Parity and risk of
death from
subarachnoid
hemorrhage in
women: Evidence from
a cohort in Taiwan
Abstract—The authors examined the relationship in women between age at first birth, parity, and subarachnoid hemorrhage mortality. They followed each woman from the time of her first birth and linked vital status with a mortality database. The risk was increased by 8% for each additional year of mother’s age at first birth. The relative risk was 0.63 for women who had borne two children and 0.62 for women with three or more births.
NEUROLOGY 2006;67:514–515
Chun-Yuh Yang, PhD, MPH; Chih-Ching Chang, MD, PhD; Hsin-Wei Kuo, MD; and Hui-Fen Chiu, PhD
Subarachnoid hemorrhage (SAH) is the only type of stroke that occurs more often in women than in men, for reasons that are poorly understood.1
Hypertension, cigarette smoking, and alcohol drinking are risk factors for SAH.2 These risk
fac-tors, however, are more common in men than in women, so the excess of SAH in women is not related to these factors.
Hormonal factors, including oral contraceptive (OC) use2and hormone replacement therapy (HRT),2
have been suggested as possible explanations for the female susceptibility to SAH. However, study results have not been consistent.
To date, there are limited data regarding the rela-tionship between childbearing and SAH.3-5One study
reported no relationship between parity and SAH3; a
second study reported that there was an increase in the risk for SAH in women who had given birth to more than one child when compared with nullipa-rous women, but the association failed to reach sig-nificance4; and a third study reported a decreasing
trend between the risk of SAH and increasing parity.5
We studied a cohort of women who experienced a first and singleton childbirth between January 1, 1978, and December 31, 1987, to further explore the relationship between parity and the risk of death from SAH.
Methods. It is the responsibility of the parents or the family to register infant births within 15 days. The registration form, which requests information on maternal age, education, parity, date of delivery, infant gender, and birth weight, is completed by the physician attending the delivery. The Birth Registration System, which is managed by the Department of Interior, has released computerized data on live births since 1978. Because most
deliv-eries take place in either a hospital or a clinic and it is mandatory to register all live births at local household registration offices, the birth registration data are considered complete, reliable, and accurate.
The study cohort consisted of all women with a record of a first and singleton childbirth in the Birth Register between January 1, 1978, and December 31, 1987. Information on subsequent births was also retrieved from the Birth Register. Each woman has her own personal identification number, which was used to track the women from the time of their first birth to December 31, 2003. Their vital status was ascertained by linking records with the mortality database, identifying the date of any deaths occurring in this cohort.
The person-years of follow-up for each woman were calculated from the date of first birth to the date of death or December 31, 2003. Death rates were calculated by dividing the number of deaths from SAH by the number of person-years of follow-up. Cox proportional hazard regression models were used to estimate the relative risks (RRs) of death from SAH associated with parity (the number of children recorded in the last birth record of each woman registered during follow-up). SAH death is defined accord-ing to the ICD-9 (Code 430). The adjustment variables in the final model included age at first birth and parity. Analyses were per-formed using the SAS package. Values of p ⬍ 0.05 (two sided) were considered significant.
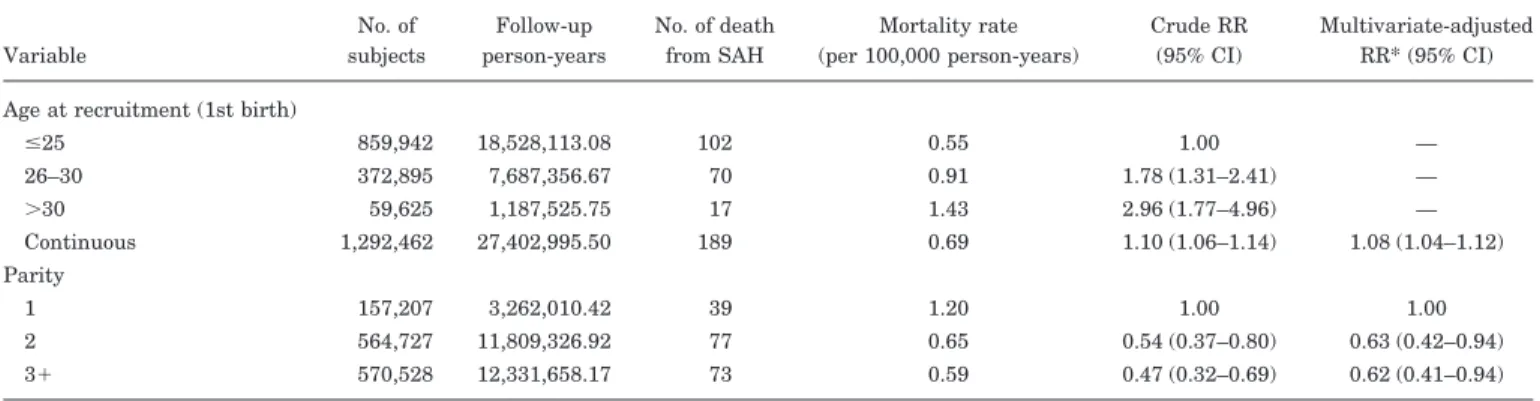
Results. Altogether, 1,292,462 primiparous women with complete information were included in the analysis (table). A total of 27,402,995.5 person-years were observed. There were 189 SAH deaths, yielding a mortality rate of 0.69 cases per 100,000 person-years. No significant effects of marital status, years of schooling, and birthplace on risk of SAH deaths were found (data not shown). After adjust-ment for age at first birth, the RRs for SAH death were 0.63 (95% CI ⫽ 0.42-0.94) for women who had borne two children and 0.62 (95% CI 0.41 to 0.94) for women with three or more births, when compared with women who had borne one child. The RR was 1.08 (95% CI 1.04 to 1.12) for each additional year of mother’s age at first birth after adjustment for parity.
Discussion. We used a prospective study to exam-ine the relationship between parity and the risk of death from SAH. Previous studies all used case– control designs.3-5
The results of previous studies concerning the as-sociation between parity and risk of SAH have been inconclusive.3-5 Our study findings are in agreement
with the results of a large population-based case– control study.5 Other case– control studies3,4 have
found no significant association between parity and SAH. Our data, like the previous study with a posi-tive result,5 take into account the effect of the num-From the Institute of Public Health, College of Health Sciences (C.-Y.Y.,
C.-C.C., H.-W.K.), and Institute of Pharmacology, College of Medicine (H.-F.C.), Kaohsiung Medical University, Kaohsiung, Taiwan.
This study was partly supported by a grant from the National Science Council, Executive Yuan, Taiwan (NSC-94-2314-B-037-056).
Disclosure: The authors report no conflicts of interest.
Received January 3, 2006. Accepted in final form March 28, 2006. Address correspondence and reprint requests to Dr. Chun-Yuh Yang, Insti-tute of Public Health, Kaohsiung Medical University, 100 Shih-Chuan 1st RD, Kaohsiung, Taiwan 80708; e-mail: [email protected]
ber of children on the risk of SAH. In other studies, however, parous women were compared only with nulliparous women, and nulliparity may reflect an inability to conceive or complete a pregnancy be-cause of health factors with unknown influences on the risk of SAH.5
We found that the risk of death from SAH in-creases with age at first birth. The reasons are un-known, but they may relate to long-lasting hormonal changes including lower sex hormone– binding globu-lin (SHBG) levels and higher total estrogen levels. Lower levels of SHBG have been suggested to be associated with decreased serum levels of estradiol bound to SHBG, and with lower bioavailability, re-sulting in atherogenic changes and hypertension6
and possibly in increases in the risk of SAH.
The mechanism by which increased parity may confer protection against future development of SAH in women remains unknown. The protective effect of higher parity may be related to the higher progester-one levels during pregnancy, resulting in a better balance between progesterone and estrogens during this period.7In contrast, nulliparity has been
associ-ated with increased estradiol levels. Estrogens lead to increased blood pressure7 and therefore may
in-crease the risk of SAH.
Mortality data rather than data on inpatient cases were used in this study; however, the mortality of a disease is a function of its incidence and fatality rate. Lack of verification of the diagnosis of SAH may include many patients with intracerebral hemor-rhage (ICH). ICH occurs twice as often as SAH,8and
distinction between these two types of hemorrhage without CT scanning or MRI is erroneous in approx-imately 20% of patients.9The proportion of patients
in whom the diagnosis is confirmed by CT or MRI is not available in this study. However, there is no reason to believe that the misclassification of SAH deaths might have occurred differentially by parity, and therefore, this factor was unlikely to account for the association we observed.
Cigarette smoking, alcohol drinking, and
hyper-tension have been documented as risk factors for SAH.2The prevalence rates of cigarette smoking and
alcohol drinking are low (approximately 5%) in Tai-wanese women.10 Given these low prevalences, the
association between parity and SAH deaths in our study is unlikely to be affected remarkably by these behaviors. There is no information available on hy-pertension for individual study subjects, and thus it could not be adjusted for directly in the analysis. However, there is no reason to believe that there would be any correlation between hypertension and parity.
Hormonal factors including OC use and HRT have been used to explain the female susceptibility to SAH, but we were unable to adjust for these two factors in the current study because of the lack of available data. Because OC use and HRT are uncom-mon in Taiwan compared with Western countries, the confounding effect resulting from these two fac-tors should be small, if they existed at all.
References
1. Torner JC. Epidemiology of subarachnoid hemorrhage: seminars in neurology. Neurology 1984;4:354–369.
2. Teunissen LL, Rinkel GJ, Algra A, van Gijn J. Risk factors for sub-arachnoid hemorrhage: a systematic review stroke 1996;27:544–549. 3. Mhurchu CN, Anderson C, Jamrozik K, Hankey G, Dunbabin D.
Hor-monal factors and risk of aneurysmal subarachnoid hemorrhage: an international population-based case-control study. Stroke 2001;32:606– 612.
4. Okamoto K, Horisawa R, Kawamura T, Asai A, Ogino M, Takagi T, Ohno Y. Menstrual and reproductive factors for subarachnoid hemor-rhage risk in women: a case-control study in Nagoya, Japan. Stroke 2001;32:2841–2844.
5. Gaist D, Pedersen L, Cnattingius S, Sorensen HT. Parity and risk of subarachnoid hemorrhage in women: a nested case- control study based on national Swedish registries. Stroke 2004;35:28–33.
6. Anderson DC. Sex hormone-binding globulin. Clin Endocrinol 1974;3: 69–96.
7. Fisch IR, Frank J. Oral contraceptives and blood pressure. JAMA 1977; 237:2499–2503.
8. Broderick JP, Brott TG, Tomsick T, Miller R, Huster G. Intracerebral hemorrhage more than twice as common as subarachnoid hemorrhage. J Neurosurg 1993;78:188–191.
9. van Gijn J, van Dongen KJ. Computed tomography in the diagnosis of subarachnoid hemorrhage and ruptured aneurysm. Clin Neurol Neuro-surg 1980;82:11–24.
10. Yen ML, Yen BL, Bai CH, Lin RS. Risk factors for ovarian cancer in Taiwan: a case-control study in a low-incidence population. Gynecol Oncol 2003;89:318–324.
Table Relative risk of death from SAH by age at first birth and parity
Variable No. of subjects Follow-up person-years No. of death from SAH Mortality rate (per 100,000 person-years) Crude RR (95% CI) Multivariate-adjusted RR* (95% CI) Age at recruitment (1st birth)
ⱕ25 859,942 18,528,113.08 102 0.55 1.00 — 26–30 372,895 7,687,356.67 70 0.91 1.78 (1.31–2.41) — ⬎30 59,625 1,187,525.75 17 1.43 2.96 (1.77–4.96) — Continuous 1,292,462 27,402,995.50 189 0.69 1.10 (1.06–1.14) 1.08 (1.04–1.12) Parity 1 157,207 3,262,010.42 39 1.20 1.00 1.00 2 564,727 11,809,326.92 77 0.65 0.54 (0.37–0.80) 0.63 (0.42–0.94) 3⫹ 570,528 12,331,658.17 73 0.59 0.47 (0.32–0.69) 0.62 (0.41–0.94) * Mutually adjusted.
SAH⫽ subarachnoid hemorrhage; RR ⫽ relative risk.