ORIGINAL PAPER
Design and Implementation of Web-Based Mobile Electronic
Medication Administration Record
Sung-Huai Hsieh&I-Ching Hou&Po-Hsun Cheng&
Ching-Ting Tan&Po-Chao Shen&Kai-Ping Hsu&
Sheau-Ling Hsieh&Feipei Lai
Received: 17 February 2009 / Accepted: 30 April 2009 / Published online: 22 May 2009 # Springer Science + Business Media, LLC 2009
Abstract Patients’ safety is the most essential, critical issue, however, errors can hardly prevent, especially for human faults. In order to reduce the errors caused by human, we construct Electronic Health Records (EHR) in the Health Information System (HIS) to facilitate patients’ safety and to improve the quality of medical care. During the medical care processing, all the tasks are based upon physicians’ orders. In National Taiwan University Hospital (NTUH), the Electronic Health Record committee proposed a standard of order flows. There are objectives of the standard: first, to enhance medical procedures and enforce hospital policies; secondly, to improve the quality of medical care; third, to collect sufficient, adequate data for EHR in the near future. Among the proposed procedures, NTUH decides to establish a web-based mobile electronic medication administration record (ME-MAR) system. The system, build based on the service-oriented architecture (SOA) as well as embedded the HL7/XML
standard, is installed in the Mobile Nursing Carts. It also implement accompany with the advanced techniques like Asynchronous JavaScript and XML (Ajax) or Web services to enhance the system usability. According to researches, it indicates that medication errors are highly proportion to total medical faults. Therefore, we expect the ME-MAR system can reduce medication errors. In addition, we evaluate ME-MAR can assist nurses or healthcare practitioners to admin-ister, manage medication properly. This successful experience of developing the NTUH ME-MAR system can be easily applied to other related system. Meanwhile, the SOA architecture of the system can also be seamless integrated to NTUH or other HIS system.
Keywords Patients’ safety. Quality of medical care . Electronic health records .
Mobile electronic medication administration record DOI 10.1007/s10916-009-9310-9
S.-H. Hsieh
:
C.-T. Tan:
S.-L. Hsieh:
F. LaiInformation Systems Office, National Taiwan University Hospital, Taipei, Taiwan
S.-H. Hsieh
:
P.-C. Shen:
K.-P. Hsu:
F. LaiDepartment of Computer Science and Information Engineering, National Taiwan University,
Taipei, Taiwan
F. Lai
Department of Electrical Engineering, National Taiwan University,
Taipei, Taiwan
S.-L. Hsieh
Network and Computer Centre, National Chiao Tung University, Hsin Chu, Taiwan
F. Lai
Graduate Institute of Biomedical Electronics and Bioinformatics, National Taiwan University,
Taipei, Taiwan I.-C. Hou
Department of Nursing, National Taiwan University Hospital, Taipei, Taiwan
P.-H. Cheng
Software Engineering Department, National Kaohsiung Normal University, Kaohsiung, Taiwan
S.-H. Hsieh (*) Information Department,
National Taiwan University Hospital No.7, Chung-San South Road,
Taipei, Taiwan
Introduction
The trend of health information system
In last two decades, many hospitals have applied informa-tion system to aid the medical, nursing, and administrative staff for daily routine operations. It is not only for the convenience of the hospital staffs, but also for better medical quality of patient cares. However, the aspects of the information system related to the hospitals in the past may be different from those at current. The goal of health information systems was and is as simple as relevant: to contribute a high-quality, efficient patient care [1]. There-fore, it is a patient-centered approach towards medical and nursing cares. In addition, the administrative and manage-ment tasks need to support those cares [2].
As mentioned above, because of the transition, from traditional paper-based to computer-based, the Electronic Health Record (EHR) has become the most popular topic among medical informatics. By developing EHR, we can manage and retrieve patients’ health data easily, reduce paper usages. Health records are the critical assets of patients. Once all medical records are translated or trans-formed into EHR, the patients can easily carry their own data. The essence of developing HIS is in fact to improve safety over the health care institutions. Publication of the U.S. Institute of Medicine’s 1999 reported: “To Err is Human” [3]. By implementing the safety rule sets (for both medical, nursing staffs and patients) into HIS, computer can always notify the staffs without inducing errors. Further-more, once medical errors inevitably occur, HIS has the ability to collect those errors, then the researches can analyze them and stored in the HIS database. Later, the system can provide solutions, issue new rules and strate-gies, as well as indicate further modifications to make the system safer and more reliable.
NTUH present status
National Taiwan University Hospital (NTUH) has adopted healthcare information system for more than 25 years, and developed a new generation of HIS since 4 years ago. However, the health record is still paper-based due to ease of usage and legal reasons. In fact, currently we are still in a transition phase. Most patients’ data have been installed into the database, but portions of the medical processes have not been implemented in the NTUH HIS. Thus, not all legal health records are available in the system. Now, the EHR committee is taking charge of organizing standard processes for physicians prescribed data in NTUH. The committee decides what should be modified among the existing HIS subsystems and which subsystem should be constructed with additional, specific functionalities in order
to support EHR. Moreover, all the computerized data, collected during the processes, will be formalized into EHR in the near future to replace the current paper-based charts. Motivation and objective
As mentioned above, the EHR committee has sketched a complete plan of the flows of EHR orders. We plan to modify the existing systems or implement new ones to cover the entire process. The orders are prescribed, generated by the physicians initially, and the orders are received by the nurses. After the nurses review the orders, the nurses initiate and perform those orders. However, the nurses execute the orders written on papers. Thus, we need to develop new systems according to the EHR committee standards to assist the nurses’ operations electronically and with mobility. Before the NTUH electronic medical administration record system establishes, the orders are transcribed by hands or hard copies. The accuracy of the transcribed orders, records may induce errors or doubtable issues that need to prevent by the nursing staffs. Our objective is to construct the mobile electronic medication administration record system (ME-MAR) to complete the closed-loop medication administration system, and then to achieve the entire process computerized. To reduce human involvements can decrease human errors, so as to improve the medication safety.
In the following sections of the paper, we first elaborate the
related work and background at NTUH in “Backgrounds.”
Detailed design principles and features of ME-MAR are illustrated in “Mobile electronic medication administration record.” In “Preliminary system asessments,” the preliminary
system assessment is provided. Finally to conclude in “Conclusion and discussion.”
Backgrounds
NTUH health information system
NTUH is an education, medical center in Taiwan with large scale. There are approximately 8,000 outpatients per day, and the hospital has 2,200 beds for inpatients. The number of staffs is more than 5,000. As numerous patients and staffs in the hospital, we need to construct a reliable, effective information system to provide high quality of health care as well as to assist staffs’ daily routines. The legacy NTUH information system, developed by venders mainly, has been incompatible with current technologies. It is difficult to manage or control by NTUH. In addition, the cost of maintenance, provided by venders, is a great burden for NTUH. Therefore, the department of information in the hospital has begun to develop our own HIS 4 years ago; the
processing is still carrying on. The NTUH HIS encom-passes many subsystems, i.e., clinics, medical report, pharmacy, pathology, etc. as well as vender developed subsystems [4]. Those subsystems will be replaced by our own newly, implemented ones in the near future.
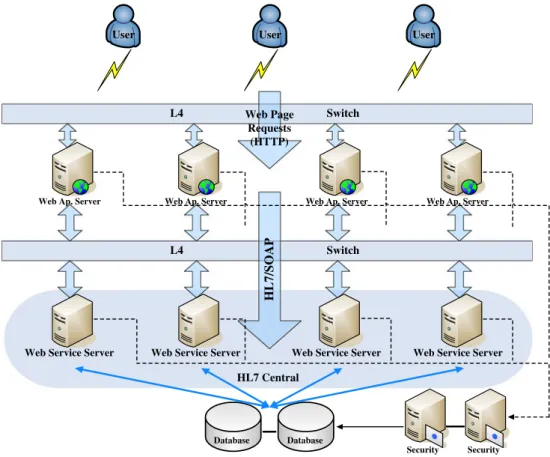
The new HIS system developed by the department of information are deploying under advanced technologies to enhance flexibility, efficiency, and ease of maintenance, using service oriented architecture (SOA) over web services in a wired, wireless environment. The over all architecture of the NTUH HIS with multi-tier is shown in Fig.1. The system separates user interfaces, subsystems and database accessing in layers to ensure data security and integrity [5]. In the diagram, the Web Services Servers represent the subsystems. Moreover, the single-sign-on mechanism, navigating via the subsystems, is included, by controlling the accessibility of every single web page for every user [6]. The healthcare certification IC card for validation during the login processes is also enclosed in the HIS.
In the NTUH HIS, the most important system is Health Level Seven (HL7) [7] Central. It takes the responsibilities to exchange data among the subsystems, i.e., Web Services Servers. As long as the subsystem communicates according to the HL7 standards, despite the platform based upon, it can exchange data correctly in the HIS [8]. In Fig. 1, it also indicates that the HIS is heavily dependent on web accessing
by either wireless or wired front-ends, users. To expedite the processes, an efficient web adaption technique is essential. The issue will be addressed in the design approaches later. The collaboration workflow with ME-MAR
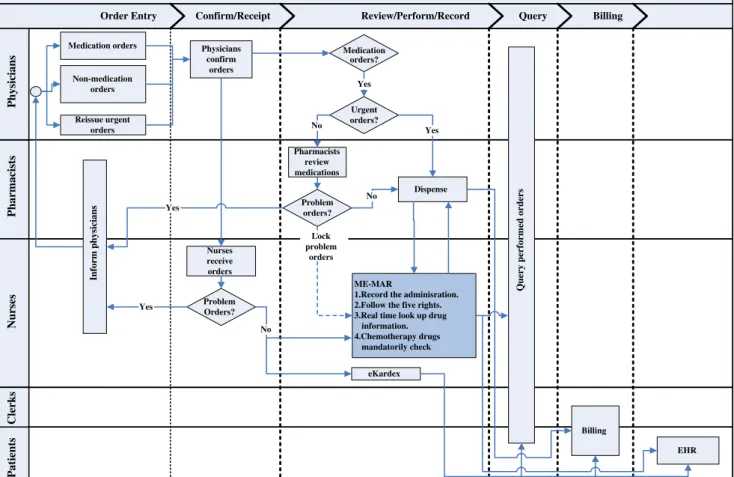
Through the process of health care, the orders pre-scribed by the physicians are the initial bases. Any examination, inspection, and dispensing are made after the orders generated. Therefore, to establish the medical records is the process after receiving the orders. The EHR committee proposed a flowchart of the prescribed
orders in NTUH, shown in Fig. 2. There are five steps
included and five characters or roles involved in the workflow. The five steps are: order entry, confirm/ receipt, review/perform/record, query, as well as billing. The five roles are: physicians, pharmacists, nurses, clerks, and patients. In the diagram, physicians generate, enter the orders. After confirmed the correctness of the orders, the pharmacists dispense the prescriptions with care. In the meanwhile, the ME-MAR system, planned to develop in the HIS, provides services: recording the administration flows electronically; looking up or searching prescribed drugs or doses dynamically; veri-fying chemotherapy drugs mandatorily in real time. The nurses distribute the medicine in wireless, mobile
Database Database
Web Ap. Server Web Ap. Server Web Ap. Server Web Ap. Server
Web Service Server Web Service Server Web Service Server Web Service Server
L4 Web Page Switch Requests (HTTP) L4 Switch HL7/SOAP Security Security HL7 Central
User User User
Fig. 1 NTUH HIS hardware architecture
nursing carts to the associated patients. The clerks calculate the billing; the patients pay the corresponding bills and can receive their own EHR.
Currently, only the computerized provider order entry (CPOE) has been implemented. Both the out-patient and the in-patient systems use the CPOE for diagnosing, prescribing, and other medical acts embedded in ME-MAR. The CPOE can assist the physicians, make their routines more efficient and reduce the medical errors occurrence. One study indicates the rate of serious
errors fall 55% [9], another study shows the rate of
overall errors fall 83% [10]. The reasons for computer-izing of prescribing orders can improve safety are: first, all orders are formatted, so that they must include a dose, route, and frequency; secondly, they are legible and the orders can be identified under all instances; third, information can be provided to the physicians during the prescription; and fourth, all orders are checked for hidden problems including allergies, drug interactions, overly high dose, drug-laboratory problems, as well as whether the dose is appropriate for liver or kidney functions [11].
Enhancement of the web developing
Because NTUH adopts web service, it is very important to avoid the web inherent shortcomings. Asynchronous Java-Script and XML (Ajax) is a popular technique in recent years, and adopting Ajax can significantly improve front-end users [12].
By introducing Ajax technique can eliminate the start-stop-start-stop nature interactive style of web application. From software architecture view, using Ajax is to add intermediary layer between the user and the server, and it seems making the Ajax application slower and less responsive, but actually it does not. When it starts to load an Ajax page, the server only initializes few data, and the most logic of the Ajax page is directly downloaded to the client, so the user would feel the Ajax page responses instantly. When the Ajax page is completely downloaded, the “Ajax” engine, it actually is written in JavaScript, communicates with the server, renders the interface, and prepares all the data needed by the Ajax page. The Ajax engine allows any interaction of the user happening asynchronously rather than communicating with the server via every single action. In this way, the client side
Order flow of the Electronic Health Record (EHR)
Order Entry Confirm/Receipt Review/Perform/Record Query Billing
Pharmacists Nurses Physicians Medication orders Non-medication orders Reissue urgent orders Physicians confirm orders Nurses receive orders Problem Orders? Inform physicians Yes Problem orders? Yes ME-MAR
1.Record the adminisration. 2.Follow the five rights. 3.Real time look up drug
information. 4.Chemotherapy drugs mandatorily check eKardex Lock problem orders Pharmacists review medications Urgent orders? Dispense Medication orders? No Yes No No
Query performed orders
Yes
Billing
EHR
Clerks
Patients
can handle almost any logic of a task, such as simple data validation, editing data in memory, etc. The server side only takes responsible for data exchanging between database and other complex data processing. In fact, according to our experience in NTUH, the users do not aware of the page “refresh” more than waiting. More precisely speaking, waiting cannot be totally eliminated. But by applying Ajax, refresh can be totally eliminated unless users want to do that. Although waiting cannot be eliminated, the waiting time can be reduced.
Mobile electronic medication administration record Architecture overview
The ME-MAR System is one of the subsystems of NTUH HIS as mentioned in“Backgrounds.” We separate the access of
database from user interfaces and the application logics. Moreover, in order to control the accessibility, the system architecture also includes session services. Figure3 shows the three components of the system architecture: ME-MAR (web application server), session services, and HL7 Central. In the diagram, the session services implement the login validation including authentication and authorization. The functionalities of the ME-MAR subsystem have been
described clearly in “The collaboration workflow with
ME-MAR.” The HL7 Central glues the ME-MAR subsystem with
all other HIS subsystem via HL7 communication standards. The front-end users are mainly designed for nurses moving mobile nursing carts and performing the prescribed orders for daily operation or routines as mentioned in the previous sections. The wireless techniques are based upon WLAN 802.11a; the client browsers reside in Notebooks.
The design principle of ME-MAR
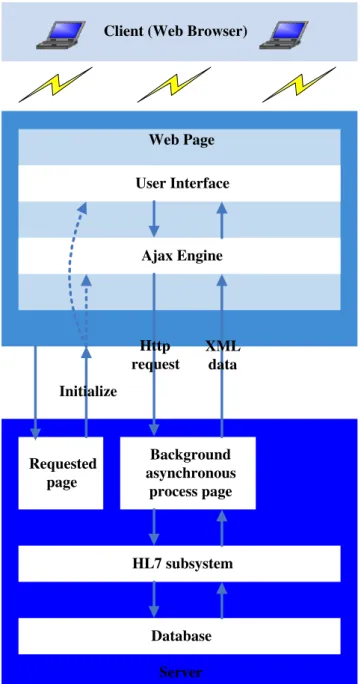
We introduced Ajax to improve the development of web applications. When the requested page is downloaded, the JavaScript codes, contained in the page, will render user interfaces and process data at background, thus the users only see the phenomenon of“flash” while the page is being
loaded. Figure 4 depicts the principle of our ME-MAR
Ajax approach.
The Ajax technique can also reduce the users’ waiting time, for example, our EMAR needs to prepare data for 3 days, and we can query data of the selected date first, and then query the data of the other 2 days in background. If we use the traditional approach for our program, the users need to wait for the data of 3 days, and it must be longer than wait for data of 1 day. The Ajax technology can provide the flow, feature for ME-MAR.
Web Ap. Server Web Ap. Server
ME-MAR Authentication Servive Authorization Service Session Services Check Session Session OK Check Permission Permission OK Security Database DataBase DataBase HL7 Library Request HL7 Response HL7 HL7 Library Receive HL7 Reply HL7
Web Service Server Web Service Server
HL7 Central
User
User
User Fig. 3 NTUH mobile electronic
medication administration record system architecture
Medication administration
Nurses are recognized as the “last line of defense” in
preventing medication errors made by pharmacists and physicians [13]. The main reasons of medication errors are: wrong route, wrong dose, wrong time, wrong drug, wrong frequency, wrong patient, without administering, ignore cosigning administration, prepare wrong diluted solution, wrong setting of devices, not comply with act (i.e. administer the drug which is only able to be administered by physician) [9]. The medication administration proce-dure that has been taught for many years is focused on the five rights: right patient, right drug, right dose, right
route, and right time [14]. The ME-MAR system must
support the five rights as possible, and comply with NTUH local policies: one sign of one case which means the nurses administer one patient at a time. Previous paper-based sheet has a biggest shortcoming, because every station prints the sheets of patients once a day, but in real clinical situations, orders might be deleted, and modified after the sheets were printed, so the nurses must transcript new orders by hands, and this action is very error-prone, besides transcription is much more time consuming than computers directly transcript orders to ME-MAR system, moreover sometimes the nurses might waste more time to figure out what illegible handwriting was supposed to. In order to reduce human errors, during the workflow of medical care manual steps must be reduced, so we want to construct a comprehensive comput-erized closed-loop medication administration system. Until now, NTUH HIS still lacks ME-MAR system to complete the closed-loop medication administration system.
Detailed features and functionalities of ME-MAR system in NTUH
Record the administration
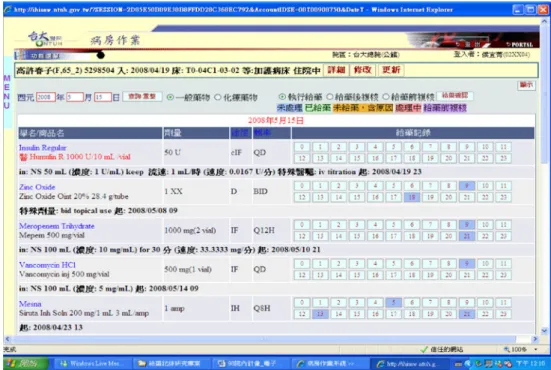
The main purpose of ME-MAR is to record the data of patients’ medication administration, the nurses need to record the administration which has already been given to the patients. In our design, the system will present the default timeslot by filling the buttons with blue accord-ing to the route code and frequency as depicted by
Fig. 5. In most cases, the nurses will administer
medications to patients in the default timeslot, but in some other cases, the nurses might administer medications later or earlier, because of many other possible clinical situations.
Follow the five rights of medication
Our system provides nurses with patient’s personal data includes patient’s name, drug name includes generic name and trade name, dose for single usage, route code, and system can calculate default time of administration accord-ing to order frequency; so our system is fully followaccord-ing the five rights of medication.
Highly warning drugs remind
As Fig. 6 shows, for those highly warning drugs, our
system displays the generic name with red to notify nurse they must carefully administer this medication to avoid medical errors or damage to patients; highly warning drug such as“Potassium Solution”.
Requested page Ajax Engine Background asynchronous process page Http request XML data User Interface Initialize Database HL7 subsystem Server Web Page Client (Web Browser)
Provide special orders
Sometimes physicians would give additional direction of the drug they prescribed, for example, before administering blood glucose drugs, nurses should administer appropriate dose according to glucose value level. Besides, there are some special order frequencies, e.g. ASORDER, when physicians prescribe such frequency, they will give addi-tional direction about the time of administration.
New and deleted orders remind
In real clinical situation, physicians may prescribe new orders or modify some active orders anytime as needed, so when the nurses review patients’ order lists, they must be able to know that there are new orders need to be done or no more perform those old orders. So we implement the mechanism to highlight the new orders, this makes sure that the nurses will note the new orders and perform them immediately if necessary. Fig. 5 The snapshot of record
the administration
Fig. 6 The snapshot of highly warning drugs remind
Easily display the details of the administration
If the nurses would like to know the details of a medication administration of particular some timeslot, they do not need to double click the button to show edit panel and then view all of the information, instead the nurses just need to move the cursor over the button, and all of the information will show under the cursor, including dose, dose unit, the reason if did not give drugs to the patients, the name of the nurse who signed for the record, name of the nurse who cosigned for the record before giving drugs, time of cosigning for the record before giving drugs, name of the nurse who cosigned for the record after giving drugs, time of cosigning for the record after giving drugs, and ME-MAR. Real time lookup drug information
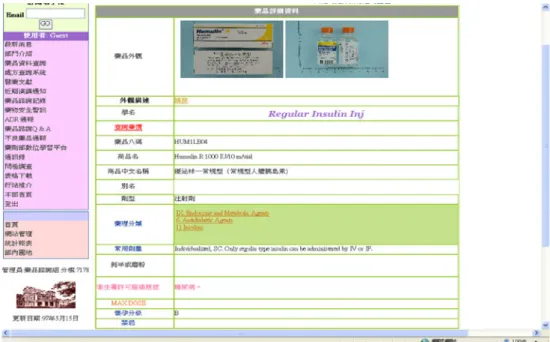
Unlike the previous paper records, the online system can provide real-time lookup drug information, this functionality can significantly improve medication safety, because all the details of a drug are available if the nurses are not familiar with any drugs, they can look up for it, and avoid give wrong drugs to the patients, at the same time, the nurses can increase their knowledge about the drug. Figure7presents the snapshot. Sort orders by route or frequency
In order to facilitate works, the nurses would view orders sorted by specific fields on the order list, they would like to check the orders with the same frequency or same route listed together, so that they can prepare the medications which should be administered at the same time or same
route. This convenient functionality can be achieved easily by programs, but it is impossible for paper sheets.
Cosign before and after administering
In order to enhance medication administration safety, when the nurses are going to administer medications to the patients, sometimes there are other nurses except the nurse who administers the medication to check orders and drugs, then give the drugs to the patients. The system does not allow the administering nurse cosigns for his or her own administration, i.e. the cosigner and administering nurse must be different.
Chemotherapy drugs mandatory check before administering
The usage of chemotherapy drugs is very critical for patients’ safety, any miss using will cause great damage to patients, so we implement a mechanism to enforce administering chemo-therapy drugs to follow three steps: chemochemo-therapy drug order review, chemotherapy drug administration review, and che-motherapy drug administration.
Check single administration dose and daily dose limitation We implement the mechanism to limit the administration dose, nurses cannot administer dose that exceed order dose in single administration, because they should not violate physicians’ orders, if necessary, physicians should modify or prescribe new orders rather than nurses sign an over dose administration.
Fig. 7 The snapshot of highly warning drugs remind
Support to prepare drugs
Before the nurses administer medications to the patients, they will prepare all drugs of one patient into his or her drug box, and in order to let the nurses know what drugs have already been prepared, we implement the mechanism to record those drugs have been prepared, but this is just auxiliary functionality, the preparation records are not formal clinical data.
Medication administration record summary print
Because of policy and legal reason, we still print all the mobile electronic medication administration records into paper sheets for patients’ health records at present. We are now in a phase transition, and it is hard to dispose paper-based record suddenly. Although we still need to print the records into paper sheets, but the quantities are greatly reduced, because previous paper-based records are printed every day, and it has to reserve much space for nurses administering, writing. After adopting ME-MAR, the paper sheets of medication administration records are printed only when the patients transfer wards or discharge, and the sheets leave no space for writing, so that we can reduce paper usage of medication administration records.
Preliminary system assessments
For ME-MAR system evaluation, we followed the three factors proposed by the Medication Administration System— Nurses Assessment of Satisfaction (MAS-NAS) Scale [15]. The three factors are: (a) efficacy, dependability and effectiveness of the system: including efficiency, user-friendliness, readiness, supplies availability, error prevention or reduction, as well as adequate turnaround time; (b) safety of the system components: encompassing assuring nurses issue administering medication correctly, pharmacists vali-dation of medicines, agreements among physicians and pharmacists in terms of prescriptions, ease of double checking, drug alert features, following the five rights, as well as healthcare practitioners coordinating; and (c) accessing
or having relevant information and medications at hand immediately: containing ease of searching data about drugs, controlling, managing medication reactions and knowledge of intended or side effects, operating adequate systems, and locating medications promptly [16]. In addition, we exam-ined the system success evaluation framework according to
DeLone and McLean [17], and focused on evaluating the
essential system characteristics of ME-MAR as well as its impacts on user performance. For the benchmark purpose, we included a paper-based workflow commonly used by nursing professionals during their analysis routines.
Evaluation
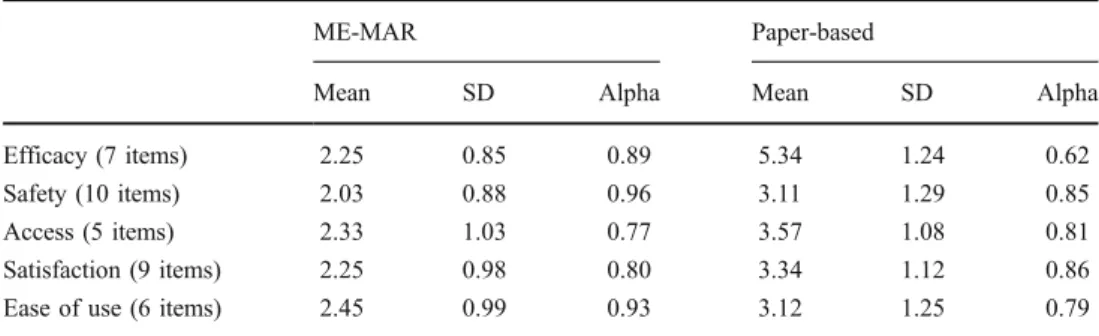
A total of 45 nursing practitioners participated in the evaluation. Among them, 22 subjects operated ME-MAR system, and 23 subjects used paper-based flows. We applied a randomized, cross-group design in the evaluation. In addition, we examined the reliability or our items by assessing its internal consistency [18]. Table1 summarizes the summary of statics of the subject’s responses, Cronbach’s alpha value [19]. It indicates the items almost construct to exceeding the commonly suggested alpha value threshold 0.8 [19].
Results
As the evaluation design, we therefore, defined the following hypotheses, evaluated the system accordingly, and obtained the corresponding results as listed in the sections below respectively.
Efficacy
The inherent shortcoming of web page is the phenomenon of“flash”, but we introduce new technique, Ajax, to avoid this shortcoming and achieving user-friendliness. We also test the system correctness for 2 months to make sure ME-MAR is able to record the administration correctly. We implement ME-MAR in a simple and straightforward approach; we believe that nurses are able to operate the system after quick education or training. There are
ME-MAR Paper-based
Mean SD Alpha Mean SD Alpha
Efficacy (7 items) 2.25 0.85 0.89 5.34 1.24 0.62
Safety (10 items) 2.03 0.88 0.96 3.11 1.29 0.85
Access (5 items) 2.33 1.03 0.77 3.57 1.08 0.81
Satisfaction (9 items) 2.25 0.98 0.80 3.34 1.12 0.86
Ease of use (6 items) 2.45 0.99 0.93 3.12 1.25 0.79
Table 1 Statics of the analysis results
descriptions of the colors which represent the status of administration. In addition, we implement sorted orders by route and frequency while supporting drugs preparation. H1 The task completion efficiency associated with ME-MAR is higher than that observed with the benchmark paper-based program.
Result Based on our analysis, the system indicates a significant main effect on task completion efficiency (p=.009). We compared the amount of time required to complete a task using the respective systems and found that, on average, subjects using ME-MAR could complete an analysis task considerably faster (mean=2.25 min, SD= 0.85 min) than their counterparts supported by the paper-based workflow (mean= 5.34 min, SD=1.24 min); the difference was significant at the 0.01 level. Thus, our data supported H1.
Safety
We design ME-MAR system followed the five rights of medication to enhance patients’ safety, and features and functionalities to facilitate safety: highly warning drugs reminding, special orders, new and deleted orders remind-ing, cosign before and after administerremind-ing, chemotherapy drugs mandatory checking before administering, and verifying single administration dose and daily dose limitations. To examine the hypotension and the result indicated as below:
H2 The safety improvement that results from the use of ME-MAR, as compared with the benchmark paper-based workflow, increases with task complexity.
Result The effect of system on patient safety was significant statistically (p=.006). Our subjects considered ME-MAR easier to use (mean=2.03, SD=0.88) than the paper-based workflow (mean=3.11, SD=1.29). The cross-groups differ-ence in safety issue was significant at the 0.01 level. Therefore, our data supports H2.
Access
The ME-MAR System is an independent page pop up from the original web page, so if the nurses need to look for other information in NTUH HIS, they can continue their medication administration concurrently. In addition, the real time lookup drug information functionality is also a new pop up window provided by the department of pharmacy. Nurses are able to search for drug information and keep
their medication administration operations. The hypothesis and result showed as following.
H3 The access of ME-MAR, as perceived by an individual, is significantly greater than that of the benchmark paper-based workflow.
Result Our analysis concludes that the system had a significant effect on access of ME-MAR (p=.045). Overall, our subjects considered ME-MAR more access for support-ing their analysis tasks (mean=2.33, SD=1.03) than the paper-based workflow with (mean=3.57, SD=1.08). The observed cross-groups difference was statistically signifi-cant at the 0.05 level. Thus, our data supports H3.
User satisfaction
User satisfaction is a fundamental aspect of system evaluation and embraces user information satisfaction
emphasizing information requirements [20]. Because of
the critical importance of information support in the HIS system, we explicitly focused on user information satisfac-tion and verified the following hypothesis.
H4 The user information satisfaction that results from the use of ME-MAR is significantly higher than that observed with the benchmark paper-based workflow.
Result According to our analysis, the main effect of the system on user information satisfaction was significant statistically (p=.036). Overall, subjects using ME-MAR exhibited higher satisfaction with the information support (mean=2.25, SD=0.98) than their counterparts supported by the paper-based workflow (mean=3.34, SD=1.12); the difference was significant at the 0.05 level. Thus, our data supports H4.
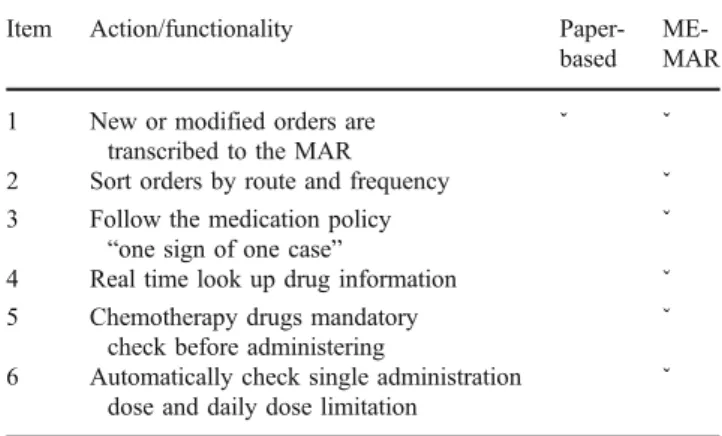
Table 2 Samples of differences between ME-MAR and the paper-based
Item Action/functionality
Paper-based ME-MAR 1 New or modified orders are
transcribed to the MAR
ˇ ˇ
2 Sort orders by route and frequency ˇ
3 Follow the medication policy
“one sign of one case” ˇ
4 Real time look up drug information ˇ
5 Chemotherapy drugs mandatory check before administering
ˇ 6 Automatically check single administration
dose and daily dose limitation
Ease of use
Perceived ease of use refers to the degree to which an individual considers his or her usage of a system to be free of effort [21]. Ease of use represents an essential motivation for individuals’ voluntarily use of the system [22], and can affect their adoption decisions significantly [23]. Hence, we tested the following hypothesis, and analyzed the result. H5 The ease of use of ME-MAR, as perceived by an individual, is significantly greater than that of the paper-based workflow.
Result According to our analysis, the effect of system on perceived ease of use was significant statistically (p=.039). Our subjects considered ME-MAR easier to use (mean= 2.45, SD=0.99) than the paper-based workflow (mean= 3.12, SD=1.25). The cross-groups difference in perceived ease of use was significant at the 0.05 level. Therefore, our data supports H5.
Comparison
Table 2 outlines the some differences between the
ME-MAR and paper-based workflow. Item1 is enhanced by implementing ME-MAR; Item 2 is for user-friendly; Item3 to item 6 are new functionalities to promote safety.
Conclusion and discussion
We have developed the Mobile Electronic Medication Administration Record System to aid the nursing staff for administering medication. We must emphasize that the main purpose the ME-MAR system is to promote patients’ safety. In addition, there is a further benefit of the system, that is, NTUH started to establish the electronic health record recently, and the medication administration record is an essential part of health record. Therefore, after we constructed the ME-MAR system, all of the patients’ medication administration data are stored in NTUH HIS. Furthermore, once the electronic health record is installed, the medication administration data is available automatically.
The evaluation results of the nurses’ satisfaction indicate that, in general, respondents are more significantly regard-ing to the ME-MAR system. We will also collect the users’ suggestions to modify the current ME-MAR in order to coordinate with their requirements. Moreover, we can combine with the RFID mechanism to further improve the system, because using machines to scan patients’ tags is conducive to identify patients correctly. The system can automatically search for patients’ ME-MAR.
As mentioned in “Backgrounds,” our goal is to
imple-ment all procedures in the order flow of HER. We have already begun to develop advanced CPOE currently; the advanced CPOE basically depends on ME-MAR, but it deals with variations of orders. ME-MAR handles medica-tion orders, and the advanced CPOE controls non-medication orders. The two systems cover the order flow of performing and recording; these are the essences of nurses’ daily operations. Another important procedure is pharmacists review medication orders, because pharmacists are experts of medication. If all medication orders are reviewed by them, when they discover problems, they can directly lock the problematic orders, and nurses will not be able to propagate the errors. The mechanism provides higher safety to patients.
The systems we developed, implemented can facilitate entire medical staff for their operations in NTUH, and improve patients’ safety as well as the quality of medical cares. This successful experience of developing NTUH ME-MAR system can be easily applied to other related system. Meanwhile, the SOA architecture of the system can also be seamless integrated to NTUH or other HIS system.
References
1. Haux, R., Winter, A., Ammenwerth, E., and Brigl, B., Strategic information management in hospitals”, An introduction to hospital information systems. Springer, New York, 2004. 2. Haux, R., Health Information System—past, present, future. Int. J.
Med. Inform. 75:268–281, 2006. doi:10.1016/j.ijmedinf.2005.08.002. 3. Kohn, L., Corrigan, J., and Donaldson, M. (eds.), To Err is Human, National Academy Press for the U.S. Institute of Medicine, Washington, 1999.
4. Yang, T. H., Cheng, P. H., et al., A scalable multi-tier architecture for the National Taiwan University Hospital Information System based on HL7 Standard. IEEE, Washington, D.C., 2006. 5. Hsieh, S. H., Hsieh, S. L., Weng, Y. C., et al.,“Middleware based
Inpatient Healthcare Information System”, Bioinformatics and Bioengineering, BIBE 2007, Proceedings of the 7th IEEE International Conference, pp. 1230–1234, 2007
6. Weng, Yung-Ching, Hsieh, Sheau-Ling, Hsieh, Sung-Huai, and Lai, Feipei, Design and Enhance a Dynamic Healthcare Portal Site. Web Intelligence and Intelligent Agent Technology Workshops, 2007 IEEE/WIC/ACM International Conferences, pp. 173–176, 2007. 7. Health Level Seven (HL7), HL7 Standard v.2.5, 2003.
8. Li-Fan Ko, Jen-Chiun Lin, et al., HL7 Middleware Framework for Healthcare Information System. HEALTHCOM 2006, 2006. 9. Bates, D. W., Leape, L. L., Cullen, D. J., Laird, N., Petersen, L. A.,
Teich, J. M., et al., Effect of computerized physician order entry and a team intervention on prevention of serious medication errors. JAMA. 280:1311–1316, 1998. doi:10.1001/jama.280.15.1311.
10. Bates, D. W., Teich, J., Lee, J., Seger, D., Kuperman, G. J., Boyle, D., et al., The impact of computerized physician order entry on medication error prevention. J. Am. Med. Inform. Assoc. 6:313– 321, 1999.
11. David, W., Bates, Using information technology to reduce rates of medication errors in hospital. BMJ. 320:788–791, 2000. doi:10.1136/bmj.320.7245.1337.
12. Garrett J. J., Ajax: A New Approach to Web Application.http:// www.adaptivepath.com/ideas/essays/archives/000385.php, 2005. 13. Hurley, A. C., Bane, A., Fotakis, S., Duffy, M. E., Sevigny, A.,
Poon, E. G., and Gandhi, T. K., Nurses’ satisfaction with medication administration point-of-care technology. J. Nurs. Adm. 37:343–349, 2007. doi:10.1097/01.NNA.0000285114. 60689.02.
14. Eisenhauer, L. A., Hurley, A. C., and Dolan, N., Nurses’ reported thinking during medication administration. J. Nurs. Scholarsh. 39:82–87, 2007. doi:10.1111/j.1547-5069.2007.00148.x. 15. Hurley, A. C., Lancaster, D., Hayes, J., Wilson-Chase, C.,
Bane, A., Griffin, M., Warden, V., Duffy, M. E., Poon, E. G., and Gandhi, T. K., The medication administration system— nurses assessment of satisfaction (MAS-NAS) scale. J. Nurs. Scholarsh. 38:298–300, 2006. doi:10.1111/j.1547-5069.2006. 00117.x.
16. Rocheleau, B., Evaluating public sector information systems: Satisfaction versus impact. Eval. Program Plann. 16:119–129, 1993. doi:10.1016/0149-7189(93)90023-2.
17. DeLone, W. H., and McLean, E. R., The DeLone and McLean model of information systems success: A ten-year update. J. Manage. Inf. Syst. 19:9–30, 2003.
18. Straub, D. W., Validating instruments in MIS research. Manage. Inf. Syst. Q. 13:147–169, 1989. doi:10.2307/248922.
19. Cohen, J., Applied multiple regression/correlation analysis for the behavioral sciences. Erlbaum, Hillsdale, 1983.
20. Ives, B., Olson, M., and Baroudi, J. J., The measurement of user information satisfaction. Commun. ACM. 26:785–793, 1983. doi:10.1145/358413.358430.
21. Davis, F. D., Perceived usefulness, perceived ease of use, and user acceptance of information technology. Manage. Inf. Syst. Q. 13:319–339, 1989. doi:10.2307/249008.
22. Venkatesh, V., Determinants of perceived ease of use: Integrating control, intrinsic motivation, and emotion into the technology acceptance model. Inf. Syst. Res. 11:342–365, 2000. doi:10.1287/ isre.11.4.342.11872.
23. Lee, Y., Kozar, K., and Larsen, K., The technology acceptance model: Past, present, and future. Commun. AIS. 12:752–780, 2003.