國家科學委員會專題研究計劃
題目
Car vedilol 與數種植物粹取成份對雜種狗慢性心臟衰
竭之治療功效:頻脈性與缺血性心臟衰竭模式之比較
Global Cardiac Therapeutic Effect of Carvedilol and
Several Plant-Principle Pharmaceutics on Chronic
Congestive Heart Failure: Comparison between Rapid
Ventricular Pacing and Microsphere Ischemia Models in
Dogs
(NSC 88-2314-B-002-122-M48)
主持人:臺大醫學院 內科
林俊立 副教授
共同主持人:臺大醫學院 臨床醫學研究所
黃水坤 教授
Introduction
Chronic congestive heart failure is the common end of many cardiovascular diseases (1), including coronary arterial, valvular, cardiomyopathic, congenital, inflammatory mechanisms. The decompensation of active myocardial contractile performance leads to the congestion of blood flow in the lungs, visceral organs and extremities, and finally the death of the victims. Appropriate pharmacological correction of the progressive cardiac malfunction remains insatisfactory, although some good news has been emerging, e.g. the angiotensinconverting enzyme inhibitor (2) and β -blockers (3, 4, 5).
In our 3-year project of the pursuit of new plant-principle therapeutics for the treatment of chronic congestive heart failure, we attempted to set up an animal model of chronic congestive heart failure and delineate the cellular, ion channel and molecular levels of myocardial dysfunction and the effects of various promising drugs. In the first year, we have been successful in establishing the canine model of chronic congestive heart failure by the implantation of ventricular overdrive pacing pacemakers, and tests the influence of well-accepted carvedilol in the treatment of the congestive heart failure. Meanwhile, the ischemic model of heart failure by coronary microsphere embolization was given up due to the great reduction of the program funding.
Mater ials and Methods
Canine model of congestive hear t failur e
Because of the shortage of budget, the initial idea of comparing two distinct canine heart failure models, i.e. pacing heart failure vs. coronary occlusion heart failure, was forced to be given up. We tested the model of ventricular overdrive pacing-induced congestive heart failure in a series of dogs with or without the use of carvedilol.
Four groups of mongrel dogs were enrolled consecutively in the first year of the study, i.e. the pacing only group (Group A-1), the pacing plus carvedilol group (Group A-2), the sham group (Group B-1) and the sham plus carvedilol group (Group B-2). All the animals were implanted with an artificial
pacemaker, only that the sham group had the pacemaker shut off. All the pacing group animals were paced from right ventricular apex at a rate of 3.9 Hz (234 ppm) by a commercially available high-speed pacemaker (Itrel-3, Medtronic, Minneapolis, USA).
After taking baseline echocardiography study, all the dogs were anesthesized by intravenous pentobarbital, and intubated for controlled ventilation by Harvard respirator. The right-sided (or less commonly, left-sided) internal jugular vein was percutaneously punctured and inserted the screw-in or tin-tipped ventricular pacing lead (Medtronic or Intermedics). When the pacing lead was positioned at the apex of right ventricle under fluoroscopy, the pacing threshold, local signal amplitude and slew rate were tested by external programmer. The pacing threshold was taken as acceptable when less than 1 volt, and the pacing impedance less than 1000 ohms. Then, pacing function was initiated. The generator was tunneled and located on the back of the neck of the animal.
Monitor ing of car diac function by echocar diogr aphy.
The animals were followed up by transthoracic echocardiography every 2 weeks. After mild anesthesia by low-dose pentobarbital, the animal was put on left decubitus position to study cardiac echocardiography. The dimensions of all 4 cardiac chambers were evaluated in 4-chamber view, longitudinal and short-axis views. Left atrial, left ventricular and (if possible) right ventricular dimensions, as well as interventricular septum and left ventricular posterior wall thickness were measured and left ventricular fractional shortening and ejection fraction were calculated.
Hemodynamics, Electr ophysiology and pathological study
After 6-8 weeks of continuous pacing, all the pacing group animals demonstrated the clinical evidences of chronic congestive heart failure including 4-chamber dilatation of the heart, markedly diminished cardiac contractility and even ascites of the animals.
All the animals were then re-anesthetized by pentobarbital and reintubated for controlled ventilation. Using Seldinger technique, femoral artery was cannulated and inserted the Millar micromanometer-tipped catheter. Aortic
pressure, left ventricular pressure and the first derivative of pressure vs. time (dp/dt) were accurately measured with the Millar catheter. The right thoracotomy was started and the pericardium was opened. Cardiac electrophysiology study focusing on the induction of atrial tachyarrhythmias was conducted from both right and left atrial epicardial surface by a deflectible quadripolar catheters (Mansfield).
After the study, the heart was immediately removed and weighed. The heart was quickly perfused with oxygen-rich Tyrode solution, and cut into multiple pieces for detailed basic studies for all 4 cardiac chambers, including action potential provocation, ion channels of single cell, and various calcium or other-handling proteins.
Results
Canine congestive hear t failur e model
The implantation of high-speed artificial pacemaker has been smooth for the whole 21 mongrel dogs in the first year. The dislodgment of the pacing lead is few, being 1 in the 21 animals. However, the destruction of the pacing lead, or even the pacemaker, has been not uncommon, being in 5 of the 21 animals. The destruction of pacing device is , without exception, the result of scratch laceration of the suture wound by the animals.
The animals were separated into 4 groups, i.e. pacing only (8 dogs, Group A-1), pacing plus carvedilol (6 dogs, Group A-2), sham only (2 dogs, Group B-1) and sham plus carvedilol (5 dogs, Group B-2), according to the use or not of high-speed pacemaker or carvedilol. Over all, the number of dogs died suddenly before the final study was 5 (2 died immediately after anesthesia in the final study) in the Group A-1, 2 (1 died suddenly in anesthesia) in the Group A-2 and none in both sham groups (Group B-1, B-2).
E volu t ion of ca r d ia c con t r a ct ile p er for ma n ce in ca n in e con gest ive h ea r t fa ilu r e m od el
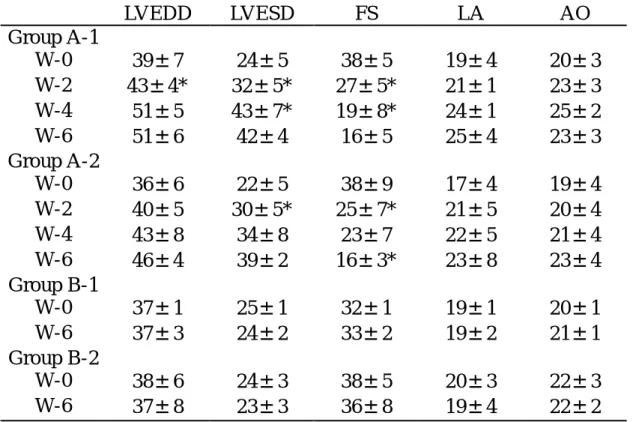
As shown in tableⅠ , the left ventricular diastolic and end-systolic dimensions increased rapidly and progressively in Group A-1.
Reflecting the change in cardiac chamber size, the left ventricular fractional shortening depressed rapidly as well. For Group A-2 animals, the dilatation of the left ventricular chambers and the depression of left ventricular contractility (fractional shortening) kept plateaued between the second and the fourth week before further deterioration. The sham group animals (Group B-1, B-2) had no change of the left ventricular size or dimensions over the 6-8 weeks of observation.
I n d u ct ion of a t r ia l t a ch ya r r h yt h m ia s in con gest ive h ea r t fa ilu r e
The inducibility of nonsustained or sustained atrial tachyarrhythmias has been evenly distributed in pacing and sham group animals: 1 in Group A-1, 1 in Group A-2, 1 in Group B-1, and 2 in Group B-2. The lack of inducible atrial fibrillation in our study is believed to be related to the relatively small animal weight. The mean animal body weight was 153 kg, ranging 10 kg to 26 kg, in the present study.
Discussion
In the first year of the integrated study project, we have demonstrated the reliable stability of creating congestive heart failure by ventricular overdrive pacing at a rate of 3.9 Hz (234 ppm). The dilatation of the cardiac chambers and the depression of cardiac contractile performance became manifest from the second week of continuous pacing on, and deteriorated steadily. The risk of sudden cardiac death was likewise apparent in the overdrive pacing group of animals without the use of carvedilol. However, the inducibility of atrial tachyarrhythmias was not different between pacing and non-pacing animals in the present study.
An im a l m od els of con gest ive h ea r t fa ilu r e
There are multiple animal models suitable for the study of congestive heart failure, including dilated cardiomyopathy by microsphere embolization, pacing tachycardia cardiomyopathy, ischemic congestive heart failure by proximal coronary artery ligation. In the present study, we successfully reproduced the animal model of tachycardia cardiomyopathy by ventricular overdrive pacing in the dogs
(6,7). The cardiac chambers dilated progressively and the cardiac performance deteriorated rapidly within 6 weeks. The risk of sudden cardiac death is high within 6 weeks in the present study. The unusual high unexpected death is at least partly related to the unqualified health status of the mongrel dogs available in Taipei. The frequent inadequate body weight (mostly under 20 kg, not to say 30 kg) and frequent contamination of canine filariasis are the two main factors for the poor condition of the dogs undergoing continuous pacing protocol. The source of healthy, large mongrel dogs is unpredictable in Taipei, or even in the whole Taiwan.
T h e effect of ca r ved ilol in t h e evolu t ion of con gest ive h ea r t fa ilu r e
Carvedilol is a combined beta-and alpha-blocker. Recent clinical large-scale studies have proved the efficacy of carvedilol in the improvement of mild, moderate to advanced congestive heart failure in humans(3, 4, 5, 8, 9). More over, carvedilol has been proved to be effective in reducing the risk of sudden cardiac death (5), which is not seen in previous trials using angiotensin-converting enzyme inhibitors (2). Similar improvement in both total mortality and sudden cardiac death in the treatment of congestive heart failure is reported in another beta-blocker trial using long-acting metoprolol. Nevertheless, the therapeutic benefit of carvedilol has also been claimed to be related to its antioxidant or radical scavenger effects (10, 11).
In our study, the pacing group supplemented with carvedilol is proved to be slurred in the progression of congestive heart failure. The number of dogs died suddenly is also less in the Group A-2 compared to that in the Group A-1. However, the benefit is not evident. This could be attributed to the number of the animals undergoing the study and the generally improper health condition of the dogs. Further detailed studies in terms of myocyte action potential, muscle tension, and channel/receptor change would be helpful in elucidation of the carvedilol effects.
P r ovoca t ion of a t r ia l t a ch ya r r h yt h mia in con gest ive h ea r t fa ilu r e
Several animal studies have proved that the incidence and inducibility of atrial fibrillation in dogs with pacing-induced congestive heart failure is high. The electrophysiologic mechanism is postulated to
be the combination of atrial stretch and macroreentrant circuits.
In our study, the propensity of atrial fibrillation is not demonstrated by a similar dog model. The main factor, we believed, is the small size of mongrel dogs in Taipei. Atrial fibrillation is a dysrhythmia dependent very much on the atrial mass. The more the atrial mass, e.g. that in humans or even larger animals, the more the risk of atrial fibrillation. For the creation of sustained atrial fibrillation, we have to use the pig, instead of mongrel dogs, according to previous experience. The low incidence of atrial fibrillation in own pacing dogs is most likely the result of small atrial mass. Our dog model is not suitable for the study of atrial fibrillation in congestive heart failure.
C on clu sion s.
We have successfully established the chronic canine model of congestive heart failure by continuous ventricular overdrive pacing for 6 weeks. The efficacy of carvedilol is emerging, but not proved definitely due to the limited animal number. However, the unpredictable quality of the mongrel dog source is a long-term problem and threat to the study.
Refer ences
1. Kanel WB: Epidemiological aspects of heart failure. Cardiol Clin 1989; 7: 1-9.
2. The CONSENSUS Trial Study Group. Effects of enalapril on mortality in severe congestive heart failure: results of the Cooperative North Scandinavian Enalapril Survival Study (CONSENSUS). N Engl J Med 1987; 316: 1429-1435.
3. Packer M, Colucci WS, Sackner-Bernstein JD, Liang CS, Glodscher DA, Freeman I, Gottlieb SS, Pearle D, Cody RJ, Gregory JJ, Kantrowitz NE, Le Jemtel TH, Young ST, Lukas MA, Shusterman NH, for the PRECISE Study Group. Double-blind, placebo-controlled study of the effects of carvedilol in patients with moderate to severe heart failure: the PRECISE trial. Circulation 1996; 94: 2793-2799. 4. Bristow MR, Gilbert EM, Abraham WT, Adams KF, Fowler MB,
Young S, Shusterman N, for the MOCHA Investigators. Carvedilol produces dose-related improvements in left ventricular function and survival in subjects with chronic heart failure. Circulation 1996; 94: 2807-2816.
5. MERIT-CHF Study Group. Effect of metoprolol CR/XL in chronic heart failure: metoprolol CR/XL randomized intervention trial in congestive heart failure (MERIT-HF). Lancet 1999; 353: 2001-2007. 6. Wilson JR, Douglas P, Hickey WF. Experimental congestive heart
failure produced by rapid ventricular pacing in the dog: cardiac effects. Circulation 1987; 75: 857-867.
7. Armstrong PW, Stopps TP, Ford SE, DeBlod AJ. Rapid ventricular pacing in the dog: pathophysiologic studies of heart failure. Circulation 1986; 74: 1075-1084.
8. Bristow MR, Ginsburg R, Minobe WA, Cubiccioti RS, Sageman WS, Lurie K, Billingham ME, Harrison DC, Stinson EB. Decreased catecholamine sensitivity and β -adrenergic receptor sensitivity in failing human hearts. N Engl J Med 1992; 307: 205-211.
9. Cohn JN, Levine TB, Olivari MT, Garberg V, Leura D, Francis GS, Simon AB, Rector T. Plasma norepinephrine as a guide to prognosis in patients with chronic congestive heart failure. N Engl J Med 1984; 311: 819-823.
10. Mann DL, Kent RL, Parsons B, Cooper G Ⅳ. Adrenergic effects on the biology of the adult mammalian cardiocyte. Circulation 1992; 85: 790-804.
11. Ye TL, Cheng HY, Lysko PG, McKenna PJ, Feurstein R, Gu JL, Lesko KA, Davis LL, Feuerstein G. Carvedilol, a new vasodilatior and beta-adrenoceptor antagonist, is an antioxidant and free radical scavenger. J Pharmacol Exp Ther 1992; 263: 92-98.
Table 1. The evolution of cardiac chamber dimensions and cardiac contractile performance in canine congestive heart failure produced by rapid ventricular pacing.
LVEDD LVESD FS LA AO Group A-1 W-0 39±7 24±5 38±5 19±4 20±3 W-2 43±4* 32±5* 27±5* 21±1 23±3 W-4 51±5 43±7* 19±8* 24±1 25±2 W-6 51±6 42±4 16±5 25±4 23±3 Group A-2 W-0 36±6 22±5 38±9 17±4 19±4 W-2 40±5 30±5* 25±7* 21±5 20±4 W-4 43±8 34±8 23±7 22±5 21±4 W-6 46±4 39±2 16±3* 23±8 23±4 Group B-1 W-0 37±1 25±1 32±1 19±1 20±1 W-6 37±3 24±2 33±2 19±2 21±1 Group B-2 W-0 38±6 24±3 38±5 20±3 22±3 W-6 37±8 23±3 36±8 19±4 22±2 AO, aorta size; FS, fractional shortening; LA, left atrial dimension; LVEDD, LVESD, left ventricle end-diastolic, end-systolic dimensions; Group A-1, A-2, B-1, B-2, as described in Text; All cardiac chamber dimensions are measured by M-mode echocardiography, in mm. W-0, -2, -4, -6, 0, 2, 4, 6 weeks after the start of pacing or sham study. Q, P<0.05 of W-2 vs. W-0, W-4 vs. W-2, W-6 vs. W-4.