電子健康照護服務中溝通對於支援程序與員工服務品質之間關係的影響 - 政大學術集成
47
0
0
全文
(2) The Impact of Communication on the Relationship between Support Process and Employee Service Quality in the Context of e-Health. ABSTRCT. In the information society, electronic healthcare service (e-health), the new concept of medical treatment has been introduced to improve health and healthcare. In order to let the service process more efficiently and improve the performance of whole service delivery system, we discuss about the internal of the delivery system. The main topic of this study is to investigate the e-health care delivery service. We make the interview with doctors, IT staffs and healthcare staffs, and then we find out the delivery system can divide into three parts: 1. staff training, 2. intra-organization communication, 3. service process. Our research framework is based on part of service blueprinting, discussing the interaction between each components of our research framework. Later, we join communication into intra-organization to discuss whether a good communication between intra-organizations can contribute to higher levels of employee service quality or not, and we get a positive conclusion. Through our analysis, we find out that the communication would be the most important factor in delivery service including diagonal communication, upward communication, downward communication and horizontal communication in the organization. Finally, we hope our study and finding can lead the e-health service delivery system more efficient and come to maturity.. 立. 政 治 大. ‧. ‧ 國. 學. n. er. io. sit. y. Nat. al. Ch. engchi. i Un. v. Keywords: e-Health, Delivery, Service Blueprinting, Training, Communication.. i.
(3) CONTENT CHAPTER 1: INTRODUCTION ...................................................................... 1 CHAPTER 2: LITERATURE REVIEW .......................................................... 3 2.1 Service blueprinting ..................................................................................... 3 2.2 Support processes in the service delivery system ........................................ 4 2.2.1 IT Support processes ....................................................................................... 4 2.2.2 Training support processes .............................................................................. 5 2.3 Communication in service delivery systems................................................ 5 2.4 Summary ...................................................................................................... 6. CHAPTER 3: DEVELOPMENT OF RESEARCH FRAMEWORK ............ 8. 政 治 大. 3.1 Research Framework ................................................................................... 8 3.2 Support Processes ........................................................................................ 8. 立. 3.2.1 IT Support Process .......................................................................................... 8. ‧ 國. 學. 3.2.2 Training Support Process ................................................................................ 9. ‧. 3.3 Communication ............................................................................................ 9 3.3.1 Diagonal Communication.............................................................................. 10 3.3.2 Upward Communication ............................................................................... 10 3.3.3 Downward Communication........................................................................... 11 3.3.4 Horizontal Communication ........................................................................... 11. sit. y. Nat. n. al. er. io. CHAPTER 4: RESEARCH ANALYSIS ........................................................ 12. i Un. v. 4.1 Research Methodology .............................................................................. 12 4.1.1 Data Collection .............................................................................................. 12 4.2 Research Analysis ...................................................................................... 14 4.2.1 Case Background ........................................................................................... 14 4.2.2 Framework Application ................................................................................. 15. Ch. engchi. CHAPTER 5: DISCUSSION ........................................................................... 22 5.1 Cross-Case Analysis Results ...................................................................... 22 5.1.1 Impact of diagonal communication on IT support ........................................ 23 5.1.2 Impact of other communications on training support .................................... 24. 5.2 Managerial Implications ............................................................................ 25. CHAPTER 6: CONCLUSION ......................................................................... 27 6.1 Summary .................................................................................................... 27 6.2 Limitations and Implications of Future Research ...................................... 27 ii.
(4) REFERENCE .................................................................................................... 29 Appendix A: Question List of the Group Interview (Chinese) ..................... 32 Appendix B: Interview Contents and Framework Application (Chinese) .. 33. 立. 政 治 大. ‧. ‧ 國. 學. n. er. io. sit. y. Nat. al. Ch. engchi. iii. i Un. v.
(5) TABLES & FIGURES Figure 3-1: Research Framework……………………………………….………..8 Figure 4-1: Research Roadmap……………..…………………….…………….12 Table 4-1: Validities and reliability tests………………………………………....13 Table 4-2: Cross-case analysis………………………………………….……….21 Figure 5-1: Summary of case analysis………………………………….………22. 立. 政 治 大. ‧. ‧ 國. 學. n. er. io. sit. y. Nat. al. Ch. engchi. iv. i Un. v.
(6) CHAPTER 1: INTRODUCTION In today‘s rapidly globalizing information society, electronic healthcare services (e-health), a new generation of medical information and communication technologies, have been introduced to improve modern day healthcare (Spil and Schuring, 2006). E-health is a consumer-centered model of healthcare where stakeholders collaborate to arrange, deliver, and manage healthcare, through emerging information technologies (IT) and the Internet (Eysenbach G., 2001). The scope of healthcare delivery is broadened by e-health. Traditionally, the center of health has always been the hospital; when debilitated, patients would have to go to the hospital for disease diagnosis and treatment. E-Health, however, changes traditional healthcare delivery by placing the patients at the center of services. Through Internet and wireless technologies, healthcare can be delivered to the patients anytime at anyplace (Silber, 2003; Wilson, Leitner, & Moussalli, 2004).. 政 治 大. The e-Health delivery system is designed to improve the quality, availability, and effectiveness of healthcare. It often focuses on providing tele-monitoring and tele-consultation to remote elderly patients or patients with chronic diseases at home. The system can also offer help in the management of care, the preparation of care plans, and the coordination of actions and tasks taken by members of care teams (Spil and Schuring, 2006).. 立. ‧. ‧ 國. 學. er. io. sit. y. Nat. However, while the e-Health delivery system continues to help us in many ways through its variety of services, there are still many challenges which we have to overcome. Spil and Schuring (2006) suggest that the following recommendations will help organizations improve the performance of e-health systems. These include:. al. n. iv n C Meaningful collaboration with recipients. U h ehealthcare i h n c g Efficient strategies and techniques to monitor patterns of internet use among. . consumers. Preparation for upcoming technological developments. Balancing connectivity and privacy. Better understanding the balance between face-to-face and virtual interactions. Equitable access to technology and information across the globe.. The performance of e-Health is greatly affected by the design of service delivery. Inadequate service deliveries (i.e. unstable monitoring devices), may lead doctors to propose erroneous diagnoses. Harnett (2004) has mentioned several aspects of service delivery that providers should take into account: bandwidth, availability, latency, security, and ubiquity. To improve efficiency, Graschew (2008) also emphasized the importance of integrating all the services into one delivery platform. Beyond these, there are several other aspects of the system that could use improvement, including the functionality, usability, reliability, performance, and scalability of service delivery 1.
(7) system (Shelman 2008). While most studies discuss the influence of only the IT factors on e-Health delivery, some have included non-IT factors, such as staff training (Rowe, Savigny, Lanata and Victora, 2005) and the communication between service providers (Spil and Schuring 2006); while not as obvious, these factors likewise have a direct influence on the performance of e-health delivery and may be contributing causes to the success or failure of these systems. Past literature has put much focus on factors affecting the systems‘ performance, such as integrated ability (Graschew, Roelofs, Rakowsky and Schlag, 2008) and functionality; and, unfortunately, less on patient satisfaction and employee internal performance (Spil and Schuring 2006). We believe that there is a need to consider both IT and non-IT factors of e-Health service delivery design. Patient satisfaction, training lessons for employees and communication between employees are all the important factors that may affect the performance of e-Health delivery and cannot be neglected (Rowe, Savigny, Lanata and Victora, 2005).. 政 治 大. Bitner et al. (2008) have suggested a practical technique for service innovation known as ―Service Blueprinting‖, a method for viewing internal service processes. A typical service blueprint includes five components: customer actions, onstage/visible contact employee actions, backstage/invisible contact employee actions, support processes, and physical evidence. These key components provide an overview so that employees and internal units can relate what they do to the entire, integrated service system (Gummesson and Brundage, 1991). While past literature on healthcare service delivery has put much focus on the systems‘ external performance in terms of integrated ability (Graschew, Roelofs, Rakowsky and Schlag, 2008), function, and patient satisfaction, few studies focus on internal service qualities, such asemployee performance (Spil and Schuring 2006). Therefore, our research aims to use service blueprinting to discuss both the IT and non-IT factors that impact the internal performance of e-health service delivery systems;we argue that these factors will not only affect the internal service performance of e-Health delivery, but the external service performance in terms of patient‘s satisfaction, as well (Rowe, Savigny, Lanata and Victora, 2005). Our research questions are summarized as follows:. 立. ‧. ‧ 國. 學. n. er. io. sit. y. Nat. al. Ch. engchi. i Un. v. 1. What kind of support processes will allow healthcare staff to provide good service quality? 2. What kind of intra-communication can moderate the relationship between support process and the employees‘ service quality? 3. Does healthcare staff service quality affect patient action?. 2.
(8) CHAPTER 2: LITERATURE REVIEW We first will apply the service blueprinting concept to find out what factors influence the quality of e-Health service delivery. Since internal operational factors serve as the foundation for service delivery quality, we will also include literature relevant to these topics in our discussion of service blueprinting below.. 2.1 Service blueprinting Service blueprinting is a very versatile technique that can be used for both innovation and service improvement. It may well be the best method for measuring service success and may also hold the key to future service innovations (Bitner, Ostrom and Morgan, 2008). Service blueprints can be described as service roadmaps -- tangible, visual documents that lay out where and how customers and companies interact. More specifically, blueprints are information-laden documents made up of five components that, when drawn up together, can help make the customer-company relationship and customer experience clear (W.P. Carey, 2008). The five components of a typical service blueprints are as follows:. 立. 政 治 大. ‧ 國. 學. ‧. Customer actions: include all of the steps that customers take as part of the service delivery process. Onstage/visible contact employee actions: the actions of frontline contact employees that occur as part of face-to-face encounters with customers. Backstage/visible contact employee actions: non-visible interactions with customers, such as telephone calls, as well as other activities that employees undertake in order to prepare to serve customers or that are part of their role responsibilities. Support processes: all activities carried out by individuals in a company who are not contact employees, but whose functions are crucial in carrying out the services process. Physical evidence: all of the tangibles that customers are exposed to or collect during their interaction with a company. Service blueprinting has been widely used in many industries, including the healthcare industry. For example, Marie Stopes International, organization providing reproductive health information, has used service blueprinting to examine who is "on-stage" and what needs to be communicated. The company specifies the customer contact point via physical evidence, solves human resources and operations problems, and finally links them to each moment-of-truth. To sum up, by using a modified service blueprinting tool that incorporates physical evidence, service scripts for onstage personnel, and operations necessary for each moment of truth to be successful, blueprinting has been able to improve the service quality at clinics (Bitner, Ostrom and Morgan, 2007).. io. sit. y. Nat. n. al. er. . Ch. engchi. 3. i Un. v.
(9) More specifically, there exists a definite cause and effect relationship between the five components. Support processes influence the backstage contact employee actions, which in turn affect the performance of onstage contact employees and, by extension, customer satisfaction. The first two processes are generally recognized as internal service operations. The quality of internal service operations has been identified as one of the essential elements of an overall service quality strategy (Feldman, 1991; Nagel & Cilliers, 1990). Sincethe focus of our research is on internal service performance, we will introduce literature relating to support processes and backstage contact employee operations and focus our discussions on the field of e-Health care service delivery.. 2.2 Support processes in the service delivery system Support processes are defined as activities that support employee services and help employees to achieve their task conveniently and effectively. After reviewing past literature, we found out that many sources on e-Health have highlighted two main, supporting activities in e-Health delivery: IT activities (Harnett, 2004; Graschew, 2008; Shelman, 2008) and employee training activities (Rowe, Savigny, Lanata and Victora, 2005). IT activities focus on data and service system integration for service delivery processes, and employee training activities focus on the enhancement of knowledge, abilities and skills.. 立. 政 治 大. ‧. ‧ 國. 學. 2.2.1 IT Support processes. y. Nat. sit. n. al. er. io. A number of firms have employed IT to build service capabilities into their products, greatly improving the speed and accuracy of their service. For example, Federal Express has adopted an information system to minimize unexpected factors that might delay package deliveries (Thomas, 1992). Extending this, Thomas (1992) has made the following conclusions about the impact of IT on service processes: Automation: Eliminates human labor from service process. Informational: Captures information about process performance, which can then be analyzed by humans. Sequential: Changes the sequence of processes or enables parallelism in order to achieve cycle-time reductions. Tracking: Closely monitors process status and objects. Analytical: Improves analysis of information and decision making. Geographical: Coordinates processes across distances. Integrative: Provides information on various aspects of the process stored in databases spread throughout the organization is consolidated in a desktop workstation. Intellectual: Captures and distributes intellectual assets; enables knowledge to be shared across the firm. Disintermediation: Eliminates inefficient intermediaries from service processes.. Ch. engchi. 4. i Un. v.
(10) His findings can also be applied to other service industries, including healthcare In our research model, IT could provide analytical data that would help doctors and healthcare staff to evaluate patient conditions; in addition, integration of IT would help healthcare staff to record patient statistics for future references. In summary, IT plays a vital role in the support processes of service industries, provides for the informational and integrative needs of the company (Harnett 2001, Graschew 2008), and thus, influences service quality. 2.2.2 Training support processes Since employees at the front stage interact with customers directly, their service quality greatly influences customer satisfaction; for this reason, employee training is a necessity in the success of e-Health service delivery. According to past literature such as Bartel (1994), and Saibang et al. (1998), good employee training not only increases productivity, but also enhances the image of the company.. 政 治 大. In 1997, Summers et al. developed an evaluation framework, known as the ―Knowledge Skills Abilities‖ (KSA) test to evaluate training performance. In this context, knowledge refers to an organized body of information associated with facts or procedures which, if applied, makes adequate job performance possible. Skill refers to a proficiency in manual, verbal or mental manipulation of data or things; examples of this include typing on a keyboard or operating a vehicle. Ability refers to the power to perform an observable activity at a given time, e.g., the ability to plan and organize work. More specifically, ability stems from the individual drawing upon previous experience from similar activities or behaviors to complete the job. Anthony et al. (1996) have stated that KSA is a very useful tool in determining who the best applicants are when several candidates qualify for a job.. 立. ‧. ‧ 國. 學. er. io. sit. y. Nat. al. v. n. In summary, IT and employee training are two important dimensions of support processes in service delivery. Without well-integrated IT, loading and manipulating data would be difficult, and without appropriate training, employees would be lacking in the knowledge, skill, and ability needed to perform their jobs.. Ch. engchi. i Un. 2.3 Communication in service delivery systems Organizational communication has been widely recognized as a method for resolving gaps, misunderstandings, and non-synchronized messages within organizational units. Stephen & Arnold (1997) have outlined four communication flows within the intra-organizational context: upward communication, downward communication, horizontal communication, and diagonal communication. Upward communication occurs when information flows from the lower levels of a hierarchy to the higher levels. The goal is to encourage managers to listen to their employees‘ suggestions and to provide employees with a channel to ask their upper-level managers for advice. In our service blueprinting architecture, upward communication would allow e-health staff to consult with doctors within the training support process. 5.
(11) Downward communication occurs when information flows from the top of the organizational management hierarchy to the lower levels; the purpose of this is to inform employees about what is important, what is valued, and how to perform a task in the best possible way. In our service blueprinting architecture, downward communication would allow doctors to transfer information and advice to e-health staff within the training support process. Horizontal communication occurs wheninformation is shared among people at the same level in the organization, community, or peer group; it is usually used as a means of coordinating efforts. In our service blueprinting architecture, horizontal communication would allow e-health staff to help and support to each other within the training support process. Diagonal Communication occurs between people who are at different levels of the organizational hierarchy and in different departments or units (Eleanor and Philip, 2007). Members within an organization can solve problems, share information across. 政 治 大 different work groups, and立 coordinate tasks between departments or project teams ‧. ‧ 國. 學. (Papa et al. 1997). In our service blueprinting architecture, diagonal communication would allow IT staff to help e-Health staff with IT support problems and troubleshooting.. io. sit. y. Nat. These four communication flows are formed in order to eliminate misunderstandings and to improve the performance of intra-organization (Stephen & Arnold, 1997).. n. al. er. In an e-Health context, the four communication flows can be described as the following: the flow from doctors to their healthcare staff (downward communication), healthcare staff to doctors (upward communication), healthcare staff to healthcare staffs (horizontal communication), and healthcare staff to IT staffs (diagonal communication). More specifically, in downward communication, doctors can relate to healthcare staff important knowledge regarding what is important, what is valued, and how to perform a task in the best possible way. In upward communication, healthcare staff can consult doctors with what they don‘t know or ask a superintendent for advice. In horizontal communication, healthcare staff can coordinate with each other to accomplish tasks, support colleagues, and solve problems together. In. Ch. engchi. i Un. v. diagonal communication, IT staff can help healthcare staff to understand how to use IT devices and to provide technical assistance when needed.. 2.4 Summary After reviewing past literature, we found that several sources have put too much focus on what the delivery systems produce (Harnett, 2004; Graschew, 2008; Shelman, 6.
(12) 2008), and too little on how they perform. To address this issue, it is important to understand more about employee internal performance (Spil and Schuring, 2006). Therefore, in our research, we will apply the service blueprinting technique to explore factors that would impact the performance of internal service operations. We believe that it is important to take the KSA-oriented training (Summers, Timothy and Suzanne, 1997) and IT integration into the concern, when evaluating the quality of employee service. Moreover, we will look at the four communication flows (Stephen and Arnold, 1997), while discussing the elimination of intra-organizational barriers and gaps to make organizations more united and efficient. We propose that through improved support processes and communications, organizations will enhance employee service quality, which in turn will improve customer satisfaction and lead the success of e-Health services.. 立. 政 治 大. ‧. ‧ 國. 學. n. er. io. sit. y. Nat. al. Ch. engchi. 7. i Un. v.
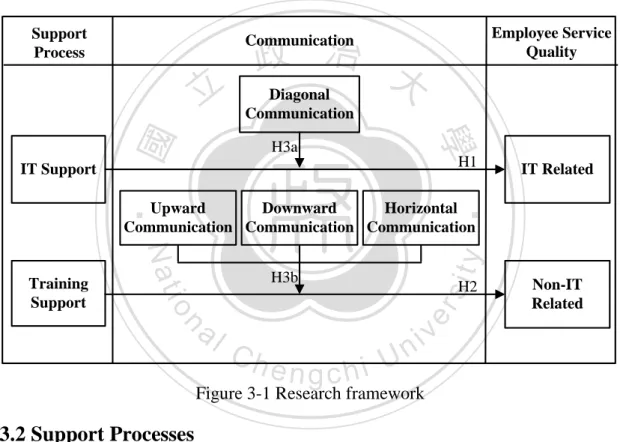
(13) CHAPTER 3: DEVELOPMENT OF RESEARCH FRAMEWORK 3.1 Research Framework According to the service blueprinting of service innovation (Kingman, 1989; W.P. Carey, 2008) and the four communication types within intra-organizations (Stephen and Arnold, 1997), we have identified the research framework shown in Figure 3-1. Derived from the service blueprinting model, our research framework aims to examine the relationship between support processes and employee service quality. We argue that various communication types will impact the relationship between support processes and employee service quality. The details about this framework and hypotheses are described below.. Support Process. 政 治 大 Diagonal. Communication. 學. ‧ 國. 立 IT Support. Employee Service Quality. Communication. H3a. H1. IT Related. ‧. Upward Downward Horizontal Communication Communication Communication. sit. y. Nat. H3b. n. al. H2. er. io. Training Support. Ch. engchi. i Un. Non-IT Related. v. Figure 3-1 Research framework. 3.2 Support Processes According to service blueprint (Kingman, 1989; W.P. Carey, 2008), support processes refer to processes that help a service to achieve goals. In our research, we have separated support processes into two categories, IT support and training support. 3.2.1 IT Support Process IT can be widely applied to support e-Health service delivery. It can allow patients to measure their own body health index, assist doctors in diagnosing patient conditions, and help healthcare staff to store patient records more conveniently. Though there are currently nine types of IT support for service industries (Thomas 1992), Celler et al. (2003) have found that IT is increasingly being used to manage chronic illnesses and help nurses in telemedicine videophone consultations that use home telecare systems. 8.
(14) Bates (2000) has found that using IT in hospitals has helped to prevent many common medical errors; applications such as using robots to fill prescriptions, bar coding, and computerization of the medical administration records have already helped to reduce error rates. Unquestionably, IT systems play a vital role in our research. Healthcare staff use them to store and analyze patient records, to track patient conditions, and more—functions which, as a result of IT, have increased service quality. Therefore, we propose that healthcare staff with good IT support processes will have high service quality. Thus, we develop the hypothesis H1: H1: The healthcare staff with good IT support processes will have high service quality. 3.2.2 Training Support Process. 政 治 大. Training Support refers to the employee training provided by companies to enhance their employees‘ professional ability to serve customers. Blegen et al. (2001) have found that the education, training, and experiences of nurses positively affect the quality of patient care. Summers et al. (1997) have pointed out that employees should receive KSA-oriented training programs. Because e-Health is still relatively new in hospitals, it is important for hospital management to provide specialized training programs in e-Health related knowledge, disease diagnosis, healthcare consulting skills, and so on. Additionally, Puntis et al. (1991) found that an intensive staff training program implemented at a hospital led to a significant reduction of the catheter sepsis rate.. 立. ‧. ‧ 國. 學. io. sit. y. Nat. n. al. er. In our research study,, healthcare staff would enhance their knowledge, abilities, and skills relating to e-Health via different training programs. Hence, with adequate training support, healthcare staff would provide more professional service and improved non-IT related service quality. Thus, we propose hypothesis H2:. Ch. engchi. i Un. v. H2: The healthcare staff with adequate training support will provide improved non-IT related service quality.. 3.3 Communication Herbert (1947) has stated that clear communication is absolutely essential to the success of an organization. Stephen et al. (1997) has also pointed out that via communication, we can eliminate misunderstandings and improve organizational performance. Organizational communication research has therefore often been construed in terms of an information exchange cluster, one that involves information, networks, uncertainty, messages, load, and (more recently) technology (Conrad and Haynes, 2001). Therefore in our research framework, we have integrated communication into e-Health service delivery in order to highlight the importance of communication on the quality of employee service. In the following section, we will 9.
(15) discuss the four communication flows in intra-organization, as researched by Stephen and Arnold (1997). 3.3.1 Diagonal Communication Previously, we defined diagonal communication as the sharing of information between people who are in different departments or units (Eleanor and Philip, 2007). In terms of e-Health, this refers to the communication between the healthcare and IT staffs. Although IT can help improve the efficiency and convenience of service processes, it can also be a hindrance when healthcare staffs don‘t know how to use the systems. In this situation, communication between the healthcare and IT staff is especially important, so that service quality will not be diminished. Healthcare staff should consult with IT personnel what problem they may have and how to fix them; in this manner, issues relating to the inadequacy of the equipment may be avoided. Since the healthcare IT staffs are not in the same department, diagonal communication is necessary to solve work-related problems (Wilson, 1992). IT staff could help healthcare staff understand how to use certain measuring tools or other e-Health related devices; any problem the healthcare staff may have, they could consult with the IT department In summary, healthcare staffs that have good communication with their IT support staff will be better off than without their help. Furthermore, this communication would contribute to higher levels of employee service quality. Thus, we develop the hypothesis H3a:. 政 治 大. 立. ‧. ‧ 國. 學. io. sit. y. Nat. H3a: When there is good communication between the healthcare and IT staffs, IT support may lead to higher levels of employee service quality.. n. al. er. 3.3.2 Upward Communication. Ch. i Un. v. Stephen and Arnold (1997) have defined upward communication as information flowing from the lower levels of an organizational hierarchy to the upper levels. In our research, it refers to the communication flow from healthcare staff to the doctors. Conrad and Haynes (2001) have found that upward communication can help staff with good decision making.. engchi. In our research, healthcare staffs are required to provide patient information to doctors and to consult doctors for advice whenever they have problems. With training support, healthcare staff can provide professional service to patients, but sometimes they may not know how to answer a patient‘s question or have some other non-IT problem they don‘t know, in which case, they would consult doctors for advice. Therefore, we argue that the communication between healthcare staffs and doctors is important, and that enhanced training support would contribute to higher levels of employees‘ non-IT related service quality.. 10.
(16) 3.3.3 Downward Communication Downward communication refers to information flowing from the upper levels of an organizational hierarchy to the lower levels (Stephen and Arnold 1997). Downward communication occurs when managers give orders, recognition, or performance appraisals to employees, which makes service tasks more effective (Grunig, 1992). In our research, downward communication occurs when doctors communicate with the healthcare staff. Doctors inform healthcare staff about what is important, what is valued, and how to perform a task in the best possible way. Using this procedure, healthcare staff would be more adept in handling difficult situations and would provide higher quality service to patients. Thus, the communication between doctors and healthcare staffs is an important factor in enhancing employee service quality and improving training support 3.3.4 Horizontal Communication. 治 政 大between people at the same Horizontal Communication refers to the communication level of an organization 立 or community (Stephen and Arnold, 1997). Horizontal ‧. ‧ 國. 學. communication provides unity and a sense of direction among employees, accurate feedback, and the ability to implement change effectively. Horizontal communication helps a leader gain control and maintains a level of common purpose between co-workers (Massie, 1960; Parkinson, 1997).. n. al. er. io. sit. y. Nat. In our research, horizontal communication occurs when healthcare staffs communicate with each other. Though healthcare staffs should normally carry out their own cases, sometimes problems may arise where they require additional assistance; hence, having a strong support and information distribution network between healthcare staffs would be extremely beneficial. Relaying information about e-Health to other healthcare staffs would also help each individual staff enhance their own knowledge. Via horizontal communication, healthcare staff can share information, experience, and support with each other, so they may provide higher quality services to patients.. Ch. engchi. i Un. v. In sum, we believe that communication between healthcare staffs would enhance training support and contribute higher levels of employee service quality; thus, we propose hypothesis H3b: H3b: When there is good communication between healthcare staffs, and healthcare staff and doctors, training support can lead to higher levels of employee service quality.. 11.
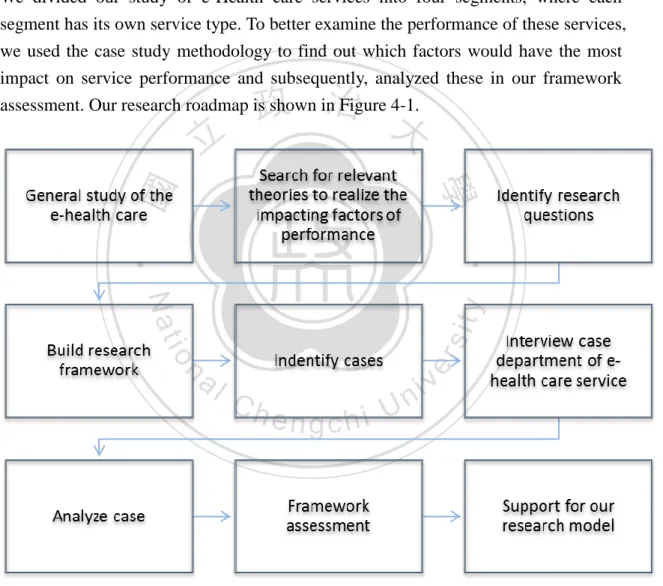
(17) CHAPTER 4: RESEARCH ANALYSIS To test our framework, we developed a multiple-case study that used four segments of data from the e-Health care service program at the National Taiwan University Hospital (NTUH). In this section we will provide the background of our cases and then analyze the variables which we proposed in our research model.. 4.1 Research Methodology We divided our study of e-Health care services into four segments, where each segment has its own service type. To better examine the performance of these services, we used the case study methodology to find out which factors would have the most impact on service performance and subsequently, analyzed these in our framework assessment. Our research roadmap is shown in Figure 4-1.. 立. 政 治 大. ‧. ‧ 國. 學. n. er. io. sit. y. Nat. al. Ch. engchi. i Un. v. Figure 4-1: Research roadmap 4.1.1 Data Collection Our data sources were comprised of group interviews conducted from January of 2010 to June of 2010. For each segment, we interviewed the healthcare, IT, and physician staff, respectively for 30 minutes to an hour. All interviews were recorded on tape, and all sessions were transcribed before the data was analyzed. To enhance the 12.
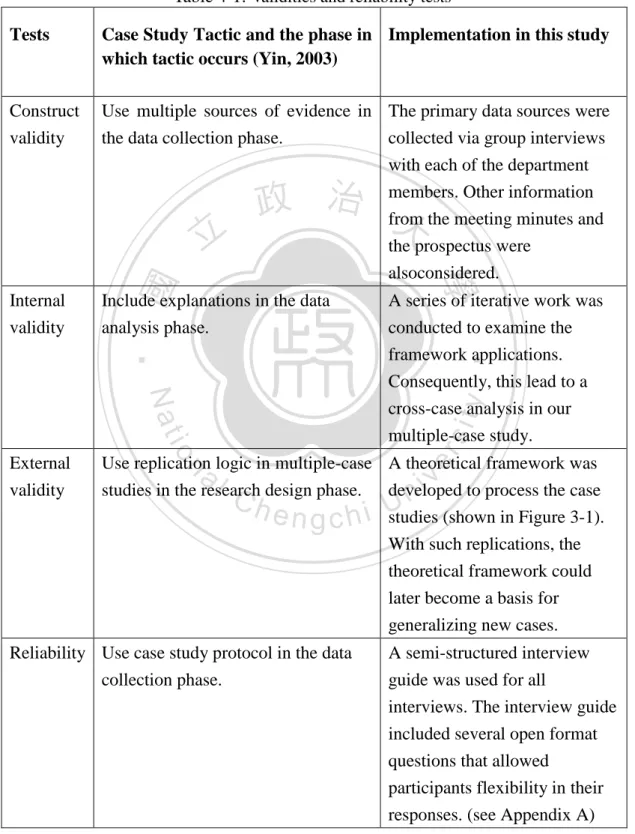
(18) validity of our answers, summaries of the major findings of each interview were verified by the participants after the end of each interview session. Moreover, to verify the construct validity, internal and external validity, and reliability of the case study proposed by Yin (2003), the following recommended case study tactics were used. Our results are presented in Table 4-1.. Table 4-1: Validities and reliability tests Tests. Case Study Tactic and the phase in Implementation in this study which tactic occurs (Yin, 2003). Construct validity. Use multiple sources of evidence in The primary data sources were the data collection phase. collected via group interviews with each of the department members. Other information. Include explanations in the data analysis phase.. A series of iterative work was conducted to examine the framework applications. Consequently, this lead to a cross-case analysis in our. ‧. multiple-case study.. al. er. io. sit. y. Nat. Use replication logic in multiple-case A theoretical framework was studies in the research design phase. developed to process the case studies (shown in Figure 3-1). With such replications, the theoretical framework could later become a basis for generalizing new cases.. n. External validity. 學. Internal validity. the prospectus were alsoconsidered.. ‧ 國. 立. 政 治 from 大 the meeting minutes and. Ch. engchi. Reliability Use case study protocol in the data collection phase.. i Un. v. A semi-structured interview guide was used for all interviews. The interview guide included several open format questions that allowed participants flexibility in their responses. (see Appendix A). 13.
(19) 4.2 Research Analysis In this section, we will first introduce the background of each case segment of e-Health care service. Then, we‘ll analyze these cases according to the framework proposed in Chapter 3. 4.2.1 Case Background The National Taiwan University Hospital (NTUH), which is one of the largest hospitals in Taiwan, established an e-Health center in 2009, which emphasized the delivery of real-time healthcare service through remote devices. Furthermore, patients received continuous medical care and health consultation through remote health monitoring even after they were discharged from the hospital. In this study, we will investigate the performance of NTUH e-Health service. The NTUH divides services into four segments, which are distinguished by four different medical situations: Post-discharge Care Service (A1), Cardiovascular Disease Care Service (A2), Chronic Disease Care Service (A3), and Hospice Care Service (A4).. 立. 政 治 大. ‧ 國. 學. ‧. A1: Post-discharge care service: A care service provided after a patient is discharged from the hospital, e.g. when a healthcare staff calls a recently discharged patient to record and analyze their body index and provide tele-consultation.. er. io. sit. y. Nat. A2: Cardiovascular disease care service: A service provided for patients with cardiovascular disease that uses a set of body index measurement devices called the ―baby bot‖. Patients have to upload their data to healthcare staff, after which healthcare staff record and analyze their body index, and provide appropriate tele-consultation and diagnosis of the problem.. al. n. iv n C A3: Chronic Disease Care hService: i U that provides body index e n g cAhservice measurement devices to patients with chronic disease, (e.g. a sphygmomanometer or blood sugar measurement device). Patients have to upload their data to healthcare staffs, whereupon healthcare staff analyze their body index and provide tele-consultation. A4: Hospice Care Service: A service that provides near-death patients with tele-consultation, video conferencing, and psychological and religious counseling. Each service has its own healthcare staff that monitors the patients‘ health and provides urgent consultation, when patients require daily health information or call in for help. Physicians would support the health care services by providing professional medical suggestions. It‘s expected that patients who use e-Health service receive faster service and increased quality of life.. 14.
(20) 4.2.2 Framework Application For each of the four segments, we ask, ―Which department has the best performance and influencing factor?‖ ―Can good communication between the different support processes positively affect employee service quality?‖ To answer these questions, we will next interpret these cases using the research framework proposed in the earlier chapter.. Support process In the context of our research framework, support processes can be divided into two variables, training and IT support (see row I in Table 4-2). 1. Training support. In terms of e-Health service, hospitals should provide relevant training for the healthcare staffs to do their job. From the group interview and the prospectus, we discovered that each. 政 治 大 department needs different training for its health staffs. Since these staffs inherently 立 do not have relevant experience, hospitals should provide training to enhance SOP ‧. ‧ 國. 學. processing abilities, specialized service, health education, and knowledge of appropriate phone-calling procedures to all departments. More specifically, the A3 department needs to provide training for nutritional-based knowledge, and A4 needs to provide the training for psychological and religion counseling, according to their specific service needs. From our interview with healthcare staffs and doctors, we found that the A1. sit. y. Nat. n. al. er. io. department did not provide any out of the four required trainings; the A2 department provided three out of the four required trainings; The A3 department provided four out of the five required trainings; and, A4 provided all required trainings for their healthcare staffs. We assessed the degree of training support based on the percentage of trainings required and the numbers provided by the department. Therefore, we ranked A1 with a low level, A2 and A3 department with a medium to high level, and A4 department with the highest level of support.. Ch. engchi. i Un. v. Below are excerpts of our interviews: There is no health education training; we just depend on our experience (A1 healthcare staff). I think our priority should be to promote how to take care of the patient; usually, they just provide us with the general lesson (A2 healthcare staff). We think they should provide nutrition and diet related lessons (A3 healthcare staff). 15.
(21) Training should be for people who need further enrichment in hospice care Knowledge (A4 healthcare staff). 2. IT support. In terms of e-Health, IT systems and measuring devices also helps healthcare staffs provide crucial services. Healthcare staffs in the A1 department, with the help of IT systems, record and measure patients‘ data, generate reports, analyze physiology data, and provide consultations by phone. In our interview, we found out that the A1 department thinks that the integration of IT systems and the provision of health reports are the most deficient of the four IT supports. Healthcare staff in the A2 department, use IT systems to record patients‘ data, generate reports, analyze physiology data, make phone calls, and help patients to solve problems with their measure devices (issues about their stability, ease of use, compatibility, and design). In our interview, the A2 department believed that the reliability, ease of use, and compatibility of the measuring devices and new functions of IT system need further improvement. The A3 department healthcare staff, with the help of IT systems,. 立. 政 治 大. ‧. ‧ 國. 學. receives measuring data via 3G, record patients‘ measuring data, analyze physiology data, and make phone calls to patients. In our interview, we found that the A3 department thinks the reliability and ease of use of the measuring device, the integration, and data transmission compatibility of the IT systems have the most deficiencies. The A4 department healthcare staff, with the help of IT systems, makes video conferencing via 3G, arrange patients‘ data, and make phone calls. In our interview, we found that the A4 department thinks that 3G signal causes the most. sit. y. Nat. n. al. er. io. issues. We assess the degree of IT supports based on the percentage of deficiencies reported on all IT supports in the department. In sum, we‘ve assessed that departments A1, A2 and A3 provide a medium level of support, and that A4 provides medium to high level of support.. Ch. engchi. i Un. v. Below are excerpts from our interviews: If there were better integration of the IT systems and support staff who could direct me to the system that what I need, things would be a lot easier (A1 healthcare staff). Measuring device problems are a big deal, since we measure data every day and need to make decisions by it (A2 healthcare staff). Losing signal is our biggest problem; sometimes data which was sent two days ago isn’t received until two days later (A3 healthcare staff). Besides using 3G, there are others are good signal supports. (A4 healthcare staff). 16.
(22) Communication Communication includes four major subcategories: diagonal communication, upward communication, downward communication, and horizontal communication (see Table 4-2, row II). 1. Diagonal communication. In e-Health, healthcare staffs have to help patients to solve problems with devices and measure data using IT systems; consequently, it is essential that they have good communication with the IT staff. We define this level of communication by the examining the coordination between healthcare staffs and IT staffs with regards to different devices and systems. Healthcare staffs have to coordinate with IT staffs frequently, especially in the A2 department, since there are so many devices involved. The A3 department has two main measuring devices involved, and the A4 and A1 departments have one and no devices involved, respectively. Using the number of devices as a basis, we can. 政 治 大 determine the department‘s frequency of communication with IT staffs. Our results 立 show that the A1 department has the lowest level of communication, A3 and A4 have. ‧ 國. 學. a medium level, and A2 has the highest. Below are excerpts from our interviews:. ‧. er. io. sit. y. Nat. When a member from the IT staff comes to set up the measuring machine for patients, they’ll let us know ahead of time, so we can start making a schedule (A2 healthcare staff). We have asked the IT staff to adjust measuring machines before (A3 healthcare staff).. n. al. Ch. engchi. i Un. v. We’ve had the problem of delayed e-mails, but the IT department couldn’t repair immediately, as it was during a holiday (A3 healthcare staff). 2. Upward communication. Healthcare staffs have to consult with doctors when they have problems, or other demanding situations. From the interviews, we found out that upward communication most often occurs when healthcare staffs have a question relating to medication, a follow-up, or patients‘ consultation question in order to truly address the patients‘ condition. Healthcare staffs usually met with physicians once or twice a week. The A3 department met the most often, and asked about all the topics except medication, in general; A1 didn‘t communicate with doctors about the medication or follow-up questions; A2 didn‘t communicate with doctors about patients‘ consultation; and, A4 didn‘t make communication with doctors in regards to follow-ups and patient consultations. Thus, we assessed the level of communication based on the frequency 17.
(23) that the healthcare staffs consulted the doctor, and found that the A1 department had the lowest level, A3 and A4 had a medium level, and A2 had the highest level. Below are excerpts from our interviews: We communicate with doctors face to face to tell them which patient has a problem. Also, we have meetings once a week, so we can consult to doctors (A1 healthcare staff). Often, we’d ask doctors if a patients’ medication needed to be adjusted, or whether the patient needed a follow-up (A2 healthcare staff). If a patient has problem, we would refer to a doctor for advice (A3 healthcare staff).. 政 治 大. We have meeting every Tuesday to report to doctors and discuss the cases we’ve had (A4 healthcare staff).. 立. ‧. ‧ 國. 學. 3. Downward communication. Doctors have to instruct healthcare staffs on what they think would help healthcare staffs. We define this level of communication by the number of times doctors instruct healthcare staffs of their own accord. From the interviews, we found out that downward communication occurs when doctors want to give feedback, or share a message, either in person, or in the regular meetings that occur once or twice a week. A1 department doctors had the most occurrences of downward communication for both purposes; A2 and A4 doctors mostly shared. sit. y. Nat. n. al. er. io. messages, and A3 doctors only gave feedback. We determined that the A1 department had the highest level of downward communication, A2 and A4 department had a medium-to-high level, and A3 department had a medium level.. Ch. engchi. i Un. v. Below are excerpts from our interviews:. We have meetings once a week, where the doctor tells us what to trace (A1 healthcare staff). We give them feedback on problem solving and encourage them to consult us, whenever they have an issue (A1 doctor). We transmit important messages to healthcare staffs (A2 doctor). We have meetings twice a week and give them feedback on the spot; but I think they [the healthcare staff] should personally contact me, because otherwise, I would think they did not have problem (A3 doctor). 4. Horizontal communication. From our interviews, we found that healthcare staffs 18.
(24) have to hand over tasks when they are off work to another staffs who are on duty. They also have to support and share experiences with each other, in order to have a better job performance. We define this level of communication by the number of ―job-handing over‖, and support and experience sharing between the healthcare staffs. A1 has the best of all the above items; A2 has a little problem with handing over and experience sharing; and both A3 and A4 have lack in support and have a problem in experience and message sharing. We assessed that the A1 department has the highest level of horizontal communication, A2 has a medium-to-high level, and A3 and A4 both have medium levels. Below are excerpts from our interviews: We have to support with each other and share messages through meetings once a week (A1 healthcare staff).. 政 治 大. Some people are effective in handing over, but some are not (A2 healthcare staff).. 立. ‧ 國. 學. We would upload data of patients’ problem and hand it over to the system (A4 healthcare staff).. Employee service quality. ‧. sit. y. Nat. Employee service quality can be classified into two subcategories: IT related service quality and non-IT related service quality (shown in Table 4-2, row III).. n. al. er. io. 1. IT related service quality. Healthcare staffs have to a responsibility to provide adequate IT-related service quality to patients. Examples of this service include: helping patients to solve problems with measuring devices, generating healthy reports, and analyzing the patient‘s body index with IT systems. It follow that patients are directly affected by the IT-related service quality. Thus, we define the IT related service quality of a department by the service completeness, given by IT systems. Through our interviews and data analysis, we discovered that the IT systems in the A2 department demonstrate all of above service qualities. In contrast, the A1 IT department doesn‘t help patients solve device problems, and the A3 and A4 departments don‘t provide healthy reports to patients. Thus, we‘ve designated the A1 and A4 department with medium level of service quality, the A2 department with high. Ch. engchi. i Un. v. level, and the A3 department with medium-to-high level. Below are excerpts from our interviews: We would use the IT system for tracing patients’ health index, but we can also generate the health report ourselves (A1 healthcare staff). 19.
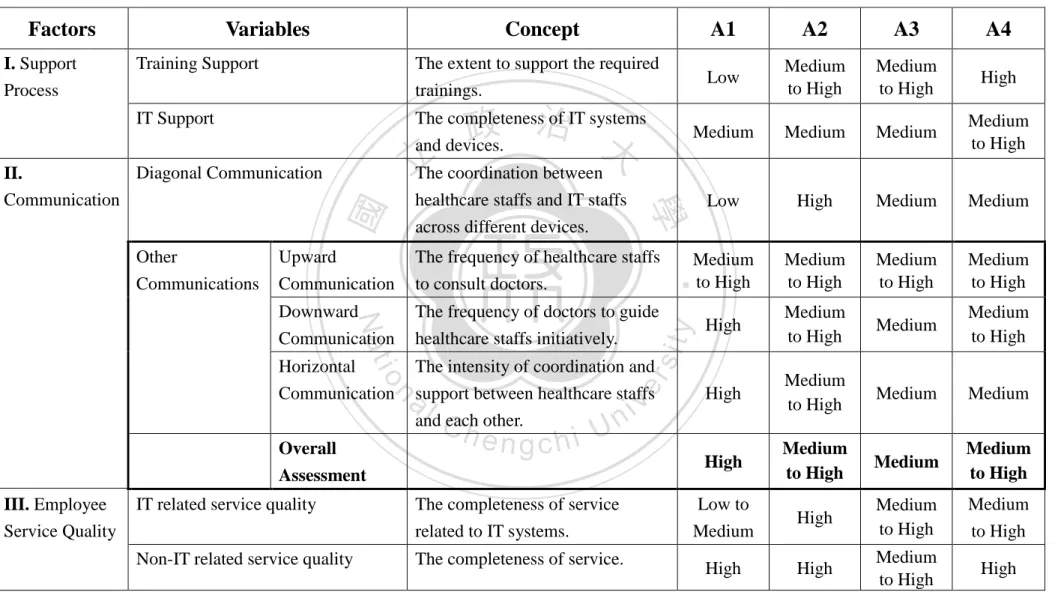
(25) We have to help patients to solve their problems with measuring devices, since unusual data measurements would cause them to worry (A2 healthcare staff). We analyze patients’ body indexes and to solve their problems using a measuring device (A3 healthcare staff). We use IT systems to reorganize and acquire data, and to video conference with patient (A4 healthcare staff). 2. Non-IT related service quality. Healthcare staffs also provide lots of service unrelated to IT. For example, we‘ve discovered that healthcare staffs provide consultations, make phone calls to patients, and provide assurances and relief to worried patients. In this study, we define non-IT related service quality by the degree of service completeness. From our interviews and research, we found out that only the A3 department has did not provide adequate relief and concerns to patients; the other three departments performed well enough in all the above mentioned service items.. 立. 政 治 大. ‧ 國. 學. Therefore, we‘ve assessed the A1, A2 and A4 department to have a high level non-IT related service quality, and theA3 department to have a medium-to-high level. Below are excerpts from our interviews:. ‧. sit. y. Nat. We would check-in on the patient by phone and provide call in service for consultation in order to allow the patient to feel more close to us (A1 healthcare staff).. er. io. When patient called in for consultations, we would give them advice on medicines and diets, thereby providing relief (A2 healthcare staff).. al. n. iv n C We would call out to patients h three i U out of concern for them (A3 e ntimes g c ahweek healthcare staff).. Besides medicinal care, we provided extra services such as psychological and religious counseling (A4 healthcare staff). So far, we have seen the factors that impact the performance of delivery system from case to case. Table 4-2 summarizes these factors according to the above analysis (for original Chinese content of interviews, see Appendix B). In the table, we can compare the concept of each variable in our model, and the level of each department corresponding to each concept. From this table, we can conclude that communication factors do influence support processes to positively affect employee service quality.. 20.
(26) Table 4-2: Cross-case analysis. Concept. A1. A2. A3. A4. Training Support. The extent to support the required trainings.. Low. Medium to High. Medium to High. High. IT Support. The completeness of IT systems and devices.. Medium. Medium. Medium. Medium to High. Low. High. Medium. Medium. Medium to High. Medium to High. Medium to High. Medium to High. High. Medium to High. Medium. Medium to High. High. Medium to High. Medium. Medium. High. Medium to High. Medium. Medium to High. Low to Medium. High. Medium to High. Medium to High. High. High. Medium to High. High. 政 治 大. Downward Communication. The frequency of doctors to guide healthcare staffs initiatively.. Horizontal Communication. The intensity of coordination and support between healthcare staffs and each other.. io. sit. The frequency of healthcare staffs to consult doctors.. Nat. Upward Communication. al. n. Overall Assessment III. Employee Service Quality. y. healthcare staffs and IT staffs across different devices.. ‧. Other Communications. 立 The coordination between. 學. Diagonal Communication II. Communication. er. I. Support Process. Variables. ‧ 國. Factors. Ch. engchi U. v ni. IT related service quality. The completeness of service related to IT systems.. Non-IT related service quality. The completeness of service.. 21.
(27) CHAPTER 5: DISCUSSION Across the four cases, we observed different levels of support, communication, and employee service quality. In this chapter, we will first illustrate the result of the cross-case analysis and then discuss the results in comparison to our research model.. 5.1 Cross-Case Analysis Results Figure 5-1 shows the summary of case analysis presented in the last chapter. As the charts (a) and (b) indicate, we can see the impact of diagonal communication on IT support of each department, as well as the impact of other communications on the non-IT support of each department. (a). 政 治 大. The impact of diagonal communication on IT support. 立. IT support. io. A4. Department. al. n. (b). y. A3. sit. A2. IT related service quality. er. Level. ‧. ‧ 國. 學. Nat. A1. Diagonal communication. Ch. engchi. i Un. v. The impact of other communications on training support. Training support Level. Communication of overall Non-IT related service quality A1. A2. A3. A4. Department. Figure 5-1. Summary of case analysis: (a) the impact of diagonal communication on IT support and (b) impact of other communications on non-IT support. 22.
(28) 5.1.1 Impact of diagonal communication on IT support As the chart indicates, A1, A2 and A3 belong to a medium level of IT support process, while A4 belongs to a medium-to-high level of IT support process. It was observed in the preceding chapter that each department needs to strive for more completeness in their provision of IT-related service. In terms of diagonal communication, A1 and A2 belong to a low and high level, respectively, while A3 and A4 belong to a medium level. In IT-related service quality, we see that A1 belongs to a low-to-medium level; A4 belong to medium level, A2 belongs to a high level, and A3 belongs to a medium-to-high level. In later paragraphs, we will examine hypothesis H1 and H3a, which we introduced in a previous section. First, we examine our H1 hypothesis, which stated that ―healthcare staffs with good IT support process would be able to provide good IT-related service quality.‖ We. 治 政 大 they weren‘t at the same related service quality had a low-to-medium level. Even level, we can still classify 立 this as a positive relationship. The A2 department had a can see that the A1 department had a medium level of IT support and the employee IT. ‧ 國. 學. medium level of IT support and a high level of employee IT-related service quality; we can see that this does not demonstrate a positive relationship. The A3 department. ‧. had a medium level of IT support and a medium-to-high level of employee IT-related service quality. Though this is not classified as being on the same level, we can easily. sit. y. Nat. classify this as a positive relation. The A4 department had a medium-to-high level of IT support and a medium-to-high level of employee IT related service quality, as well,. io. er. so we can also conclude this as a positive relation. To sum up, we could not. al. n. iv n C them to provide good IT-related service; U case study does not support h e n therefore, h i our c g hypothesis 1. We predict that other factors may have been needed to sufficiently back completely determine that healthcare staffs with good IT support process would allow. support the hypothesis. The second hypothesis we will examine isH3a, which states, ‖when there is good communication between healthcare staffs and IT staffs, IT support will contribute to higher levels of employees IT-related service quality.‖ We can see that A1 department had a medium level of IT support, since the hospital only provided half of the IT system that employees in needed; and, additionally, the communication between healthcare staffs and IT staffs was bad. Therefore, inadequate IT support seems to have a relationship with employee service quality that may have caused it to lower. The A2 department had a medium level of IT support, since the hospital only provided half of IT system that employees needed, but the healthcare staff had good communication with the IT staffs; this shows that, even if IT support isn‘t good 23.
(29) enough, there can still be a high level of employee IT related service quality. The A3 department had a medium level of IT support, since the hospital only provided half of IT system that employees needed, and, additionally, the communication between healthcare staffs and IT staffs wasn‘t very good. However, A3‘s employee IT related service quality exhibited an unexpected medium-to-high quality. In this case, we think even though the healthcare staff didn‘t have good communication with the IT staff, through their ability to learn spontaneously, they were able to recover the setback. Lastly, the A4 department had a medium-to-high level of IT support, since the hospital provided almost all the IT support needed; and, once again, the communication between healthcare staffs and IT staffs was not optimal. Therefore, its employee IT related service quality also had a medium-to-high level. In sum, our case study adequately supports hypothesis H3a, which states: when. 治 政 大 quality. contribute to higher levels of employees‘ IT-related service 立. there is good communication between healthcare staffs and IT staffs, IT support can. 5.1.2 Impact of other communications on training support. ‧ 國. 學. Let‘s now look at the impact of other communications on non-IT support. Figure 5-1 chart (b) shows that A1 belongs to a low level of training support process, A2 and A3. ‧. belong to a medium-to-high level of training support process, and A4 belongs to a. Nat. y. high level of training support process. It was observed in the preceding chapter that the. three. communications. al. (upward,. downward. and. horizontal. er. of. io. levels. sit. each department requires more extensive support training. In terms of the overall. n. communication), A1 belongs to a high level, A2 and A4 belong to a medium-to-high. Ch. i Un. v. level, and A3 belongs to a medium level. For non-IT related service quality. engchi. (diagrammed in chart b), we see that A1, A2 and A4 belong to a high level, while A3 belongs to medium-to-high level. In the following paragraph, we will examine our hypotheses H2 and H3b, as proposed in a former section. We will first examine hypothesis H2: ―Healthcare staffs with good Training support process will provide good non-IT related service quality‖. Our results show that the A1 department had a low level of training support, but a high level of employee non-IT related service quality; clearly these two levels have an inverse relationship. The A2 department had a medium-to-high level of training support and a high level of employee non-IT related service quality. Even though these didn‘t they have same quality level, we can still classified this as a positive relationship. The A3 department exhibited a medium-to-high level of training support, as well as a medium-to-high level of employee service non-IT related quality, in which we can classify as a positive relationship. Lastly, the A4 department had a high level of 24.
(30) training support, in addition to a high level of employee non-IT related service quality, which also demonstrated a positive relationship. To sum up, we could not completely conclude that healthcare staffs with good training support process would provide good non-IT related service; to prove this, we would need other factors to back up the hypothesis. We therefore conclude that our case study does not support hypothesis 2, that ―healthcare staffs with good training support process would provide good non-IT related service quality.‖ We next examine hypothesis H3b, which states that ―upward, downward, and horizontal communication can allow training support to contribute to a higher or lower level of employee non-IT related service quality. We can see that the A1 department had a low level of training support, since they did not provide need training; fortunately, however, the healthcare staffs had good overall communication. 治 政 大 had a medium-to-high employee non-IT related service quality. The A2 department 立 the hospital only lacked one missing training session, level of training support, since using the three types effectively, and thus, were able to demonstrate a high level of. ‧ 國. 學. and additionally exhibited a medium-to-high level of communication between its employees; this communication made up their lack of training support, and thus. ‧. contributed to a higher level of employee non-IT related service quality. The A3 department had a medium-to-high level of training support, since the hospital also. sit. y. Nat. only missed lacked in one training session; thus, with medium level of healthcare staff communication, its employee non-IT related service quality was still at a. io. er. medium-to-high level. The A4 department still had a high level of training support,. al. n. iv n C U three communications, which healthcare staffs had a medium-to-high h e nlevel g cofhalli of. since the hospital provides all training that employees needed; and additionally, the lead to a higher level of employee non-IT related service quality.. Therefore, our case study supports hypothesis 3b, which states that, ―when there is good communication between healthcare staffs and doctors, as well as between each other, training support can contribute to higher levels of employees‘ non-IT related service quality.. 5.2 Managerial Implications According to Figure 5-1, we find that communication plays an important role in managerial implications, even the level of IT support or training support is low. If the level of communication is high, this would increase employee service quality and vice versa. As a result, we realize that quality e-Health services should provide training support to healthcare and before they start their service and provide IT support to 25.
(31) assist the service process. To facilitate service performance, the four types of communication should also be included.. 立. 政 治 大. ‧. ‧ 國. 學. n. er. io. sit. y. Nat. al. Ch. engchi. 26. i Un. v.
(32) CHAPTER 6: CONCLUSION 6.1 Summary In Taiwan, e-Health has become a new trend of medical treatment and healthcare, especially in remote areas, since it can reduce the number of required resources and provide more convenience to hospitals and patients. In our research, in order to make the service process more efficient and improve the performance of whole service delivery system, we discussed the factors that influence the internal processes of a delivery system. By studying related literature, we build our research model to measure the factors that may impact the performance of delivery system and, in doing so, divided the whole delivery service system into. 政 治 大. four parts: (1) the support process which includes training and IT, (2) the IT and non-IT service quality of healthcare staffs, (3) the communication within the whole. 立. e-Health service team, and (4) customer quality action. To test the proposed hypotheses,. ‧ 國. 學. we carried out group interviews to gather useful insights about healthcare delivery services; and, after a series of measurement assessments and a cross-case analyses, we found many of our hypotheses d to be valid.. ‧. Through our research, we found that support processes can influence the service. y. Nat. quality of employee and that communication is the most important factor in the. sit. delivery of service—more specifically, the diagonal, upward, downward, and. er. io. horizontal communication within the organization. Through careful analysis, we have. al. n. iv n C Final, we give some suggests for departments: h eeach i U h n c g • A1: To enhance training support and IT support,. shown that these factors have a great impact on the e-Health delivery system. and their diagonal. communication. •. A2: To enhance IT support.. •. A3: To enhance IT support, and their communication within organization.. •. A4: To enhance their diagonal communication.. 6.2 Limitations and Implications of Future Research In our study, we evaluated our measurements by group interviews and organizing weekly meeting minutes. For future research, we hope in the future, through our lasting research and cooperate with NTUH, we could extend our research to discuss whether employee service quality could influence patients‘ satisfaction quality or not. The service quality can be investigated from two categories, IT related service quality and non-IT related service quality. 27.
(33) As to IT-related service quality, Bates (2000) mentioned healthcare staff can use information technologies to prevent medication errors and to improve their service quality. In our research, healthcare staff would use IT to record patient data, provide tele-consultation through remote-area devices, and provide patients with their own IT-analyzed health reports. Additionally, should patients consult the healthcare staff about IT device related problems, the healthcare staff would be sufficiently trained enough to provide a correct answer for them. Since these services are supported by IT, employee service quality is thus directly correlated to IT related service quality; if healthcare staff provide good service quality using IT, patients will feel more confident in the not only the service supported by IT related devices, but the whole ITintegrated system itself (Nagel & Cilliers, 1990). Regarding with non-IT related service quality, Eysenbach (2001) proposed that the most important goal for e-Health services is the control and alleviation of disease. In our research, patient relief is the most important goal that hospital staffs care about.. 政 治 大 Healthcare staff employee training has focused largely on providing good service 立 quality to patients; for instance, nurses would reply patients‘ questions using their ‧. ‧ 國. 學. professional knowledge, respond with good attitudes, and so on. This is what we define as non-IT related service quality. If healthcare staffs do not provide good service quality to patients, for example, not being able to provide correct answers to questions, patients may lose confidence in e-Health services. We believe that the ability of healthcare staffs to provide good non-IT related service quality directly influences patient satisfaction quality and assurance. These two propositions can be. sit. y. Nat. n. al. er. io. further examined in the future.. Ch. engchi. 28. i Un. v.
(34) REFERENCE 1. A Key to Service Innovation: Services Blueprinting. January 30, 2008 in [email protected]. Carey. 2. Anthony, W. P., Perrewe, P. L., & Kacmar, K. M. (1996). Strategic human resource management. Fort Worth : Dryden 3. Bartel, Ann P. 1994. ―Productivity Gains Form the Implementation of Employee Training Programs.‖ Industrial Relations (October). 4. Bates DW. Using information technology to reduce rates of medication errors in hospitals. BMJ 2000;320:788–91.. 政 治 大 quality of care. J of Nurs Admin 2001;31:33-9. 立. 5. Blegen MA, Vaughn T, Goode CJ. Nurse experience and education: effect on. ‧ 國. 學. 6. B Parkinson, P Hudson, R Senior, C Short(1996).Horizontal Bilateral Communications Improved by Extended Classical Approaches.. ‧. 7. Brett Harnett, Current Principles and Practices of Telemedicine and e-Health, IOS Press, Volume 131,February 22, 2008;pp55-65.. y. Nat. sit. 8. Celler BG, Lovell NH, Basilakis J. Using Information technology to improve the. io. al. er. management of chronic disease. Medical Journal of Australia2003; 179(5):242–6.. v. n. 9. Conrad C. & Haynes J. (2001). Development of key constructs. In F. M. Jablin & L. Putnam (Eds.), The new handbook of organizational communication: Advances in theory, research, and methods (pp. 47-77). Thousand Oaks, CA: Sage.. Ch. engchi. i Un. 10. D. C. Goodman and K. Grumbach, ―Does Having More Physicians Lead to Better Health System Performance?‖ Journal of the American Medical Association, January 23, 2008 299(3): 335–37. 11. E.Gummesson and J. Kingman-Brundage, ―Service Design and Quality: Applying Service Blueprinting and Service Mapping to Railroad Services,‖ in Eleanor J. Sullivan, Philip J. Decker, The effective healthcare staffs: leader and manager, 2005. 12. Eysenbach G. What is e-health? J Med Internet Res .2001,3(E20). 13. Feldman, S. (1991), ―Keeping the customer satisfied inside and out‖, Management Review, Vol. 80 No. 11, pp. 58-60. 29.
(35) 14. Graschew G, Roelofs TA, Rakowsky S, Schlag PM. Network design for telemedicine--e-health using satellite technology. Stud Health Technol Inform 2008; 131: 67-82. 15. Grunig, J. E. (1992). Communication, public relations, and effective organizations: An overview of the book. In J. E. Grunig (Ed.), Excellence in public relations and communication management. Hillsdale, NJ: Lawrence Erlbaum Associates. 16. Herbert Simon, Administrative Behavior, 4th ed., p 208. 17. Joseph L. Massie (1960). Automatic Horizontal Communication in Management. The Journal of the Academy of Management, Vol. 3, No. 2. (Aug., 1960), pp. 87-91. 18. Keith Shelman, Changing from Paper to Paperless Hospitals in Busy Academic Center, IOS Press, Volume 131,February 22, 2008;pp83-96.. 立. 政 治 大. ‧ 國. 學. 19. Kingman-Brundage, J., 1995, Service mapping: back to the basics, Understanding Service Management,edited by Glynn, W. J. and Barnes, J. G., John Wiley & Sons, Chichester, 119-142.. ‧. 20. Mary Jo Bitner, Amy Ostrom, and Felicia Morgan 2007 ‗Service blueprinting: A practical technique for service innovation.‘ California Management Review, 50/3: 66-94.. sit. y. Nat. n. al. er. io. 21. Nagel, P. and Cilliers, W. (1990), ―Customer satisfaction: a comprehensive approach‖, International Journal of Physical Distribution & Logistics Management, Vol. 20 No. 6, pp. 2-46.. Ch. engchi. i Un. v. 22. Papa, Michael J., Tom D. Daniels, and Barry K. Spiker (1997). Organizational Communication Perspectives and Trends (4th ed.). Thousand Oaks: Sage Publications Inc. 23. P. Kunst and J. Lemmink ed., Quality Management in Services (Assen/Maastricht, Nertherlands: Van Gorcum, 1991). 24. Puntis JWL, Holden CE, Smallman S, Finkel Y, George R, Booth IW. Staff training: a key factor in reducing intravascular catheter sepsis. Arch Dis Child 1991; 66:335-337. 25. Rowe, A., de Savigny, D., Lanata, C., Victora, C. (2005). How can we achieve and maintain high-quality performance of health workers in low resource settings. Lancet, 366, 1026-1035. 30.
(36) 26. Saibang, P., & Schwindt, R. C. (1998). The need for employee training in hotels in Thailand. International Journal of Training and Development, 2(3), 205-214. 27. Shortell, S. and Kaluzny, D., Essentials of Health Care Management, 1997, p.242-243. 28. Silber, D. (2003), The Case for eHealth, The European Commission‘s conference on eHealth, Brussels,Belgium. 29. Summers A, Timothy P, Suzanne B. Strategic skills analysis for selection and development, Human Resource Planning, 1997, 20: 14~19. 30. Thomas H. Davenport, Process Innovation Reengineering Work through Information Technology, Harvard Business Press, 1992.. 政 治 大. 31. Ton A. M. Spil, Roel Schuring, ―E-health systems diffusion and use: the innovation, the user and the Use IT Model‖, 2006.. 立. 32. Wilson D. 1992, ―Diagonal communication links within organizations‖, The. ‧ 國. 學. Journal of Business Communication, 29(2), 129-143.. ‧. 33. Wilson, P., Leitner, C., & Moussalli, A. (2004). Mapping the Potential of eHealth: Empowering the Citizen through eHealth Tools and Services, In Proc of E-Health Conference 2004, Cork, Ireland. Retrieved March 15, 2009.. y. Nat. n. al. er. io. Oaks, CA, 2003.. sit. 34. Yin, R. K. Case study research: design and methods Sage Publications, Thousand. Ch. engchi. 31. i Un. v.
數據
+2

相關文件
In fact, his teachers believe that it is his good ear for music that has helped him with the precise pronunciation of different languages – especially with a tonal language like
已參加政府主辦或委辦之 教保員、訓練員、生活服務 員、照顧服務員、家庭托顧 服務員、臨時及短期照顧服 務員或個人助理相關訓練
為了解民眾對本機關各項 為民措施及服務人員的評 價,委外辦理「整體服務 品質滿意度調查」 ,針對洽 公民眾、受訓學員、轄區
(2) 一案到底服務專員對於 求職挫折民眾,提供情緒 支持與關懷服務,運用諮 商技巧正向鼓勵求職民 眾,以提升求職民眾自信
擴大商品及服務、民族、文化及信息交流。為支援基礎設施建設,中國帶頭成立 1,000 億美元 的亞洲基礎設施投資銀行,有 57 個國家作為創始成員國參與其中。中國亦於
△△聯合診所所提供之服務範圍計有門診醫療服務(一樓)及 復健治療服務(二樓)兩項,本研究係針對一樓「門診醫療服務流 程」進行研究。由於△△聯合診所之門診醫療服務不具設計及研發
服務提供者透過 SOAP 訊息將網路服務註冊在 UDDI 中,服務需求者也可以透 過 SOAP 向服務仲介者查詢所需的 Web Service 並取得 Web Service 的 WSDL 文件,2.
醫院工作實務中常聽及醫師、護士、行政支援人員及病患抱怨許
