行政院國家科學委員會專題研究計畫 成果報告
三酸甘油酯過高病人之治療對低密度脂蛋白及高密度脂蛋
白細分類, 以及內皮細胞功能之影嚮
計畫類別: 個別型計畫 計畫編號: NSC91-2314-B-002-282- 執行期間: 91 年 08 月 01 日至 92 年 07 月 31 日 執行單位: 國立臺灣大學醫學院內科 計畫主持人: 廖朝崧 計畫參與人員: 陳菀菁,蔡齡鈺 報告類型: 精簡報告 處理方式: 本計畫可公開查詢中 華 民 國 93 年 2 月 16 日
國
國
科
科
會
會
專
專
題
題
研
研
究
究
計
計
畫
畫
成
成
果
果
報
報
告
告
撰
撰
寫
寫
格
格
式
式
一、說明 國科會基於學術公開之立場,鼓勵一般專題研究計畫主持人發表其研究成 果,但主持人對於研究成果之內容應負完全責任。計畫內容及研究成果如涉及 專利或其他智慧財產權、違異現行醫藥衛生規範、影響公序良俗或政治社會安 定等顧慮者,應事先通知國科會不宜將所繳交之成果報告蒐錄於學門成果報告 彙編或公開查詢,以免造成無謂之困擾。另外,各學門在製作成果報告彙編時, 將直接使用主持人提供的成果報告,因此主持人在繳交報告之前,應對內容詳 細校對,以確定其正確性。 本格式說明僅為統一成果報告之格式,以供撰寫之參考,並非限制研究成 果之呈現方式。精簡報告之篇幅(不含封面之頁數)以 4 至 10 頁為原則,完整 報告之篇幅則不限制頁數。 成果報告繳交之期限及種類(精簡報告、完整報告或期中報告等),應依本 會補助專題研究計畫作業要點及專題研究計畫經費核定清單之規定辦理。 二、內容格式:依序為封面、中英文摘要、目錄(精簡報告得省略)、報告內容、參 考文獻、計畫成果自評、可供推廣之研發成果資料表、附錄。 (一)報告封面:請至本會網站(http://www.nsc.gov.tw)下載製作(格式如附件一)。 (二)中、英文摘要及關鍵詞(keywords)。 (三)報告內容:請包括前言、研究目的、文獻探討、研究方法、結果與討論(含 結論與建議)…等。若該計畫已有論文發表者,可以 A4 紙影印,作為成果 報告內容或附錄,並請註明發表刊物名稱、卷期及出版日期。若有與執行 本計畫相關之著作、專利、技術報告、或學生畢業論文等,請在參考文獻 內註明之,俾可供進一步查考。 (四)頁碼編寫:請對摘要及目錄部分用羅馬字 I 、II、 III……標在每頁下方中 央;報告內容至附錄部分請以阿拉伯數字 1.2.3.……順序標在每頁下方中央。 (五)附表及附圖可列在文中或參考文獻之後,各表、圖請說明內容。 (六)計畫成果自評部份,請就研究內容與原計畫相符程度、達成預期目標情況、 研究成果之學術或應用價值、是否適合在學術期刊發表或申請專利、主要 發現或其他有關價值等,作一綜合評估。 (七)可供推廣之研發成果資料表:凡研究性質屬應用研究
及技術發展
之計畫, 請依本會提供之表格(如附件二),每項研發成果填寫一份。 三、計畫中獲補助國外或大陸地區差旅費、出席國際學術會議差旅費或國際合作研 究計畫差旅費者,須依規定撰寫心得報告(出席國際學術會議者須另附發表之 論文),以附件方式併同成果報告繳交,並請於成果報告封面註記。 四、打字編印注意事項 1. 用紙 使用 A4 紙,即長 29.7 公分,寬 21 公分。 2. 格式 中文打字規格為每行繕打(行間不另留間距),英文打字規格為 Single Space。 3. 字體報告之正文以中英文撰寫均可。在字體之使用方面,英文使用 Times New Roman Font,中文使用標楷體,字體大小請以 12 號為主。
行政院國家科學委員會補助專題研究計畫
; 成 果 報 告
□期中進度報告
(計畫名稱)
計畫類別:; 個別型計畫 □ 整合型計畫
計畫編號:NSC 91-2314-B-002-282-
執行期間:91 年 8 月 01 日至 92 年 7 月 31 日
計畫主持人:廖朝崧
共同主持人:
計畫參與人員: 陳菀菁,蔡齡鈺
成果報告類型(依經費核定清單規定繳交):□精簡報告 □完整報告
本成果報告包括以下應繳交之附件:
□赴國外出差或研習心得報告一份
□赴大陸地區出差或研習心得報告一份
□出席國際學術會議心得報告及發表之論文各一份
□國際合作研究計畫國外研究報告書一份
處理方式:除產學合作研究計畫、提升產業技術及人才培育研究計畫、
列管計畫及下列情形者外,得立即公開查詢
□涉及專利或其他智慧財產權,□一年□二年後可公開查詢
執行單位:台大醫學院 內科
附件一中 華 民 國 93 年 2 月 15 日
可供推廣之研發成果資料表
□ 可申請專利 □ 可技術移轉 日期:93 年 2 月 15 日國科會補助計畫
計畫名稱:三酸甘油酯過高病人之治療對低密度脂蛋白及高密度脂 蛋白細分類以及內皮細胞功能之影響 計畫主持人: 廖朝崧 計畫編號:NSC 91-2314-B-002-282 學門領域:技術/創作名稱
發明人/創作人
中文: (100~500 字)技術說明
英文:可利用之產業
及
可開發之產品
技術特點
推廣及運用的價值
※ 1.每項研發成果請填寫一式二份,一份隨成果報告送繳本會,一份送 貴單位 研發成果推廣單位(如技術移轉中心)。 ※ 2.本項研發成果若尚未申請專利,請勿揭露可申請專利之主要內容。 ※ 3.本表若不敷使用,請自行影印使用。 附件二The effects of treatment of hypertriglyceridemia on the subfractions of LDL and HDL and the endothelial function
三酸甘油酯過高病人之治療對低密度脂蛋白及高密度脂蛋白細分類, 以及內皮細胞功能之影嚮 中文摘要: 高三酸甘油酯血症在中國人是相當常見的血脂異常,過去對於三酸甘油酯與動脈硬化 的關係有諸多爭議,但近年來已認為三酸甘油酯是動脈硬化的一個獨立危險因子。高三酸 甘油酯血症同時也是新陳代謝症候群的一個主要角色。富含三酸甘油酯的脂蛋白在人類具 有高度誘發動脈硬化之作用。本研究探討高三酸甘油酯血症對單核細胞粘附作用及內皮細 胞功能之影響。一共有 90 位病人進行 122 次試驗,其中 30 人進行 2 次試驗。結果發現, 經治療後病人的血脂都有明顯改變,三酸甘油酯明顯下降,高密度脂蛋白膽固醇明顯上升。 單核細胞粘附作用並未受三酸甘油酯所影響,但與低密度酯蛋白膽固醇有關。三酸甘油酯 過高病人其內皮細胞功能變差,但經治療,三酸甘油酯下降後則內皮細胞功能恢復。總結 之,三酸甘油酯並非決定單核細胞粘附作用之重要因素,但低密度脂蛋白膽固醇則是。高 三酸甘油酯血症可明顯造成內皮細胞功能失常,此一失常在三酸甘油酯改善後可以獲得改 善。 關鍵詞:高三酸甘油酯血症,動脈硬化,糖尿病,低密度脂蛋白,低密度脂蛋白細分類, 高密度脂蛋白,高密度脂蛋白細分類,內皮細胞功能 Abstract
Hypertriglyceridemia is a very common lipid disorder in Chinese. The role of high serum
triglyceride (TG) in atherosclerosis has been controversial for a long time, but recently it has been widely accepted that TG is definitely an independent risk factor for atherosclerosis.
Hypertriglyceridemia is one important component of metabolic syndrome. TG-rich lipoproteins have been identified highly atherogenic in humans. We studied the effects of
hypertriglyceridemia on in vitro mononuclear cell adhesion to cultured human endothelial cells and the in vivo endothelial function by using brachial artery flow mediated dilatation method. A total of 90 patients with 122 tests were completed. Thirty patients had 2 studies. We found that after intervention the patients had their lipid profile markedly changed with reduction of TG and increase of HDL-C. The mononuclear cell adhesion was found not correlated with serum TG level but could be affected by LDL-C level. Patients with high TG levels had impaired
endothelial function which was found improved after reduction of the serum TG levels. It was concluded that TG was not an important factor in determining the adhesion of mononuclear cells to endothelial cells but LDL-C was. Hypertriglyceridemia could significantly affect the
endothelial function through impairment of flow-mediated vasodilatation.
Key words: hypertriglyceridemia; atherosclerosis; diabetes mellitus; low density lipoprotein; low
endothelial function
INTRODUCTION
The role of hypertriglyceridemia (HTG) in the pathogenesis of atherosclerosis has been a controversy for decades (1,2). This fact is reflected in the previous National Cholesterol
Education Program (NCEP) guidelines for the treatment of high blood cholesterol published in 2002 (3) and the rules for the use of lipid lowering drugs set by the National Health Insurance of Taiwan. Austin reviewed 17 case-control studies and 18 prospective studies and concluded that there is a significant correlation between serum triglyceride (TG) levels and coronary artery disease (CAD) (2). Recent studies further demonstrated HTG as an independent risk factor for atherosclerosis and CAD (4-7). In the newest NCEP guidelines (published in 2002), the importance of TG was more mentioned and the prominent role of metabolic syndrome was especially emphasized (3).
Hypertriglyceridemia is one important component of the insulin resistance-linked "metabolic syndrome" (3). TG-rich lipoproteins, such as very low density lipoprotein remnant and
intermediate dense lipoprotein, have been identified highly atherogenic (8,9). Some large scale clinical trials also showed the efficacy of TG-lowering regimens on the secondary as well as primary prevention of coronary heart disease (10).
In Taiwan, the prevalence of non-insulin dependent diabetes mellitus (DM) is high and is increasing in recent years. DM is closely related to atherosclerosis (11-16). Yet, only about 25-50% of the excess risk of atherosclerosis can be attributed to traditional risk factors. Among the additional risk factors, quantitative and qualitative abnormalities in serum lipoproteins, especially the TG-rich lipoproteins, in diabetics is proposed to be very important risk factors (17-22). In daily practice in taking care of cardiovascular patients, we found that a high percentage of atherosclerotic patients are diabetics and the CAD patients with DM are very frequently presented with extreme severity and wide spread distribution of the atherosclerotic lesions.
Hypertriglyceridemia has been found to be associated with small, dense low density lipoprotein (LDL), small, dense very low density lipoprotein (VLDL), increased intermediate density lipoprotein (IDL) and decreased high density lipoprotein (HDL), mainly HDL2b (2,4,8,20). As to our knowledge, there are few, if any, reported studies on the changes of
endothelial function and the level and composition of LDL and HDL in patients with HTG after lipid lowering medication. This kind of studies are especially lack in Chinese in Taiwan.
PURPOSE OF THE STUDY
1) to study the lipid profile and lipid composition, including LDL subfractions and HDL level and subfractions, in patients with HTG (>200 mg/dl) with or without DM; 2) to study the effects of medical interventions, including life style modification and drug therapy, on the lipid profile and lipid composition of patients with high TG;
3) to study the effects of improvement of HTG on human endothelial function, by measuring flow-mediated dilatation of the brachial artery with high resolution ultrasound; and
4) to study the effects of treatment on HTG on mononuclear cell adhesion to cultured human umbilical vein endothelial cells before and after medical intervention.
It is expected that through this study the patterns of subfractions of LDL and HDL in Chinese patients with HTG may be identified. The benefits of treatment on HTG may be
confirmed which may contribute to the prevention and treatment of atherosclerotic cardiovascular disorders.
SUBJECTS AND METHODS 1. Study subjects
The study subjects included patients with HTG (200-500 mg/dl) with normal (total cholesterol <200 mg/dl) or borderline high (total cholesterol 200-239 mg/dl) cholesterol (3). Totally, 90 cases were included and 122 studies were performed. There were 31 patients with DM and 59 patients without DM.
2. Study procedure
The study subjects had blood samples checked for fasting serum lipids and fasting glucose and, when indicated, 2-hour PC glucose and HbA1c. Patients with serum TG levels fitting the study criteria were invited to participate in this study. All participants had signed an inform consent.
On the initial phase of this study, the patients were asked to be fasting for 12 hours. Blood samples were taken for analyzing subfractions of LDL and HDL and for the study of adhesion of mononuclear cells to cultured human umbilical vein endothelial cells (HUVEC) (see below). A study on brachial artery flow mediated dilatation for endothelial function was
performed in fasting state (23).
The patients were then instructed to start life style modification which included body weight control, exercise, diet control and smoking cessation. Lipid profile after life style modification was rechecked in 1-2 months. If the TG levels decreased to normal range (<200 mg/dl), the studies on subfractions of LDL and HDL, brachial artery flow mediated dilatation, and the study of mononuclear cell adhesion were repeated. If the TG levels do not reach this target (<200 mg/dl), lipid lowering regimens were started. The potential drugs may be fibrates and/or statins, depending on the profile of lipid abnormality and the response of the patients to medication. The response of the patients was followed with regular blood examination for lipid profile. If the TG levels decrease to normal range (<200 mg/dl) or with marked decrease
(decrease by >30% initial level), the studies on subfractions of LDL and HDL, brachial artery flow mediated dilatation, and the study of mononuclear cell adhesion were repeated.
3. Study on brachial artery flow mediated dilatation
Brachial artery flow mediated dilatation was studied according to the method of Celermajer et al (23). In brief, after fasting for at least 12 hours, the patients first rested quietly for 10 minutes before study. A high resolution ultrasound instrument (Hewlett-Packard Sonos 5500) with a 7.5 MHz linear array probe was used for the measurement of the right brachial artery diameter 3-5 cm above the elbow. The end-diastolic media-to-media distance was measured. After that measurement, a blood pressure cuff was applied to the right arm and a blood pressure 30 mmHg higher than the systolic blood pressure is applied to occlude the blood flow to the right forearm for 4.5 minutes. The diameter of the brachial artery was measured again 1 minute after decompression (flow-mediated dilatation). To study the endothelium-independent dilatation, the patients received one tablet of sublingual nitroglycerin (0.6 mg) and the brachial artery diameter was measured again and maximum diameter recorded.
4. Study on mononuclear cell adhesion to HUVEC
The mononuclear cell adhesion to the cultured HUVEC was carried out by the method of Berliner et al (24).
a) Isolation of serum
Fasting venous blood from patients was collected in tubes containing EDTA. One tube of blood (3 ml) is centrifuged at 3000 rpm for 15' and plasma was collected and stored at -70 degree C, and used for analysis later.
b) Isolation of mononuclear cells
To isolate mononuclear cells from the blood, the method of Menon et al. was used (25). Anticoagulated human blood (with EDTA) was layered over an equal volume of Histopaque 1077 (Sigma), and then centrifuged at 400 x g for 30' at room temperature. Mononuclear cells were collected from the interphase, resuspended in Tris buffer (TBS, 20 mM Tris, 0.15 M NaCl, pH 7.4). After sedimentation by centrifugation at 250 g for 10', the cells were washed and
resuspended in TBS buffer and ready for use in experiments.
c) Adhesion study
HUVEC were cultured in 6-well culture plates. At confluence, HUVECs were rinsed with serum-free medium for 3 times. Mononuclear cells from the patients, 2x105 cells in 250 µl in DMEM containing 1% heat-inactivated serum, were added to each well, and then kept in incubator at 37-degree C. After 1 h, the non-adherent mononuclear cells were rinsed off and the wells fixed with 1% glutaraldehyde. The attached cells were counted in each of 20 microscopic fields.
5. Study on LDL subfractions and HDL subfractions
method, LDL could be separated into LDL-I, LDL-II and LDL-III. As found by Griffin, in CAD patients, the LDL-III was especially elevated and which was corresponding to small, dense LDL as detected by non-denaturing gradient gel electrophoresis. For comparison, in this study, the LDL subfractions were also analyzed using gradient gel electrophoresis according to the methods of Krauss (27).
The HDL subfractions were studied by the combined precipitation method using polyethylene glycol 6000 and dextran sulfate, as described by Lundberg (28).
RESULTS Study population
There were totally 90 cases collected in this study with a total of 122 studies performed. Thirty-one of the study subjects were diabetic, 59 were non-diabetic. The mean age was 62.9+9.9 years (range 39 to 78 years). Sixty patients had 1 single study while 30 patients had 2 studies. Most of the patients with more than one study had their triglyceride levels improved or controlled to normal ranges after intervention.
Lipid Changes
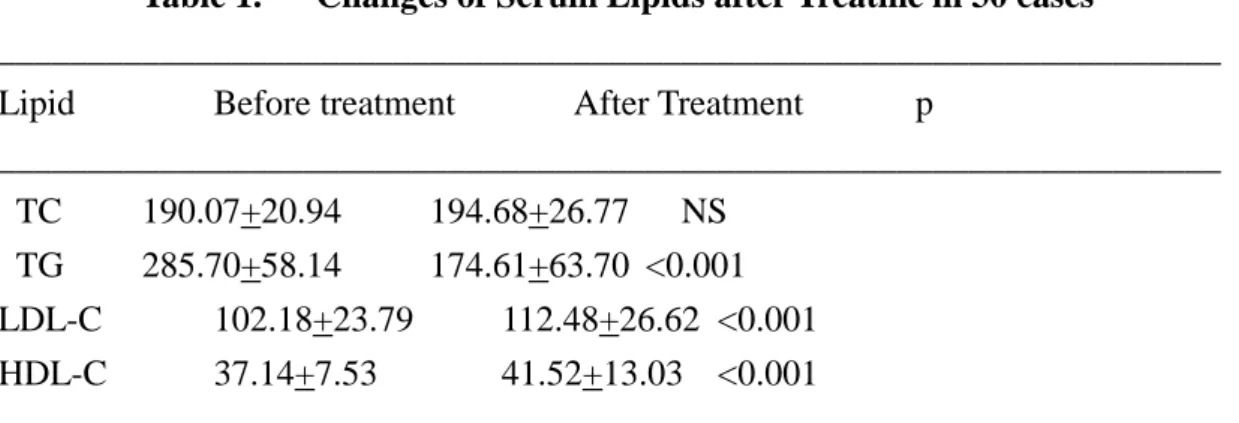
For all studies as a whole, the lipid data were as follows: total cholesterol, 199.07+26.05 mg/dl; triglyceride, 255.81+93.49 mg/dl; LDL-C, 109.37+23.75 mg/dl; HDL-C, 39.52+9.76 mg/dl. Among the 30 patients who had 2 studies, the lipid data before intervention were: total cholesterol, 190.07+20.94 mg/dl; triglyceride, 285.7+58.14 mg/dl; LDL-C, 102.18+23.79 mg/dl; HDL-C, 37.14+7.53 mg/dl. These data changed to: total cholesterol, 194.68+26.77 mg/dl; triglyceride, 174.61+63.7 mg/dl; LDL-C, 112.48+26.62 mg/dl; HDL-C, 41.52+13.03 mg/dl. The changes were significant for triglyceride (285.7+58.14 mg/dl vs. 174.61+63.7 mg/dl, p<0.001), LDL-C (102.18+23.79 mg/dl vs. 112.48+26.62 mg/dl, p<0.001) and HDL-C (37.14+7.53 mg/dl vs. 41.52+13.03 mg/dl, p<0.001) (Table 1).
Table 1. Changes of Serum Lipids after Treatme in 30 cases
____________________________________________________________________ Lipid Before treatment After Treatment p
____________________________________________________________________ TC 190.07+20.94 194.68+26.77 NS TG 285.70+58.14 174.61+63.70 <0.001 LDL-C 102.18+23.79 112.48+26.62 <0.001 HDL-C 37.14+7.53 41.52+13.03 <0.001 ___________________________________________________________________ *TC= total cholesterol; TG= triglyceride; LDL-C= low density lipoprotein cholesterol; HDL-C= high density lipoprotein cholesterol.
Mononuclear cell adhesion and brachial artery flow mediated dilatation
In comparing with the reference subject (the principal investigator), the mononuclear cell
adhesion to the cultured HUVEC was found to be 107.38+47.19% for all 122 studies. For the 60
patients who had only one study, the cell adhesion was averaged 110.59+59.15%. For the patients
with 2 studies, the cell adhesion data for the first and second studies were 105.05+32.06% and
102.43+34.02%, respectively (p=NS). It was found that mononuclear cell adhesion to cultured
HUVECs was affected by the level of serum LDL-C among the all studies as a group (p=0.047)
or among the patients who had only one study (p=0.044).
In the study of brachial artery flow mediated dilatation, for all studies, the mean
brachial artery diameter was 4.5+0.65 mm at basal state which increased to 4.95+0.65 mm after
pressure application (increment, 0.45+0.25 mm). For the patients who had only one study, the
data for the brachial artery flow mediated dilatation study were 4.39+0.66 mm and 4.81+0.62 mm,
respectively, with an increment of 0.42+0.25 mm. For the patients with 2 studies, the data for the
first study were 4.57+0.61 mm at basal condition which increased to 5.0+0.7 mm after pressure
application (increment, 0.43+0.24 mm or 9.85+0.93%). At the second study, the data were: at
basal, 4.64+0.64 mm; after pressure, 5.14+0.59 mm; increment, 0.5+0.25 mm, 11.23+1.11%.
There was no significant difference between the two studies. Yet, it was interesting to note that, in
comparing the second study to the first study, the percent change of the brachial artery diameter
after nitroglycerin application was significantly increased (11.98+1.05% vs. 12.22+1.15%,
p=0.011).
In correlating the brachial artery flow mediated dilatation with the lipid levels, we
found that in patients with 2 studies, this correlation was significant at the first study when serum
TG was abnormally high (p=0.021). This correlation disappeared at the second study when the
abnormality of TG improved.
HDL and LDL subfraction study
we studied 31 cases. We did subfraction analysis on all lipids. For HDL, we could separate it into
2 to 5 fractions and for LDL, more than 4 fractions, might up to more than 10 fractions, according
to the electric charges. We will perform further analysis for the collected serum samples in the
near future to complete this work.
DISCUSSION
It was found that, among our study subjects, after intensive life style modification and, if
necessary, drug management, the serum TG level could be significantly reduced and, at the same
time, HDL-C increased. But, we also observed that, in our cases, the LDL-C was significantly
increased (from 102.18 mg/dl to 112.48 mg/dl).
Unexpectedly, we could not found a correlation between serum TG level and in vitro
mononuclear cell adhesion. As we initially proposed, we detected a correlation between serum
TG level and endothelial cell function as studied by the brachial artery flow mediated dilatation
method. After improvement in serum TG level, the endothelial cell function became improved in
hypertriglyceridemic patients. It may be interesting to note that after improvement in serum TG
level, the endothelial independent arterial dilatation, as studied by NTG application, was also
improved. The mechanism may need further investigation.
We will continue our work on the subfraction studies on lipids. This part seems to give
interesting information about the correlation between lipid abnormalities and cell adhesion and
endothelial function.
References
1. Hulley SB, Rosenman RH, Bawol RD, Brand, RJ. Epidemiology as a guide to clinical decisions: The association between triglyceride and coronary heart disease. N Engl J Med 1980;302:1383-9.
2. Austin MA. Plasma triglyceride and coronary heart disease. Arterioscler Thromb 1991;11:2-14.
3. Third Report of the National Cholesterol Education Program (NCEP) Expert Panel on Detection, Evaluation, and Treatment of High Blood Cholesterol in Adults (Adult Treatment Panel III) Final Report. Circulation 2002;106:3143-421.
4. Gotto AM. Triglyceride the forgotten risk factor. Circulation 1998;97:1027-8. 5. Jeppesen J. Triglyceride concentration and ischemic heart disease. An eight-year
follow-up in the Copenhagen Male Study. Circulation 1998;97:1029-36. 6. Hokanson JE, Austin MA. Plasma triglyceride level is a risk factor for
cardiovascular disease independent of high-density lipoprotein cholesterol level: a meta analysis of population-based prospective studies. J Cardiovasc Risk
1996;3:213-9.
7. Tanne D, Koren-Morag N, Graff E, Goldbourt U. Blood lipids and first-ever ischemic stroke/transient ischemic attack in the Bezafibrate Infarction Prevention (BIP) Registry. High triglycerides constitute an independent risk factor. Circulation 2001;104:2892-97. 8. Cohn JS, Marcoux C, Davignon J. Detection, quantification, and characterization
of potentially atherogenic triglyceride-rich remnant lipoproteins. Arterioscler Thromb Vasc Biol 1999;19:2474-86.
9. Sniderman AD, Scantlebury T, Cianflone K. Hypertriglyceridemic hyperapoB: the unappreciated atherogenic dyslipidemia in type 2 diabetes mellitus. Ann Intern
Med 2001;135:447-59.
10. Rubins HB, Robins SJ, Collins D, et al. Gemfibrozil for the secondary prevention of coronary heart disease in men with low level of high density lipoprotein cholesterol. N Engl J Med 1999;341:410-8.
11. Pyorala K, Laakso M, Uusitupa M. Diabetes and atherosclerosis: an epidemiologic view. Diabetes Metab Rev 1987;3:463-524.
12. Pan WH, Cedres LB, Liu K, et al. Relationship of clinical diabetes and asymptomatic hyperglycemia to risk of coronary heart disease mortality in men and
women. Am J Epidemiol 1986;123:504-56.
13. Krolewski AS, Kosinski EJ, Warram JH, et al. Magnitude and determinants of coronary artery disease in juvenile-onset, insulin-dependent diabetes mellitus. Am J
Cadiol 1987;59:750-5.
14. Kannel WB. Lipid, diabetes, and coronary heart disease: insight from the Framingham study. Am Heart J 1985;110:1100-7.
15. Steiner G. Atherosclerosis, the major complication of diabetes. Adv Exp Med Biol 1985;189:277-97.
16. Bierman EL. Atherogenesis in diabetes. Arterioscler Thromb 1992;12:647-56. 17. Steiner G. Intermediate-density lipoproteins, diabetes and coronary artery disease.
Diab Res Clin Prac 1998;40:(Suppl)S29-33.
18. Tkac I, Kimball BP, Lewis G, Uffelman K, Steiner G. The severity of coronary atherosclerosis in type 2 diabetes mellitus is related to the number of circulating
triglyceride-rich lipoprotein particles. Arterioscler Thromb Vasc Biol 1997;17:3633-8.
19. Steiner G, Lewis GF. Hyperinsulinemia and triglyceride-rich lipoproteins. Diabetes 1996;45:(Suppl 3)S24-S26.
20. Lewis GF, Steiner G. Hypertriglyceridemia and its metabolic consequences as a risk factor for atherosclerotic cardiovascular disease in non-insulin-
dependent diabetes mellitus. Diab Metab Rev 1996;12:37-56.
21. Bae JH, Bassenge E, Lee HJ, et al. Impact of postprandial hypertriglyceridemia on vascular responses in patients with coronary artery disease: effects of ACE
inhibitors and fibrate. Atheroscler 2001;158:165-71.
22. WHO Study Group. Diabetes mellitus. Report of WHO Study Group. Tech Rep Ser 1985;727:1-113.
23. Celermajer DS, Sorensen KE, Gooch VM, et al. Non-invasive detection of endothelial dysfunction in children and adults at risk of atherosclerosis. Lancet 1992;340:1111-5.
24. Berliner JA, Territo MC, Sevanian A, Ramin S, Kim JA, Bamshad B, Esterson M, Fogelman AM. Minimally modified low density lipoprotein stimulates monocyte endothelial interactions. J Clin Invest 1990;85:1260-6. 25. Menon RP, Sudhakaran PR. Enhanced adhesion of human mononuclear cells to nonenzymatically glycosylated collagen I. Mol Cell Biochem 1995;148:115-21.
26. Griffin BA, Caslake MJ, Yip B, et al. Rapid isolation of low density lipoprotein (LDL) subfractions from plasma by density gradient ultracentrifugation.
Atherosclerosis 1990;83:59-67.
27. Krauss RM. Heterogeneity of plasma low-density lipoprotein and atherosclerosis risk. Curr Opin Lipidol 1994;5:339-49.
28. Lundberg B, Hogstrom S, Pietilainen P, et al. Separation of plasma high-density lipoprotein subclasses by a combined precipitation method using
polyethylene glycol 6000 and dextran sulfate. Scand J Lab Invest 1984;44:305-9.