行政院國家科學委員會專題研究計畫成果報告
多囊性卵巢症候群與卵巢過度刺激症候群的相關研究
Polycystic Ovar y Syndr ome and Ovar ian Hyper stimulation Syndr ome
計畫編號:NSC88-2314-B-002-385
執行期限:87 年 8 月 1 日至 88 年 7 月 31 日
主持人:楊友仕 執行機構及單位名稱:台大醫學院婦產科
一、中文摘要 多囊性卵巢症候群(Polycystic ovarian syndrome, PCOS)婦女經常需要借助外在促 性腺激素的刺激以達到排卵的目的。但是 也 因 此 易 造 成 卵 巢 過 度 刺 激 症 候 群 (0varian hyperstimulation syndrome, OHSS)。造成 PCOS 婦女卵巢對外在促性 腺激素刺激過於敏感的機轉未明,可能與 cytochrome P450c17酵素有關。造成 OHSS 的真正機轉也是不完全清楚,主要是因微 血管內皮細胞通透性增加,導致大量的腹 水或胸水形成。造成炎性反應的細胞動力 素(IL-6, IL-8, TNF-α)及 vascular endothelial growth factor (VEGF)可能參與血管增生與 濾泡生成的過程。假設這些細胞動力素在 排卵前後急速增加,然後引發 OHSS 發生, 那麼在適當時機檢測這些細胞動力素,將 可用來事先預測 OHSS 的發生。本研究計 畫成果主要在討論 PCOS 經促性腺激素刺 激後,在排卵前後血清及濾泡液內的細胞 動力素的變化如何?可否用來事先預測 OHSS 的發生?與 OHSS 發生與否的相關 性又是如何?我們發現濾泡液內的 IL-6 可 事先預測 OHSS 的發生,但是排卵前後至 胚胎植入前血清內的細胞動力素(IL-6, IL-8, TNF-α及 VEGF)無法預測 OHSS 的發生。 PCOS 婦女卵巢對外在促性腺激素刺激過 於敏感的機轉,無法以排卵前後血清及濾 泡液內的細胞動力素的變化來解釋。 關鍵詞:多囊性卵巢症候群、卵巢過度刺 激症候群、細胞動力素 Abstr actSevere ovarian hyperstimulation syndrome (OHSS) is an important consideration when
PCOS patients undergoing superovulation protocols. The risk of OHSS appears to be higher in these women undergoing ovulation induction. The exact mechanism for this increased sensitivity of the polycystic ovary to exogenous gonadotropins is not clearly understood, possibly as a result of cytochrome p-450c17 dysregulation. The pathogenesis of OHSS also remains poorly understood. The underlying mechanism response for the clinical manifestations of OHSS appears to be an increase in capillary permeability of mesothelial surface with acute fluid shift out of the intravascular space. The inflammatory cytokine (IL-6, IL-8, TNF-α) and vascular endothelial growth factor (VEGF) may be involved in accelerated metabolism in the growing follicles and angiogenesis occurred in the follicles of PCOS. If changes of these cytokines begin in the peri-ovulatory period, these may be used to predict more specifically which patients with PCOS will develop OHSS. The main purpose of this study is to examine these inflammatory cytokines in plasma and follicular fluid during peri-ovulatory period and correlated with serum steroid hormone in normal and PCOS patients undergoing in-vitro fertilization (IVF) and to assess the association between serum and follicular fluid cytokines concentrations and subsequently developing severe OHSS. This study suggests that elevated levels of IL-6 in the follicular fluid at the time of oocyte retrieval may predict early stage of OHSS. However, measurements of serum IL-6, IL-8, TNF-α and VEGF between the days of hCG administration and ET are not predictive for this syndrome. The mechanism for the increased sensitivity of the polycystic ovary to exogenous gonadotropins could not be explained by changes of inflammatory
cytokines in plasma and follicular fluid during peri-ovulatory period.
Keywor ds: Polycystic ovary syndrome,
Ovarian hyperstimulation syndrome, Cytokine 二、緣由與目的 多囊性卵巢症候群(Polycystic ovarian syndrome, PCOS)婦女經常需要借助外在促 性腺激素的刺激以達到排卵的目的。但是 也因此易造成卵巢過度刺激症候群 (OHSS)。造成 PCOS 婦女卵巢對外在促性 腺激素刺激過於敏感的機轉未明,可能與 cytochrome P450c17酵素有關。造成 OHSS 的真正機轉也是不完全清楚,主要是因微 血管內皮細胞通透性增加,導致大量的腹 水或胸水形成。造成炎性反應的細胞動力 素(IL-6, IL-8, TNF-α)及 vascular endothelial growth factor (VEGF)可能參與血管增生與 濾泡生成的過程。假設這些細胞動力素在 排卵前後急速增加,然後引發 OHSS 發生, 那麼在適當時機檢測這些細胞動力素,將 可用來事先預測 OHSS 的發生。本計畫主 要目的在研究 PCOS 經促性腺激素刺激 後,在排卵前後血清及濾泡液內的細胞動 力素的變化如何?可否用來事先預測 OHSS 的發生?與 OHSS 發生與否的相關 性又是如何?瞭解以上各點將有助於瞭解 在 PCOS 婦女卵巢對外在促性腺激素刺激 過於敏感的機轉中,所佔的角色。
三、MATERIALS AND METHODS Subjects and Study Design
From September 1998 to March 1999, we recruited 156 consecutively IVF patients. The ovarian stimulation protocols were performed as previously described [1]. All patients were followed for the development of OHSS. According to the classification proposed by Galon et al. (14), 7 (4.5%) had moderate OHSS and 5 (3.2%) had severe OHSS. The study group comprised 12 patients who
developed early-form moderate (n = 7) or severe (n = 5) OHSS required hospitalization. The two control groups comprised randomized selection of 12 high-risk women and 12 matched low-risk women in whom OHSS did not develop.In all patients, peripheral venous blood was drawn in the morning on the days of hCG administration, oocyte retrieval, and ET. During oocyte retrieval, clear follicular fluid from individual follicles of ≥ 18 mm was collected and pooled in each patient. The follicular fluid was centrifuged immediately (2,000 × g), and the
supernatant was stored, together with the serum samples, at -70°C before assay for cytokines and steroids.
Cytokines and hor mones assay
Levels of IL-6, IL-8 and TNF-α in serum and follicular fluid were measured with a solid-phase chemiluminescent enzyme immunoassay system (Immulite; Diagnostic Products Corporation, Los Angeles, CA). Serum and follicular VEGF concentrations were quantitated using an ELISA (Quantikine; R&D System, Inc., Minneapolis, MN). Serum and follicular fluid E2 and progesterone
concentrations were assayed using a chemiluminescent immunoassay (Immulite; Diagnostic Products Corporation).
四、RESULTS(結果)
The clinical and laboratory data in the study and the two control groups are presented in Table 1. There are more patients with PCOS in study group than that in the two control groups.
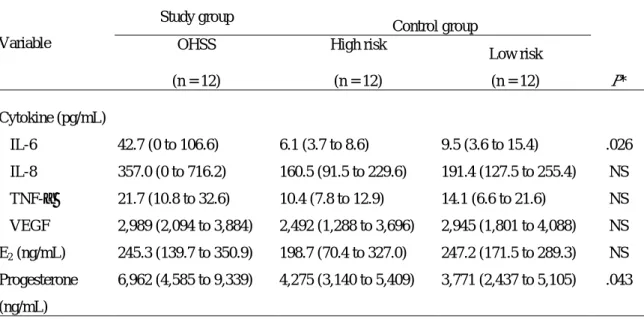
Follicular fluid concentrations of IL-6 as well as P (Table 2) were significantly higher in the OHSS group than in the two control groups. Follicular fluid levels of IL-8, TNF-α, VEGF, and E2 showed no statistically
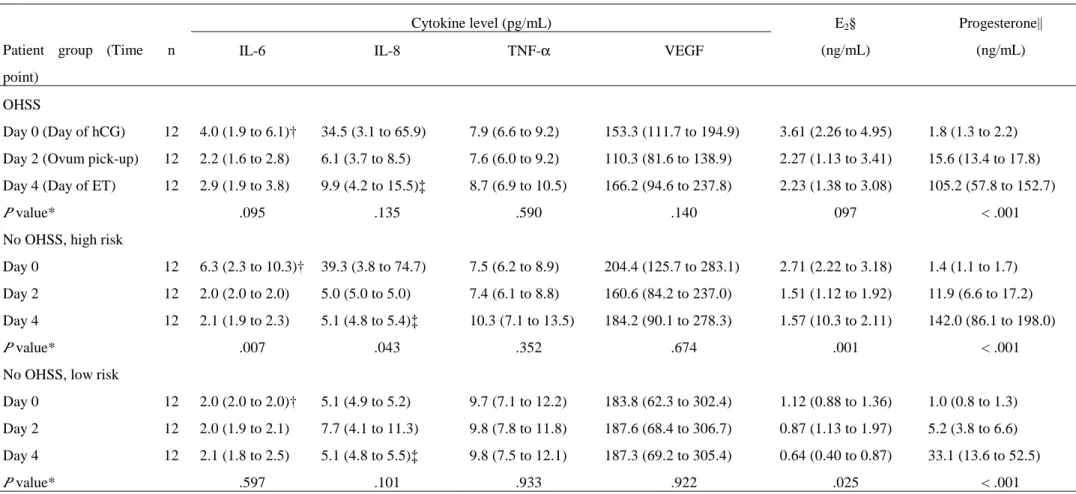
significant difference among the three groups. Table 3 shows changes in serum levels of cytokine profile and steroids on the days of hCG administration, oocyte retrieval, and ET.
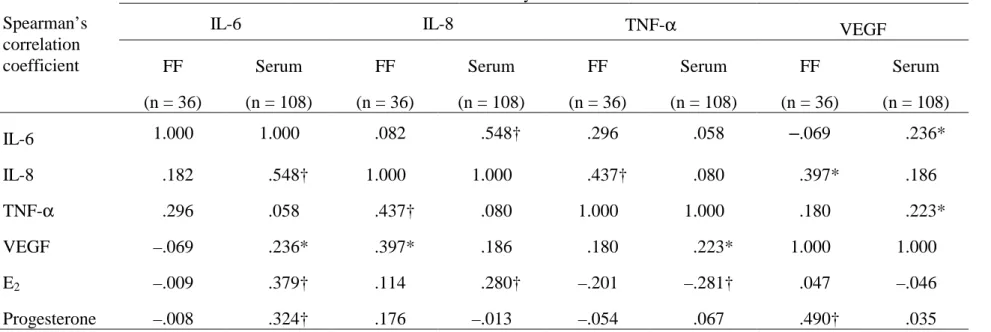
levels with steroid concentrations in serum and follicular fluid.
五、DISCUSSION(討論)
The unique feature of our study is that we assessed multiple relevant cytokines in serum and follicular fluid simultaneously in patients who subsequently developed OHSS and matched controls who did not. We also examine the possible role of serial measurement of these mediators between the day of hCG administration and the day of ET in the prediction of OHSS. We found that only follicular fluid IL-6 levels at the time of oocyte retrieval can serve as an early predictor for the development of OHSS. We further expanded on the assay of circulating cytokines by showing that serum levels of IL-6 between the day of hCG administration and the day of ET are not predictive for this syndrome. This suggests the ovary may be the main resource of mediators that work as the initiators of the changes and lead to the full appearance of OHSS.
Our findings are concomitant with those of Krasnow et al. and Geve et al., who reported no difference in follicular fluid VEGF levels was detected between OHSS and controls. Based on our work and previous reports, circulating VEGF levels between the day of hCG administration and the day of ET do not appear to be a good marker or predictor of OHSS.
Our data illustrated the minimal cytokine variability in serum between the day of hCG administration and the day of ET. Therefore, it is unlikely that serum concentrations of these cytokines during this period could serve as early predictors for the development of OHSS. Moreover, the mechanism for the increased sensitivity of the polycystic ovary to exogenous gonadotropins could not be explained by changes of inflammatory cytokines in plasma and follicular fluid during peri-ovulatory period.
六、參考文獻
1. Chen CD, Wu MY, Chen HF, Chen SU, Ho HN, Yang YS. Prognostic importance of serial cytokine changes in ascites and pleural effusion in women with severe ovarian hyperstimulation syndrome. Fertil Steril 1999:72:286-92. 七、計畫成果自評 本研究計畫新發現濾泡液內的 IL-6 可 事先預測 OHSS 的發生,但是排卵前後至 胚胎植入前血清內的細胞動力素(IL-6, IL-8, TNF-α及 VEGF)無法預測 OHSS 的發生。 卵巢過度刺激症候群病人是否為多囊性卵 巢病人並不影響血清及濾泡液內的細胞動 力素濃度的變化。PCOS 婦女卵巢對外在促 性腺激素刺激過於敏感的機轉,無法以排 卵前後血清及濾泡液內的細胞動力素的變 化來解釋。我們找到相關預測指標,能夠 比較準確預測卵巢過度刺激症候群的發 生。有助於降低發生率。研究成果達成預 期目標,極具臨床應用價值。
八、表格
Table 1 Clinical and laboratory data in the study and control groups
Study group Control group
OHSS High risk Low risk
Variable (n = 12) (n = 12) (n = 12)
No. of patients with PCOS (%) 7 (58.3) 3 (25.0) 1 (8.3)*
Age (y) 30.9 ± 4.8 33.7 ± 2.8 34.0 ± 6.2
No. of hMG ampules 23.5 ± 9.6 18.3 ± 5.7 19.0 ± 5.1 E2 level on day of hCG
administration (pg/mL)
3,607 ± 2,121 2,705 ± 757 1,117 ± 375*
No. of oocytes retrieved 23.4 ± 9.1 16.5 ± 8.8 7.1 ± 3.9* No. of embryos transferred 5.3 ± 1.1 4.8 ± 1.1 3.7 ± 1.7*
Clinical pregnancy (%)† 8 (75) 4 (25) 4 (25)
Note: Values are means ± SD unless otherwise indicated. OHSS = ovarian hyperstimulation syndrome; PCOS = polycystic ovary syndrome.
* P < .05 (versus study group).
† No of patients who became pregnant (%).
Table 2 Follicular fluid concentrations of various cytokines and steroid hormones in the study and control groups
Study group
Control group
OHSS High risk
Low risk Variable (n = 12) (n = 12) (n = 12) P* Cytokine (pg/mL) IL-6 42.7 (0 to 106.6) 6.1 (3.7 to 8.6) 9.5 (3.6 to 15.4) .026 IL-8 357.0 (0 to 716.2) 160.5 (91.5 to 229.6) 191.4 (127.5 to 255.4) NS TNF-α 21.7 (10.8 to 32.6) 10.4 (7.8 to 12.9) 14.1 (6.6 to 21.6) NS VEGF 2,989 (2,094 to 3,884) 2,492 (1,288 to 3,696) 2,945 (1,801 to 4,088) NS E2 (ng/mL) 245.3 (139.7 to 350.9) 198.7 (70.4 to 327.0) 247.2 (171.5 to 289.3) NS Progesterone (ng/mL) 6,962 (4,585 to 9,339) 4,275 (3,140 to 5,409) 3,771 (2,437 to 5,105) .043
Note: Values are means (95% confidence intervals) unless otherwise indicated. * Determined by Kruskal-Wallis test.
Table 3 Changes in serum levels of various cytokines and steroids on the days of hCG administration, oocyte retrieval, and embryo transfer.
Cytokine level (pg/mL) Patient group (Time
point)
n IL-6 IL-8 TNF-α VEGF
E2§ (ng/mL) Progesterone|| (ng/mL) OHSS Day 0 (Day of hCG) 12 4.0 (1.9 to 6.1)† 34.5 (3.1 to 65.9) 7.9 (6.6 to 9.2) 153.3 (111.7 to 194.9) 3.61 (2.26 to 4.95) 1.8 (1.3 to 2.2) Day 2 (Ovum pick-up) 12 2.2 (1.6 to 2.8) 6.1 (3.7 to 8.5) 7.6 (6.0 to 9.2) 110.3 (81.6 to 138.9) 2.27 (1.13 to 3.41) 15.6 (13.4 to 17.8) Day 4 (Day of ET) 12 2.9 (1.9 to 3.8) 9.9 (4.2 to 15.5)‡ 8.7 (6.9 to 10.5) 166.2 (94.6 to 237.8) 2.23 (1.38 to 3.08) 105.2 (57.8 to 152.7)
P value* .095 .135 .590 .140 097 < .001
No OHSS, high risk
Day 0 12 6.3 (2.3 to 10.3)† 39.3 (3.8 to 74.7) 7.5 (6.2 to 8.9) 204.4 (125.7 to 283.1) 2.71 (2.22 to 3.18) 1.4 (1.1 to 1.7) Day 2 12 2.0 (2.0 to 2.0) 5.0 (5.0 to 5.0) 7.4 (6.1 to 8.8) 160.6 (84.2 to 237.0) 1.51 (1.12 to 1.92) 11.9 (6.6 to 17.2) Day 4 12 2.1 (1.9 to 2.3) 5.1 (4.8 to 5.4)‡ 10.3 (7.1 to 13.5) 184.2 (90.1 to 278.3) 1.57 (10.3 to 2.11) 142.0 (86.1 to 198.0)
P value* .007 .043 .352 .674 .001 < .001
No OHSS, low risk
Day 0 12 2.0 (2.0 to 2.0)† 5.1 (4.9 to 5.2) 9.7 (7.1 to 12.2) 183.8 (62.3 to 302.4) 1.12 (0.88 to 1.36) 1.0 (0.8 to 1.3) Day 2 12 2.0 (1.9 to 2.1) 7.7 (4.1 to 11.3) 9.8 (7.8 to 11.8) 187.6 (68.4 to 306.7) 0.87 (1.13 to 1.97) 5.2 (3.8 to 6.6) Day 4 12 2.1 (1.8 to 2.5) 5.1 (4.8 to 5.5)‡ 9.8 (7.5 to 12.1) 187.3 (69.2 to 305.4) 0.64 (0.40 to 0.87) 33.1 (13.6 to 52.5)
P value* .597 .101 .933 .922 .025 < .001
Note: Values are means (95% confidence intervals) unless otherwise indicated. IL = Interleukin; TNF = tumor necrosis factor; VEGF = vascular endothelial growth factor; OHSS = ovarian hyperstimulation syndrome.
* Determined by Kruskal-Wallis test. †P = .015 by Kruskal-Wallis test. ‡P = .017 by Kruskal-Wallis test.
§ P < .05 among the groups at each time-point, Kruskal-Wallis test. || P < .05 among the groups at each time-point, Kruskal-Wallis test.
Table 4 Correlations of cytokine levels in serum and follicular fluid with steroid levels.
Cytokine
IL-6 IL-8 TNF-α VEGF
Spearman’s correlation coefficient FF (n = 36) Serum (n = 108) FF (n = 36) Serum (n = 108) FF (n = 36) Serum (n = 108) FF (n = 36) Serum (n = 108) IL-6 1.000 1.000 .082 .548† .296 .058 –.069 .236* IL-8 .182 .548† 1.000 1.000 .437† .080 .397* .186 TNF-α .296 .058 .437† .080 1.000 1.000 .180 .223* VEGF –.069 .236* .397* .186 .180 .223* 1.000 1.000 E2 –.009 .379† .114 .280† –.201 –.281† .047 –.046 Progesterone –.008 .324† .176 –.013 –.054 .067 .490† .035
* Correlation was significant at the 0.05 level (2-tailed). FF = follicular fluid; IL = Interleukin; TNF = tumor necrosis factor; VEGF = vascular endothelial growth factor.