國立臺灣大學公共衛生學院健康政策與管理研究所 碩 士 論 文
Institute of Health Policy and Management College of Public Health
National Taiwan University Master Thesis
患有重度二尖瓣逆流的老年患者能否從經導管二尖瓣 的修補手術治療中受益?
Can elderly patients with severe mitral regurgitation benefit from trans-catheter mitral valve repair?
李慶威 Ching-Wei Lee
指導教授:鍾國彪 教授 Advisor: Prof. Kuo-Piao Chung
中華民國一百零七年六月
Jun, 2018
論文口試委員審定書、國立臺灣大學碩士班研究生論文審定證明書。
Acknowledgement
This research is completed in conjunction of structural heart team in Taipei Veterans General Hospital and Professor Kuo-Piao Chung’s laboratory in National Taiwan University. During this period, I have worked with a great number of people, especially my mentors in the hospital (Dr. Shih-Hsien Sung and Dr. Wen-Chung Yu), who contributed to my research in various ways. It is my pleasure to show my appreciation to them all in my humble acknowledgement.
I would like to convey my gratitude to Professor Kuo-Piao Chung for his supervision, advice, and guidance in the quality management for this novel trans-catheter technique. With his inspiration and instruction, our team has been awarded The Symbol of National Quality by Institute for Biotechnology and Medicine Industry in 2017. He provided me persistent encouragement and support in many ways. I am sincerely indebted to him more than he knows.
Finally, this research is dedicated to my family- I-Hsin Lee (my father), Ku- Hwa Chen (my mother), Yu-Ling Ho (my wife), and my two adorable daughters (Sunny and Jessie) for their love and support. Their encouragement made all this effort possible.
ENGLISH ABSTRACT
Background: Age is a traditional risk factor for open-heart surgery. The efficacy and safety of transcatheter edge-to-edge mitral valve repair, using MitraClip, has been demonstrated in patients with severe mitral regurgitation (MR). Since octogenarians or even older patients are usually deferred to receive open-heart surgery, the main interest of this study is to elucidate the procedural safety and long term clinical impact of MitraClip in elderly patients.
Methods: Patients with symptomatic severe MR were evaluated by the heart team.
For those with high or prohibitive surgical risks, transcatheter mitral valve repair was performed in hybrid operation room. Transthoracic echocardiography (TTE), blood tests, and six-minute walk test (6MWT) were performed before, 1-month, 6-month, and 1 year after surgery.
Results: A total of 46 consecutive patients receiving MitraClip procedure were enrolled. 19 patients (84.2 ± 4.0 years, 63% male) were over 80 year-old and 27 (73.4
± 11.1 years, 81% male) were younger than 80. Except for poorer left ventricular ejection fraction (LVEF) in the younger group, there was no significant difference in baseline characteristics, comorbidities, and surgical risk profiles. The procedural success rate was similar (aged ≥80 years and <80 years, 95% vs. 93%, p = 1.00).
There was no peri-procedural death, myocardial infarction, stroke or any events requiring emergent cardiac surgery in both groups. Compared with baseline, the significant reduction in MR severity was achieved after the procedure and sustained for 1 year. At the same time, all the patients benefited from significant improvement
in New York Heart Association (NYHA) functional class after the procedure. The NT-proBNP level continuously decreased since 1st month after the index procedure. The 6MWT increased from 259 ± 114 meters to 313 ± 107 (p = 0.02) at 1 month, and up to 319 ± 92 (p = 0.03) at 1 year. During follow-up period, 6 patients experienced death whereas 3 are cardiovascular mortality. The overall 1-year survival rate was 86% (80% in aged ≥80 years and 88% in those < 80 years, p = 0.590). There was also no difference in 1-year free from all-cause mortality or heart failure admission rate between two groups (70% in aged ≥80 years and 78% in those < 80 years, p = 0.738).
By univariate analysis, pre-procedural 6MWT was a predictor for all-cause mortality (OR 0.99, 95% CI: 0.982-0.999, p = 0.026) after the MitraClip procedure but not age (OR 1.12, 95% CI: 0.975-1.299, p = 0.108)
Conclusions: Trans-catheter edge-to-edge mitral valve repairs are safe and have positive clinical impact in subjects with severe MR, even in advanced age.
Octogenarians can also benefit from MitraClip procedure in respect of heart failure symptoms and functional capacities.
Keywords: mitral regurgitation; transcatheter mitral valve repair
CHINESE ABSTRACT
背景:年齡是開心手術的傳統危險因子。 使用 MitraClip 的經導管緣至緣二尖 瓣修補手術的有效性和安全性已在重度二尖瓣逆流患者中得到證實。 由於 80 歲以上的老年患者通常因為年長而不願意或是被外科醫師拒絕接受開心手術,
因此本研究的主要目的是闡明 MitraClip 在老年患者中的安全性和長期臨床效果。
方法:患有重度二尖瓣逆流的心臟病患者皆須接受心臟團隊的完整評估。 對於 手術風險較高的患者,在複合手術室進行經導管二尖瓣修修補手術。 在手術前,
1 個月,6 個月和 1 年時進行經胸前心臟超音波檢查,血液檢查和 6 分鐘步行試 驗。
結果:共有連續 46 名接受 MitraClip 手術的患者收入此項研究。 共 19 位病患超 過 80 歲(平均 84.2±4.0 歲,男性 63%),27 位病患年齡小於 80 歲(平均 73.4±11.1 歲,81%男性)。除年齡較小此組病患的左心室射出分率較低之外,
兩組在其他合併症和手術風險概況沒有顯著差異。兩組的手術成功率相似(年 齡≧80 歲 vs. <80 歲,95%vs. 93%,P = 1.00)。在手術安全性方面,兩組均未 發生手術期死亡,心肌梗死,中風或任何需要緊急心臟手術的事件。與手術前 相比,術後二尖瓣逆流嚴重程度顯著降低,並持續 1 年。同時,所有患者在手 術後都從紐約心臟協會心衰竭功能類的顯著改善中受益。 心衰竭指數 NT- proBNP 水平從術後 1 個月時持續下降並持續到一年的隨訪。六分鐘可行走距離 在 1 個月時從 259±114 米增加到 313±107(p = 0.02),在 1 年時增加到 319±92
(p = 0.03)。追蹤期間,6 例患者死亡,其中包含3 例心血管死亡。總體 1 年
生存率為 86%(80 歲以上為 80%,80 歲以下為 88%,p = 0.590)。兩組患者
歲以下為 78%,P = 0.738)。通過單變量分析,術前六分鐘可行走距離是 MitraClip 術後全因死亡率的預測指標(OR 0.99,95%CI:0.982-0.999,P = 0.026),而非年齡(OR 1.12,95%CI:0.975-1.299 ,p = 0.108)
結論:經導管緣至緣的二尖瓣修補手術是安全的,對重度二尖瓣逆流的患者即 使在高齡時也具有正面的臨床效果。 對於心臟衰竭症狀和功能恢復,80 歲以上 的病患也可以受益於 MitraClip 手術。
關鍵詞:二尖瓣逆流; 經導管二尖瓣修補手術
目錄
Chapter 1 Introduction 8
Chapter 2 Methods
2.1. Study participants 2.2. Study protocol
2.3. Echocardiographic measurements 2.4. Transcatheter mitral valve repair 2.5. Statistical analysis
10 10 10 11 11 Chapter 3 Results
3.1. Patient characteristics 3.2. Procedure outcomes
3.3. Clinical improvements and 1-year follow-up
13 13 13 Chapter 4 Discussion
4.1. Clinical unmet need of treating severe MR in elderly patients 4.2. Current experience of transcatheter mitral edge-to-edge repair in elderly patients
4.3. Reimburse or not? From health economic perspective 4.4 Limitation
15 15
17 18
Chapter 5 Conclusion and future direction 19
Reference 20
Tables and figures 24
Appendix 1. Literature review
Appendix 2. Institution review board documentation
31 39
CHAPTER 1. INTRODUCTION
More than 10% of the subjects, aged≥ 75 years have moderate to severe mitral regurgitation (MR)1. From population studies, severe MR is considered as an aging disease since the disease burden is higher in elderly subjects. Along with the prolonging of life expectancy, the trend of deaths related to valvular heart disease upstroke significantly in the past three decades.2 Patients with symptomatic severe MR, if left untreated, would experience progressive heart failure, and the 5-year mortality rate could be as high as 50%.3 Although mitral valve repair or replacement is the standard treatment for severe MR, almost one-half of the patients were deferred to receive surgery in Euro Heart Survey.4 Moreover, up to 85% of the octogenarians refused or declined to receive open-heart surgery mainly because of advanced age.
The expected number of underutilization in mitral valve surgery could be higher in Asians due to culture differences between east and west. There is a clinical unmet need in treating severe MR properly especially in elderly subjects.
The transcatheter edge-to-edge mitral valve repair, using MitraClip (Abbott Vascular, Menlo Park, CA, USA), has been suggested as an alternative of mitral valve therapy for patient with severe symptomatic MR who carries high or prohibitive surgical risk.5 In the Endovascular Valve Edge-to-Edge Repair Study (EVEREST II), MitraClip has shown superior safety and acceptable durability up to 5-years in surgical eligible patients with severe MR.6,7 The safety and feasibility of MitraClip regarding to the improvements of clinical symptoms and exercise capacities as well as reverse remodeling effect has also been reported in the initial first 20 Taiwanese.8 On the other hand, the paucity of data in procedural safety and long term clinical impact in elderly patients warrant further study to elucidate, especially in Asians.
In the present study, we retrospectively exam our cohort subjects who receive trans-catheter mitral valve repair for severe MR in a single tertiary center.
Octogenarians or even older patients were compared to younger subjects in respect of procedural outcomes and long-term clinical impact after receiving MitraClip.
CHAPTER 2. MATERIALS AND METHODS 2.1. Study participants
Subjects with heart failure and severe MR were eligible for this study. All patients would undergo a standard diagnostic workup, including medical history taking, physical examinations, functional capacity assessments by the New York Heart Association (NYHA) classification and 6-minute walk test (6MWT). The echocardiogram, diagnostic coronary angiography, and right heart catheterizations were performed for pre-operative evaluation. The heart team would disclose the surgical risks and shared-decision-making process was applied for the choice of treatment. Patients undergone trans-catheter mitral valve repair were enrolled in this analysis. The investigation conformed to the principles outlined in the Declaration of Helsinki. A written informed consent approved by our institutional review board was obtained from each subject before enrollment.
2.2. Study protocol
In addition to the pre-operative evaluations, patients would undergo repeated assessments for functional capacity and cardiac performance by transthoracic
echocardiogram at 1, 6, and 12 months after the index procedure. Blood tests at fasting were also obtained for the measures of hemoglobin, serum creatinine, and N- terminal pro-B type natriuretic peptide (NT-proBNP) levels. All participants were followed in the clinics or by telephone contact every month for a year.
2.3. Echocardiographic measurements
All patients received a comprehensive Doppler and M-mode transthoracic echocardiography according to the recommendations of American Society of
Echocardiography.9, 10 Left ventricular ejection fraction were measured by biplane Simpson’s method and the effective regurgitant orifice of mitral regurgitation were also calculated.11 The severity of mitral regurgitation was then graded as mild (grade 1), mild- to moderate (grade 2), moderate- to severe (grade 3), or severe (grade 4) accordingly.12 The etiology of MR is classified as degenerative MR (prolapsing leaflets or rupture chordae) and functional MR (consequence of annulus dilatation or abnormal left ventricular function).13
2.4. Transcatheter mitral valve repair
The procedure was conducted under general anesthesia with the guidance of fluoroscopy and transesophageal echocardiography in a hybrid operative room. The techniques for trans-catheter mitral edge-to-edge repair have been described in detail.
6 In brief, MitraClip was introduced into left atrium after the transseptal puncture to grasp the leaflets and minimize the regurgitation.
Clinical end points were defined according to the Mitral Valve Academic Research Consortium (MVARC).14 Procedural success was defined as a successful implantation of one or more clips to immediately reduce mitral regurgitation of less than grade 2.15 Procedure related complications of single leaflet detachment,
myocardial infarction, stroke, major vascular complications, conversion to surgery, prolonged intubation for more than 48 hours, and acute kidney injury were recorded accordingly. The procedure duration was defined as the time interval between start of vascular puncture and end of the vascular closure.
2.5. Statistical analysis
Means, standard deviations, and percentages were used to describe the
characteristics of the study population. Independent t-test and χ2- test were used to compare the baseline characteristics between octogenarians and younger patients.
Because of the skewed distribution, NT-proBNP was taken in Ln transformation prior to the statistical analysis. Predictors of all-cause death among baseline characteristics, echocardiographic findings, blood test, and pre-procedure functional capacity
variables were investigated using penalized logistic regression. Cumulative events rate at follow-up were plotted according to the Kaplan-Meier method and differences in survival and disease-free intervals were tested with the log-rank test. Statistical significances were set at P<0.05 and all statistical analyses were carried out using SPSS 15.0 (SPSS Inc., Chicago, IL, USA)
CHAPTER 3. RESULTS 3.1. Patient characteristics
A total of consecutive 46 patients treated with MitraClip were included in this analysis. 19 patients (84.2 ± 4.0 years, 63% male) were over age of 80 years and 27 (73.4 ± 11.1 years, 81% male) were younger than 80. The baseline characteristics were displayed in Table 1. The patients in both groups were characterized by high surgical risk (median EuroSCORE II of 10.2 % and median STS-PROM score of 7.3% for mortality), and multiple morbidities. As compare to younger group, there were more degenerative MR (aged ≥80 years and <80 years, 68% vs. 37%, p = 0.04) and having better left ventricular systolic function (LVEF, aged ≥80 years and <80 years, 54.9 ± 11.3% vs. 44.4 ± 15.2%, p = 0.014) in the elderly group. All of the participants had severe MR with a mean effective regurgitation orifice of 49 ± 21 mm2 and 94% of them were with NYHA Fc III to IV symptoms.
3.2. Procedure outcomes
Among the 46 procedures, the procedures success rate was 95% in the elderly group and 93% in the younger group (p=1.00). There was no peri-procedure death, myocardial infarction, stroke or any adverse events requiring emergent cardiac surgery in both groups. There was no significant difference in vascular access
complications, rate of using mechanical ventilation over 48 hours, and post-procedure hospital stays between groups. (Table 2)
3.3. Clinical improvements and 1-year follow-up
After the index procedure, the clinical symptoms and functional capacity were significantly improved with time. More than 80% of patients were with NYHA Fc I or
II symptoms during follow-up, as opposed to only 13% of patients were with NYHA Fc I or II before intervention (Figure 1a). After fixing the MR, 94% of patients were with mild or mild to moderate degree of MR at 1 month and 92% of patients were remained mild or mild to moderate degree of MR at 1 year (Figure 1b). The Ln NT- proBNP level decreased from 7.6 ± 1.2 to 7.3 ± 1.2 at 1 month (N=40, p = 0.004), 6.9
± 1.4 at 6 months (N=36, p < 0.001), and further down to 6.6 ± 0.8 (N=19, p = 0.008) at 1 year (Figure 2a). The 6MWT increased from 259 ± 114 meters to 313 ± 107 (N=34, p = 0.02) at 1 month, and up to 319 ± 92 (N=16, p = 0.03) at 1 year (Figure 2b). During follow-up period, 6 patients experienced death whereas 3 are
cardiovascular mortality. The overall 1-year survival rate was 86% (80% in aged ≥80 years and 88% in those < 80 years, p = 0.590) (Figure 3a). There was also no
difference in 1-year free from all-cause mortality or heart failure admission rate between two groups (70% in aged ≥80 years and 78% in those < 80 years, p = 0.738) (Figure 3b). By univariate analysis, pre-procedural 6MWT was a predictor of all- cause mortality (OR 0.99, 95% CI: 0.982-0.999, p = 0.026) after the MitraClip procedure but not age (OR 1.12, 95% CI: 0.975-1.299, p = 0.108) (Table 3).
CHAPTER 4. DISCUSSION
The present study has demonstrated the efficacy and safety of trans-catheter mitral valve repair with MitraClip to treat patients with severe MR in both
octogenarians and younger patients who carry high surgical risks.
4.1. Clinical unmet need of treating severe MR in elderly patients
Advanced age is a traditional risk factor for peri-operative morbidities or mortality in open-heart surgery.1617 In Euro Heart Survey, every 10-years increase of age carries nearly 70% incremental risk for 1-year mortality in subjects who
underwent surgical mitral valve intervention.4 In the same survey, impaired left ventricular ejection fraction, older age, and comorbidities were the most striking characteristics of patients who denied surgery. From systemic review, even surgical correction is the standard treatment for subjects with severe MR, surgical correction of MR in octogenarians is associated with high perioperative mortality and poor long- term survival with an uncertain benefit on quality of life.18
4.2. Current experience of transcatheter mitral edge-to-edge repair in elderly patients
As compare to surgical mitral valve intervention, trans-catheter mitral valve repair with MitraClip device appears remarkably safe in the elderly population in terms of acute mortality and complications.19 From GRASP (Getting Reduction of Mitral Insufficiency by Percutaneous Clip Implantation) registry, MitraClip was shown to be safe and effective in mot patients, with similar hospital length of stay, one-year clinical outcomes and re-hospitalization rates in either elderly or younger patients.20 As comparing to previous studies, our cohort demonstrated that
octogenarians after the procedure could benefit from increase of walking distances in 6MWT. This functional regain sustained during 1 year-follow up. This information is important especially in the elderly subjects. In patients with severe MR, effort
dyspnea or exercise intolerance significantly limited physical activity and clinical frailty was adversely affects quality of life.21 In fact, Metze et al. found frailty or pre- frailty was diagnosed in 94% of patients who underwent trans-catheter mitral valve repair.22 Interestingly, we found the distance of pre-procedure 6MWT can predict the all-cause mortality at 1 year. This finding may correspond to previous study, which showed frail patients still benefit from trans-catheter mitral valve repair in spite of higher mortality compared with non-frail patients.22 In TRAMI (The transcatheter mitral valve interventions) registry, pre-procedural 6MWT distance <200 meters showed a strong trend towards increased 1-year mortality in patients underwent MitraClip procedure.23
Given the Asian patients are reluctant to undergo open-heart surgery and the observed mortality is higher than the surgical risk prediction model,24,25 there is an unmet need to ameliorate the disease awareness and the therapeutic adherence in Asians. Even though more than half of the subjects who underwent MitraClip procedure at age over 75 in western registries, Asians paid more attention about peri- operative complications and long-term efficacy especially after age of 80. In our study, the 1 year overall survival rate is 86%,26 which is very similar to western data, 80% in the TRAMI registry from Germany, 84% in GRASP registry from Italy, 27 83% in ACCESS-EU registry in the Europe.28 In TRAMI registry, they found the predictors of 1-year mortality were NYHA class IV, anemia, previous aortic valve intervention, poor renal function, peripheral artery disease, left ventricular ejection fraction <30%, severe tricuspid regurgitation and procedural failure but not age per se. Every 5-years
increasing age above 60, the surgical risk upgrade in the EuroSCORE II (the European System for Cardiac Operative Risk Evaluation II) for open-heart surgery.
Using GRASP registry, Buccheri et al. developed a risk model for prediction of 1- year mortality in patients undergoing MitraClip implantation. By calculate the data of natural log proBNP level, NYHA Fc IV, mean arterial blood pressure, and
hemoglobin, the GRASP nomogram had superior discriminative ability than
traditional surgical risk prediction model with EuroSCORE II and STS-PROM (the Society of Thoracic Surgeons Predicted Risk of Mortality score).27 The negative impact of advanced age on surgical risk is not observed in trans-catheter mitral valve repair. However, there are still uncertainties of procedure long-term efficacy when we try to treat extremely elderly patients with trans-catheter approach. Nonagenarians showed an increased peri-procedural mortality and higher mortality in follow-up compared to octogenarians who underwent trans-catheter aortic valve intervention (TAVI).29 Nowadays, there is no data investigating safety and efficacy of trans- catheter mitral valve intervention in nonagenarians. In our cohort, two nonagenarians with degenerative MR received MitraClip procedures. One subject suffered from acute rupture of abdominal aortic aneurysm and led to mortality at 6 months after index procedure. Another patient suffered from re-hospitalization due to heart failure at 1 month after index hospitalization. This finding indicates age alone is not a predictive factor but apply for treatment should be carefully evaluated by the heart team on an individual basis.
4.3. Reimburse or not? From health economic perspective
Since the American and European guidelines have recommended the trans- catheter mitral valve repair is a reasonable treatment option in patients with
prohibitive surgical risks.5, 30, the utilization of therapy across the national population is highly correlated with the reimbursement policy.31 Not surprising, higher national economic index and TAVI-specific reimbursement systems were associated with higher utilizations of this therapy. The financial barrier of every individual to access the therapy should be evaluated by health-economy approach. Compare to
conservative medical treatment along, the average treatment effect of MitraClip in subjects with severe MR was decreasing 9.5% probability of dying at 12 months, decreasing 50% probability of re-hospitalization for heart failure at 12 months, and 3.01 incremental quality-adjusted life years. The incremental cost-effectiveness ratio is € 7908, which is taken into cost-effective treatment in Europe.32 In Taiwan, the National Health Insurance Administration reimbursed the procedural fee for TAVI and age over 80 is one of the indications for the procedure. Our study demonstrated superior safety and efficacy of MitraClip in octogenarians and further study is warranted to evaluate future potential for reimbursement.
4.4. Limitation
Our study has the inherent limitations of its observational design, single center experience, and the data were collected retrospectively. Even the preliminary data may have encouraged the clinical application of MitraClip, the case number is still limited. The long-term impacts of MitraClip on hemodynamics, clinical outcomes and functional recovery after 1 year should be further evaluated. Parallel surgical or medical control groups are lacking. According to the guideline, we believe MitraClip should be reserved for patients with high or prohibitive surgical risks.
CHAPTER 5. CONCLUSION AND FUTURE DIRECTION
In conclusion, trans-catheter edge-to-edge mitral valve repairs are safe and have positive clinical impact in Asians with severe MR, even in advanced age. For those with eligible vavular anatomy, octogenarians can also benefit from MitraClips in respect of heart failure symptoms and functional capacities improvement up to 1-year follow-up. This preliminary experience in Taiwan demonstrates that advanced age per se should not be the only reason for deferring trans-catheter mitral valve repair.
Since mini-invasive open-heart surgery has great progress in the last decades, tailored therapy to every individual who suffer from severe MR will be a promising approach. Age, left ventricular systolic function, comorbidities, and expectation from patient and families should be evaluated coordinately by heart team approach. Our preliminary work contribute to a little part in the whole picture of treating elderly patients with severe MR. In the near future, we will try to compare the change in left ventricular remodeling, arterial stiffness, neurological cognitive function as well as functional capacity before and after the trans-catheter mitral valve repair. We believe with every little contribution per se, the disease burden in disability of elderly with severe MR will be much eased by proper treatment.
REFERENCES
1. Nkomo VT, Gardin JM, Skelton TN, Gottdiener JS, Scott CG and Enriquez- Sarano M. Burden of valvular heart diseases: a population-based study. Lancet.
2006;368:1005-11.
2. Coffey S, Cox B and Williams MJ. Lack of progress in valvular heart disease in the pre-transcatheter aortic valve replacement era: increasing deaths and minimal change in mortality rate over the past three decades. Am Heart J.
2014;167:562-567 e2.
3. Goel SS, Bajaj N, Aggarwal B, Gupta S, Poddar KL, Ige M, Bdair H, Anabtawi A, Rahim S, Whitlow PL, Tuzcu EM, Griffin BP, Stewart WJ, Gillinov M, Blackstone EH, Smedira NG, Oliveira GH, Barzilai B, Menon V and Kapadia SR. Prevalence and outcomes of unoperated patients with severe symptomatic mitral
regurgitation and heart failure: comprehensive analysis to determine the
potential role of MitraClip for this unmet need. Journal of the American College of Cardiology. 2014;63:185-6.
4. Mirabel M, Iung B, Baron G, Messika-Zeitoun D, Detaint D, Vanoverschelde JL, Butchart EG, Ravaud P and Vahanian A. What are the characteristics of
patients with severe, symptomatic, mitral regurgitation who are denied surgery?
Eur Heart J. 2007;28:1358-65.
5. Nishimura RA, Otto CM, Bonow RO, Carabello BA, Erwin JP, 3rd, Fleisher LA, Jneid H, Mack MJ, McLeod CJ, O'Gara PT, Rigolin VH, Sundt TM, 3rd and Thompson A. 2017 AHA/ACC Focused Update of the 2014 AHA/ACC Guideline for the Management of Patients With Valvular Heart Disease: A Report of the American College of Cardiology/American Heart Association Task Force on Clinical Practice Guidelines. J Am Coll Cardiol. 2017;70:252-289.
6. Feldman T, Foster E, Glower DD, Kar S, Rinaldi MJ, Fail PS, Smalling RW, Siegel R, Rose GA, Engeron E, Loghin C, Trento A, Skipper ER, Fudge T, Letsou GV, Massaro JM, Mauri L and Investigators EI. Percutaneous repair or surgery for mitral regurgitation. N Engl J Med. 2011;364:1395-406.
7. Feldman T, Kar S, Elmariah S, Smart SC, Trento A, Siegel RJ, Apruzzese P, Fail P, Rinaldi MJ, Smalling RW, Hermiller JB, Heimansohn D, Gray WA, Grayburn PA, Mack MJ, Lim DS, Ailawadi G, Herrmann HC, Acker MA, Silvestry FE, Foster E, Wang A, Glower DD, Mauri L and Investigators EI. Randomized Comparison of Percutaneous Repair and Surgery for Mitral Regurgitation: 5-Year Results of EVEREST II. Journal of the American College of Cardiology. 2015;66:2844-54.
8. Lee CW, Sung SH, Tsai YL, Chang TY, Hsu CP, Lu CC and Shih CC. Initial experience with percutaneous edge-to-edge transcatheter mitral valve repair in a tertiary medical center in Taiwan. J Chin Med Assoc. 2018;81:305-310.
9. Lang RM, Bierig M, Devereux RB, Flachskampf FA, Foster E, Pellikka PA, Picard MH, Roman MJ, Seward J, Shanewise JS, Solomon SD, Spencer KT, Sutton MS, Stewart WJ, Chamber Quantification Writing G, American Society of
Echocardiography's G, Standards C and European Association of E.
Recommendations for chamber quantification: a report from the American Society of Echocardiography's Guidelines and Standards Committee and the Chamber Quantification Writing Group, developed in conjunction with the
European Association of Echocardiography, a branch of the European Society of Cardiology. J Am Soc Echocardiogr. 2005;18:1440-63.
10. Rudski LG, Lai WW, Afilalo J, Hua L, Handschumacher MD,
Chandrasekaran K, Solomon SD, Louie EK and Schiller NB. Guidelines for the echocardiographic assessment of the right heart in adults: a report from the American Society of Echocardiography endorsed by the European Association of Echocardiography, a registered branch of the European Society of Cardiology, and the Canadian Society of Echocardiography. Journal of the American Society of Echocardiography : official publication of the American Society of
Echocardiography. 2010;23:685-713; quiz 786-8.
11. Zoghbi WA, Enriquez-Sarano M, Foster E, Grayburn PA, Kraft CD, Levine RA, Nihoyannopoulos P, Otto CM, Quinones MA, Rakowski H, Stewart WJ, Waggoner A, Weissman NJ and American Society of E. Recommendations for evaluation of the severity of native valvular regurgitation with two-dimensional and Doppler echocardiography. J Am Soc Echocardiogr. 2003;16:777-802.
12. Zoghbi WA, Adams D, Bonow RO, Enriquez-Sarano M, Foster E, Grayburn PA, Hahn RT, Han Y, Hung J, Lang RM, Little SH, Shah DJ, Shernan S,
Thavendiranathan P, Thomas JD and Weissman NJ. Recommendations for Noninvasive Evaluation of Native Valvular Regurgitation: A Report from the American Society of Echocardiography Developed in Collaboration with the Society for Cardiovascular Magnetic Resonance. J Am Soc Echocardiogr.
2017;30:303-371.
13. Enriquez-Sarano M, Akins CW and Vahanian A. Mitral regurgitation.
Lancet. 2009;373:1382-94.
14. Stone GW, Adams DH, Abraham WT, Kappetein AP, Genereux P, Vranckx P, Mehran R, Kuck KH, Leon MB, Piazza N, Head SJ, Filippatos G, Vahanian AS and Mitral Valve Academic Research C. Clinical Trial Design Principles and Endpoint Definitions for Transcatheter Mitral Valve Repair and Replacement: Part 2:
Endpoint Definitions: A Consensus Document From the Mitral Valve Academic Research Consortium. J Am Coll Cardiol. 2015;66:308-321.
15. Nickenig G, Estevez-Loureiro R, Franzen O, Tamburino C, Vanderheyden M, Luscher TF, Moat N, Price S, Dall'Ara G, Winter R, Corti R, Grasso C, Snow TM, Jeger R, Blankenberg S, Settergren M, Tiroch K, Balzer J, Petronio AS, Buttner HJ, Ettori F, Sievert H, Fiorino MG, Claeys M, Ussia GP, Baumgartner H, Scandura S, Alamgir F, Keshavarzi F, Colombo A, Maisano F, Ebelt H, Aruta P, Lubos E, Plicht B, Schueler R, Pighi M, Di Mario C and Transcatheter Valve Treatment Sentinel Registry Investigators of the ERPotESoC. Percutaneous mitral valve edge-to-edge repair: in-hospital results and 1-year follow-up of 628 patients of the 2011-2012 Pilot European Sentinel Registry. Journal of the American College of Cardiology.
2014;64:875-84.
16. Roques F, Michel P, Goldstone AR and Nashef SA. The logistic EuroSCORE.
Eur Heart J. 2003;24:881-2.
17. Nashef SA, Roques F, Sharples LD, Nilsson J, Smith C, Goldstone AR and Lockowandt U. EuroSCORE II. Eur J Cardiothorac Surg. 2012;41:734-44;
discussion 744-5.
18. Andalib A, Mamane S, Schiller I, Zakem A, Mylotte D, Martucci G, Lauzier P, Alharbi W, Cecere R, Dorfmeister M, Lange R, Brophy J and Piazza N. A systematic review and meta-analysis of surgical outcomes following mitral valve surgery in
octogenarians: implications for transcatheter mitral valve interventions.
EuroIntervention. 2014;9:1225-34.
19. Buzzatti N, Maisano F, Latib A, Taramasso M, Denti P, La Canna G, Colombo A and Alfieri O. Comparison of outcomes of percutaneous MitraClip versus surgical repair or replacement for degenerative mitral regurgitation in octogenarians. Am J Cardiol. 2015;115:487-92.
20. Scandura S, Capranzano P, Caggegi A, Grasso C, Ronsivalle G, Mangiafico S, Ohno Y, Attizzani GF, Cannata S, Giaquinta S, Farruggio S, Ministeri M, Dipasqua F, Pistritto AM, Imme S, Capodanno D, Di Salvo ME and Tamburino C. Percutaneous mitral valve repair with the MitraClip system in the elderly: One-year outcomes from the GRASP registry. Int J Cardiol. 2016;224:440-446.
21. Uchmanowicz I and Gobbens RJ. The relationship between frailty, anxiety and depression, and health-related quality of life in elderly patients with heart failure. Clin Interv Aging. 2015;10:1595-600.
22. Metze C, Matzik AS, Scherner M, Korber MI, Michels G, Baldus S, Rudolph V and Pfister R. Impact of Frailty on Outcomes in Patients Undergoing
Percutaneous Mitral Valve Repair. JACC Cardiovasc Interv. 2017;10:1920-1929.
23. Ledwoch J, Franke J, Lubos E, Boekstegers P, Puls M, Ouarrak T, von Bardeleben S, Butter C, Schofer J, Zahn R, Ince H, Senges J and Sievert H.
Prognostic value of preprocedural 6-min walk test in patients undergoing transcatheter mitral valve repair-insights from the German transcatheter mitral valve interventions registry. Clin Res Cardiol. 2018;107:241-248.
24. Zhang GX, Wang C, Wang L, Lu FL, Li BL, Han L and Xu ZY. Validation of EuroSCORE II in Chinese patients undergoing heart valve surgery. Heart Lung Circ. 2013;22:606-11.
25. Wang C, Tang YF, Zhang JJ, Bai YF, Yu YC, Zhang GX and Han L.
Comparison of four risk scores for in-hospital mortality in patients undergoing heart valve surgery: A multicenter study in a Chinese population. Heart Lung.
2016;45:423-8.
26. Puls M, Lubos E, Boekstegers P, von Bardeleben RS, Ouarrak T, Butter C, Zuern CS, Bekeredjian R, Sievert H, Nickenig G, Eggebrecht H, Senges J and Schillinger W. One-year outcomes and predictors of mortality after MitraClip therapy in contemporary clinical practice: results from the German transcatheter mitral valve interventions registry. Eur Heart J. 2016;37:703-12.
27. Buccheri S, Capodanno D, Barbanti M, Popolo Rubbio A, Di Salvo ME, Scandura S, Mangiafico S, Ronsivalle G, Chiaranda M, Capranzano P, Grasso C and Tamburino C. A Risk Model for Prediction of 1-Year Mortality in Patients
Undergoing MitraClip Implantation. Am J Cardiol. 2017;119:1443-1449.
28. Maisano F, Franzen O, Baldus S, Schafer U, Hausleiter J, Butter C, Ussia GP, Sievert H, Richardt G, Widder JD, Moccetti T and Schillinger W. Percutaneous mitral valve interventions in the real world: early and 1-year results from the ACCESS-EU, a prospective, multicenter, nonrandomized post-approval study of the MitraClip therapy in Europe. J Am Coll Cardiol. 2013;62:1052-1061.
29. Scholtz S, Dimitriadis Z, Vlachojannis M, Piper C, Horstkotte D, Wiemer M, Gummert J, Fujita B, Benzinger M, Ensminger SM, Borgermann J and Scholtz W.
Transcatheter Aortic Valve Implantation in Nonagenarians: Procedural Outcome and Mid-Term Results. Heart Lung Circ. 2018;27:725-730.
30. Baumgartner H, Falk V, Bax JJ, De Bonis M, Hamm C, Holm PJ, Iung B, Lancellotti P, Lansac E, Munoz DR, Rosenhek R, Sjogren J, Tornos Mas P,
Vahanian A, Walther T, Wendler O, Windecker S and Zamorano JL. 2017
ESC/EACTS Guidelines for the management of valvular heart disease: The Task Force for the Management of Valvular Heart Disease of the European Society of Cardiology (ESC) and the European Association for Cardio-Thoracic Surgery (EACTS). Eur Heart J. 2017.
31. Mylotte D, Osnabrugge RLJ, Windecker S, Lefevre T, de Jaegere P, Jeger R, Wenaweser P, Maisano F, Moat N, Sondergaard L, Bosmans J, Teles RC, Martucci G, Manoharan G, Garcia E, Van Mieghem NM, Kappetein AP, Serruys PW, Lange R and Piazza N. Transcatheter aortic valve replacement in Europe: adoption trends and factors influencing device utilization. J Am Coll Cardiol. 2013;62:210-219.
32. Armeni P, Boscolo PR, Tarricone R, Capodanno D, Maggioni AP, Grasso C, Tamburino C and Maisano F. Real-world cost effectiveness of MitraClip combined with Medical Therapy Versus Medical therapy alone in patients with moderate or severe mitral regurgitation. Int J Cardiol. 2016;209:153-60.
33. Braunschweig F, Cowie MR and Auricchio A. What are the costs of heart failure? Europace. 2011;13 Suppl 2:ii13-7.
34. Murashita T, Okada Y, Kanemitsu H, Fukunaga N, Konishi Y, Nakamura K and Koyama T. Feasibility and efficacy of mitral valve repair for degenerative mitral regurgitation in the elderly. Ann Thorac Cardiovasc Surg. 2014;20:1001-7.
35. Asgar AW, Khairy P, Guertin MC, Cournoyer D, Ducharme A, Bonan R, Basmadjian A, Tardif JC and Cohen DJ. Clinical outcomes and economic impact of transcatheter mitral leaflet repair in heart failure patients. J Med Econ.
2017;20:82-90.
36. Guerin P, Bourguignon S, Jamet N and Marque S. MitraClip therapy in mitral regurgitation: a Markov model for the cost-effectiveness of a new therapeutic option. J Med Econ. 2016;19:696-701.
FIGURES AND TABLES
Table 1 Baseline characteristics between the elderly and younger patients
n = 19 (%), age≥ 80 n = 27 (%), age<80 P value Age (years)
Male Height (cm) Weight (Kg) Morbidities, n (%)
Diabetes mellitus Hypertension
Coronary artery disease Prior stroke
Peripheral vascular disease Chronic atrial fibrillation Prior open heart surgery EuroSCORE II
STS-PROM score HF, NYHA Fc III-IV Laboratory data
Serum creatinine (mg/dL)
84.2 ± 4.0 12 (63) 158.6 ± 9.3
59.8 ± 9.9
6 (32) 14 (74) 10 (53) 5 (26)
1 (5) 12 (63)
3 (16) 9.6 ± 10.8
7.8 ± 5.4 18 (95)
1.5 ± 0.9
73.4 ± 11.1 22 (81) 163.7 ± 7.1 64.2 ± 11.9
6 (22) 14 (52) 14 (52) 5 (19)
2 (7) 16 (59)
6 (22) 10.7 ± 17.1
6.8 ± 8.8 25 (93)
1.9 ± 1.6
<0.001 0.190 0.042 0.195
0.477 0.135 1.000 0.528 0.772 1.000 0.588 0.814 0.681 0.772
0.209
EuroSCORE II= European System for Cardiac Operative Risk Evaluation II;
STS-PROM= the Society of Thoracic Surgeons Predicted Risk of Mortality score;
HF= Heart Failure; NYHA Fc= New York Heart Failure Association Functional class; NT-proBNP= N-terminal prohormone of brain natriuretic peptide; HgB=
Hemoglobin; Na= Serum sodium level; Alb= serum albumin level; Glu= fasting blood glucose; Total cholesterol= serum total cholesterol level; MR= mitral regurgitation; EROA= effective regurgitant orifice area; PASP = pulmonary artery systolic pressure; LVEF = left ventricular ejection fraction.
Ln NT-proBNP HgB (g/dL) Na (mEq/L) Alb (g/dL) Glu (mg/dL)
Total Cholesterol (mg/dL) Echocardiographic parameters Degenerative MR
Functional MR MR EROA (cm^2) LVEF (%)
PASP (mmHg)
7.4 ± 1.2 11.3 ± 1.5
141 ± 6 3.7 ± 0.4 118 ± 49 159 ± 48
13 (68) 6 (32) 45.7 ± 21.3 54.9 ± 11.3 49.7 ± 12.4
7.9 ± 1.3 12.4 ± 2.1
140 ± 4 3.8 ± 0.4
97 ± 20 149 ± 35
10 (37) 17 (63) 52.4 ± 20.9 44.4 ± 15.2 57.3 ± 19.5
0.243 0.06 0.584 0.796 0.082 0.450
0.04
0.299 0.014 0.204
Table 2 Characteristics of the index procedure.
n = 19 (%) n = 26 (%) P value Procedure success
Procedure death
Single leaflet detachment Conversion to surgery
Stroke (embolic/hemorrhagic) Myocardial infarction
Acute kidney injury
Vascular access complications Ventilation > 48 hours
Procedure duration (minutes) Post-procedure hospital stay (days)
18 (95) 0 (0) 0 (0) 0 (0) 0 (0) 0 (0) 0 (0) 1 (5) 1 (5) 195 ± 94 6.6 ± 4.3
25 (96) 0 (0) 0 (0) 0 (0) 0 (0) 0 (0) 0 (0) 1 (4) 3 (12) 176 ± 80 6.3 ± 4.6
1.00 1.00 1.00 1.00 1.00 1.00 1.00 1.00 0.632 0.457 0.827
Table 3 Effects of variables associated with all-cause mortality tested by multiple logistic regressions
OR 95% CI p
Age 1.12 0.975-1.299 0.108
Sex 0.682 0.069-6.784 0.744
LVEF 1.018 0.943-1.099 0.641
PASP 1.039 0.979-1.103 0.203
EuroSCORE II 1.020 0.969-1.074 0.452
FMR 2.211 0.363-13.470 0.390
NT-proBNP 1.000 1.000-1.000 0.798
6MWT distance (meters)
0.990 0.982-0.999 0.026
Serum creatinine 1.282 0.762-2.158 0.350
LVEF = left ventricular ejection fraction; PASP = pulmonary artery systolic pressure; EuroSCORE II= European System for Cardiac Operative Risk
Evaluation II; FMR= functional mitral regurgitation; NT-proBNP = N-terminal prohormone of brain natriuretic peptide; 6MWT = 6 minute walk test.
Figure 1.
(A) Results for NYHA class improvement before, 1 month, 6 months and 12 months after clip implantation.
(B) Results for MR reduction before, 1 month, 6 months and 12 months after clip implantation.
Fig. 2.
(A) Results for Ln NT-proBNP level before, 1 month, 6 months and 12 months after clip implantation.
(B) Results for 6-minute walk distance (meters) before, 1 month, 6 months and 12 months after clip implantation.
Figure 2
Fig. 3. Kaplan-Meier curves at one-year follow-up (A) Freedom from all-cause death
(B) Freedom from all-cause death or re-admission for heart failure.
Figure 3
APPENDIX 1 (LITERATURES REIVEW) 1 重度二尖瓣逆流的疾病負擔
二尖瓣是位於左心房和左心室之間質地柔軟的構造, 正常情況之下在心臟舒張時, 二尖瓣膜會完全打開讓血流通過, 當心臟收縮時, 二尖瓣膜會完全閉合, 使血流能 隨著動脈完全的向前供應至全身器官, 當二尖瓣膜因各類疾病的因素, 而造成瓣 膜無法正常完全關閉時, 隨著心臟收縮, 便會有部份血液會經由二尖瓣膜的縫隙 倒流回心房, 此即稱之為二尖瓣膜逆流, 而因為血液倒流會令心臟、肺部及其他 器官負荷加重,也導致心臟變得擴大。最終,這額外的負荷會導致其他更嚴重 的心臟問題(如心臟衰竭),並可能會引致心跳不規律、中風,甚至猝死等情 況. 二尖瓣膜逆流的分類大致為原發性(因為瓣葉脫垂或腱索斷裂)和續發性(因為 瓣膜環擴大或是心臟擴大功能變差).13 二尖瓣膜逆流的疾病負擔相當可觀。這是 美國最常見的心臟瓣膜病,影響 75 歲及以上的約 10 人中的一人或約 400 萬美
國人1. 隨著預期壽命的延長,過去三十年來與瓣膜性心臟病有關的死亡趨勢顯
著增加.2 有症狀的嚴重二尖瓣膜逆流患者如果不及時治療,將會出現進行性心
臟衰竭,5 年死亡率可能高達 50%,而即便沒有因為此項疾病死亡的病患,也
有高達 90%會經歷心臟衰竭而住院的狀況。3在美國每年 390 億的心臟衰竭費用
中,約 60%是由於心臟衰竭住院治療引起的,其中許多與嚴重二尖瓣膜逆流有 關.33
2 高齡的嚴重二尖瓣膜逆流患者: 臨床尚未被滿足的治療需求
臨床上對於嚴重二尖瓣膜逆流患者,目前歐美的治療指南首選是以開心手術修 復或置換二尖瓣為主。然而,在所有的開心手術中,都必須使用心臟麻痺液和
體外循環機,這可能對手術中風險,或手術後的復原,在老年人或左心室收縮 功能差的病人成為艱鉅的挑戰。事實上,二尖瓣手術風險過高的患者除使用無 效的藥物治療外沒有其他治療選擇。高達 85%的 80 歲以上的老人拒絕接受開 心手術,主要的考量就是因為年齡過大。由於東西方之間的文化差異,一般而 言,因爲亞洲人對於開刀治療這個選項更趨於保守,我們可以預期有更高比率 的亞洲高齡患者無法或是拒絕接受二尖瓣膜開心手術,因此在高齡族群的嚴重 二尖瓣膜逆流患者上,我們需要發展更合適的治療選項,來解決這個臨床上未 被滿足的需求。
3 經導管二尖瓣膜夾手術
MitraClip 這個緣對緣的經導管二尖瓣膜夾修補手術,在隨機對照試驗中 (EVEREST II) 6,7證實安全性和有效性後,於 2013 年 10 月 24 日獲得了 FDA 批 准可使用於已經被心臟團隊確定為高手術風險的嚴重二尖瓣膜逆流患者。在過 去的 10 年中,已經進行了多項臨床研究,已確定該手術對改善生活質量以及健 康經濟效益的合理安全性和長期臨床效果32。(Table 1 and 2) 李等人在最初的 20 位接受 MitraClip 手術的台灣人中8,也證明了此項手術後,患者可改善臨床症 狀和運動能力以及進一步的心臟重朔性效應。然而在另一方面,針對高齡族群,
MitraClip 的手術安全性和長期療效追蹤的數據,目前仍然相對缺乏,尤其是在 亞洲人,至今仍未有相關文獻闡明。
4 80 歲以上有嚴重二尖瓣膜逆流患者的長者應該接受開心手術還是經導管二尖 瓣膜夾手術
Murashita 等人在接受開心二尖瓣手術的 75 歲以上患者中證明了可接受 的手術安全性(住院死亡率 7.3%)和長期存活率(5 年 81%)。然而,有限的
案例數量(N = 55)和單中心設計是這項研究的主要局限性。而且此研究的老 年患者平均年齡為 77 歲,這對 80 歲以上老人也不具有代表性34。通過 Andalib 等人的系統回顧和薈萃分析,顯示對於 80 歲以上老年人的開心二尖瓣手術治療 死亡率高(手術死亡率 7-13%)和長期生存率差(1 年和 5 年時 67%和 29%的 存活率),而且對術後生活質量的影響不確定 18。另一方面,Buzzatti 等人發現 25 名接受 MitraClip 治療的 80 歲以上老年人,儘管年齡較大,症狀較多並且伴 有較多合併症,但與手術組(35 例)相比,術後並發症明顯減少(P <0.05)。
19 然而即便是相關的研究已顯示高齡長者接受經導管瓣膜手術治療的安全性和
有效性,但因為此項手術在臺灣仍屬高單價的自費手術,且任何手術皆有相關 的併發症或手術成功率等治療不確定性問題,在醫療團隊跟病患討論治療可能 的選擇性時,除了臨床實證的療效之外,病患和病患家屬的期望在意的事項也 是決定治療與否的關鍵因素。
5 醫病共同決策在心臟瓣膜介入治療的角色
醫病共同決策 (Shared-decision-making, SDM)是一種以病患為中心,讓醫療照護 團隊和病患一同審視現有的實證和所有可能的治療選項,共同完成決定的過程。
在這個過程當中,醫療人員應盡所能的讓病患了解治療所可能產生的好處和相 關風險,而病患應讓醫療人員理解疾病對自身造成的影響和對未來生活的期許,
藉由不斷的溝通和對話,找到雙方都能接受的最合適治療。雖然執行 SDM 本 身,按照字面上的說明應該是臨床上相當好而且值得推動的程序,然而 SDM 的推動對醫療人員而言的確是有相當的挑戰。醫療行為本身就充滿了許多決定 的空間,這些醫療行為的決定者,通常是醫師,己經習慣在複雜的資訊當中,
整理並分析出對病人最為有利的決定,尤其是心臟的瓣膜手術這樣充滿風險而
且重要的手術決定,如果依照病患的所有檢查結果根據現有歐美治療指南建議,
手術應當被執行,身為醫療資訊最為完整和清楚的醫師,如果因為最後病患堅 持不接受手術時,為何要透過 SDM 來做出可能對病患不利的決定呢? 雖然上述 的論述似乎是符合醫學倫理上醫師必須為病患維護最大利益的精神,然而卻對 於病患自主權造成侵害,更重要的是醫療行為的結果仍是存在有不確定性,以 為出自善意的手術如果結果不如預期,對病患以及家屬不但是很大的挫敗,更 重要的是可能會造成對醫療團隊的責難或不諒解,甚至可能衍生出不必要的醫 療法律糾紛。執行完 SDM 後病患可能會做出對自身疾病醫學上較不利的決定,
但是對於病患自主權的尊重是身為醫療人員應當謹守的本分和倫理,醫病共同 決策的精神就是在於醫療相關從業人員應當盡最大的力量協助病患了解自身疾 病狀況以及最合適治療的方式,讓最大比例的病患都能接受到最合宜的治療,
且享有最好的臨床結果。
6 經導管二尖瓣膜夾手術的臨床和衛生經濟學影響
加拿大的 Asgar 等人研究顯示比起傳統藥物治療,MitraClip 手術可將患者預期 壽命提高到 3.6 年(藥物治療組 1.8 年),質量調整壽命年(QALY)也可有效增 加至 2.76 年(藥物治療組 1.13 年)。每增加一個質量調整壽命年,成本效益比
(ICER)的花費是 32,300 加拿大元。35 Armeni 等人研究顯示 MitraClip 治療嚴 重二尖瓣膜逆流的患者平均治療效果為 12 個月時死亡概率降低 9.5%,12 個月 時心臟衰竭再住院率降低 50%,MitraClip 治療比起藥物治療可增加 3.01 質量 調整生命年,而增量成本效益比為 7908 歐元,這在歐洲成為具有成本效益的治
療手段32。Guerin 等人研究使用馬爾可夫模型,發現增加一個生存年的成本效
益比 ICER 計算時考慮了第一年 MitraClip 器械產生的額外成本(手術組為
29,984 歐元對比藥物治療組為 8557 歐元),以及隨後幾年的成本降低(手術組 為每年 3122 歐元對比藥物治療組 8557 歐元)。因此,平均 ICER 計算為增加 一個生存年為 20,720 歐元36 。
7 國家健康保險給付政策對於經導管二尖瓣膜夾手術的評估與建議
過往許多的研究己經充份顯示在重度二尖辧膜逆流的病患,如果接受過經導管 二尖瓣膜手術後,跟傳統藥物治療的病患相比較,可大幅下降因為心臟衰竭而 再住院的比率。因此在住院醫療服務相對昂貴的國家,給付此項高價的手術可 以省下更為昂貴的住院給付,又可以讓病患得到較好的生活品質甚至回到工作 崗位,對國家生產力有所貢獻,這樣的國家保險給付政策被認為是值得且符合 成本效益的,目前世界己經全面給付此項器械的使用國家為德國和日本。然而 在國內,住院成本花費相對不是如此的昂貴,接受此項手術所產生的經濟效益 分析與德日相比較可能仍會有所差異,本篇研究雖然闡明高齡患者仍可從此項 手術當中得到臨床上功能的提升和生活品質的改善,但是我們也必須知道,台 灣國人 2016 年的平均餘命剛剛好是 80 歲,意昧著在 80 歲以上的長者做手術所 能延長的生命相對有限,這些對台灣健康保險給付的政策擬定都是需要審慎評 估的,相對高齡患者,本團隊治療了一些年輕但因為重度臟功能不良瀕臨換心 的病患,因為等待換心不及,又苦於重度瓣膜逆流而反覆心衰竭住院或甚至是 用上主動脈氣球幫浦以維生的狀況,如果接受完成功的經導管瓣膜手術,病患 不僅僅可免於反覆住院的狀況,甚至可以重返職場,成為家庭的經濟來源,給 付這樣病患所得到的經濟效益是非常巨大的,如同現行換心手術給付條件限制 在 65 歲以下病患的概念,國家健康保險給付經導管二尖瓣膜手術的政策,應可 朝向此方向進行,當然更為嚴謹的成本效益分析研究仍然是相當重要的依據。
對於而預計會在今年底發表隨機分派的臨床試驗結果的 COAPT trial
(Cardiovascular Outcomes Assessment of the MitraClip Percutaneous Therapy for Heart Failure Patients With Functional Mitral Regurgitation)將會提供更重要的臨床 實證,供各個國家在訂定相關給付政策考量依據。
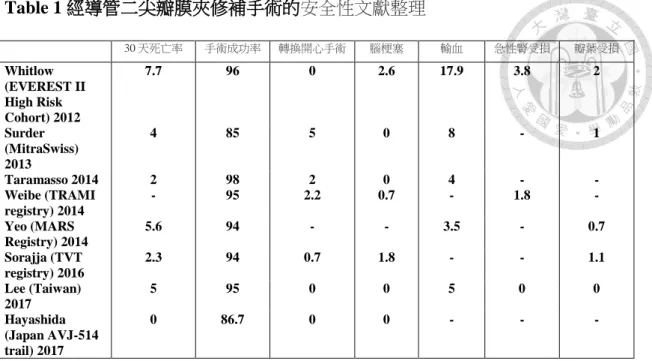
Table 1 經導管二尖瓣膜夾修補手術的安全性文獻整理
30 天死亡率 手術成功率 轉換開心手術 腦梗塞 輸血 急性腎受損 瓣葉受損 Whitlow
(EVEREST II High Risk Cohort) 2012
7.7 96 0 2.6 17.9 3.8 2
Surder (MitraSwiss) 2013
4 85 5 0 8 - 1
Taramasso 2014 2 98 2 0 4 - -
Weibe (TRAMI registry) 2014
- 95 2.2 0.7 - 1.8 -
Yeo (MARS Registry) 2014
5.6 94 - - 3.5 - 0.7
Sorajja (TVT registry) 2016
2.3 94 0.7 1.8 - - 1.1
Lee (Taiwan) 2017
5 95 0 0 5 0 0
Hayashida (Japan AVJ-514 trail) 2017
0 86.7 0 0 - - -
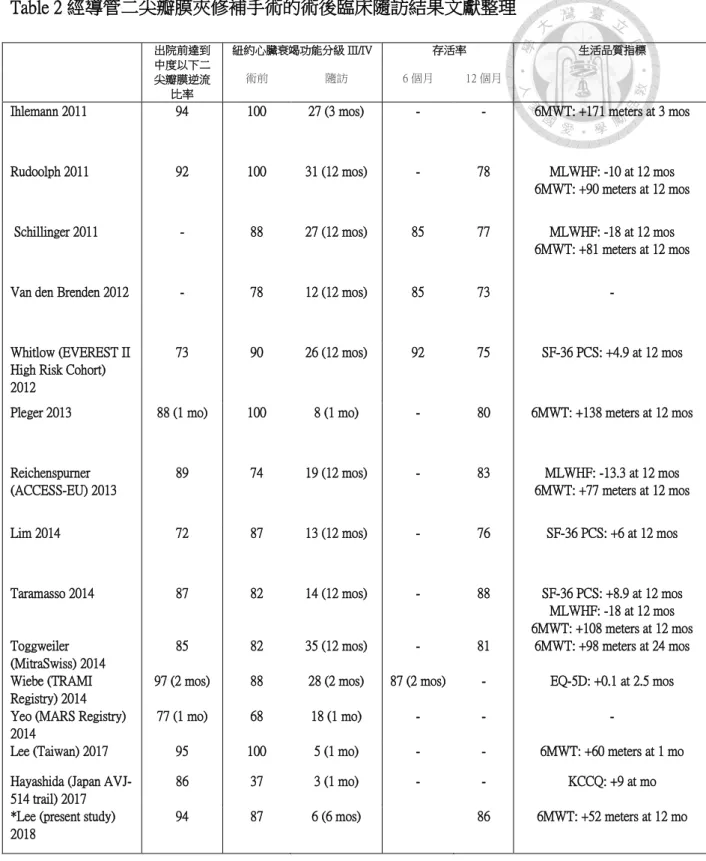
Table 2 經導管二尖瓣膜夾修補手術的術後臨床隨訪結果文獻整理
出院前達到 中度以下二 尖瓣膜逆流
比率
紐約心臟衰竭功能分級 III/IV 存活率 生活品質指標 術前 隨訪 6 個月 12 個月
Ihlemann 2011 94 100 27 (3 mos) - - 6MWT: +171 meters at 3 mos
Rudoolph 2011 92 100 31 (12 mos) - 78 MLWHF: -10 at 12 mos
6MWT: +90 meters at 12 mos
Schillinger 2011 - 88 27 (12 mos) 85 77 MLWHF: -18 at 12 mos
6MWT: +81 meters at 12 mos
Van den Brenden 2012 - 78 12 (12 mos) 85 73 -
Whitlow (EVEREST II High Risk Cohort) 2012
73 90 26 (12 mos) 92 75 SF-36 PCS: +4.9 at 12 mos
Pleger 2013 88 (1 mo) 100 8 (1 mo) - 80 6MWT: +138 meters at 12 mos
Reichenspurner (ACCESS-EU) 2013
89 74 19 (12 mos) - 83 MLWHF: -13.3 at 12 mos
6MWT: +77 meters at 12 mos
Lim 2014 72 87 13 (12 mos) - 76 SF-36 PCS: +6 at 12 mos
Taramasso 2014 87 82 14 (12 mos) - 88 SF-36 PCS: +8.9 at 12 mos
MLWHF: -18 at 12 mos 6MWT: +108 meters at 12 mos Toggweiler
(MitraSwiss) 2014
85 82 35 (12 mos) - 81 6MWT: +98 meters at 24 mos
Wiebe (TRAMI Registry) 2014
97 (2 mos) 88 28 (2 mos) 87 (2 mos) - EQ-5D: +0.1 at 2.5 mos Yeo (MARS Registry)
2014
77 (1 mo) 68 18 (1 mo) - - -
Lee (Taiwan) 2017 95 100 5 (1 mo) - - 6MWT: +60 meters at 1 mo
Hayashida (Japan AVJ- 514 trail) 2017
86 37 3 (1 mo) - - KCCQ: +9 at mo
*Lee (present study) 2018
94 87 6 (6 mos) 86 6MWT: +52 meters at 12 mo
APPENDIX 2 (INSTITUTION REVIEW BOARD DOCUMENTATION)