探討遠距照護服務之關鍵因子 - 政大學術集成
81
0
0
全文
(2) Exploring key service features that impact the intention, adoption, and continued use of e-health services. ABSTRACT According to previous research, e-health systems must be customer-focused to survive in today’s competitive market. Although previous studies have discussed e-health ICT usage, few studies have focused on the customer’s point of view. It is still unclear what customers’ requirements for good e-health service are. Thus, this research attempts to determine the service features that affect customers’ intention to adopt and use e-health services. We use the service concept to classify the service features into five categories: by whom, what, for whom, when, and how. We are. 治 政 interested in discovering these service features that can大 trigger the interest of potential 立 customers, enhance their willingness to adopt the service, and motivate the existing. ‧ 國. 學. customers to continue using the service.. ‧. The results of this research have shown that the factors that affect people’s intention to adopt the services are: the channel to join the service, the components of the services, disease type and ages , the frequency of service supply, and the satisfaction of service and platform. Also, the factors that affect people adopt the services include: the channel to join the service, the components of the service, disease type and ages, the frequency of service supply, and the satisfaction of service and platform Furthermore, the result shows the factors that affect people to continue using the service are: the component of the service, disease type and ages and the satisfaction of service and platform.. n. er. io. sit. y. Nat. al. Ch. engchi. i Un. v. Keywords: e-health, telecare, service features, service adoption, service usage. ii .
(3) CONTENTS ABSTRACT .......................................................................................................................... II CONTENTS ......................................................................................................................... III CHAPTER 1 – INTRODUCTION ................................................................................... 1 CHAPTER 2: LITERATURE REVIEW ........................................................................ 3 2.1 E-health care service design issues .......................................................................... 3 2.1 By Whom (service delivery) .................................................................................... 3 . 政 治 大. 2.2 What (service offerings)........................................................................................... 4 . 立. 2.3 For Whom (customer segment) ............................................................................... 7 . ‧ 國. 學. 2.4 When (user demands) .............................................................................................. 7 . ‧. 2.5 How (satisfaction) .................................................................................................... 7 . sit. y. Nat. CHAPTER 3-RESEARCH MODEL AND HYPOTHESIS ........................................ 9 . n. al. er. io. 3.1 Research Model ....................................................................................................... 9 . Ch. i Un. v. 3.2.1 Service features - By whom ................................................................................ 10 . engchi. 3.2.2 Service features – What ...................................................................................... 11 3.2.3 Service features - For whom ............................................................................... 12 3.2.4 Service features – When ..................................................................................... 12 3.2.5 Service features – How ....................................................................................... 12 CHAPTER 4-RESEARCH PLAN ................................................................................. 14 4.1 Case Background ................................................................................................... 14 4.2 Measurements ........................................................................................................ 14 4.3 Data Collection ...................................................................................................... 17 iii .
(4) 4.4 Reliability............................................................................................................... 20 4-5 Discriminant validity ............................................................................................. 22 CHAPTER 5: RESULTS AND DISCUSSION............................................................ 24 5.1 Results .................................................................................................................... 24 5.1 .1 Factors that affect the intention to adopt E-health ............................................. 24 5.1 .2 Factors that affect the adoption of e-health........................................................ 27 5.1. 3 Factors that affect people’s continued use of e-health ....................................... 30 5.1.4 The summary of our analysis .............................................................................. 33 . 政 治 大. 5.2 Findings.................................................................................................................. 35 . 立. ‧ 國. 學. CHAPTER 6: CONCLUSION ....................................................................................... 39 6.1 Summary ................................................................................................................ 39 . ‧. REFERENCE ..................................................................................................................... 17 . y. Nat. n. al. er. io. sit. APPENDIXA: QUSTIONAIRE ..................................................................................... 47 . i Un. v. APPENDIXB: THE APPROVAL OF NTUH INSTITUTIONAL REVIEW BOARD ................................................................................................................................ 53 . Ch. engchi. APPENDIX C THE ANOVA TABLE OF INTENTION TO ADOPTION ........... 54 APPENDIX D THE ANOVA TABLE OF ADOPTION ............................................ 62 . iv .
(5) CHAPTER 1 – INTRODUCTION Health care providers have long wished to have access to patient information for more effective diagnosis and treatment.(González, Quesada et al. 2006). As information and communication technology (ICT) has developed, e-health has drawn attention from the public. E-health has changed the vision of health care. One definition of e-health care is the use of ICT to enhance health care. E-health care is used to describe most aspects of healthcare delivery or management that are enabled by ICT. (Oh H 2005). According to the World Health Organization (WHO), e-health is health care combined with the usage of electronic communication and information technology in the health sector as well as the delivery, capability and support of health care components through the use of information and communications technology. WHO has also indicated that e-health is a service that may involve clinical communications between healthcare providers and patients such as providing online referrals, prescribing treatments electronically and sharing electronic health records.. 立. 政 治 大. ‧. ‧ 國. 學. Although previous studies have discussed ICT usage in e-health, the use of ICT is not the only feature of e-health. The corresponding service features should also be taken into consideration. One study reported that a successful organization exists when it can provide better quality service and offer more services.(Mohammad Nabil Almunawar and Anshari 2012) Moreover, from the service organization’s perspective, a service must be designed with an appropriate mix of physical and non-physical components.(Mohammad Nabil Almunawar and Anshari 2012). It is important to know the critical features of a service in order to design appropriate e-health services. Accordingly, we aim to discover the service features in e-health that are valued by customers. This research will help service designers to improve e-health service design.. n. er. io. sit. y. Nat. al. Ch. engchi. i Un. v. Previous studies have deliberated how organizations design an e-health service. Previous research has suggested that to improve the design of an e-health system in order to satisfy stakeholders, an e-health service should be customer focused. (Marvin E. González et al., 2006). One study suggested that, to survive in today’s competitive market, health care organizations must incorporate the customer’s perspective. Even though customers might not precisely know their needs, they have a preconceived notion of what a service is, even if they may not have experienced it previously (Johnston and Clark, 2001) Thus, this research aims to discover what service features would affect customers’ intention to adopt and use an e-health service. Many previous studies investigated patterns of health-related Internet use. .
(6) However, few studies have discussed e-health services from the customers’ point of view. Previous studies attempted to determine customers’ expectations of e-health care, but they still did not have a detailed evaluation of customers’ needs. In terms of the current e-health environment in Taiwan, many government-supported projects are trying to promote the development of e-health services. Most e-health services face difficulty in attracting customers to adopt the service, and because of the lack of customers, those institutions terminate their services after the state aid ends. Therefore, the aim of this research is to determine the e-health service features that customers demand the most often. We will determine the key features that cause customers to adopt and continue using an e-health service, thereby keeping the service operational. This research will divide customers into two groups: existing customers and potential customers. First, for potential customers, we aim to determine (1) what are. 治 政 大customer adopt the e-health the major service features that would make a potential 立 care service? Furthermore, for existing customers, we aim to determine (2) what kind. ‧ 國. 學. of service features make a customer continue using it?. ‧. After answering these two questions, this research also aims to (3) distinguish service features that are relevant in different usage stages (intention to adopt, adoption and usage).. n. er. io. sit. y. Nat. al. Ch. engchi. 2 . i Un. v.
(7) CHAPTER 2: LITERATURE REVIEW To provide a better understanding of the impact of e-health care service features, this section reviews the literature related to e-health service design issues. We then use the service concepts to discuss key features of e-health services. 2.1 E-health care service design issues What is a service? It has been stated that all economic activities that are intangible and that imply an interaction to be realized between a service provider and consumer could be called service (Looy et al., 2003). With the increasing importance of service design in an organization, the management of new service development (NSD) has become a key competitive concern for many companies (Menor, Tatikonda and Sampson, 2002; Johnson, Menor, Roth and Chase, 2000; Fitzsimmons and Fitzsimmons, 2000; Johne and Storey, 1998; Gallouj and Weinstein, 1997). However, it could be argued that NSD is the overall process of developing new service offerings. 政 治 大 (Johnson et al., 2000). As products and services are becoming more and more similar 立 and it becomes easier for organizations to copy others’ products and services,. ‧. ‧ 國. 學. organizations may choose to compete through something that transcends their service offerings. After conducting research on NSD, we have found that a feature that covers service design and service innovation is the service concept (Goldstein et al., 2002). The service concept is more emotional than a business model, deeper than a. Nat. y. sit. n. al. er. io. brand, more complex than a good idea and more solid than a vision. The service concept helps us begin to understand how customers and service providers view services—as a sum of components (e.g., processes, facilities, tasks). Heskett (1986) has defined the service concept as the way in which the “organization would like to have its services perceived by its customers, employees, shareholders and lenders.”. Ch. engchi. i Un. v. Based on this idea of the service concept, this research will divide e-health service features into the following 5 parts: by whom, what, for whom, when and how (Goldstein et al., 2002). Details about the five dimensions of the service concept are discussed below. 2.1 By Whom (service delivery) The phrase “by whom” has many descriptions in the service concept. According to one of these descriptions, this dimension of the service concept aims to convey whether the service is delivered by personnel or by machines (Vincent Giard, 2003). Alternatively, “by whom” has been conceived to convey whether the service is delivered by specific service employees and/or systems of the service provider (Christian Gronröos, 1984). 3 .
(8) In this research, “by whom” refers to the channels and devices by which customers decide to adopt an e-health service. The decision may result from the impact of social relations, self-evaluation, and suggestions from professionals. We discuss these channels in more detail in the following sections. Social relations. Social factors have been noted to guide a variety of health promotion and intervention programs (Bandura, 2004), and they play major roles in a conceptual framework that has been proposed to study adolescent healthcare-related issues (Manganello, 2008). Social influence reflects the influence of subjective norms as presented in the theory of reasoned action (Fishbein & Ajzen, 1975) and the theory of planned behavior (Ajzen, 1991). This concept emphasizes the role of social influence in people’s decisions to undertake certain behaviors. Because social relations play an important role in healthcare-related issues, we can expect that social influence might also be essential to the entire e-health process.. 立. 政 治 大. ‧. ‧ 國. 學. Self-evaluation. Past literature has stated that more and more individuals are obtaining health-related information from the Internet. Furthermore, a report has found that the information that individuals gather directly affects their decisions about treatment for their illnesses (Rainie et al., 2000). A telephone-based survey conducted in the US also found that health information on the Internet affects people’s health care decisions. Furthermore, one study found that people use the Internet to access health information, such as general health tips, disease-specific information, health commodities, or hospital information (Manganello, 2008).. n. er. io. sit. y. Nat. al. Ch. i Un. v. Suggestions from Professionals. In e-health, the relationship between patient and professional medical staff has to be taken into consideration. Because patients usually expect the doctor to provide advice and treatment, building trust is important to the patient-doctor relationship (Hart et al., 2006).. engchi. 2.2 What (service offerings) Past studies have defined “what” in the service concept as the service offerings that should be included in the service (Peter T. Hill, 1977; Gadrey Jean, 2000). According to the Strategies Department ITU Telecommunication Development Sector, the term e-health refers to all digital health-related information, covering products such as instruments to ensure the constant monitoring of blood pressure in ambulatory patients. Such systems also play an important role in e-health, as in computer-assisted surgery systems, and the most important component of e-health is services. Recent studies have shown that continuous patient monitoring is an important 4 .
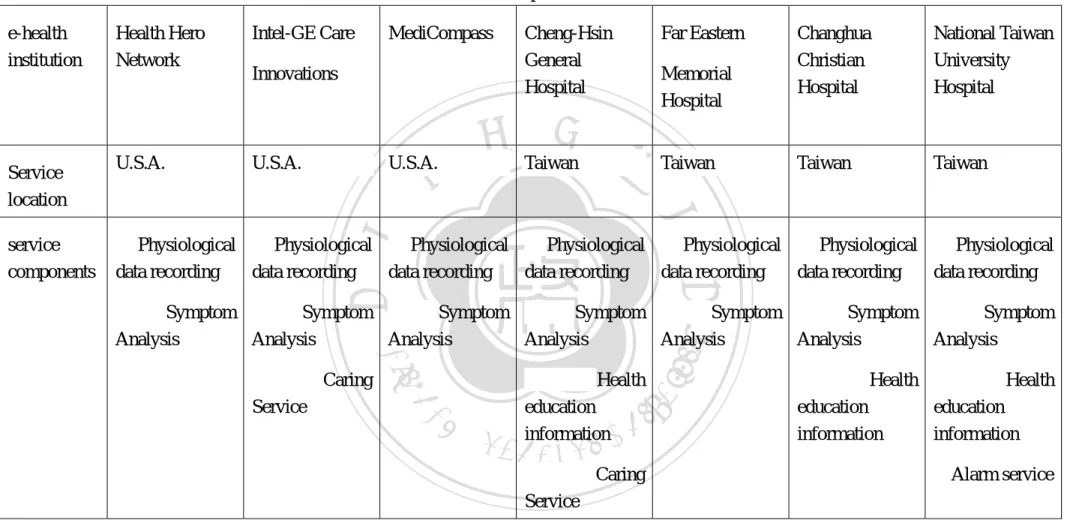
(9) e-health service offering. Home monitoring of elderly patients, as well as patients with chronic diseases, increases the individual’s comfort, enhances the patient’s quality of life, and encourages patient empowerment while reducing the number of needless transfers a hospitals and the cost of the health care services provided. Previous reports have also noted the importance of incorporating medical education into health care services. However, incorporating medical education into health care services raises concerns regarding delivering individual patient’s health-related information on the web (Eysenbach and Jadad 2001). In reviewing the current service offerings provided in the major e-health centers in Taiwan, we found that the following six services are offered (Table 1). 1. Physiological data recording 2. Symptom analysis. 政 治 大. 3. Health education information 4. Medical information. 立. ‧ 國. 學. 5. Alarm service. 6. Home caring service. ‧. n. er. io. sit. y. Nat. al. Ch. engchi. 5 . i Un. v.
(10) Table 2-1. E-health care service components in Taiwan & other countries. Service location. U.S.A.. Intel-GE Care. MediCompass. Innovations. 立. U.S.A.. U.S.A.. Far Eastern. Cheng-Hsin General Hospital. Memorial Hospital. 政 治 大 Taiwan. Taiwan. Changhua Christian Hospital. National Taiwan University Hospital. Taiwan. Taiwan. 學. ✓ Physiological ✓ Physiological ✓ Physiological ✓ Physiological ✓ Physiological ✓ Physiological ✓ Physiological data recording data recording data recording data recording data recording data recording data recording. ‧. service components. Health Hero Network. ‧ 國. e-health institution. n. al. Ch. engchi. i n U. ✓ Caring Service. 6 . sit. ✓ Health education information. er. io. ✓ Caring Service. y. Nat. ✓ Symptom ✓ Symptom ✓ Symptom ✓ Symptom ✓ Symptom ✓ Symptom ✓ Symptom Analysis Analysis Analysis Analysis Analysis Analysis Analysis. v. ✓ Health ✓ Health education education information information ✓Alarm service.
(11) 2.3 For Whom (customer segment) “For whom” refers to the people who become customers of a health care service (Dumoulin & Flipo, 1991). Previous research has shown that geographic and other external effects affect the development and adoption of Internet-related technologies in various customer sectors. It also suggested that e-health service design should emphasize the differences in sex, age, location, and size of the medical practice (Egea et al., 2010). One study suggested that specific external indicators (e.g., age) affect the use of specific e-health services (Burt and Sisk, 2005). Undoubtedly, a given customer service strategy should include decisions regarding the need to separate customers on the basis of their service requirements. (Theodoras, 2009). In other words, a customer service strategy determines the most important service elements and what levels of service are to be offered to each customer segment (Huiskonen & Pirttila, 1998).. 2.4 When (user demands). 立. 政 治 大. ‧ 國. 學. The “when” dimension of the service concept refers to when a service is needed by the users. Storing or maintaining an inventory of a service is impossible for suppliers. ‧. (Parasuraman et al., 1988), so understanding the connection between supply and user. y. Nat. demand is an important issue (Lovelock, 1983). Past literature has examined the. sit. e-health supply regarding the frequency of services such as home visits and telecare. er. io. services (Juretic & Meghan, 2012). It has been suggested that practitioners and. al. n. iv n C frequency of offering healthcare services Bunting, 2011). h e n(Christiea g c h i& U. researchers should consider the further development and application of the effective. 2.5 How (satisfaction) The “how” dimension of the service concept has been defined many times. This dimension has been stated to refer to the solutions that are provided to the customers’ problems (Christian, 1984). Moreover, Dumoulin & Flipo claimed that this dimension focuses on certain processes, procedures or codified behaviors and how they are achieved. It represents how customers’ needs are fulfilled during the service delivery process. According to Parasuraman (1988), service quality has become the most powerful means for a service organization to establish a competitive advantage and achieve success. The outcome is directly linked to how the customer feels about the service. 7 .
(12) Thus, in this study, we will focus on users’ feedback regarding satisfaction. User’s satisfaction with e-health can be measured in two dimensions: the service itself and the platform. Satisfaction with the e-health platform is important, because e-health is developed upon an ICT-based platform. ICT includes health information networks, telemedicine services, personal wearable and portable communication systems, electronic health records, and health portals (Silber D, 2003). The quality of the platform is directly related to the quality of e-health, thus affecting customer’s satisfaction with the service.. 立. 政 治 大. ‧. ‧ 國. 學. n. er. io. sit. y. Nat. al. Ch. engchi. 8 . i Un. v.
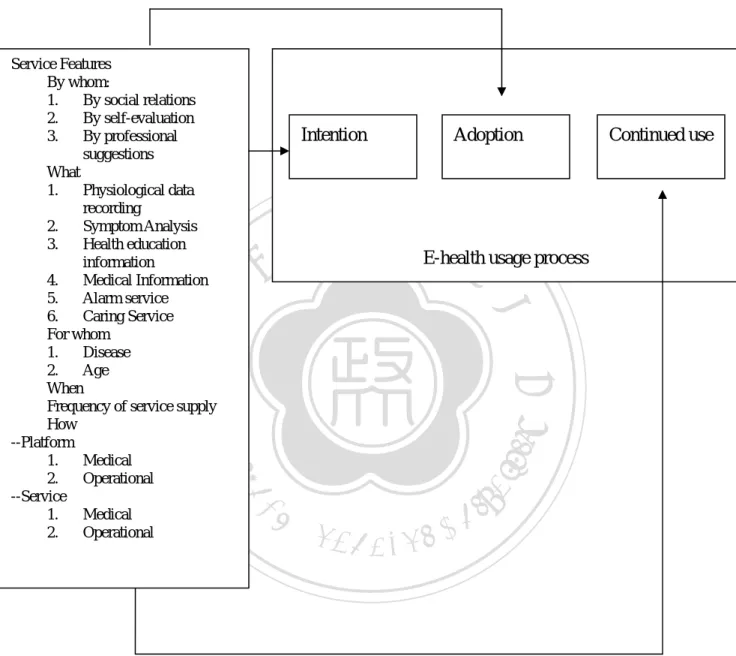
(13) CHAPTER 3-RESEARCH MODEL AND HYPOTHESIS 3.1 Research Model Based on our literature review, we propose the following research framework. . Intention. 立. Adoption . 政 治 大 E-health usage process. ‧ 國. ‧. n. al. er. io. sit. y. Nat. . Continued use. 學. Service Features whom: z By 1. By social relations 2. By self-evaluation 3. By professional suggestions z What 1. Physiological data recording 2. Symptom Analysis 3. Health education information 4. Medical Information 5. Alarm service 6. Caring Service z For whom 1. Disease 2. Age z When Frequency of service supply z How --Platform 1. Medical 2. Operational --Service 1. Medical 2. Operational. Ch. engchi. i Un. v. . Figure 3-1 Research framework Based on expectation-confirmation theory (ECT) (Anderson and Sullivan, 1993; Dabholkar et al., 2000; Oliver 1980, 1993; Patterson et al. 1997; Tse and Wilton 1988), we divided the e-health usage process into the following three stages: intention to adopt, adoption, and continued use. Patients’ intention to use the e-health service is highly 9 .
(14) related to their perception of the value of e-health and their expectations of this service. The intention leads to the initial decision to adopt this service. The initial experience then influences the decision to repurchase the service and continue using it. In this research, we are interested in discovering the important service features that affect the intention to adopt, adoption, and continued use of e-health. Based on a review of the literature, we use the service concept to categorize our interest in the following 5 dimensions of e-health service features: by whom, what, for whom, when, and how. 3.2.1 Service features - By whom The “by whom” dimension refers to the channels and devices by which customers choose a given service. The channels can be doctors or friends. According to the Technology Acceptance Model (TAM), social influence and subjective norms can explain an individual’s intentional or voluntary adoption of a technology (Hsu and Lu, 2004, Karahanna and Straub, 1999, Liao et al., 1999, Liker and Sindi, 1997, Taylor and Todd, 1995 and Venkatesh and Davis, 2000). Past studies have also showed that a consumer’s choice is the result of a complex interplay of cultural, social, personal, and psychological factors (Anilkumar and Joseph, 2012). Furthermore, Ajzen and Fishbein (1980) postulated that a consumer’s intent to purchase and his or her purchase patterns are influenced by personal and social factors.. 立. 政 治 大. ‧ 國. 學. ‧. Thus, we can assume that people would choose a service or product because of relatives or friends’ recommendations or experiences with that product.. n. al. er. io. sit. y. Nat. A previous study noted that self-evaluation is an important aspect of the consumer decision-making processes (Grewal, Cline & Davies, 2003). People make a purchase decision based on their own evaluation of a product’s price and functions. Moreover, professional suggestions from doctors or nurses might affect patient attitudes toward e-health. Previous have studies found that doctors’ suggestions usually determine patients’ decisions about their own medical care (Hart et al., 2006). Therefore, we assume that professional suggestions from doctors or medical professionals affect patients’ intention to adopt and continued use of an e-health service.. Ch. engchi. i Un. v. The following hypotheses are proposed: H1a: Social relations have an impact on a patient’s intention to adopt e-health. H1b: Self-evaluation has an impact on a patient’s intention to adopt e-health. H1c: Professional suggestions have positive impact on a patient’s intention to adopt e-health. H2a: Social relations have an impact on a patient’s continued use of e-health. H2b: Self-evaluation has an impact on a patient’s continued use of e-health channels or devices. 10 .
(15) H2c: Professional suggestions have an impact on a patient’s continued use of e-health channels or devices. 3.2.2 Service features – What The following key service features of e-health were determined from a study of the literature: physiological data recording, symptom analysis, health education information, medical information, alarm service, and caring service. These key service features are assumed to influence patients’ perceived usefulness of e-health.. TAM shows that when people perceive usefulness and ease of use of information technology, they will adopt that technology. Furthermore, according to the Post Acceptance Model of IS Continuance, when a user perceives the usefulness of a specific information technology, he/she will continue to use that technology. We propose the following hypotheses: H3a: Having a physiological data recording would have an impact on a patient’s intention to adopt E-health.. 政 治 大 H3b: Having symptom 立 analysis would have an impact on a patient’s intention to. adopt E-health.. ‧ 國. 學. H3c: Having health education information would have an impact on a patient’s intention to adopt E-health.. ‧. H3d: Having medical information would have an impact on a patient’s intention to adopt E-health.. y. Nat. sit. al. er. io. H3e: Having an alarm service would have an impact on a patient’s intention to adopt E-health.. v. n. H3f: Having a caring service would have an impact on a patient’s intention to adopt E-health.. Ch. engchi. i Un. H4a: Having physiological data recording would have an impact on a patient’s continued use of E-health. H4b: Having symptom analysis would have an impact on a patient’s continued use of E-health. H4c: Having health education information would have an impact on a patient’s continued use of E-health. H4d: Having medical information would have an impact on a patient’s continued use of E-health. H4e: Having an alarm service would have an impact on a patient’s continued use of E-health. H4f: Having a caring service would have an impact on a patient’s continued use of E-health. 11 .
(16) 3.2.3 Service features - For whom Previous research has shown that demographic and other external effects affect the development and adoption of Internet-related technologies in various sectors. It also suggested that e-health service design should take into account differences in sex, age, location, and size of the medical practice (Egea et al., 2010). In the case of e-health, age is often considered in the design of a service. Issues such as how to reduce IT complexity to encourage elderly people to adopt e-health services have often been discussed in the literature. In addition to age, disease type is an important factor that service designers should consider. For example, different types of disease may require different frequencies of service supply. We propose the following hypotheses: H5a: Age would have an impact on a patient’s intention to adopt E-health. H5b: Disease type would have an impact on a patient’s intention to adopt E-health.. 政 治 大 H6b: Disease type would have 立an impact on a patient’s continued use of E-health. H6a: Age would have an impact on a patient’s continued use of E-health.. ‧. ‧ 國. 學. 3.2.4 Service features – When This section attempts to determine when the service will be needed to fit user demands. Because storing or maintaining an inventory of a service is impracticable (Parasuraman et al., 1988), understanding the connection between supply and user demand is an important issue (Lovelock, 1983). In the context of e-health, service frequency is an important design issue. For example, Juretic and Meghan (2012) have discussed what response frequency would be suitable for a home telehealth service. We expect that patients might demand a high frequency of services because intensive service usually results in service satisfaction. Thus, we propose the following hypotheses:. n. er. io. sit. y. Nat. al. Ch. engchi. i Un. v. H7: The frequency of service supply would have an impact on a patient’s intention to adopt E-health. H8: The frequency of service supply would have an impact on a patient’s continued use of E-health. 3.2.5 Service features – How In e-health, service functions can be categorized into medical functions and operational functions. The whole service process can be divided into service and platform. Both functions and processes require an assessment of quality. According to Parasuraman (1988), service quality has become the most powerful means for a service organization to establish a competitive advantage and achieve success. Czepiel and Akerele (1974) also believed that customer satisfaction can be considered an 12 .
(17) integrated response to the evaluation of service quality. ECT also holds that consumers’ intention to repurchase a product or continue service use is determined primarily by their satisfaction with prior use of that product or service (Anderson and Sullivan 1993; Oliver 1980, 1993). We can expect that when patients feel satisfied about functions and processes of a service, they will adopt and continue to use that service. The following hypotheses are proposed: H9aa: Medical satisfaction with the platform would have an impact on a patient’s intention to adopt E-health. H9ab: Operational satisfaction with the platform would have an impact on a patient’s intention to adopt E-health. H9ba: Medical satisfaction with the service would have an impact on a patient’s intention to adopt E-health.. 政 治 大. H9bb: Operational satisfaction with the service would have an impact on a patient’s intention to adopt E-health.. 立. ‧ 國. 學. H10aa: Medical satisfaction with the platform would have an impact on a patient’s continued use of E-health. H10ab: Operational satisfaction with the platform would have an impact on a patient’s continued use of E-health.. ‧. y. Nat. H10ba: Medical satisfaction with the service would have an impact on a patient’s continued use of E-health.. sit. al. n. . er. io. H10bb: Operational satisfaction with the service would have an impact on a patient’s continued use of E-health. . Ch. engchi. 13 . i Un. v.
(18) CHAPTER 4-RESEARCH PLAN 4.1 Case Background The National Taiwan University Hospital (NTUH) was inaugurated in 1895. For this study, NTUH is establishing an e-health service for diabetes patients. The service has its own healthcare staff that monitors patients’ health and provides consultation for patients who have problems. Through this service, patients can upload their daily physical data record, and physicians can give medical suggestions and answer patients’ questions about their illness. To offer patients a good experience, NTUH has collaborated with us to establish an e-health service model that offers customers service propositions that fit their demands. 4.2 Measurements. 政 治 大. The constructs of the proposed research model are explained in the previous chapters. We conceptualized the measurement of the constructs, and the independent and dependent variables are shown in Table 4-1 and Table 4-2, respectively. Table 4-1 Independent variables. 學. ‧ 國. 立. Independent variables. n. al. sit. The extent to which the e-health service is introduced through friends and relatives The extent to which the e-health service is discovered through patient-related organizations. The extent to which the e-health device is recommend by friends and relatives.. er. SR1. Ch. SR2. SR3 Self-evaluation. Measurements of by whom. y. Items. ‧. io. Social relations. Nat. Components. engchi. v. SE1. The extent to which the e-health service is evaluated by searching through the Internet, newspapers or magazines. SE2. The extent to which the e-health device is chosen due to the price.. SE3. The extent to which the e-health device is chosen for its functionality. 14 . . i Un.
(19) The extent to which the e-health device is chosen because of its brand. The extent to join the e-health service is for better health. The extent to which the e-health service is discovered by doctors. The extent to which the e-health service introduced through by doctors. The extent to join the e-health service is by the trust of medical team.. SE4 SE5 Professional suggestions. PF1 PF2 PF3. Components. Items. Measurements of what. Physiological values recorded. PR1. The degree of usage regarding the recording of physiological values.. n. al. HI2C h HI3. Medical Information. MI1 MI2. MI3. MI4. y. sit. io. HI1. er. AF3. The degree of usage regarding various analysis forms. The extent to which the analysis form is expected by patients. Patients’ opinion with regular health reports. The degree of usage regarding health education information. The extent to which health education information is expected by patients. The extent to which health education information is prioritized by patients. The degree of usage regarding various medical information. The extent to which the provision of medical information on the system platform is expected by patients. The extent to which the provision of medical information is prioritized by patients. The extent to which the provision of medical information services is expected. ‧. AF2. Nat. Health education information. AF1. 學. Analysis form. ‧ 國. 立. 政 治 大. engchi. 15 . i Un. v.
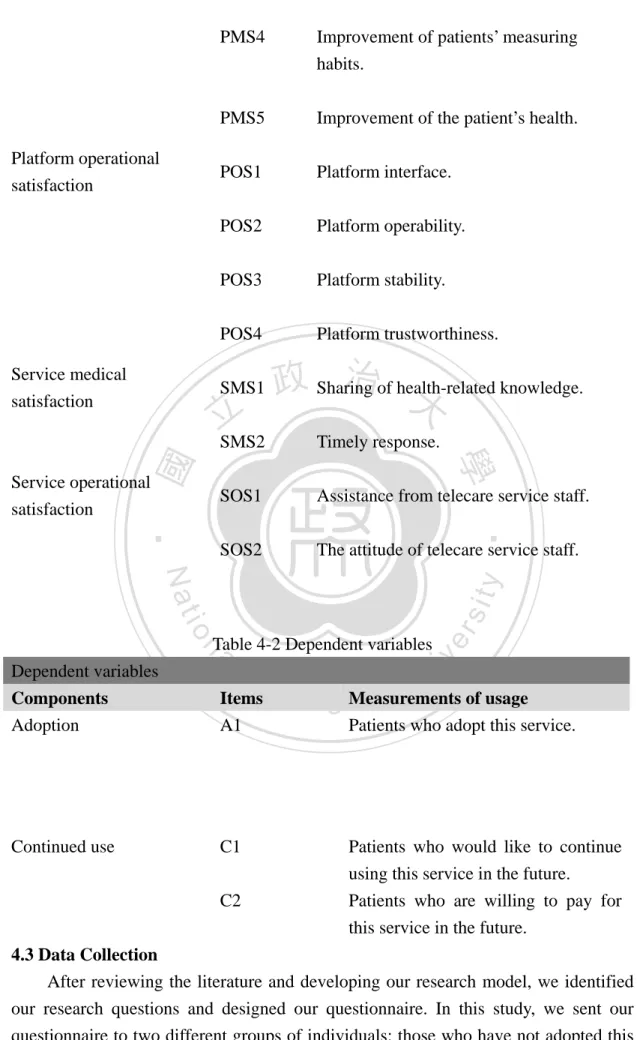
(20) AS1. AS2 AS3 CS1 CS2 CS3. io. Components. Measurements of for whom. A1. The age range of e-health service users.. D1. The disease type of e-health service users.. Items. Measurements of when. n. al. y. Nat. Disease. Items. ‧. Age. Frequency. prioritized by patients.. 學. Components. ‧ 國. CS4 立. 政 The治 extent to大 which the caring service is. F1. Ch. sit. Caring Service. er. Alarm service. by patients. The extent to which the alarm service is expected to be synchronously shared by patients’ relatives and friends. The extent of patients’ opinion to the alarm service. The extent to which the alarm service is prioritized by patients. The degree of usage regarding the caring service. The extent to which caring service is expected by patients. The patients’ view of the caring service.. iv n usage frequency of the e-health i U e nThe h c g service platform.. F2. The usage frequency of various e-health service offerings.. Components. Items. Measurements of how. Platform medical satisfaction. PMS1. Platform convenience.. PMS2. The control of physical conditions.. PMS3. Platform information.. 16 .
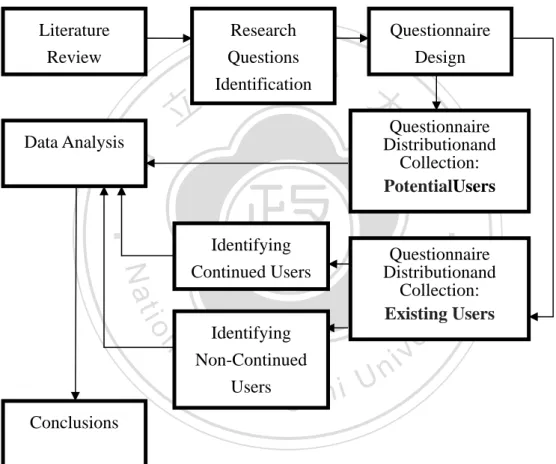
(21) Platform operational satisfaction. Service medical satisfaction. PMS4. Improvement of patients’ measuring habits.. PMS5. Improvement of the patient’s health.. POS1. Platform interface.. POS2. Platform operability.. POS3. Platform stability.. POS4. Platform trustworthiness.. SMS1. 立. 治of health-related knowledge. 政 Sharing 大 Timely response.. SOS1. Assistance from telecare service staff.. SOS2. The attitude of telecare service staff.. Service operational satisfaction. ‧. ‧ 國. 學. SMS2. al. Components Adoption. Items A1. Continued use. C1. n. Ch. er. io. sit. y. Nat Dependent variables. Table 4-2 Dependent variables. i Un. v. e n g cMeasurements of usage hi Patients who adopt this service.. Patients who would like to continue using this service in the future. Patients who are willing to pay for this service in the future.. C2. 4.3 Data Collection After reviewing the literature and developing our research model, we identified our research questions and designed our questionnaire. In this study, we sent our questionnaire to two different groups of individuals: those who have not adopted this 17 .
(22) service but have the potential to adopt it and those who are already users of the e-health service. We define individuals who have yet to adopt the service as potential e-health service users. Once they adopt the service, they become e-health adopters. In this study, both potential users and adopters are diabetes patients. For potential users, we are interested in investigating the factors that will impact their intention to adopt the e-health service. For adopters, we are interested in identifying factors that will impact their intention to continue using this service. We will also compare the two groups to identify the factors that will impact the adoption of the e-health service. The flow of the research process is shown in figure 4-1.. Literature Review. Research Questions Identification. 立. Questionnaire Design . 政 治 大. Questionnaire Distributionand Collection: PotentialUsers. Data Analysis. ‧. sit. Identifying. er. io. Questionnaire Distributionand Collection: Existing Users. y. ‧ 國. 學. Nat. Identifying Continued Users. n. a l Non-Continued iv n C hUsers engchi U. Conclusions Figure 4-1 Flow of the Research Process First, we collected the questionnaire from those who have already joined the NTUH e-health service. The NTUH e-health service began on 2011/09/05 with 92 users. We designed a questionnaire and uploaded it to the service’s online platform on April 2012, and users could choose whether to respond to the questionnaire. After 4 months, we collected responses from 50 users. The results of the survey showed that there are no significant differences between genders. In addition, 63% of platform users are type-1 diabetes patients. In Type 1 diabetes, the patient’s body has 18 .
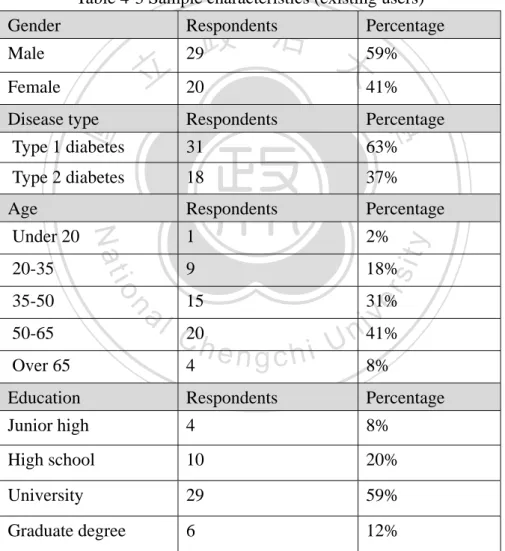
(23) destroyed the insulin-producing beta cells in the pancreas. It is known as an autoimmune disease and tends to appear early in life. Type 1 diabetes reportedly accounts for only approximately 5–10% of all diabetes cases (Daneman, 2006). However, patients who suffer from Type 2 diabetes often do so because they were overweight and unfit and had been for some time. Type 2 diabetes tends to appear later in life. Most respondents are aged between35 and 65 years, meaning they were primarily middle-aged. Moreover, most users have completed education beyond the high school level. The sample characteristics for the existing users of the e-health platform are presented in Table 4-3. Table 4-3 Sample characteristics (existing users) Gender. Percentage 治 政 29 大 59%. Respondents. Male. Disease type. Respondents. Percentage. Type 1 diabetes. 31. 63%. Type 2 diabetes. 18. 37%. Age. Respondents. Percentage. 1. 2%. 9. 18%. 15. io. al. n. 35-50 50-65 Over 65. C20h 4. y. sit. 20-35. Nat. Under 20. ‧. ‧ 國. 41%. 學. 20. er. 立. Female. 31%. engchi. iv 41% n U 8%. Education. Respondents. Percentage. Junior high. 4. 8%. High school. 10. 20%. University. 29. 59%. Graduate degree. 6. 12%. After we collected the data from existing users, we collected data from those who were not members of the service. We obtained NTUH’s approval (see Appendix B) to collect our data in their clinic. We administered our questionnaire at the Department of Internal Medicine in National Taiwan University Hospital (NTUH). 19 .
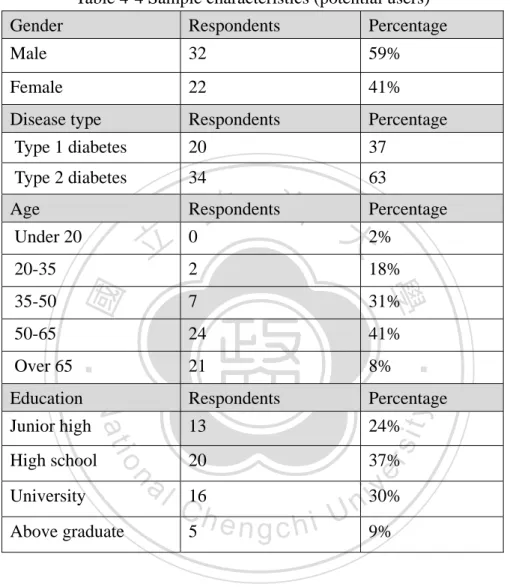
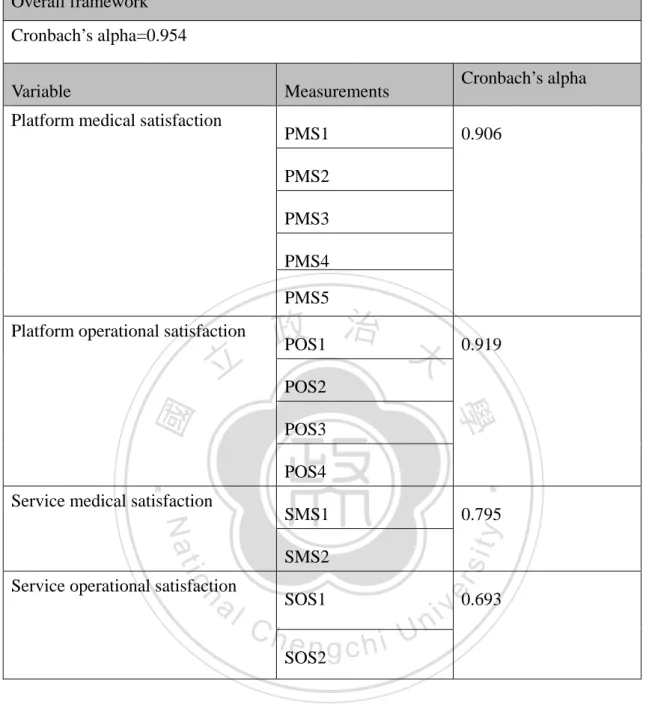
(24) Over 1 month, we collected responses from 54 individuals at the clinics. Most respondents were over 50 years of age. The sample characteristics for potential users are presented in Table 4-4. In total, we collected 104 questionnaires (including potential users and existing users) for analysis. Table 4-4 Sample characteristics (potential users) Gender. Respondents. Percentage. Male. 32. 59%. Female. 22. 41%. Disease type. Respondents. Percentage. Type 1 diabetes. 20. 37. Type 2 diabetes. 34. 63. Age. Respondents. 立. Under 20. 18%. 7. 31%. 24. 41%. Over 65. 21. 8%. Education. Respondents. Percentage. 13. 24%. 20. 37%. io. High school. al. n University Above graduate. C16h 5. y. ‧. Nat. Junior high. sit. 50-65. er. 35-50. 學. 2. ‧ 國. 20-35. 政 治 大Percentage 0 2%. engchi. iv 30% n U 9%. 4.4 Reliability Table 4-5 indicates the reliability of the constructs in our framework.Construct reliability was assessed using Cronbach’s alpha. The test indicated that all of the constructs have reasonably satisfactory alpha values. The alpha coefficient for the four items is 0.954, suggesting that they have a relatively high level of internal consistency (note that a reliability coefficient of 0.7or higher is considered “acceptable” in most social science research).. 20 .
(25) Table 4-5 Reliability Analysis Overall framework Cronbach’s alpha=0.954 Variable. Cronbach’s alpha. Measurements. Platform medical satisfaction. PMS1. 0.906. PMS2 PMS3 PMS4 PMS5. Platform operational satisfaction. POS2 POS3. sit. n. al. SMS2 SOS1. v 0.693 i n. Ch. U i e h n c g SOS2. 21 . er. io. Service operational satisfaction. . 0.795. y. Nat. SMS1. ‧. POS4. Service medical satisfaction. 0.919. 學. ‧ 國. 立. 治 政 POS1 大.
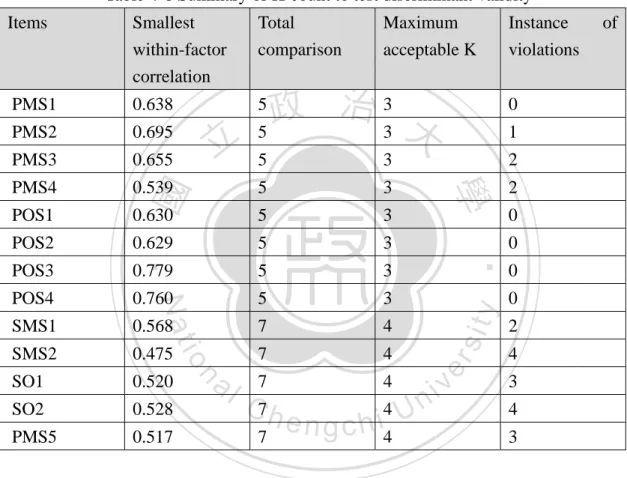
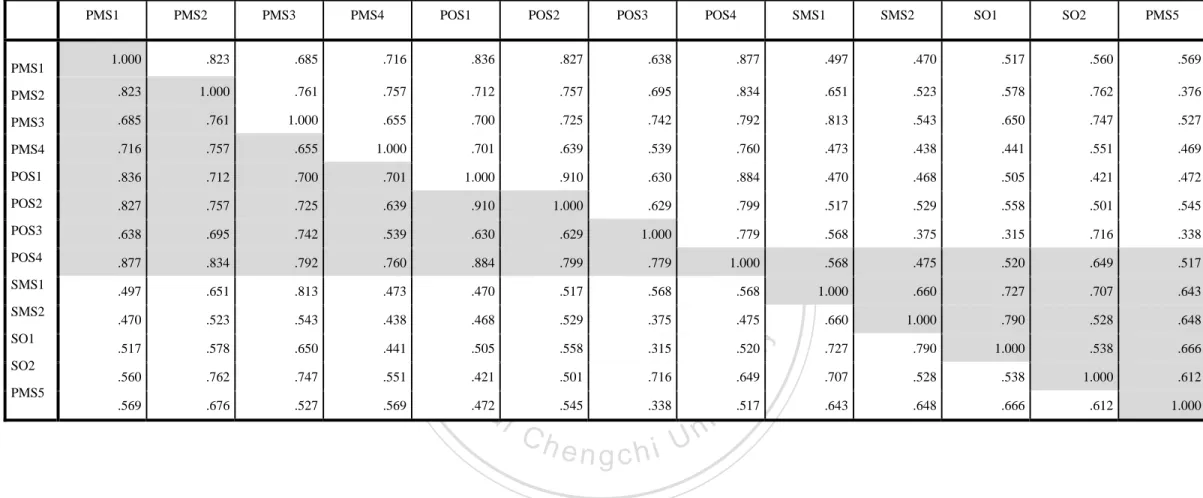
(26) 4-5 Discriminant validity To claim discriminant validity, the correlations between the different factors should be low. For each item, we first identify its lowest within-factor correlation. Then, we compare this value to its correlation with items from all other factors and count number of instances (K) that the former value is lower. The value of K should be less than one-half those of the potential comparisons. Table 4-6 summarizes the values of K from all comparisons listed in Table 4-7. We find all the items take values less than the maximum acceptable K,which indicates that our measures exhibit discriminant validity. Table 4-6 Summary of K-count to test discriminant validity Items. Smallest within-factor correlation. PMS1. 0.638. PMS2. 0.695. PMS3. 0.655. PMS4. Total comparison. Instance violations. 治3 政 5 3 大. 0. 5. 3. 2. 0.539. 5. 3. 2. POS1. 0.630. 5. 3. POS2. 0.629. 5. 3. POS3. 0.779. 5. 3. POS4. 0.760. 5. 3. SMS1. 0.568. 7. 4. SMS2. 0.475. 7. 4. SO1. 0.520. SO2. 0.528. PMS5. 0.517. 5. n. er. io. sit. y. ‧. Nat. al. i C7h 4 Un engchi 7. 4. 7. 4. 22 . 1. 學. ‧ 國. 立. . . Maximum acceptable K. v. 0 0 0 0 2 4 3 4 3. of.
(27) Table 4-7 Correlation Matrix. PMS1. PMS2. PMS3. PMS4. POS1. POS2. POS3. SMS1. SMS2. SO1. SO2. PMS5. 1.000. .823. .685. .716. .836. .827. .638. .877. .497. .470. .517. .560. .569. PMS2. .823. 1.000. .761. .757. .712. .757. .695. .834. .651. .523. .578. .762. .376. PMS3. .685. .761. 1.000. .655. .700. PMS4. .716. .757. .655. 1.000. .701. POS1. .836. .712. .700. .701. POS2. .827. .757. .725. .639. POS3. .638. .695. .742. .539. POS4. .877. .834. .792. .760. SMS1. .497. .651. .813. .473. .470. .523. .543. .438. .517. .578. .650. .441. .560. .762. .747. .551. .569. .676. .527. .569. .543. .650. .747. .527. .639. .539. .760. .473. .438. .441. .551. .469. 1.000. .910. .630. .884. .470. .468. .505. .421. .472. .910. 1.000. .629. .799. .517. .529. .558. .501. .545. .630. .629. 1.000. .779. .568. .375. .315. .716. .338. .884. .799. .779. 1.000. .568. .475. .520. .649. .517. .470. .517. .568. .568. 1.000. .660. .727. .707. .643. .468. .529. .375. .475. .660. 1.000. .790. .528. .648. .505. .558. .315. .520. .727. .790. 1.000. .538. .666. .421. .501. .716. .649. .707. .528. .538. 1.000. .612. .545. .338. .643. .648. .666. .612. 1.000. al. n. .472. Ch. engchi U. 23 . y. sit er. io. PMS5. .813. ‧. SO2. .792. Nat. SO1. .742. 學. SMS2. 政 治 大 .725. 立. ‧ 國. PMS1. . POS4. v ni. .517.
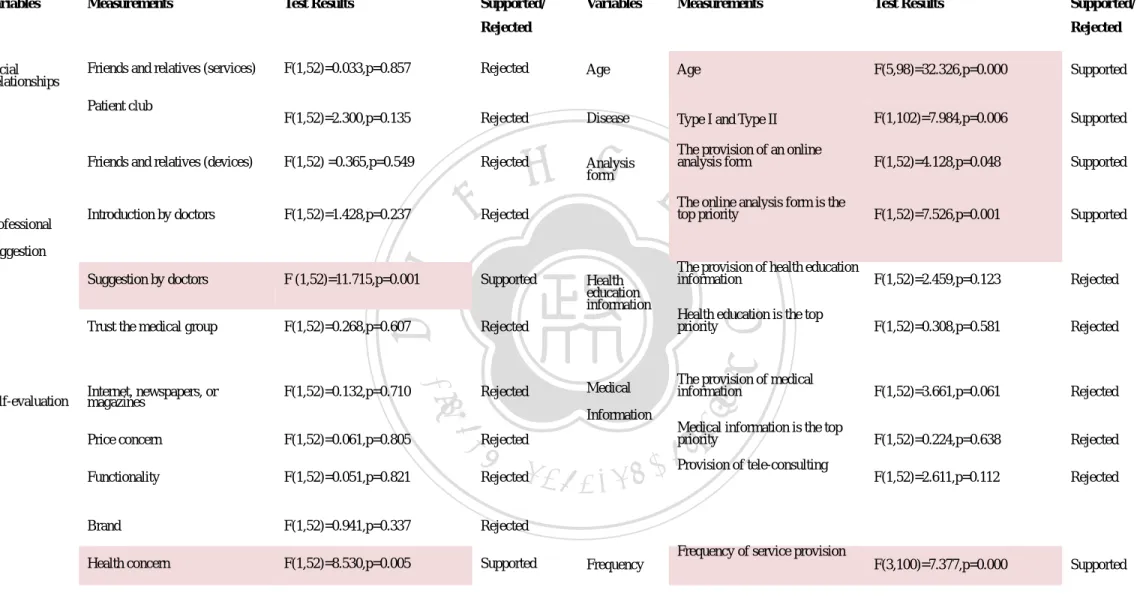
(28) CHAPTER 5: RESULTS AND DISCUSSION In this chapter, we describe the results of our statistical analysis and discuss the statistically insignificant variables and the managerial implications of our framework. 5.1 Results In this study, we elected to employ an ANOVA (analysis of variance) to test our hypotheses. We analyzed the differences between the group means for those who intend to adopt the service, have adopted the service, and choose to continue using the service. We tested each service feature separately against the dependent variables to identify the significant ones. (The complete results will be presented in appendices C,D, and E). The results are presented below followed by a discussion of our findings.. 政 治 大. 5.1 .1 Factors that affect the intention to use the E-health service First, we discuss the factors that affect the intention to use the e-health service. We compare the group of individuals who reported their intention to use the service to those who did not. We use the willingness to use the service as our dependent variable. We model the willingness to use the service using 5 levels: from high willingness to low willingness. We define respondents who selected levels 1 to 3 as individuals who do not intend to use the service and those who selected levels above 3 as having such an intention. The results reveal that among 54 respondents, 17 intend to use the service and 37 people do not (See table 5-1). Table 5-1 Willingness to use the service. 立. ‧. ‧ 國. 學. n. er. io. sit. y. Nat. al. Ch. Are willing to use the service Are not willing. Respondents. engchi. to use the service. The test results are summarized in Table 5-2.. 24 . i Un. v. Percentage. 17. 31%. 37. 69%.
(29) Table 5-2 Results regarding patients’ intention to use the e-health service Dependent Variable: Willing to use the service Variables. Measurements. Test Results. Supported/. Variables. Measurements. Test Results. Rejected Social Relationships. Friends and relatives (services). Supported/ Rejected. F(1,52)=0.033,p=0.857. Rejected. Age. Age. F(5,98)=32.326,p=0.000. Supported. F(1,52)=2.300,p=0.135. Rejected. Disease. Type I and Type II. F(1,102)=7.984,p=0.006. Supported. Friends and relatives (devices). F(1,52) =0.365,p=0.549. Rejected. The provision of an online analysis form. F(1,52)=4.128,p=0.048. Supported. Introduction by doctors. F(1,52)=1.428,p=0.237. The online analysis form is the top priority. F(1,52)=7.526,p=0.001. Supported. Suggestion by doctors. F (1,52)=11.715,p=0.001. Supported. F(1,52)=2.459,p=0.123. Rejected. Trust the medical group. F(1,52)=0.268,p=0.607. Rejected. F(1,52)=0.308,p=0.581. Rejected. Internet, newspapers, or magazines. F(1,52)=0.132,p=0.710. F(1,52)=3.661,p=0.061. Rejected. F(1,52)=0.224,p=0.638. Rejected. F(1,52)=2.611,p=0.112. Rejected. F(3,100)=7.377,p=0.000. Supported. Patient club. The provision of health education information Health education is the top priority. y. Health education information. ‧. Nat. Information. The provision of medical information. sit. Medical. Rejected. er. io. Self-evaluation. 學. Suggestion. Rejected. ‧ 國. Professional. 立. 政 治 大 Analysis form. n. Medical information is the top priority a Rejected iv l C n Provision of tele-consulting Rejectedh e ngchi U. Price concern. F(1,52)=0.061,p=0.805. Functionality. F(1,52)=0.051,p=0.821. Brand. F(1,52)=0.941,p=0.337. Rejected. Health concern. F(1,52)=8.530,p=0.005. Supported. Frequency of service provision Frequency. . 25 .
(30) . Table 5-2 Results regarding patients’ intention to use the e-health service Dependent Variable: Willing to use the service Variables. Measurements. Test Results. Supported/. Variables. Measurements. Test Results. Reject Alarm service. The provision of alarm service. F(3,50)=3.169,p=0.032. Supported. Supported/ Rejected. Platform. 政 治 大. Operability.. F(3,50)=3.208,p=0. 031. Supported. Stability.. F(3,50)=2.334,p=0. 085. Rejected. Trustworthiness.. F(4,49)=1.303,p=0. 282. Rejected. Sharing of health-related knowledge.. F(3,50)=7.569,p=0. 000. Supported. Timely response.. F(4,49)=22.641,p= 0.000. Supported. Assistance from telecare service staff.. F(4,49)=11.353,p= 0.000. Supported. The attitude of telecare service staff.. F(3,50)=2.319,p=0. 087. Rejected. operational. 立. F(1,52)=1.890,p=0.175. Convenience.. Rejected. F(3,50)=1.022,p=0.391. Rejected. satisfaction. The control of physical conditions.. F(3,50)=1.305,p=0.283. Rejected. Medical information.. F(3,50)=6.981,p=0.001. Improvement of patients’ measuring habits.. F(4,49)=1.754,p=0.153. Improvement of the patient’s health.. F(3,50)=3.423,p=0.024. Supported. Platform interface.. F(3,50)=3.727,p=0.017. Supported. y. Nat. Supported. n. al. Ch. Rejected. engchi. operational satisfaction. 26 . Service operational satisfaction. er. io. Platform. Service medical. ‧. satisfaction. satisfaction. 學. Platform medical. Provision of caring service. Rejected. ‧ 國. Caring Service. F(1,52)=3.524,p=0.666. sit. Alarm service is the top priority. i n U. v.
(31) Table 5-3 summarizes the hypotheses that are supported and rejected. Table 5-3 results regarding the intention to use the e-health service By whom. What. H1a (Social Relationships) --- rejected. H4a (Physiological values recorded). For whom. When. How. H7a (Age). H10 (Frequency) ---supported. H13aa (Platform medical satisfaction). --- rejected. ---supported. --- rejected. H1b (Self-evaluation) ---supported. H4b (Analysis form) ---supported. H13ab (Platform operational satisfaction) ---supported. H7b (Disease) ---supported. H1c (Professional suggestion) ------supported. H13ba (Service medical satisfaction) ---supported. H4c (Health education information) --- rejected. 立. 政 治 大. ‧ 國. 學. H4d (Medical Information) --- rejected. ‧. H4e (Alarm service) ------supported H4f (Caring Service) --- rejected. er. io. sit. y. Nat. al. H13bb (Service operational satisfaction) --- rejected. n. 5.1 .2 Factors that affect the decision to use thee-health service Non-adopters are those who have yet to being using the service but may do so in the future, and adopters are those who currently use the service. Our aim is to determine whether any factor that differs significantly between these two groups. Table 5-4 reports that 48% of the respondents are adopters and 53% are non-adopters. Table 5-4 willingness to continue using the service. Ch. engchi. i Un. Respondents. Percentage. Adopter. 50. 48%. Non-adopter. 54. 53%. The test results are summarized in Table 5-5.. 27 . v.
(32) Table 5-5 Results for patients who use the e-health service Dependent variable: Adoption of e-health service Variables. Measurements. Test Results. Supported/. Variables. Measurements. Test Results. Rejected Social Relationships. Friends and relatives (services). Supported/ Rejected. F(1,102)=0.547,p=0.461. Rejected. Age. Age. F(5,98)=32.326,p=0.000. Supported. F(1,102)=0.265,p=0.608. Rejected. Disease. Type I and Type II. F(1,102)=7.984,p=0.006. Supported. Friends and relatives (devices). F(1,102)=8.090,p=0.005. Supported. The provision of an online analysis form. F(1,102)=0.679,p=0.412. Rejected. Introduction by doctors. F(1,102)=51.535,p=0.000. Supported. The online analysis form is the top priority. F(1,102)=10.393,p=0.000. Supported. Suggestion by doctors. F(1,102)=6.974,p=0.010. Supported. The provision of health education information. F(1,102)=3.277,p=0.073. Rejected. Trust the medical group. F(1,102)=0.191,p=0.663. Rejected. Health education is the top priority. F(1,102)=14.736,p=0.000. Supported. Internet, newspapers, or magazines. F(1,102)=20.029,p=0.000. F(1,102)=26.078,p=0.000. Supported. F(1,102)=10.684,p=0.001. Supported. F(1,102)=26.261,p=0.000. Supported. F(3,100)=7.377,p=0.000. Supported. Patient club. y. ‧. Medical. io. Information. The provision of medical information. sit. Supported. er. Nat. Self-evaluation. Health education information. 學. Suggestion. ‧ 國. Professional. 立. 政 治 大 Analysis form. Medical information is the top priority. al. i vof tele-consulting n Provision C Supported h e ngchi U. F(1,102)=0.219,p=0.640. Functionality. F(1,102)=6.769,p=0.011. Brand. F(1,102)=5.967,p=0.016. Supported. Health concern. F(1,102)=0.957,p=0.331. Rejected. n. Price concern. Rejected. Frequency of service provision Frequency. . 28 .
(33) . Table 5-5 Results for patients who use the e-health service (continued) Dependent variable: Adoption of e-health service Variables. Measurements. Test Results. Supported/. Variables. Measurements. Test Results. Rejected Alarm service. The provision of alarm service. F(3,100)=4.532,p=0.005. Supported. Rejected Platform. Operability. F(3,100)=3.997,p= 0.010. Supported. Stability. F(4,99)=2.301,p=0. 064. Rejected. Trustworthiness. F(4,99)=0.987,p=0. 418. Rejected. Sharing of health-related knowledge. F(3,100)=5.360,p= 0.002. Supported. Timely response. F(4,99)=3.114,p=0. 019. Supported. Assistance from telecare service staff. F(4,99)=3.361,p=0. 013. Supported. operational. F(1,102)=2.136,p=0.147. Rejected. F(1,102)=0.939,p=0.425. Medical information. F(3,100)=4.210,p=0.008. Improvement of patients’ measuring habits.. F(4,99)=0.988,p=0.418. io. Rejected. Supported. al. Rejected. n. Improvement of the patient’s health. F(4,99)=3.710,p=0.007. Platform interface. F(3,100)=2.234,p=0.089. ‧. The control of physical conditions. Ch. eSupported ngchi Rejected. operational satisfaction. 29 . Service medical satisfaction. Nat. Platform. F(3,100)=0.555,p=0.646. y. satisfaction. Rejected. Service operational satisfaction. sit. Convenience.. satisfaction. 學. Platform medical. 立. Provision of caring service. 政 治 大 Supported. ‧ 國. Caring Service. F(1,102)=24.692,p=0.000. er. Alarm service is the top priority. Supported/. i n U. v.
(34) Table 5-6 summarizes the hypotheses that are supported and rejected. Table 5-6 results regarding the decision touse the e-health service By whom. What. H2a. H5a. (Social Relationships). (Physiological values recorded). ---supported. For whom H8a (Age). When. How. H11(Frequency). H14aa. ---supported. (Platform medical satisfaction). ---supported. --- rejected. H2b (Self-evaluation). H5b. ---supported. (Analysis form). ---supported H14ab. H8b (Disease). ---supported. (Platform operational satisfaction). ---supported. ---supported. H2c. H5c. H14ba. (Professional suggestion). (Health education information). (Service medical satisfaction). ------supported. ---supported. --- rejected. 政 治 大. 立 (Medical Information) H5d. (Service operational satisfaction). (Alarm service) ------supported. sit. y. Nat. H5f. io. n. al. er. (Caring Service) --- rejected. --- rejected. ‧. ‧ 國. 學. ---supported H5e. H14bb. i Un. 5.1. 3 Factors that affect the continued use of the e-health service. Ch. engchi. v. We then examine existing users to identify factors that affect their decision to continue using the service. The dependent variable is the willingness to continue using the service and is used to divide the sample into two groups: those who would be willing to continue the service if a fee were charged and those who would not. Table 5-8 shows that among 50 users, 62% are willing to continue and 38% are not. Table 5-9 presents the results. Table 5-8 willingness to pay for the service Respondents Willing to continue use if charged. 31. 62%. Not willing to continue use if charged. 19. 38%. 30 . Percentage.
(35) Table 5-9 Results for patients who would like to continue using the service Dependent variable: Willing to continue the service if a fee is charged. Variables. Measurements. Test Results. Supported/. Variables. Measurements. Test Results. Rejected Social Relationships. Friends and relatives (services). Rejected. F(1,48)=1.258,p=0.268. Rejected. Physical data recorded. Recording of physiological values. is top priority. F(1,48)=1.653,p=0.205. Rejected. Analysis form. Friends and relatives (devices). F(1,48)=0.403,p=0.528. Rejected. Introduction by doctors. F(1,48)=0.09,p=0.925. Suggestion by doctors. F(1,48)=0.061,p=0.807. Rejected. Trust the medical group. F(1,48)=0.565,p=0.456. Rejected. Internet, newspapers, or magazines. F(1,48)=0.063,p=0.803. Rejected. Price concern. F(1,48)=0.343,p=0.561. Functionality. F(1,48)=1.632,p=0.208. Brand. F(1,48)=0.682,p=0.413. Health concern. F(1,48)=0.43,p=0.836. Patient club. The provision of an online analysis form. F(1,48)=1.632,p=0.208. Rejected. The online analysis form is the top priority. F(1,48)=5.476,p=0.023. Supported. The provision of health education information. F(1,48)=0.504,p=0.481. Rejected. Health education is the top priority. F(1,48)=0.230,p=0.633. Rejected. F(1,48)=1.350,p=0.251. Rejected. F(1,48)=0.128,p=0.722. Rejected. F(1,48)=0.199,p=0.658. Rejected. Tele-consullting is the top priority. F(1,48)=0.533,p=0.469. Rejected. The provision of health education information. F(1,48)=0.608,p=0.439. Rejected. Rejected Health education information. Medical information is the top priority. Medical. Rejected. Information. er. io. sit. Nat. y. The provision of medical information. Rejected. n. al. Ch. Rejected. Rejected. engchi. 31 . Supported. ‧. Self-evaluation. 政 治 大. F(1,48)=4.323,p=0.032. 學. Suggestion. 立. ‧ 國. Professional. Supported/. i n U. v. Provision of tele-consulting.
(36) Table 5-9 The test results of patients who would like to continue the service (continued) Measurements Variables. Measurements. Supported/. Test Results. Variables. Test Results. Rejected Alarm service. Supported/ Rejected. The provision of alarm service. F(3,46)=1.052,p=0.379. Rejected. Platform medical satisfaction. Alarm service is the top priority. F(1,48)=1.632,0.208. Rejected. Platform. Improvement of patients’ measuring habits. F(4,45)=3.091,p=0.025. Supported. F(3,46)=2.525,p=0.069. Rejected. Operability. F(3,46)=4.179,p=0.011. Supported. Stability. F(4,45)=3.291,p=0.019. Supported. Trustworthiness. F(3,46)=2.256,p=0.094. Rejected. Sharing of health-related knowledge.. F(3,46)=3.404,p=0.025. Supported. Timely response.. F(3,46)=1.129,p=0.347. Rejected. Assistance from telecare service staff.. F(3,46)=3.404,p=0.025. Supported. The attitude of telecare service staff.. F(3,46)=1.646,p=0.179. Supported. Platform interface. operational satisfaction. Provision of caring service. 政 治 大. Rejected. F(1,48)=0.682,p=0.413. 立. Disease. The disease type of e-health service users.. F(1,48)=5.851,p=0.019. Supported. Frequency. Frequency of service provision. F(2,47)=0.394,p=0.676. Rejected. Rejected. Convenience. F(3,46)=2.269,p=0.093. Rejected. Improvement of patients’ measuring habits. F(3,46)=1.176,p=0.329. The control of physical conditions. F(3,46)=2.542,p=0.068. Rejected. Medical information. F(3,46)=3.404,p=0.025. Supported. io. Service operational. satisfaction a lRejected iv n Ch engchi U. n. satisfaction. y. F(2,47)=1.241,p=0.298. er. The usage frequency of various e-health service offerings.. medical. Service medical satisfaction. Nat. Platform. Supported. ‧ 國. F(4,45)=5.595,p=0.001. 32 . ‧. The age range of e-health service users.. 學. Age. sit. Caring Service.
(37) We summarize the results of our hypothesis tests in the following table (see table 5-10). Table 5-10 Results of hypothesis tests for continuing users By whom. What. For whom. When. How. H3a (Social Relationships) --- rejected. H6a (Physiological values recorded). H9a (Age). H12(Frequency) --- reject. H15aa (Platform medical satisfaction). ---supported ---supported. H3b (Self-evaluation) --- rejected. ---supported. H6b (Analysis form) ---supported. H15ab (Platform operational satisfaction) ---supported. H9b (Disease) ---supported. 政 治 大. H6c (Health education information) --- rejected. 立. H15ba (Service medical satisfaction) ---supported. 學 ‧. ‧ 國. H3c (Professional suggestion) --- rejected. H15bb (Service operational satisfaction) ---supported. al. n. H6e (Alarm service) --- rejected H6f (Caring Service) --- rejected. er. io. sit. y. Nat. H6d (Medical Information) --- rejected. Ch. engchi. i Un. v. 5.1.4 Summary of our analysis We summarize the impact of factors across different stages of use in Table 5-11. We discuss these results further in the following section.. 33 .
(38) Table5-11 The summary of impact factors across different stages of use. What. What. -- age. -- Analysis form. 政 治 大. 立. Frequency. For whom. -- Frequency. -- disease. ‧. io. n. al. Ch. engchi. 34 . Factors that affect theall three stages. For whom. Nat. -- Medical information. -- Physiological values recorded. By Whom -Self-evaluation -- Professional suggestion. Factors that affect intention and continued use. 學. -- Health education information. What. Factors that affect adoption and continued use. y. By Whom --social relations. Factors that affect both intention and adoption. sit. What -- Alarm service. Factors that only affect the continued use stage. er. Factors that only affect the adoption stage. ‧ 國. Factors that only affect the intention stage. i n U. v. How -- Platform medical satisfaction -- Platform operational satisfaction -- Service medical satisfaction -- Service operational satisfaction. Factors that have no impact across the three stages What --Caring Service.
(39) 5.2 Findings Finding 1: The provision of alarm services is crucial for creating patient intention The examination showed that the alarm service is a significant service feature distinguishing patients with no intention to use the service from those who do. Thus, service providers should emphasize the alarm service when marketing the service to the patients. We further analyzed how the patients would like the service be delivered. Table 5-12 shows that patients prefer instant contacts via phone to messages delivered via text or the online platform. Table 5-12 Patients’ opinions on the delivery of alarm services The number of patients preferring each means of delivering the alarm service Contact by phone call. ‧ 國. percentage. message. 3. 3. 0. 17.6%. 17.6%. 0.0%. 立. 64.7%. 學. respondents 11. Contact by Not needed 治 政 platform 大. Contact by cell phone txt. Total. 17 100.0%. ‧. n. al. er. io. sit. y. Nat. Finding 2: Social relationships, the medical information service, and the health education information service are important service features for e-health service users The investigation shows that social relationships affect the decision to use the service. We further found that this factor has a negative impact. Only 12% of adopters would follow friends’ and relatives’ recommendations to use the service, which is much lower than for non-adopters (Table 5-13). Thus, we can conclude that social relationships may improve patients’ intention to use the service but is not the key factor in the decision. Table 5-13. The impact of social relationships. Adopters respondents percentage Non-adopters. Ch. engchi. v. Use is due to the recommendations of friends and relatives. The recommendations of friends and relatives will not affect my use. Total. 6 12.0%. 44 88.0%. 50 100%. . i Un.
(40) respondents percentage. 19 35.2%. 35 64.8%. 54 100%. The investigation also shows that different service elements will affect patients’ use decisions. We found that opinions on consulting services significantly differ between adopters and non-adopters (see table 5-14). Further, the results show that adopters are more likely to expect consulting services. In addition to consulting services, the provision of educational information is also important for adopters. Table 5-15 shows that 30% of the adopters ranked the provision of educational information as their top priority. Table 5-14 The impact of consulting service on adoption Whether patients expect consulting services yes. 立. 17 34%. ‧ 國. 33 66%. %. 35 64.8%. ‧. 19 35.2%. total. 學. Adopters respondents percentage Non-adopters respondents percentage. 政 no 治 大. %. sit. y. Nat. Adopters respondents percentage Non-adopters respondents percentage. al. n. yes. er. io. Table 5-15 The impact of health education information on adoption Whether patients prioritize health education. 15 30% 2 3.7%. Ch. no. engchi. i Un. v. total. 35 70%. 50 100%. 52 96.3%. 54 100%. Finding 3: Recording physiological information has a significant impact on continued use The investigation reveals that recording physiological information is an important service feature that will affect patients’ willingness to continue using the service. The reason may be that recording physiological information is effective for diet control. The data indicate that effectively managing physiological information 36 .
(41) can improve glycemic control and decrease glycosylated hemoglobin (HbA1c) by up to 2%.Conversely, a lack of dietary compliance is a major barrier in achieving glycemic control in diabetes. Therefore, patients would be concerned about controlling what they eat, and thus recording physiological information is important to patients. Finding 4: Self-evaluation, professional suggestions, and the frequency of service supply affect both intention and adoption The findings indicate that promoting the service through the Internet or magazines is effective in increasing the intention to use and the adoption of the service. Service designers could also cooperate with doctors to promote the e-health service. Finding 5. 政 治 大. User age affects both intention and continued use The investigation also reveals that user age has affects patients’ intentions and continued use. The analysis further shows the patients who exhibit the highest levels of intention are between 35 and 50 years of age, and those who are willing to continue their use regardless of the expense are between 60 and 65 (see table 5-16) The results can help service designers identify target groups for service promotion.. 立. ‧. ‧ 國. 學. Nat. n. al. Ch. engchi. Over 65. er. io. Effect of user age on intention and continued use Under 20 20-35 35-50 60-65 intention to use e-health services 13.5% 48.6% 35.1% percentage 2.7% continue using e-health services 20% 30% 40% percentage 2%. sit. y. Table 5-16 The impact of user age on intention and continued use. i Un. v. 8.5%. 8%. Finding 6: The analysis form service, user disease type, platform medical satisfaction, platform operational satisfaction, and service medical satisfaction are important service features that affect the three stages of use. Our study found that providing analysis forms is important across the three stages of use. The analysis also found that patients who suffer from Type 2 diabetes are more likely to intend to use the service. However, patients who suffer from Type 1 diabetes are more willing to adopt and continue to use the service. This difference deserves further analysis in the future. Moreover, our study found that individuals with higher levels of platform medical satisfaction, platform operational satisfaction, and service 37 .
(42) medical satisfaction are more likely to intend to use the service and are more willing to use and continue using the e-health service. Finding 7: The Caring Service cannot discriminate among the three stages of use Of the variables we tested, we found that caring service cannot effectively discriminate among of usage levels. Based on our questionnaire interviews in the clinic, many patients express an interest in the caring service, and thus the caring service maybe equally important across the three stages, and thus this variable does not exhibit significant differences across usage groups.. 立. 政 治 大. ‧. ‧ 國. 學. n. er. io. sit. y. Nat. al. Ch. engchi. 38 . i Un. v.
(43) CHAPTER 6: CONCLUSION 6.1 Summary In Taiwan, many government-supported projects aim to establish e-health services, but most of these efforts fail because of insufficient customer adoption. Once government support ends, so does the service. Therefore, the aim of this study is to determine key service features that can attract customers to adopt and continue to use e-health services. The final goal is to make the e-health services sustainable. We divided customers into three groups: potential customers, adopters, and adopters who are willing to continue to use the service. We use the service concept to classify our service features into five categories: by whom, what, for whom, when, and how. We are interested in identifying the service features that can interest potential customers, enhance their willingness to adopt the service, and motivate existing customers to continue using the service. We compare opinions on service features across these three groups and determine features on which opinions differ significantly across the groups. The results can help hospitals such as NTUH to design e-health services.. 立. 政 治 大. ‧ 國. 學. ‧. The results indicate that the factors affecting patients’ intention to adopt the services are:. y. Nat. (1) The channel to join the service (through patients’ self- evaluation). er. io. (3) Disease type and age. sit. (2) The components of the services (symptom analysis, alarm service). al. n. iv n C h eplatform. service and i U n g c h(Operational. (4)The frequency of service provision. (5) Satisfaction with the satisfaction with the platform, Medical satisfaction with the platform, Operational satisfaction with the service). Moreover, the factors that affect patient decisions to use the services include: (1) The channel to join the service (through patients’ self- evaluation, social relationships, professional suggestion) (2) The components of the service (symptom analysis, health education information, medical information) (3) Disease type and age (4)The frequency of service provision (5) Satisfaction with the service and platform. (Operational satisfaction with the platform, Medical satisfaction with the platform, Medical satisfaction with the service, 39 .
(44) Operational satisfaction with the service) Furthermore, the results indicate the factors affecting patients’ decisions to continue using the service are: (1) The components of the service (physiological data recording, symptom analysis) (2) Disease type and age (3) Satisfaction with the service and platform. (Operational satisfaction with the platform, Medical satisfaction with the platform, Medical satisfaction with the service, Operational satisfaction with the service) 6.2 Limitations and Suggestions for Future Research. In this study, we summarize important e-health service features based on past research and explore their impacts on different usage stages. The results can help e-health service designers to understand what the important service features are and how to increase patients’ use levels. In this study, we examine user type into age and disease. We suggest that future researcher could take different family income or the wiliness of family members into consider, we also suggest that future researchers should build upon the model developed in this study through a further examination of the service factors identified. Moreover, our data were all collected from NTUH. NTUH is one of the largest medical centers in the metropolitan area of Taiwan, and hence the results of this research may to some extent reflect patients’ opinions in the metropolitan areas of Taiwan. Future researchers could conduct similar research. 立. 政 治 大. ‧. ‧ 國. 學. sit. y. Nat. n. al. er. io. focusing on individuals residing in rural areas. A survey conducted across different areas could also further verify the results of this study.. Ch. engchi. 40 . i Un. v.
(45) Reference Al-Gahtani, S. S., & King, M. (1999). Attitudes, satisfaction and usage: factors contributing to each in the acceptance of information technology. Behaviour & Infomation Technology, 18(4), 277-297. Anderson, E. W., & Sullivan, M. W. (1993). The antecedents and consequences of customer satisfaction for firms. Marketing science, 12(2), 125-143. Arch G.M., Ngaire K.F., Clive D.B., Katherine H. &Christopher P. (2003) Perspectives from the United Doctors developing patient trust: Perspectives from the United States and New Zealand.NZFP , 30(5),336-341". 政 治 大. Bhattacherjee, A. (2001). Understanding information systems continuance: An expectation-confirmation model. MIS quarterly, 25(3), 351-370.. 立. ‧ 國. 學. Catwell, L., & Sheikh, A. (2009). Evaluating eHealth Interventions: The Need for Continuous Systemic Evaluation. Plos Medicine, 6(8), 1-6.. ‧. n. al. er. io. sit. y. Nat. Clark, G., Johnston, R., Shulver, M., 2000. Exploiting the service concept for service design and development. In: Fitzsimmons, J., Fitzsimmons, M. (Eds.), New Service Design. Sage, Thousand Oaks, CA, pp. 71–91.. i Un. v. Communication from the Commission to the Council, the European Parliament, the European Economic and Social Committee and the Committee of the Regions. e-Health-making healthcare better for European citizens: an action plan for a European e-Health Area. Available at: http://europa.eu.int/eur-lex/en/com/ cnc/2004/com2004_0356en01.pdf. Accessed January 29, 2006.. Ch. engchi. Cooper, R. B.; and Zmud, R. W. (1990) .Information Technology Implementation Research: A Technological Diffusion Approach. Management Science, vol. 36, n°2, 1990, pp. 123-139. J. A. Czepiel, L. Rosenberg and A. Akerele, Perspectives on Consumer Satisfaction,Proceedings of the 1974 National Conference, American Marketing Association Chicago: American Marketing Association, 1975: 119-123. Reprinted in Japan in YTV Report, No. 98 (May 1975): 64-69. 41 .
數據
+7
相關文件
Reading Task 6: Genre Structure and Language Features. • Now let’s look at how language features (e.g. sentence patterns) are connected to the structure
• To introduce the use of the LPF as a tool for planning the school English Language curriculum; and
Understanding and inferring information, ideas, feelings and opinions in a range of texts with some degree of complexity, using and integrating a small range of reading
Writing texts to convey information, ideas, personal experiences and opinions on familiar topics with elaboration. Writing texts to convey information, ideas, personal
• ‘ content teachers need to support support the learning of those parts of language knowledge that students are missing and that may be preventing them mastering the
Promote project learning, mathematical modeling, and problem-based learning to strengthen the ability to integrate and apply knowledge and skills, and make. calculated
Now, nearly all of the current flows through wire S since it has a much lower resistance than the light bulb. The light bulb does not glow because the current flowing through it
• to develop a culture of learning to learn through self-evaluation and self-improvement, and to develop a research culture for improving the quality of learning and teaching
Writing texts to convey simple information, ideas, personal experiences and opinions on familiar topics with some elaboration. Writing texts to convey information, ideas,
