醫學生醫學倫理教學研究:第三年
The Teaching of Medical Ethics to Medical Students: The Third Year
計畫主持人: 李明濱 共同主持人: 謝博生、林信男
執行單位: 台大醫學院社會醫學科、精神科、內科
計畫編號: NSC87-2511-S-002-017
執行期間: 86年8月 1日至87年7月31日
中文摘要
醫學倫理學的教育與研究已漸受重視,但有關教學評估研究仍極度缺乏。本研究 目的在於針對不同學年度之同年班級探討利用啟發式小組教學技巧實施醫學倫理學教 學的相關問題,及其短期成效評估;本研究分別針對八十四、八十五及八十六學年度台 大醫學院醫學系修習醫學倫理學課程之六年級學生為對象,前二學年度每組學生約20-22人,最後一學年度,每組為26人左右;修習時間每組六週,小組討論課程每週四小時。 討論過程由同學主持,以問題為基礎及個案為中心,由至少2位跨科之導師指導,進行 討論。在課程結束時,以自填問卷評量方式由學生不具名評估學習成效、團體氣氛及團 體互動。經由三學年之研究結果發現,討論式小組教學適用於醫學倫理學之教學;就整 體 評 量 而 言 , 三 學 年 的 極 多 數 的 學 生 認 為 醫 學 倫 理 教 育 對 行 醫 生 涯 很 重 要 (92.9%:98.4%:90.9%),大多數同學對課程內容安排(68.8%:74.4%:68.8%)及進行方式 (56.3%:69.8%:55.4%)均表滿意;而多數學生覺得倫理知識(70.5%:84.1%:71.1%)有明顯 的收穫,而對倫理思考能力(72.3%:89.7%:78.5%)亦有明顯的幫助。三個不同學年度之 團體互動與氣氛的評量結果,整體而言,各年度都維持在良好狀況,而以八十五學年度 為最佳。經由同一模式的教學,三學年的成效評估顯示教學成效穩定且在倫理知識與倫 理思考方面的收穫都有意義的持續增加;在團體學習及團體氣氛方面亦表現持續的改 善。逐步複迴歸分析發現,團體學習因素分別可解釋倫理知識收獲變異量的22.8%,倫 理推理變異量的25.1%。第三年計劃特別探討住院病人之醫病溝通問題,針對188位無認 知功能障礙的住院病人所做的深度面談結果發現,約45%左右的個案分別對病情、治療 不瞭解,醫病溝通關係不好;這提示平日倫理溝通應列入醫學倫理教育的基礎內容之 中,而不能只一味地探討重大之倫理兩難。 關鍵詞:醫學倫理學教育,成效評估,小組教學
[Abstract]
The Teaching of Medical Ethics to Medical Students: The Thir d Year
In most western countries, the study of medical ethics has been emphasized in medical school curricula since the early 1970s. However, medical school curricula in Taiwan have yet to place a similar emphasis on medical ethics. The present study evaluated students’ understanding of medical ethics and opinions about course content following completion of a course in medical ethics taught using a small-group tutorial method. The participants were the sixth-year students at the National Taiwan University College of Medicine in the academic years 1995-1996 and 1996-1997 and 1997-1998. The course was conducted as weekly four-hour discussions for six consecutive weeks. The students were divided into six groups with approximately 20-22 members in each group. Each two-hour session was facilitated and coordinated by the tutors, two senior psychiatric faculty members and one or two physicians in other specialties or allied professionals. During each session, four students in each group were assigned a special topic, which was described on prepared handouts. Those students were then asked to give a brief presentation on the topic. One of the students was designated as the group leader. Following the presentation, all of the students were asked to give problem-based and case-centered examples as triggers for open discussion. A series of reliable questionnaires were developed to assess the teaching effectiveness, and to measure the group interaction and group atmosphere. Post-course questionnaire surveys for three consecutive academic year students revealed that a great majority (92.9%: 98.4%: 90.9% in 1995, 1996 and 1997 class respectively) of the students considered ethics education to be important for professional development, and 75.8%: 83.9%: 75.2% believed that ethics courses should be taught during clinical training (years 5 and 6). The majority of students were very satisfied with both the course content (68.8%: 74.4%: 68.8%) and the teaching format (56.3%: 69.8%: 55.4%). Regarding the effectiveness of the course, survey results indicated that 70.5% to 84.1% of the students reported to have significant gains on general knowledge of ethics and 72.3% to 89.7% of them in the ability to perform ethical reasoning. The students’ ratings on group interaction and group atmosphere showed significant correlation with the degree of gain of ethical knowledge and ethical reasoning. Stepwise multiple regression analysis revealed that group learning factors could account on 22.8% of variance of ethics knowledge and 25.1% of variance of ethics reasoning. The present study also found that were 45% of hospitalized inpatients were judged to have poor physician-patient relationship, poor communication on disclosures of medical information and treatment strategy.
In conclusion, the third year study consistently demonstrated that students were satisfied with the teaching methods and course content of medical ethics education using a small-group tutorial method. The findings of the present study also provide valuable information to suggest the importance of daily ethics of doctor-patient communication in ethics education.
醫學倫理在於規範醫病關係與醫療行為,使能達於真善美的程度,近年來醫學倫 理學教育在國內外已深受重視。由於醫學倫理學不像生物學有絕對一成不變的答案,因 此其教學及認知學習,最適合採用討論方式進行;利用討論、批判、辯論、角色扮演、 經驗分享之小組方式進行,以達到學習的目標。本研究為系列研究之第三年,目的在於 將啟發式小組教學方法應用於醫學系六年級之醫學倫理學教學,並針對三組不同學年度 學生,探討課程內容、進行方式、課後心得評估、短期教學成效以及影響教學成效的團 體互動因素;以提供未來相關之教學改進與發展之參考。
研究方法
對象: 本研究係針對醫學倫理學課程;而以84、85及86學年度,修習醫學倫理學之醫學系 六年級學生為對象。 課程規劃與設計: 本研究之醫學倫理學課程(二學分)採取小組教學方式,且與精神醫學課程(六週, 四學分)之上課與見習合併進行;其課程設計已於文獻: 一、單元題目之擬定:為擬定小組討論課程之單元題目與內容大綱,作者根據下列步驟, 分析、整理後定出課程之單元主題: 1、函請各科主任提供該科執行醫療業務有關且可供醫學生討論的醫學倫理題目,以及 除該科外,醫學倫理課程所應該討論的題目。並請各科推薦對醫學倫理教學有興趣 且可參加討論之教師及主治醫師名單。 2、將各科所列之40道題目分類整合,經由前述所有任課教師在課前之協調會中再予修 正,共擬出下列六個課程單元: (1)醫學倫理思考、醫療法規與醫學研究;(2)醫療 行為與生病行為;(3)醫療權益與責任;(4)生殖科技與生死之態度;(5)變性醫療 與器官移植;及(6)生命延長與終止等六個單元。86學年度改為十二個單元:(1)醫 學專業宣言、醫療法規暨醫療爭議;(2)醫學研究與生命科學倫理;(3)醫療專業的 內容倫理;(4)醫療行為與生病行為;(5)醫療的權利與責任;(6)生殖科技(1);(7) 生殖科技(2);(8)器官移植;(9)變性手術與美容手術;(10)醫療制度的倫理;(11) 醫學與健康知識的權力與機制;(12)生命終止的處置倫理。全班分五梯次進行,每 梯次為輪流至精神科見習之小組約26人,期間為六週;討論時間共計六週;每週四 小時;每週主題為二單元,每單元二小時;課程題目及內容綱要以單元為單位。 課程進行:84學年度與85學年度全班各分為六組,每學期三組;86學年度因前六週全班配合實 施解剖學二階段教學之「生死學」課程(為新增課程)全班分為5組。在學年度剛開始時, 予以解釋課程目的、方式;評估等事項並在課程結束時進行整體性評估,並施以課前教 育,成績評定說明及討論進行方式。在六週課程結束後,由學生不具名填寫各項學習成 效評量表。 學習成效評量 本研究之報告課程評估主要為由學生對整體課程及對團體進行過程之評估及對醫 學倫理學知識與推理之自我評量;其使用之各評量表如下: 1.整體課程評量表:含14大題;除改進之意見欄外,其餘項目分別以五分法(0-4)針對 醫學倫理學之重要性、對課程內容及進行方式的滿意度、學習的整體收獲(包括知識 與倫理思考),及撰寫期末報告投入的程度與收穫予以分項評估,同時估計自我學習 所花費的時間等。 2.團體氣氛評量表:包含18題,除了測量參與度(engagement)、逃避(avoidance)及衝 突(conflict)三個向度外,還可評量學生的緊張情緒、對老師及同學的看法及小團 體的形成等與互動相關因素的評量。本量表係根據熟悉團體動力學之專家意見,及 作者等人主導小組教學多年來之經驗,依觀察及實務經驗設計而成。 3.團體互動(學習有效因素)評量表:主要根據Yalom ID (1975)對團體學習有效因素之 報告,並配合小組教學實況重新設計而成,內容包含22題,可評量下列9項團體學習 因素:1.知識學習;2.宣洩作用;3.仿同作用;4.利他;5.團體和諧;6.共通性;7. 自我瞭解;8.社交技巧;及9.凝聚希望。 統計分析 本研究除學習成效評量表、團體氣氛評量及團體互動評量表之信度檢定Cronbach α 值外,其餘各變項結果之表示均以描述性統計說明其百分率分佈。三學年之評量結果比 較針對連續性之量化資料以t-test為主,針對類別變項則以chi-square test為主,本 研究並以倫理知識與推理收穫為依變項,逐步複迴歸分析探討團體互動與團體氣氛因表 (獨立變項)對其影響。p值<0.05定為統計上有意義。
重要結果與討論
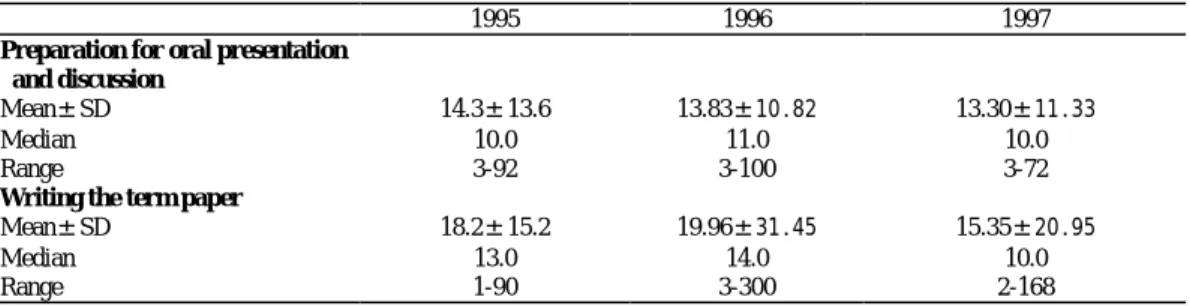
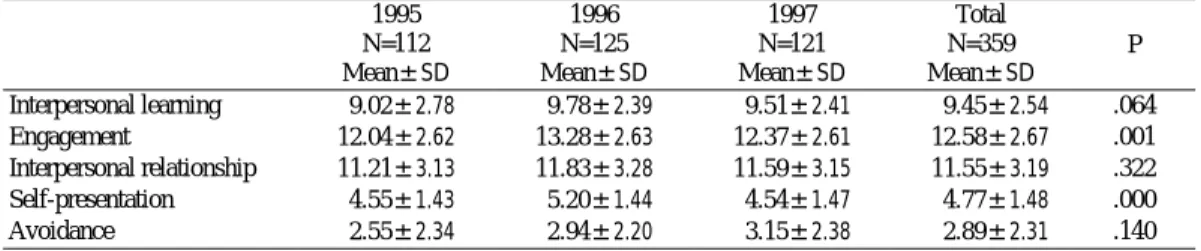
整體課程評量 針對回收學生填寫之“整體課程”評估之回收有效問卷(84學年度為112份,85學年度 為126份,86學年度為121份)分析結果,就整體收穫而言,經由六週的討論式小組教學,助;就課程內容安排而言,有68.8%、74.4%及68.8的學生認為很滿意,但對課程的進行 方式僅有56.3%、69.8%及55.4%認為很滿意。 除了參與24小時的小組教學討論外,根據學生個人的估計,為準備小組討論每位同 學所花的時間由3-100小時不等,平均為13.74小時(中數值為10小時);而花在撰寫課後 心得報告的時間由1-300小時不等,平均分別為18.2±15.2小時、19.96±31.45及 15.35±20.95小時。此外分別有79.3%、79.2%及71.1%的學生自覺撰寫報告過程之投入很 深入;而就課程結束後學生針對自選主題及心得與感想所撰寫的報告而言,則有78.3%、 80.0%及70.2%的學生認為透過撰寫報告的過程,對醫學倫理學教學的目標而言有明顯之 收穫。然而只有55.4%、55.6%及54.5%的學生「積極的」表示對於課後報告的撰寫應繼 續維持下去。 此外,關於醫學倫理學教育對於未來行醫生涯之重要性而言,分別有92.0%、98.4% 及90.0%的學生認為重要,幾乎沒有同學認為不重要;而究竟同學心目中認為醫學倫理 學課程應該排在那一年級較適合呢?大多數(63.7%、67.5%及49.6%)認為應排在六年級, 而分別有15.0%、10.6%及7.6%認為應在七年級;其他依次為五年級(分別為11.5%、17.9% 及26.9%),三或四年級(8.8%、2.4%及8.4%),而只有極少數(0.9%、1.6%及7.6%)的同學 認為可排在1-2年級;因此,超過90%的同學認為課程應安排在參與臨床見習之後的階段 修習。 團體氣氛與團體互動評量結果 小組討論目的之一在於以問題為基礎或個案為中心,透過批判性的思考與迴饋的 互動而積極主動地學習,其互動與氣氛是作者所積極關心的議題之一;所列氣氛評量表 的內容與評分結果可知同學的積極參與度頗高,而負面的氣氛如逃避、衝突及焦慮等項 目的比率均低。影響討論式小組教學學習成效之相關因素,就團體“互動”因素量表各細 項而言,依被評為「很多」及「非常多」的比率高低排序,三學年結果前幾項由高而低 依序為:學習表達能力(70.5%,81.6%,74.4%),將個人的成果與別人分享(67.0%,71.5%, 62.0%),對討論有共鳴的感覺(66.1%,71.8%,63.6%),學習如何整理資料(63.4%,79.2%, 67.8%),體會人際關係(61.3%,65.6%,60.3%),學習如何收集資料(58.9%,74.4%, 64.5%),及有團體歸屬感(58.9%,69.6%,59.5%)等。由本系列研究之結果,透過信效 度研究就此二量表之40題題目,選出20題另建構成“團體學習評量表”,其包含下列五項 向度:參與度、人際關係、規避/衝突、仿同互動學習及自我表露。就三個學年度的評 量結果(如表5所列),發現1996年之各向度得分都最高,特別是自我表露及參與度,其 差異統計上有意義。
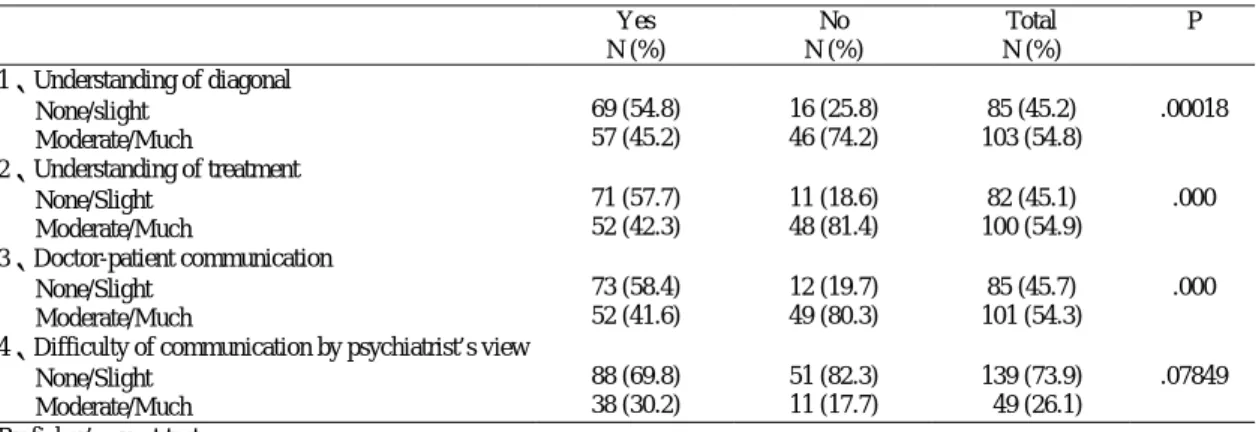
團體有效學習之互動因素 由表6可知,各項團體學習因素及撰寫期末報告之投入程度,均分別與倫理知識及 倫理推理能力之收穫程度均呈現有意義之相關。逐步複迴歸分析結果,發現團體學習因 素分別可解釋倫理知識收獲變異量的22.8%(表7-1),倫理推理變異量的25.1%(表8-1)。由 表7及表8所列,可知影響倫理知識與推理的共同因素為同學的意見及以老師為榜樣;而 影響知識收獲的另外三項主要因素為同學互相關心、團體參與感及期末報告的投入程 度。而影響倫理推理的另二項因素為:同學對自己的看法(批評)及自我瞭解優缺點。 醫病間之倫理溝通 就醫療倫理的基本層面醫病溝通而言,作者等針對262位照會精神科的病人進行分 析,結果發現轉介理由中明列病人不合作者僅6位(2.3%),明顯有醫病衝突者為10位 (3.8%)。經由精神科評估結果發現有74位(28.2%)為器質性腦功能障礙,若只針對其餘無 認知功能障礙之188位患者,以進行深度面談( indepth interview)探討:(1)病人對病情的 瞭解程度;(2)病人對治療方法的瞭解程度;及(3)病人與主治醫師之溝通狀況。 結果由表9可見188位個案中,有85(45.2%)對病情不十分瞭解,103位(54.8%)普通或 很瞭解;其中女性病人有適應障礙診斷者,對病情不瞭解的比率較高,就對治療內容的 瞭解度而言,82(45.1%)病人不瞭解或稍微瞭解,100位(54.9%)普通或很瞭解;同樣的, 女性病人及有精神疾患診斷者不瞭解之比率偏高。就醫病溝通關係而言,只有101位 (54.3%)屬於普通或溝通良好,而有85位(45.7%)並無溝通或稍微有溝通;有精神科診斷 者醫病溝通關係較差,性別則無明顯之差異。但就病情及診療之瞭解程度而言,女性患 者要比男性差。
討論
一般而言,醫學倫理學教學的主要方式包括講授式、個案或專題討論、床邊教學、 導師式教學(由學生自動找問題向導師請教);進行方式可以是以問題為導向以及個案為 中心。本研究結果發現小組教學方式很適用於倫理學教學;根據同學之整體評量及團體 氣氛與團體互動評量結果,可發現同學的學習過程中,良性的互動機會多,而且能秉持 利他的態度,在有共同問題的情境(共通性)下,經由和諧的互動而能達到主動學習、批 判、思考、分析及表達的整體目標。醫學倫理學的必要性已不容置疑,而教學的內容與 目標也較有共識性;本研究90%以上的學生都認為此課程對於醫師生涯很重要。回顧國 外文獻,將醫學倫埋置於醫學生必修課程也是近年來的事,而修習時間可以是在(1)臨床 見習前;(2)進入臨床見習後;(3)實習醫師階段;(4)住院醫師時期;其中認為在學生時 代修習者居多。就本研究調查結果而言,多數同學們仍認為應該在臨床見習時(6年級) 較適合;由三學年之研究評估,發現醫學倫理學的正式教學課程宜保有其時序之連貫 性,而將其適度分散於各學年,但重點應置於六年級見習時間;譬如針對某些入門概念 可於一、二年級時即可教授;三、四年級則可探討實際之臨床倫理議題,如醫療關係與 衝突;而在進入臨床見習與實習後,則可全面採取問題為基礎及個案為中心的方式進行 討論;如此,同學較能透過個人經驗與師長的經驗傳承而強化有效之學習。 就學生之學習成效評估結果而言,由結果中可看出就教學內容、進行方式及倫理知 識與思考推理諸層面而言,同學們多數都覺得有明顯收獲。而同學的意見、老師的示範、之狀況,其原因可能如下:1)第三年因前六週全班施行生死學課程之講授與討論,因此 全班自第七週開始,正式進入「醫學倫理與醫療行為」課程,全班分為五組,導致每組 人數由原來之22名,增至28名左右,學生之互動量將因此受到影響;2)由於生死學之開 辦,且將之視為醫學倫理學的一部分,因此第三年之課程內容略有增加,是否導致老師 的熟悉度不像第二年般的純熟。
重要結論與建議
1、以個案及實例為重點,啟發式、討論式之小組教學極適用於醫學倫理教學。三年之 教學資料及錄影,將整理成相關之教材。 2、團體學習評量表,可用作為此種討論教學之互動評量,並能預測其倫理知識與推理 能力之收穫。 3、由住院病人之訪查結果,提示醫病溝通仍是普偏存在的問題,應列入倫理教學之基 礎課程內容,不應只偏重於重大倫理兩難議題之討論。 4、醫學倫理課程安排應就質與量方面的不同,而適當安排於各不同年級,即應考慮其 階段性與連接性。 5、整合不同科別之師資共同參與討論,可增加相關之師資,同時更能刺激老師在日常 診療中更注重與倫理相關之示範教學。 6、若欲使醫學倫理教育之結果能落實於臨床實務之中,則整體醫學人文課程的整合與 規劃不容忽視;而且由畢業後進入臨床的資料分析結果而言,醫病間之倫理溝通仍 有待加強,正顯示醫學倫理繼續教育的重要性。參考文獻
1、 Ales KL, Charlson ME, Williams-Russo P, Allegrante JP: Using faculty consensus to develop and implement a medical ethics course. Academic Medicine 1992;67(6):406-8.
2、 Baylis F, Downie J: Ethics education for Canadian medical students. Academic Medicine 1991;66(7):413-4.
3、 Burling SJ, Lumley JS, McCarthy LS, Review of the teaching of medical ethics in London medical schools. [Review] Journal of Medical Ethics 1990;16(4):206-9.
4、 Calman KC, Downie RS: Practical problems in the teaching of ethics to medical students. J Med Ethics 1987;13:153-6. 5、 Delaney B, Kean L:Attitudes of Medical Students to the Teaching of Medical Ethics. Medical Education 1988;22:8-10. 6、 Fentem PH: Methods of teaching medical ethics at the University of Nottingham. J Med Ethics 1985;11:27-8. 7、 Gillon R:Medical ethics education. J Med Ethics 1987;13:115-6.
8、 Hayward RSA, Honer WG: Student-directed teaching of medical ethics at a Canadian medical school. J Med Educ 1985;60:384-9. 9、 Howe KR:Medical Students' Evaluations of Different Levels of Medical Ethics Teaching: Implications for Curricula. Medical
Education 1987;21:340-349.
10、Miles SH, Weiss Lane L, Bickel J, Walker RM, Cassel CK: Medical Ethics Education: Coming of Age. Acad Med 1989;64:705-14. 11、Mitchell KR, Lovat TJ, Myser CM: Teaching bioethics to medical students: the Newcastle experience. Medical Education 1992;26(4):290-300.
Table 1. Evaluation of medical ethics teaching in terms of student knowledge level and reasoning ability after course
completion based on global ratings by the students in three academic year classes
Degree of gain 1995 (N=112) N (%) 1996 (N=126) N (%) 1997 (N=121) N (%) Total ( N=359 ) Statistics Ethical knowledge
Very much/ Much Moderate Slight/ None 79 ( 70.5 ) 25 ( 22.3 ) 8 ( 7.1 ) 106 ( 84.1 ) 14 ( 11.1 ) 6 ( 4.8 ) 86 ( 71.1 ) 25 ( 20.7 ) 10 ( 8.3 ) 271 ( 75.5 ) 64 ( 17.8 ) 24 ( 6.7 ) df=4 x2=8.11 p=0.09 Ethical r easoning
Very much/ Much Moderate Slight/ None 81 ( 72.3 ) 24 ( 21.4 ) 7 ( 6.3 ) 113 ( 89.7 ) 10 ( 7.9 ) 3 ( 2.4 ) 95 ( 78.5 ) 21 ( 17.4 ) 5 ( 4.1 ) 289 ( 80.5 ) 55 ( 15.3 ) 15 ( 4.2 ) df=4 x2=12.0 p=0.018
Table 2. Student’s satisfaction with course content and small-group tutorial format in three different academic year class
Degree of satisfaction 1995 (N=112) 1996 (N=126) 1997 (N=121) Total ( N=359 ) Statistics Cour se content
Very much/ Much Moderate Slight/ None 77 ( 68.8 ) 31 ( 27.7 ) 4 ( 3.6 ) 93 ( 73.8 ) 28 ( 22.2 ) 5 ( 4.0 ) 83 ( 68.6 ) 31 ( 25.6 ) 7 ( 5.8 ) 253 ( 70.5 ) 90 ( 25.1 ) 16 ( 4.5 ) df=4 x2=2.18 N.S.
Teaching for mat
Very much/ Much Moderate Slight/ None 63 ( 56.3 ) 41 ( 36.6 ) 8 ( 7.1 ) 88 ( 69.8 ) 32 ( 25.4 ) 6 ( 4.8 ) 67 ( 55.4 ) 44 ( 36.4 ) 10 ( 8.3 ) 218 ( 60.7 ) 117 ( 32.6 ) 24 ( 6.7 ) df=4 x2= 6.93 N.S.
Table 3. Students’ perceptions on the importance of medical ethics education to career and development and the optimal
academic year for implementation of medical ethics course in two classes 1995 N (%) 1996 N (%) 1997 N (%) P value
Degr ee of impor tance
Very important 60 ( 53.1 ) 91 ( 72.2 ) 53 ( 43.8 )
Important 44 (38.9) 33 ( 26.2 ) 57 ( 47.1 ) NS
Moderately important 9 ( 8.0 ) 1 ( 0.8 ) 10 ( 8.3 ) Slightly important or not important 0 ( 0.0 ) 1 ( 0.8 ) 1 (0.8 )
Optimal academic year
Premedical years 1, 2 1 ( 0.9 ) 2 ( 1.6 ) 9 ( 7.6 ) Premedical years 3, 4 10 ( 8.8 ) 3 ( 2.4 ) 10 ( 8.4 )
Clinical year 5 13 (11.5 ) 22 ( 17.9 ) 32 ( 26.9 ) NS Clinical year 6 72 (63.7 ) 83 ( 67.5 ) 59 ( 49.6 )
Internship year 7 17 (15.0 ) 13 ( 10.6 ) 9 ( 7.6 )
Table 4. Time (hours) spent studying medical ethics outside the classroom in three years
1995 1996 1997
Pr epar ation for or al pr esentation and discussion
Mean±SD 14.3±13.6 13.83±10.82 13.30±11.33
Median 10.0 11.0 10.0
Range 3-92 3-100 3-72
Wr iting the ter m paper
Mean±SD 18.2±15.2 19.96±31.45 15.35±20.95
Median 13.0 14.0 10.0
N=112 Mean±SD N=125 Mean±SD N=121 Mean±SD N=359 Mean±SD P Interpersonal learning 9.02±2.78 9.78±2.39 9.51±2.41 9.45±2.54 .064 Engagement 12.04±2.62 13.28±2.63 12.37±2.61 12.58±2.67 .001 Interpersonal relationship 11.21±3.13 11.83±3.28 11.59±3.15 11.55±3.19 .322 Self-presentation 4.55±1.43 5.20±1.44 4.54±1.47 4.77±1.48 .000 Avoidance 2.55±2.34 2.94±2.20 3.15±2.38 2.89±2.31 .140 1、 By one way Anova
2、 By Scheffe’s range test; for engagement, 1996>1995,p=.001;1997>1995, p=.027 3、 By Scheffe’s range test; for self-presentation, 1996>1995, p=.002; 1996>1997, p=.003
Table 6. Correlations between gain of ethical knowledge and ethical reasoning and group learning factors
Ethical knowledge Ethical reasoning
Interpersonal learning -.399** -.431**
Engagement -.284** -.286**
Interpersonal relationship -.256** -.187**
Self-presentation -.200** -.199**
Degree of devotion to the task .197* .195**
Avoidance conflict .112* .133*
**P<0.01 * P<0.05
Table 7-1. Predictive value of items (independent variables) in group Interaction and Group Climate on degree of gain on ethical
knowledge (dependent variables) by stepwise multiple regression analysis (N=359)
F p
Step Variables R R Square
42 1 2 3 4 5 6 Classmate’s comments Considered instructor as a model
Feeling of involvement in group interaction Concerned about classmate’s viewpoints Dedication to write term paper
Concerned about and appreciated classmates or instructors
0.353 0.405 0.432 0.449 0.462 0.477 0.125 0.164 0.187 0.202 0.214 0.228 46.261 31.728 24.733 20.321 17.455 15.739 .000 .000 .000 .000 .000 .000
Table 7-2. Predictive value of dimensions of Group Learning Scales (independent variables) on degree of gain of ethical
knowledge (dependent variables) by stepwise multiple regression analysis (N=359)
F p
Step Variables R R Square
42 1 2 Interpersonal learning Engagement 0.389 0.418 0.158 0.175 65.843 37.033 .000 .000
Table 8-1. Predictive value of items (independent variables) in Group Interaction and Group Climate on degree of gain on ethical
reasoning (dependent variables) by stepwise multiple regression analysis (N=359)
Step Variables Entered R R Square F p 1 2 3 4 5 Classmate’s comments Considered instructor as model
Awareness of personal abilities and limitations Feeling of involvement in group interaction Others shared their viewpoints with me
0.386 0.449 0.476 0.488 0.501 0.149 0.201 0.227 0.238 0.251 57.017 40.800 31.560 25.110 21.476 .000 .000 .000 .000 .000
Table 8-2. Predictive value of dimensions of Group Learning Scale (independent variables) on degree of gain of
ethical reasoning (dependent variables) by stepwise multiple regression analysis (N=359) Step Variables Entered R R Square F p 1 2 Interpersonal learning Engagement 0.428 0.443 0.183 0.197 78.486 42.711 .000 .000
Table 9-1 Information disclosure and Interactional issues of physician-patient relations by sex Male N (%) Female N (%) Total N (%) P 1、Understanding of diagnosis None/slight Moderate/Much 37 (35.9) 66 (64.1) 48 (56.5) 37 (43.5) 85 (45.2) 103 (54.8) .00538 2、Understanding of treatment None/Slight Moderate/Much 36 (35.6) 65 (64.4) 46 (56.8) 35 (43.2) 82 (45.1) 100 (54.9) .00680 3、Doctor-patient Communication None/Slight Moderate/Much 42 (41.2) 60 (58.8) 43 (51.2) 41 (48.8) 85 (45.7) 101 (54.3) .18588 4、Difficulty of communication by psychiatrist’s view
None/Slight Moderate/Much 74 (71.8) 29 (28.2) 65 (76.5) 20 (23.5) 139 (73.9) 49 (26.1) .50776 By fisher’s exact test
Table 9-2 Information disclosure and Interactional issues of physician-patient relations by Psychiatric Diagnosis Yes N (%) No N (%) Total N (%) P 1、Understanding of diagonal None/slight Moderate/Much 69 (54.8) 57 (45.2) 16 (25.8) 46 (74.2) 85 (45.2) 103 (54.8) .00018 2、Understanding of treatment None/Slight Moderate/Much 71 (57.7) 52 (42.3) 11 (18.6) 48 (81.4) 82 (45.1) 100 (54.9) .000 3、Doctor-patient communication None/Slight Moderate/Much 73 (58.4) 52 (41.6) 12 (19.7) 49 (80.3) 85 (45.7) 101 (54.3) .000 4、Difficulty of communication by psychiatrist’s view
None/Slight Moderate/Much 88 (69.8) 38 (30.2) 51 (82.3) 11 (17.7) 139 (73.9) 49 (26.1) .07849 By fisher’s exact test