerebellum, supplementary motor area (SMA), pre- SMA, and premotor cortex, involved in accurate temporal processing that closely related to rhythmical movements.55 Moreover, there are two brain networks involved in timing movements. One is the basal ganglia–thalamocortical network (BGTC), which is in charge of self-generated movements and attention-dependent evaluation of temporal
intervals. The other network is cerebellar–thalamocortical network (CTC), which is responsible for matching movements to the external cues.17 The BGTC network is disrupted in PD due to dysfunction of dopaminergic cells in basal ganglia circuit; whereas, the CTC network spared or is affected lately in PD. Therefore, the beneficial effects of auditory cues may be attributed to driving the residual activity of the BGTC network or compensatory mechanism from the CTC network.16,17 For the evidence of the compensatory mechanism, del Olmo et al.25 displayed that not only improvement of gait variability but also enhanced activity of the anterior cerebellum lobe were noted after PD patients received cueing-based physical rehabilitation program for 4 weeks.
Moreover, the central nervous system (CNS) is a dynamically changing system. CNS is capable of adaptation and modification according to the externally environmental inputs, efferent demands, and behavioral influences. Based on the mechanisms of learning-induced cortical plasticity in M1, it was hypothesized that long-term potentiation (LTP) and long-term depression (LTD), which have been termed synaptic plasticity, could modify the synaptic strength of cortical connections depend on the different pattern of stimulation used. LTP and LTD describe the long-lasting enhancement or attenuation in synaptic strength respectively.22 According to the animal study, results revealed rats achieved a performance with few errors in the reach, grasp or retrieval actions after training, additionally, less LTP was induced from the trained M1, whereas normal levels
of LTP was induced from the untrained M1.23 That is, neuroplasticity through motor training was associated with improved motor performance. In human, training-induced plasticity accompanying by improved motor performance has been demonstrated.56,57 Furthermore, based on the previous research, some neuroplastic changes in the brain might occur before the behavioral changes response to the auditory-cued training. One Positron Emission Tomography (PET) study revealed significant metabolic increment in the cerebellum, parietal and temporal lobes after the patients with PD carried out the auditory cueing-based physical rehabilitation program.25 Nevertheless, gait parameters except for stride time variability after training did not differ from those obtained before training. According to the aforementioned, we may believe that the improvements in motor performances after cueing-based training is associated with the accumulation of series of neuroplasticity through serial motor training.
To explore the neuroplasticity in the human cortex, the application of the neuronal imaging techniques are needed. The common neuronal imaging techniques for human to demonstrate neuroplasticity include positron emission tomography (PET), electroencephalography (EEG), and transcranial magnetic stimulation (TMS). Among them, TMS explore the neuroplasticity as measured the cortical plasticity. Delvendahl and colleagues58 suggested that increased and decreased MEP amplitude, which reflects the strength of synaptic transmission, were assumed to present LTP-like or LTD-like synaptic
plasticity of motor cortex output neurons. However, lack of studies provide the changes of neuroplasticity after the patients with PD carry out the cued-based training. It is uncertain that if any neurophysiological changes occur following the one-session cueing- based training. Through the application of TMS, we can further investigate whether any neuroplasticity occurs before the behavioral improvements.
Overall, despite few studies regarding the mechanism behind auditory cues, the neural mechanism of the beneficial effects of auditory cues might be through the CTC network to compensate the dysfunction of basal ganglia. Furthermore, neuroplasticity induced by motor training may play a crucial role for the patients with PD to improve their gait performances. Thus, the study of the neurophysiological changes has become an important aspect of understanding the effects of auditory cues for PD.
2.3 Treadmill training for patients with Parkinson’s disease
2.3.1 Effects of treadmill training on behavior performance
Treadmill training is another common intervention for PD to improve gait performance. For the immediate effects, Pohl and colleagues59 revealed that one session of treadmill training without body weight support for 30 minutes could improve gait speed and stride length in PD; whereas, the conventional gait therapy could not. Then Bello and colleagues60 further investigated the effects of one session of treadmill training on gait in
moderate and advanced PD during “on” medication. They reported that one session of treadmill training for 20 minutes significantly increased overground gait speed and step length, especially in advanced patients (Hoehn and Yahr stage 3). These effects maintained for 5 and 10 minutes after a treadmill session. However, stride time variability did not change after treadmill walking in ether moderate or advanced patients. The speed of treadmill in the above studies was set at each participants’ self-selected comfortable speed. For the long-term effects of treadmill programs, they demonstrated the beneficial effect on gait speed and stride length in patients with PD after a period of training, which ranged from four weeks to eight weeks.61,62 Although some treadmill training in above studies had weight bearing support, Toole and colleagues63 reported the degree of weight bearing may not be crucial to achieving benefits of gait in patients with PD.
In general, these findings suggest that the treadmill training has therapeutic effects on gait in PD.
2.3.2 Effects of combined treadmill training and cueing (AC, VC, FOG)
Impaired internal rhythmic control, which is related to a dopaminergic deficiency of the nigrostriatal pathway, leads to the higher cadence, shorter step length, and higher stride time variability in PD. The auditory cues can bypass the dysfunctional neural network to improve the cadence, step length, and stride time variability in PD.
Additionally, treadmill training can also act as an external cue to normalize the spatiotemporal gait parameter in PD.64 As the patients with PD rely on allocating their attention to gait in order to modulate gait performances, the application of treadmill combined with auditory cues may potentiate positive effects on gait in comparison to single intervention alone.
Research by Chaiwanichsiri and colleagues,21 they recruited thirty PD subjects and randomly allocated to three groups. One group received treadmill training with music cue for three days a week and home walking program for three days a week (group A).
Another group received treadmill training alone for three days a week and home walking program for three days a week (group B). The other group received home walking program for six days a week (group C). The period of intervention was four weeks and followed by self-practice for other four weeks. The results indicated a significantly increased overground step length in group A. Group A had more step length than group B and C, and the effects maintained to the end of the eighth week. However, this study did not report the effects of the combined intervention is the same in freezers as well.
Only one study revealed the effects of treadmill training combined with auditory and visual cues in freezers. Frazzitta and colleagues20 recruited forty PD subjects with FOG and randomly assigned into two groups. One group received treadmill training associated auditory and visual cues, and the other group received overground walking associated
auditory and visual cues. Each group carried out training for 20 minutes every day for four weeks. The resulted demonstrated both groups had significant improvements in Unified Parkinson’s Disease Rating Scale Motor Section (UPDRS III), Freezing of Gait Questionnaire (FOGQ), 6-minute walking test (6MWT), and gait speed. Cues associated with treadmill provided more improvements in UPDRS III, FOGQ, 6MWT, and gait speed than cues without treadmill. This study suggested the treadmill training associated with auditory and visual cues might provide better effects on gait in freezers compared to conventional treatments.
Although the intervention in Frazzitta et al20 includes visual cues, this finding still give the possibility that freezers might obtain more positive effects from auditory cues combined with treadmill training. So far, lack of study investigates the different effects on gait between the freezers and non-freezers when they received treadmill training with auditory cues. The study regarding the effects of these interventions through neurophysiologic assessment is scarce. Therefore, more studies are needed to investigate whether there are differences in the neurophysiology and gait performance between the freezers and non-freezers after treadmill training with auditory cues.
2.4 Transcranial magnetic stimulation
2.4.1 Introduction of transcranial magnetic stimulation (TMS)
In 1985, Barker and his colleagues65 introduced transcranial magnetic stimulation (TMS) as a safe and non-invasive tool to activate the motor cortex and assess the integrity of the corticomotor pathways. Since its development, the use of TMS was widely applied for neurophysiological examination to explore different neurophysiological mechanisms.
Its modulation of cortical excitability was also being developed as a therapeutic tool.66 In this study, we focus on the diagnostic application of TMS.
The TMS is based on the principle of electromagnetic induction. The TMS machine consists of high-current generators and a magnetic coil, while our brain consists of many neural networks. A brief electric current passes through a magnetic coil, which is placed over the human’s head, generating a perpendicular, high-intensity magnetic field, and then the secondary electric field is induced underlying the stimulated site of the brain.
The stimuli usually focus on the primary motor cortex (M1). The secondary electric field induced the action potential in the cortical axons, and then the excitation travels along the corticospinal tract to generate muscle twitches or movements of the corresponding muscles according to the motor homunculus. The amplitude of the muscle response to TMS, which termed motor-evoked potential (MEP), is recorded by surface electromyography (EMG). The electrodes of EMG are attached to the muscle belly.
2.4.2 Common TMS parameters for assessing cortical excitability
Various TMS parameters can provide the different information about cortical excitability, the functional integrity of intracortical neurons, the conduction along the corticospinal tract, and the peripheral neural pathway to the muscles. Such measurements are used to detect the neurophysiological changes of the brain in the setting of the cortical plasticity and brain disorder. Compared to other imaging techniques such as positron emission tomography (PET) and electroencephalography (EEG), TMS parameters can be rapidly acquired and they can provide close monitoring of relatively short-duration neuroplastic changes following experimental manipulation. According to the number of stimuli in a session, the diagnostic application of TMS can be classified into two modes:
single-pulse TMS (spTMS) and paired-pulse TMS (ppTMS).66 The TMS was applied to the primary motor cortex to obtain above assessments. The following are some common TMS parameters that we used in this study.
Single-pulse TMS (spTMS)
Motor Evoked Potentials (MEPs)
While TMS is applied to the motor cortex at appropriate stimulation intensity, MEPs are generated through activation of the motor cortex and the corticospinal pathways. The amplitude of MEP reflects the integrity of the cortical tract as well as the excitability of motor cortex, nerve roots, and the conduction along the peripheral
motor pathway to the muscles.66 If the TMS is delivered on the M1 under the condition of relaxed target muscle, the MEP that induced is called resting MEP. In contrast, if the TMS is delivered on the M1 under the condition of activated target muscle, the MEP that induced is called active MEP.
Hot Spot
The hot spot was defined as the site that can induce the most consistent and prominent MEPs with the shortest latency.67 It was an optimal stimulation site that represents the target muscle corresponding to the brain. The stimulus intensity was represented by the percentage of maximal stimulator output (MSO).
Motor Threshold (MT)
The motor threshold includes resting motor threshold (RMT) and active motor threshold (AMT). The RMT is defined as the minimum stimulus intensity that can induce at least 50μV of MEP in at least 5 of 10 trials under complete muscle relaxation68, while the AMT is induced under slightly contracted target muscles.67,68 The MT reflects the neurons’ excitability and their local density.69
Cortical Silent Period (CSP)
The CSP was a period of suppressed EMG activity occurring immediately after the MEP induced by TMS. It is only induced under the condition of activated muscle while the suprathreshold stimulation is delivered. The CSP is defined as the time
from the end of the active MEP to the return of EMG activity.66 However, it is difficult to define the end of the MEP in patients with corticospinal tract dysfunction, so some researchers define the CSP as the time interval from stimulus delivery to the return of voluntary activity.70 The CSP reflects long-lasting corticospinal inhibitory mechanisms. The cortical inhibition is mediated by gamma aminobutyric type B receptors (GABABR).71
Paired-pulse TMS (ppTMS)
Short Intracortical Inhibition (SICI) and facilitation (ICF)
The ppTMS can assess the intracortical inhibitory and facilitatory mechanisms through delivering a subthreshold conditioning stimulus (CS) and a suprathreshold test stimulus (TS). A conditioning stimulus is followed by a test stimulus at different inter-stimulus intervals (ISI). Different MEPs responses depend on the stimulus intensity and the ISI. SICI is obtained at ISIs of 1-4ms, which reflects inhibitory effects.69 In terms of facilitatory effects, the ISI at 7-20ms is applied, which called ICF.69 SICI is mediated by gamma aminobutyric type A receptors (GABAAR)72 while ICF is likely mediated through N-methyl-D-aspartate (NMDA) glutamate receptors.73
2.4.3 Abnormal cortical excitability in Parkinson’s disease
Since the primary motor cortex (M1) is an important target of basal ganglia output, dysfunction of the basal ganglia–thalamocortical (BGTC) circuit in PD leads to functional disturbances of the motor cortex. Such alteration in cortical excitability of M1 can be assessed through TMS. This imaging technique can detect whether facilitatory or inhibitory changes in motor cortex. The majority of TMS studies focused on the hand area of the more affected brain to investigate the cortical excitability in PD. According to the review of Cantello and colleagues,74 most studies indicated that RMT in PD was no differences in comparison to the healthy controls. Increased MEP amplitude at resting muscle, shortened duration of CSP, reduced SICI and ICF were found.74-76 These findings suggested the cortical excitability in PD revealed excessive corticospinal output at rest and reduced intracortical inhibition.
As for the corresponding cortical excitability of the lower limbs area, two studies explored this issue. Tremblay and colleagues77 recruited 10 patients with PD to investigate the cortical excitability of the quadriceps muscles. As the patients were assessed during "on" medication, decreased RMT, increased MEP amplitude at rest, and longer duration of CSP were noted in comparison to the healthy controls; whereas, when four out of ten patients were evaluated during "off" medication, all parameters except for the duration of CSP were similar to "on" medication. They exhibited the shorter duration
of CSP during "off" medication compared to "on" medication. It suggested that the dopaminergic medications may normalize the duration of CSP, which reflects the corticospinal inhibition. However, another study reported by Vacherot and colleagues78 indicated inconsistent results. They recruited 24 patients with PD and 9 healthy controls to explore the cortical excitability of the tibialis anterior muscle. The results displayed that RMT, amplitude of MEP at rest, duration of CSP, and SICI had no differences between groups and medication states. The only reduction in ICF was noted in PD in comparison to the healthy controls and decreased ICF could be partially normalized during "on" medication. The summarized contents are presented in table 1.
Overall, the patients with PD revealed abnormal cortical excitability, especially in the duration of CSP and paired-pulse parameters. The medicine may modulate the cortical excitability. Despite this, there is the paucity of information regarding TMS evaluation over the lower extremity. Therefore, further evidence concerning the changes in the cortical excitability of the lower limbs in PD is needed to draw a clear conclusion.
2.5 Summary of review
Parkinson’s disease (PD) is a common neurodegenerative disorder due to a dopaminergic deficiency in the basal ganglia. Dysfunction of dopaminergic cells in basal ganglia leads to deficits in internal timing and automatic execution of movements such as
gait disturbances. Moreover, freezing of gait (FOG) is one of the disabling gait disturbances. Freezers exhibits more gait instability, which related to stride time variability, than non-freezers. In order to ameliorate the impaired automatic motor performance, the utilization of auditory cues can provide the temporal stimuli to regular the timing of gait. Despite abundant studies concerning the effects of auditory cues on gait in PD, most of them focused on overground walking and long-term training for several weeks and the literature assessing the role of auditory cues on FOG are scarcer and controversial. Treadmill training, which can also act as an external cue, also provides the favorable effects on the gait pattern for patients with PD. More recently, the application of treadmill combined with auditory cues may potentiate positive effects on gait in comparison to treadmill training alone. The potential mechanism behind auditory cues might be through the cerebellar–thalamocortical (CTC) network to compensate the dysfunction of basal ganglia. Furthermore, since neuronal plasticity is associated with improved motor performance, the improved gait pattern after cueing-based trainings may come from the accumulation of series of neuroplasticity through serial motor training.
Thus, the neuroplasticity in the brain plays a crucial role for the patients with PD to improved motor performances. In order to explore the neuroplasticity in the brain, transcranial magnetic stimulation (TMS) can be applied to demonstrate the cortical plasticity through assessing the cortical excitability. For the patients with PD, they
exhibited abnormal cortical excitability, especially in the duration of CSP and paired- pulse parameters, which reflects long-lasting corticospinal inhibitory mechanisms and the intracortical inhibitory and facilitatory mechanisms respectively. However, current studies provide little information on how the auditory cues work in the brain. Furthermore, scarcer studies explores the different effects of auditory cued-based training on neurophysiology and gait performance between freezers and non-freezers. Therefore, it is worth for us to investigate whether the cortical excitability can be modulated through auditory-cued treadmill training and further explore whether there are the different changes in cortical excitability and gait performance between freezers and non-freezers.
Chapter 3 Methods
3.1 Study design
This is a crossover study. Patients with PD were recruited and classified into freezer group (FOG) and non-freezer group (nFOG) based on the first question of new freezing of gait questionnaire (NFOG-Q).42 The healthy subjects were also recruited as the control group. All subjects were involved in baseline evaluation and randomly participated in training under two conditions with at least one-week washout interval. Two conditions were treadmill training with (AC condition) and without rhythmic auditory cues (NC condition). The study protocol was approved by the Institutional Review Board of National Taiwan University Hospital (Appendix A).
3.2 Subjects
This study recruited subjects with PD and healthy subjects. Subjects with PD were recruited from the Department of Neurology, the Physical Therapy Center, and the Parkinson Center at National Taiwan University Hospital. Subjects with PD were enrolled if they (1) were 20 years old and over, (2) diagnosed with idiopathic Parkinson’s disease by neurologists, (3) classified as stages I through III on the Hoehn and Yahr rating scale, (4) able to walk independently without device, (5) no hearing impairment; (6) able to
follow instructions (Mini-Mental State Examination score ≧ 24). Participants were
divided into the freezer group (FOG) or non-freezer group (nFOG) based on their response to the first question of NFOG-Q: Did you experience “freezing episodes” over the past month? We demonstrated a video about freezing episodes to make sure subjects
fully understood what freezing symptoms are. Participants were categorized as FOG group if their response was 1. They were placed in nFOG group if their response was 0.
Subjects with PD were excluded if they have (1) past histories of neurological or musculoskeletal disorder that might interfere with ambulation (e.g. stroke), (2) psychological diseases, (3) unstable cardiovascular and respiratory status, (4) dementia, (5) uncorrected visual disturbances that affect gait performance (e.g. blind people), (6) contraindications of receiving TMS assessments including family history of epilepsy, being pregnant, having a cardiac pacemaker, brain trauma, or metal implants in the brain.
The purposes and procedures were fully explained to the subjects. Participants signed the informed consent forms (Appendix B) and TMS safety questionnaire (Appendix C) before the experiments.
3.3 Procedure
All participants received treadmill training with (AC condition) and without rhythmic auditory cues (NC condition) in random order by using a computer-generated
random number. Two conditions were at least one-week washout interval. Basic data collections included age, gender, onset duration, modified Hoehn and Yahr stage, Unified Parkinson's Disease Rating Scale (UPDRS), Mini-Mental State Examination (MMSE), New Freezing of Gait Questionnaire (NFOG-Q). The above data were obtained from the subjects' interviews or assessed by the researcher. All participants were evaluated the cortical excitability and motor performance before and after training. Patients were asked to withdraw their dopaminergic drugs overnight at least 8 hours in order to eliminate the influence of medications on the outcome measures. A flow chart of this study is presented in Figure 1.
3.4 Interventions
All participants received a single session of treadmill training in two condition (AC and NC condition) with at least one-week interval. The treadmill (Model AG-2000, Aerogym trading company, Taichung, Taiwan) was used in this study. A suspension with no body weight support was provided for safety concern. We made sure that the suspension would not interfere with participants’ walking performance. All participants walked on the treadmill while holding the handrails (Figure 2). The treadmill was set at 0% incline and the training session lasted 30 minutes. Patients could rest 1-3 minutes if they subjectively feeling tired during the training. However, the resting time did not
include in our intervention time.
3.4.1 Treadmill training with rhythmic auditory cues (AC condition)
We used the metronome from the YouTube as the auditory cues. The cued frequency was set at 110% of subject's comfortable cadence on the treadmill because this cued frequency might provide the beneficial effects on the kinetic characteristic of gait and walking stability based on the previous studies.18,79,80 Participants were asked to synchronize with the rhythmic auditory cues on the treadmill for 30 minutes. The participants could ask for alternating treadmill speed in order to synchronize with auditory cues.
3.4.2 Treadmill training without rhythmic auditory cues (NC condition)
The treadmill velocity was set at the subject's comfortable walking speed on the treadmill. Participants walked comfortably on the treadmill without auditory cues for 30 minutes.
3.5 Outcome measurements
To determine the effects of treadmill training combining with auditory cues, two domains were evaluated before and after intervention: cortical excitability and motor performance. For the cortical excitability, resting and active amplitude of motor evoked
potentials (MEPs), cortical silent period (CSP), short intracortical inhibition (SICI), and intracortical facilitation (ICF) were used to record the changes in cortical excitability. For the motor performance, 10-meter walking test was selected to evaluate step time variability and gait pattern.
3.5.1 Primary Outcome measures-Cortical Excitability Transcranial Magnetic Stimulation (TMS)
The TMS was applied using Magstim BiStim2 stimulator (The Magstim Company, Whitland, UK) through a double cone coil. Electromyography was recorded using surface electrodes positioned over the tibialis anterior (TA) muscle of the more symptomatic side.
Participants were instructed to sit in a comfortable chair with backrest and keep their arms in a relaxed position. They wore the swimming cap, which consisted of one-by-one centimeter points allowing an exact positioning of the TMS coil. The coil was placed over the interhemispheric sulcus and moved around (Figure 3). Once the optimal stimulation site, called "hot spot", was identified, using pen marked the site on the cap to ensure consistent coil placement. After the hot spot was identified, the stimulus intensity would be reduced in steps of 2% maximal stimulator output (MSO) to measure the resting motor threshold (RMT). The RMT was defined as the minimum stimulus intensity that can induce at least 50μV of MEP in at least 5 of 10 trials under complete muscle relaxation.68
Experimenters asked and supervised participants to stay awake during the procedure.
Acqknowledge 4.2.1 software (Biopac Inc, California, USA) was used for data acquisition and analysis. Before and after TMS, the participants were asked if they had any adverse effects such as headache, or worsened symptoms.
TMS measurements included amplitude of resting and active MEPs, CSP, SICI, and ICF. Each measurements contained 7 times of stimulus. Each stimulation was separated by at least 5s in order to avoid carryover effects. The followings were the detail of each parameters.
- Resting motor evoked potentials (MEPs): Resting MEPs were measured at 130% of RMT when subjects completely relaxed the target muscle. The MEPs value were recorded the peak-to-peak amplitude of EMG response.
- Cortical silent period (CSP) and active MEP: CSP is a period of suppressed EMG activity following after the MEPs induced by TMS.67 CSP were measured by single TMS stimulus at 130% of RMT, while subjects executed voluntary contraction of their tibialis anterior muscle. They did dorsifleixon to a given target, and then the stimulus were given in random timing during executing action. CSP duration was recorded from stimulus delivery to the return of voluntary activity. The active MEPs value was recorded the peak-to-peak amplitude of EMG response.
- Short intracortical inhibition (SICI), and intracortical facilitation (ICF): The SICI and