行政院國家科學委員會專題研究計畫 成果報告
外傷出血性休克所導致發炎反應與基因體表現之性別差
異—使用 Metoclopramide 介入來改善發炎反應與器官衰竭
計畫類別: 個別型計畫 計畫編號: NSC93-2314-B-039-024- 執行期間: 93 年 08 月 01 日至 94 年 10 月 31 日 執行單位: 中國醫藥大學附設醫院外科部 計畫主持人: 陳瑞杰 共同主持人: 蔡世峰,樓迎統 計畫參與人員: 鍾侑庭,謝曉嵐 報告類型: 精簡報告 處理方式: 本計畫可公開查詢中 華 民 國 95 年 2 月 21 日
;
成 果 報 告
行政院國家科學委員會補助專題研究計畫
期 中 進 度 報 告
The Gender Dimorphism of Inflammatory Response Following
Traumatic Hemorrhagic Shock: A study based on its functional genomics and
validation of a novel therapeutic approach for post-traumatic multiple organ
failure by hormonal modulation (The second year)
大白鼠外傷性出血性休克後炎性反應在性別差異上之研究:
基於功能性基因體學並應用賀爾蒙調節來治療因創傷導致多重器官衰竭之嶄
新療法的研究
(第二年)
計畫類別:■ 個別型計畫 □ 整合型計畫
計畫編號:NSC92-2314-B -182A-157
執行期間:92 年 8 月 1 日至 94 年 7 月 31 日
計畫主持人:陳瑞杰
共同主持人:
計畫參與人員: 鍾侑庭、謝曉嵐
成果報告類型(依經費核定清單規定繳交):□精簡報告 ■完整報告
執行單位:中國醫藥大學附設醫院
中 華 民 國 年 月 日
The Gender Dimorphism of Inflammatory Response Following Traumatic
Hemorrhagic Shock: A study based on its functional genomics and validation
of a novel therapeutic approach for post-traumatic multiple organ failure by
hormonal modulation (The second year)
大白鼠外傷性出血性休克後炎性反應在性別差異上之研究
─基於功能性基因體學並應用賀爾蒙調節來治療因創傷導致多重器官衰竭之
嶄新療法的研究
(第二年)
Ray-Jade Chen, M.D., Yu-Ting Chung, M.D.,
Center of Emergency and Trauma Chinese Medical University Hospital,
中英文摘要: (一)計畫中文摘要 關鍵詞: 性荷爾蒙,多重器官衰竭,外傷性出血性休克, RNA 微陣列,信使核糖核蛋白, 細胞激素,Metoclopropamide。 背景:在第一年的研究中我們發現外傷性出血性休克使血清中炎性反應細胞激素的濃度明 顯增加;而以輸液及輸血的急救治療則上述的反應明顯降低。其中雌性的變化較小,顯示 雌 激 素 對 炎 性 反 應 的 確 有 調 節 的 作 用 , 這 樣 的 發 現 符 合 其 他 相 關 研 究 的 結 果 。 Metoclopramide(MCP)之使用能明顯地增加體內泌乳激素(prolactin)之分泌與濃度。同時 Metoclopramide 也已被證明能恢復休克後被抑制之免疫反應,並能保護心血管與肝臟功 能。因此,在第二年計劃中嘗試使用Metoclopramide 來介入 (intervention) 外傷性出血性休 克後之復甦治療。 目的:以Metoclopramide 來介入(intervention)外傷性出血性休克後之復甦治療,並藉由微陣 列技術,全面瞭解出血性休克導致基因體表現之變化在性別上的差異,並觀察基因體變化 與細胞層級變化及臨床指標,如:細胞激素與雌激素,以期找出其間之關連性。 方法:本實驗之對象為大白鼠,共分二組,每組 12 隻,雌雄各半。第一組:控制組(休克 及復甦治療),第二組:MCP 組(休克及復甦治療+ metoclopramide)。出血性休克採用抽血 2.5 毫升血液/公斤體重,並維持平均動脈壓為 45-55 毫米汞柱達一小時。實驗結束後四小時 給予安樂死,同時將大白鼠肝臟組織取下並且由心臟抽血。取出之肝臟組織立即放入-196 ℃液態氮急凍,再保存於-70℃之冰箱,直到接受微陣列之分析。各種血中細胞激素 TNF-α,IL-1β,IL-6 及 IL-10,同時雌激素(17β-estradiol)也予以檢測。 結果:兩組動物4 小時的存活率均為 100%。在雌激素方面,雌性明顯高於雄性,兩者有統 計學上的意義 (<0.005)。無論雌雄,以 metoclopramide 介入組(第二祖)均有較高的血清 細胞激素濃度及肝組織相對應mRNA 表現,但兩者增加的程度卻不一致。比較雌雄的差異 發現第二組雌性血清中細胞激素濃度均較雄性者有明顯的增高。在微陣列的實驗方面,大 白鼠基因晶片(GeneChip®)可檢測 31099 種基因,研究發現結果發現 1.1 %(323)的基因有 明顯改變,其中在雄性方面62 種基因強度增加,66 基因強度減少;在雌性方面 141 種基 因強度增加,55 基因強度減少。 討論:上述結果顯示 metoclopramide 對系統性炎性反應有促進的作用,對雌性的作用尤為 明顯。然而因兩組實驗動物四小時存活率為100%,這種促進作用,對外傷性出血性休克的 急救究竟是正面或是負面?在本實驗並無法得知。在微陣列的實驗,肝組織信使核糖核蛋 白(mRNA)的表現不能反映血清細胞激素濃度變化,究其原因有二:一、雖然肝臟在外傷性 出血性休克的系統性炎性反應中扮演重要角色,其mRNA 的表現仍只能代表局部的反應, 不能與代表系統性的反應的血清細胞激素的濃度等量齊觀。二、mRNA 在常溫很快就流失 掉,相信這是造成肝組織mRNA 表現量與血清細胞濃度變化量差異上最主要的原因。 結論:雖然由本實驗無法得知metoclopramide 介入對大白鼠外傷性出血性休克及急救的效 用,然而metoclopramide 的確對肝組織 mRNA 表現的調節及血清中細胞激素濃度的提升有 顯著的影響。要進一步釐清這種影響對外傷性出血性休克及急救是正面或者是負面,我們 有兩點建議:一、增加休克的嚴重度及休克時間,二、以不同劑量的metoclopramide 對外 傷性出血性休克(但無輸血或輸液)做介入治療。
(二)計畫英文摘要
Key words: Sex hormone,Multiple organs failure,Traumatic hemorrhagic shock, RNAmicroarray,mRNA,Cytokine,Metoclopropamide。
Background:In the first year study, we found that there had significant increase of plasma level of cytokines, including TNF-α、IL-1β、IL-6 and IL-10, after traumatic hemorrhagic shock. In the contrary, the above response was markedly declined after blood and fluid resuscitation. Female sub-groups had more narrow change, implying that female sex hormone(estrogen)play an important role on modulation for imflammatory response, which was in accordant with the results of other related studies. Metoclopramide (MCP) is known to increase prolactin secretion and ultimately plasma prolactin levels. And its administration can restore the depressed cardiac and hepatocellular functions and downregulate inflammatory cytokine release after trauma-hemorrhagic shock.Therefore, we try to use metoclopramide for the intervention of traumatic hemorrhagic shock and resuscitation in the second year study.
Purpose:Under the application of microarray technology, we can have a global understanding of the pattern and difference of immune restoration and gene expression following traumatic hemorrhagic shock in the male and female rats. We also want to correlate these observed gene expressions with cellular change and clinical parameters such as hormone levels and serum cytokine concentrations.
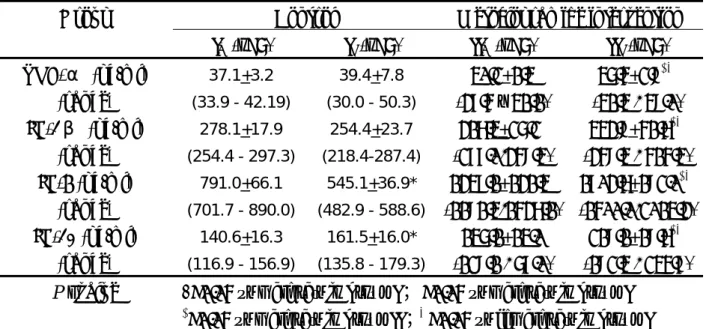
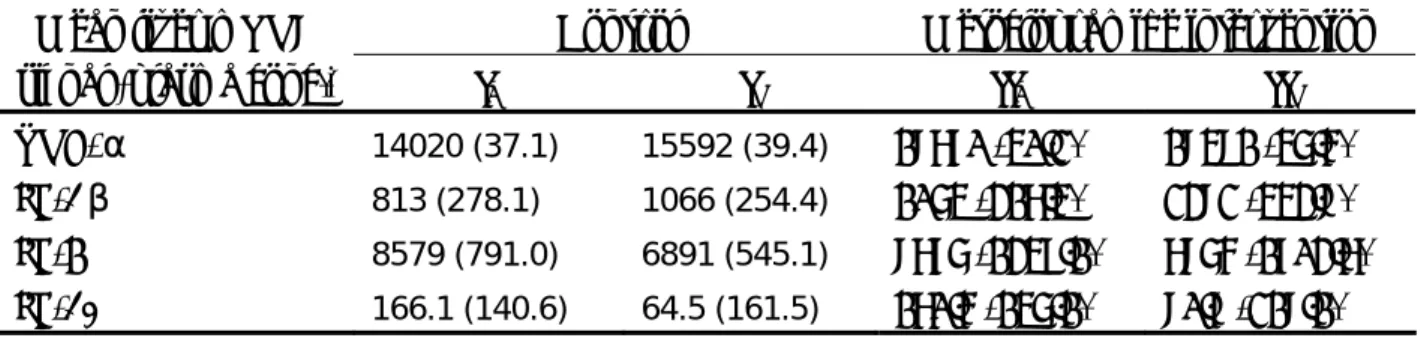
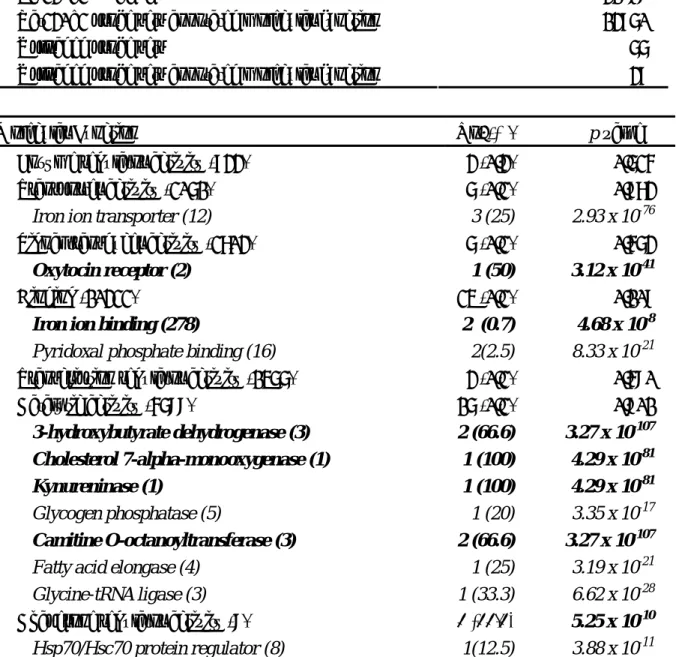
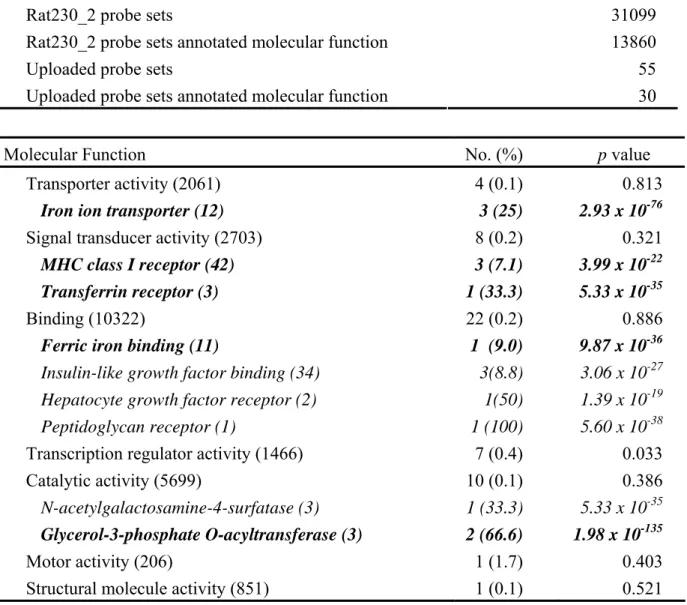
Methods:In our study, mature Sprague-Dawley rats with half for each sex, will be divided into three groups, each group having 12 rats. Group I: control group (sham operation). Group II:hemorrhagic group (sham operation + shock). Group III:resuscitative group (sham operation + shock+ resuscitation). Hemorrhagic shock will be induced by withdrawing 2.5 mL blood/kg body weight for 10 minutes. After shock, animals are resuscitated with the shed blood and lactated Ringer’s (RL) solution (2 times the shed blood volume, 5 mL/kg/h). The animals will be sacrificed by euthanasia at 4 hrs after the finish of experiment to obtain the liver and whole blood. The liver sample will be harvest and frozen rapidly in liquid nitrogen (-196℃) and storage at refreezer (-70℃) until microarray and pathological analysis. The cytokines including TNF-α,IL-1β,IL-6 及 IL-10, as well as 17β-estradiol will be measured through the blood samples. Results: The 4-hour survival rates were 100% in two groups.。In regard to 17-β estradiol, plasma levels in females were significantly higher than those in males (p<0.005). Regardless of sexes, metoclopramideintervention group(group II) had higher levels of cytokines in plasma and expression of corresponding mRNA in liver tissue. However, there was not in accordance in the degree of increment for the plasma levels of cytokines as compared with liver mRNA expression. As compared in gender difference, the female rats had significant higher plasma levels cytokines (p<0.05) in metoclopramide intervention group. In the microarray study, the GeneChip® revealed 1.1 % (323/31099) of assessed genes were altered in which 62 genes up regulated and 66 genes down regulated in male sub-group, 141 genes up regulated and 55 genes down regulated after metoclopramide intervention.
Discussion: The above results imply that metoclopramide has stimulating effect on the systemic inflammatory response, which is more prominent in female rats. However, we can not decide whether metoclopramide intervention is beneficial or harmful for traumatic hemorrhagic shock and resuscitation because all the experiment rats were survived for 4 hours after traumatic hemorrhagic shock. There are three reasons to demonstrate why the degree of change for the plasma level of cytokines were not in accordance with that of liver mRNA expression. First, althoug liver play an important role on the systemic inflammatory response after traumatic hemorrhagic shock, the expression of mRNA in liver tissue is merely a local response, in the contrary , the plasma level of cytokines represent the systemic response. Second, may be the most important, the mRNA degradates quickly in the room temperature due to short half life.
Conculsion: Although we can not decide whether metoclopramide intervention is beneficial or harmful for traumatic hemorrhagic shock and resuscitation, however, it is sure that metoclopramide has stimulating effect on the expresison of mRNA in liver tissue and cytokine leves in plasma。To verify whether it is beneficial or harmful if metoclopramide intervention for traumatic hemorrhqagic shock and resuscitation, we suggest 1. increase the severity and time of shock, 2. use different doses of metoclopramide intervention for traumatic hemorrhiagic shock, but not resuscitation with blood or fluid in the following study.
報告內容
z Introduction
[Trauma Epidemiology and Death]
Injury continues to be the leading cause of death in the first four decades of life, and remains the fourth to fifthth leading cause of death among persons of all ages in most developed countries including Taiwan.1-4 Because it is a “disease” of the young, trauma is responsible for loss of more years of productive life than any other illness. 4-9 In Taiwan, the Department of Health (DOH) reported total 9,513 trauma deaths on 2001. In fact, we have more than ten thousand annular trauma deaths in the last twenty years.3
Trunkey 10-11 reported the famous trimodal distribution of trauma death in 1983. In their study, the immediate and early deaths mostly resulted from neurologic dysfunction or major hemorrhage. Late deaths, those more than 1 week after injury, most commonly resulted from infection or multiple organ failure. Patients who survive the immediate consequences of their injuries and the accompanying loss of blood are susceptible to subsequent sepsis and multiple organ dysfunctions. 12 The mechanisms responsible for the development of multiple organ dysfunctions have not yet been established; nonetheless, it has been shown that macrocirculatory and microcirculatory disturbances are important factors in the pathogenesis of impaired organ and immune functions.13 It appears that after an initial insult such as hemorrhagic shock, the capacity of the cardiovascular and immune system to respond to a septic challenge is reduced, contributing to increased susceptibility to sepsis in trauma victims.
[Hemorrhagic shock]
Several studies in the past decade have investigated the effects of hemorrhagic shock alone or in conjunction with soft-tissue trauma (ie, laparotomy) on cell-mediated and humoral immunity.14-21 In this respect, a marked depression in specific and nonspecific immunity has been reported following hemorrhagic shock.14-15 These alterations in various organ (such as the cardiovascular, liver, gut, and adrenals) and immune functions are apparent immediately after hemorrhage (starting as early as 30 minutes after induction of hypotension), and they remains depressed for 24 hours in experimental rats.14, 16-18 Major blood loss has been also reported to induce endocrine alterations, including increased release of adrenocorticotropic hormone, corticosterone, and beta-endorphin.19
The response of the hormonal and inflammatory mediator systems in patients with hemorrhagic shock appears to represent a distinct set of responses different from those of other forms of shock.20,21 Activation of the systemic inflammatory response by hemorrhage and tissue injury is an important component of the pathophysiologic condition of post-injury hemorrhagic shock. Activators of this systemic inflammatory response include ischemia/reperfusion injury and neutrophil activation. Capillary "no-flow" with prolonged ischemia and "no-reflow" with reperfusion may initiate neutrophil activation in patients in hemorrhagic shock. The mechanisms that lead to decompensated and irreversible hemorrhagic shock include (1) "arteriolar
hyposensitivity" as manifested by progressive arteriolar vasodilation and decreased responsiveness of the microcirculation to alpha-agonists, and (2) cellular injury and activation of both proinflammatory and counterinflammatory mechanisms. These changes represent a failure of the microcirculation. Redistribution of cardiac output and persistent gut ischemia after adequate resuscitation may also contribute to the development of irreversible hemorrhagic shock.
Previous studies have shown that vascular endothelial cell dysfunction occurs during hemorrhagic shock and persists despite fluid resuscitation. Vascular endothelial cells play a critical role in the maintenance of tissue perfusion.55-57 Therefore, it is also important to investigate potential therapeutic approaches for maintaining endothelial cell function after hemorrhagic shock. One of the cornerstones in the management of trauma and hemorrhagic shock is the rapid replacement of the lost blood with fluid to maintain blood pressure and organ perfusion. However, despite seemingly successful resuscitation, a significant number of trauma patients who survive the initial insult develop sepsis and multiple organ failure later. 22-25
[Post-injury Multiple Organ Failure]
Most studies reported an incidence of multiple organ failure (MOF) in multiple trauma patients between 8 and 42%, depending upon the scoring system used and the study population.22-25 Sauaia et al. 24 described in a prospective study with 411 multiple trauma patients an incidence of MOF of 19% and a MOF-related mortality of 37%. Regel et al.23 in 1995 observed an incidence of MOF 8 to 28% with a mortality of 26 to 35% in 3,406 multiple trauma patients during an observation period of 20 years. Despite this intensive research interest, the incidence of post-injury MOF appears to be increasing as a result of optimized prehospital care and regional trauma system development, fewer critically injured patients are dying at the scene of their accident, and more are surviving the first 24 h of their trauma center care. Consequently, there are more ICU patients who are at high risk of MOF. Moreover, despite tremendous clinical efforts and basic applied research, there have been no new proven effective interventions for MOF in the past decade, and the mortality remains high (40-50%).22-25
[Pathogenesis of Post-injury MOF]
Over the past 25 years, significant research efforts have focused on the pathogenesis of post-injury MOF.26 In a 1975 editorial, Arthur Baue27 made the seminal observation that ICU patients were no longer dying of isolated organ failure, but rather of a new syndrome characterized by progressive sequential organ failure. Two years later, Ben Eiseman28 coined the term “multiple organ failure”(MOF) and identified the important risk factors to be preexisting disease, shock, and sepsis. Soon thereafter, Hiram Polk and Don Fry observed a consistent association between infection and MOF and concluded that MOF was the “fatal expression of uncontrolled infection”.29 As a result, research efforts in the early 1980s were focused on determining how the initial traumatic insult promotes infections and how these infections cause MOF. In the mid 1980s, observations from Europe by Eugene Faist 30 and Jan Goris 31 changed this research focus. They observed that a significant portion of blunt trauma patients who developed MOF did not have an identifiable infection. They concluded that MOF can occur as a
result of an “auto-destructive inflammatory response,” and research efforts subsequently refocused on explaining how a variety of noninfectious insults could cause systemic inflammatory response syndrome (SIRS) that would result in MOF independent of a bacterial infection.
The global hypothesis is that post-injury MOF occurs as a result of a dysfunctional inflammatory response. This occurs in a bimodal fashion; early MOF occurs as a result of an exuberant proinflammatory response, and late MOF occurs as a result of delayed immunosuppression and subsequent infections. After trauma, patients are resuscitated into a state of systemic hyperinflammation (i.e., SIRS). Mild to moderate SIRS is most likely beneficial (i.e., it is the normal injury stress response), but severe SIRS can precipitate early tissue injury, the severity of shock, and a variety of host factors. As time proceeds, negative feedback mechanisms down-regulate certain aspects of SIRS to restore homeostasis and potential auto-destructive inflammation. This compensatory anti-inflammatory response results in delayed immunosuppression. Again, mild to moderate immunosuppression is presumed to be beneficial, but when severe, it is associated with late infections (principally pneumonia) that can either worsen early MOF or precipitate late MOF.
[Gut Theory]
In the late 1980s and early 1990s, the experimental work at a number of trauma research centers persuasively focused attention on bacterial translocation (BT) as a unifying mechanism for MOF.32- 35 Alexander36 has defined bacterial translocation as “the passage of both viable and nonviable microbes and microbial products such as endotoxin across an anatomically intact mucosal barrier”. Although bacterial translocation was not a new concept in the late 1980s, it provided an enticing explanation of how traumatic shock could induce the “sepsis syndrome” (i.e., SIRS without an infection) that characterized early post-injury MOF.
More recently, laboratory studies have implicated that the gut is a cytokine-generating organ after shock-induced gut hypoperfusion37-39 and that gut-associated bacteria may play an important role in this inflammatory response40-41. For instance, Deitch and Chaudry37 found greater increases in IL-6 and TNF levels in portal vs. systemic circulation in rats subjected to hemorrhagic shock and resuscitation. The exact pathogenesis of post-injury MOF remains elusive and is undoubtedly multifactorial.
[Risk Factors of Post-injury MOF & Mortality]
Based on previous studies of Sauaia et al.24, age greater than 55 years, ISS greater than or equal to 25, and greater than 6 U RBC/12 hours are found as the early independent predictors of postinjury MOF. Another multiple logistic regression analysis performed by Tran et al.42 on 206 consecutive trauma patients, advancing age, chronic disease, ISS, and MOF score were selected as major predictors of death. In a statewide population-based study of 22,332 trauma patients after multiple logistic regression analysis, the predictors of in-hospital mortality were found as age, injury severity, admission physiological parameters, preexisting diseases.43 Therefore, the
risk factors of the post-injury MOF and trauma death were similar and determined under three headings, as: host factors, severity of tissue injuries, and clinical status of shock.
[Gender Difference in Trauma Outcome]
Oberholzer and colleagues44 demonstrated in 1,276 trauma patients with ISS≧9 that the incidence of posttraumatic sepsis and multiple organ dysfunction syndrome was significantly increased in severely injured males with ISS≧25 when compared with an equivalent female group(sepsis, 30.7% versus17.0%; multiple organ dysfunction syndrome, 29.6% versus 16.0%). They concluded that sex influences posttraumatic morbidity in severely injured patients and supports the concept that females are immunologically better positioned toward a septic challenge. Majetschak and colleagues45 also examined 84 patients with blunt trauma and ISS≧16 and discovered in severely injured males development of severe post-traumatic sepsis is associated with an increased cytokine producing capacity of whole blood in the early post-traumatic period. These findings may correspond to overwhelmingly inflammatory responses, which increase susceptibility for sepsis in male trauma patients. The data provide evidence for a gender specific regulation of the initial inflammatory response following severe blunt trauma.
[Gender Difference of Immune Response]
These alterations in endocrine and immune functions have been investigated using male laboratory animal, although gender differences in the susceptibility to and morbidity from sepsis have been observed in several clinical and epidemiological studies.46-48 Recent studies have suggested that male sex steroid hormones play a significant role in producing immunodepression following trauma and hemorrhagic shock.49-51 Moreover, these depressed immune responses have been associated with an increased susceptibility to and mortality due to subsequent sepsis.49,52 Furthermore, a number of investigators have shown that sexual dimorphism exists during circulatory stress, and those androgens and estrogens play a pivotal role in regulating the stress responses. 49-52
In this regard, studies by Wichmann et al.53 and Zellweger et al.54 have shown that female mice have enhanced immune responses as opposed to decreased responses in male mice after trauma-hemorrhage. Moreover, castration of male animals 14 days before hemorrhagic shock prevented the depression in myocardial functions and immune responses usually observed under those conditions.50,55,56 Furthermore, administration of the testosterone receptor antagonist flutamide improved the depressed immune responses and cardiac and hepatic functions in male animals after trauma and severe hemorrhage.57 Thus, male sex hormones appear to play a deleterious role in the development of cell and organ dysfunction after trauma and hemorrhage.58 In contrast to male mice, the elevated levels of female sex hormones, ie, prolactin and estrogen, in the proestrus state contribute to sexual dimorphism in the immune response following trauma-hemorrhage.59
The liver is a complex metabolically active organ, particularly susceptible to shock. Liver failure carries a high mortality rate because no real treatment or supportive care is known.60 Causes of these hepatic cellular changes are probably mutifactorial. A reduction in hepatic oxygen supply and subsequent hypoxia has been postulated. Neutrophil-mediated hepatic changes and oxygen radical-mediated injury are also thought to play a role in shock-induced hepatic injury.21 The hepatocyte’s ability to generate ATP is grossly reduced in an anaerobic metabolic state, which leads to cellular membrane and organelle damage followed by loss of liver function. Hepatocyte ATP level is drastically reduced during ischemia and is noted to rise again during reperfusion.61 Cellular swelling is accompanied by increased total cellular and mitochondrial calcium content, contributing to the further dysfunction of the energy-producing mechanism. The Kupffer cells and coagulations factors synthesis are also severely reduced in the shocked liver.
In the review by Jarrar & Chaudry62, they focus first on factors and mediators responsible for producing cell and organ dysfunctions, especially hepatocellular dysfunction, following trauma, hemorrhagic shock, and sepsis. The changes in signaling transduction pathways will also be discussed, specifically the role of mitogen-activated protein kinases, transcription factors, nitric oxide, heat shock proteins, and inflammatory cytokines in the development of cell and organ dysfunctions following trauma-hemorrhage and sepsis. Moreover, potential therapeutic approaches for improving cell and organ functions under adverse circulatory conditions are included.
[Sex Hormone Levels in Gender]
As previous mentioned, animal studies have revealed that female rats have protective effect of 17β-estradiol (E2) on immune function and physiological responses following trauma-hemorrhage. However, whether women experience better outcomes from injury as compared with men is still controversial in clinical studies.63-66. In clinical studies, the female sex hormone could difficultly been controlled due to varying plasma levels during menstrual cycle. On the other hand, the female sex hormone could be controlled easier in rat studies because they have short length of the estrus cycle, making them ideal for investigation of changes occurring during the reproductive cycle. The estrous cycle lasts four days and is divided as: proestrus, estrus, metestrus and diestrus, which can be determined according to the cell types observed in the vaginal smear by light microscopy67 as in our previous experiment. During estrous cycle in rats, the proestrus state shows the highest plasma concentration of estradiol and prolactin. 68 The plasma levels of both hormones are low on the morning of estrus and then gradually increase over diestrus to achieve their peak levels on the morning of proestrus.69 Wichmann et al.70 have shown that female mice subjected to hemorrhage during the proestrus state have enhanced immune responses as opposed to decreased responses in males. In summary, to achieve satisfactory results of female sex hormone on immune function and physiological responses following trauma-hemorrhage, adequate controlling of female rats in proestrus stage to keep high plasma levels of E2 plays an important role on this study.
However, poorly controlling of E2 was encountered in our previous experiment. The female sub-groups had significant greater plasma levels of E2, however, the diversity of plasma hormonal levels among female rats were large, representing that there was poorly controlling of the hormone in plasma, which may distorted the results in our study. The reason for poorly controlling of E2 is that we cannot decide the initial time of proestrus stage even though we can decide the proestrus under light microscopy. To control high level of serum E2 in rats, we plan to use castrated mature male rats followed by subcutaneous injection of E2 in this study.
[Response of Cytokines ]71-72 1. Introduction:
A. TNF-α:
Tumor necrosis factor alpha (TNF-α), also known as cachectin, is a 17.5 kD, 157 amino acid protein that is potently lymphoid factor, which exerts cytotoxic effects on a wide range of tumor cells and other target cells. TNF-α has been suggested to play a pro-inflammatory role and it is the primary mediator of immune regulation. Pro-inflammatory cytokine release after shock is central in the development of subsequent multiple organ dysfunction syndrome. According to Deitch, TNF-α, rather than IL-I or IL-6 appears to be the messenger that initiates and orchestrates the septic response. The biosynthesis of TNF-α is tightly controlled, being produced in extremely small quantities in quiescent cells, but is a major screted factor in activated cells.
B. IL-1β
Interleukin-1β(IL-1β) is translated as a 31 kD precursor that is glycosylated and cleaved into a cytosolic pro-IL-1β molecule. IL-1β with the aid of inducible transcription factors initiates the expression of a pro-inflammatory cascade of proteins and cytokines by selective regulation of other molecules. The half-life of IL-1β mRNA depends upon the cell type and the conditions of stimulation. In human blood monocytes and macrophage cell lines, the half-life of IL-1β mRNA is about 4 hours
C. IL-6:
Interleukin-6 (IL-6) is a cytokine critical to the regulation of immune and hematopoietic systems. IL-6 is a 21-kDa cytokine that is produced by variety of cells, including fibroblasts, endothelial cells, mononuclear phagocytes, neutrophils, hepatocytes, T and B lymphocytes, macrophages, and myocytes. trauma-hemorrhage that appears to be in part mediated by increased thromboxane A(2) levels.
It appears to take part in acute phase reactions and response to injury and inflammation. Elevation of serum IL-6 levels have been observed in a number of pathological conditions, including bacterial and viral infections, trauma, autoimmune diseases, inflammations and malignancies.According to Chaudry et al, IL-6 plays a significant role in the induction of hepatic dysfunction and liver injury after traumatic hemorrhagic shock.
D. IL-10
Interleukin-10 (IL-10), originally known as cytokine synthesis inhibitory factor (CSIF), is a pleiotropic cytokine with a myriad of immunomodulatory effects on a variety of cell types. Some studies suggest that interleukin-10 (IL-10) is an immunosuppressive mediator after injury or sepsis,
while others suggest that IL-10 is an important regulator of the pro-inflammatory response. On macrophages, IL-10 is known to downregulate TNF-α, IL-1, and IL-6 production.
[Microarray]
The completion of the Human Genome Project (sequencing of all ~30,000 human genes) will provide an unprecedented opportunity to study the molecular basis of injury-induced disease. Harnessing the power of rapidly surveying global variations in gene sequence and expression, microarrays afford the first tool permitting a truly integrated view of life at the molecular level. Arrays are capable currently of profiling patterns of expression for tens of thousands of genes (mouse or human) in a single experiment. The technique requires isolation of mRNA from the cells or tissue of interest, creation of complementary nucleotide "target", and hybridization of the labeled target to gene-specific "probe" nucleotides affixed to a glass or nylon matrix (the array).71 With the aid of a template describing the unique location of each probe oligonucleotide (gene), computer-driven differential analysis can be used to determine changes in gene expression (either up or down) relative to a standard (control). Far from being "fishing expeditions", arrays in recent months have determined unanticipated relationships between patterns of gene expression, indicating "cytoplasmic signaling proteins form networks of interactions rather than simple linear pathways as they are usually depicted", consistent with our overarching hypothesis.73
[Why Trauma Need Micrarray Study?]
CDNA, microarray technology, promises to become a pivotal tool in understanding the functional genomics of complex diseases, and is rarely applied on critically ill or injured patients.74 However, trauma and burns offer a unique population that is quite unlike NIH's current clinical study populations (e.g. AIDS, cancer, heart disease, arthritis, diabetes, and so forth). Most of trauma patients were entirely normal, immediately prior to the insult. This offers an unparalleled opportunity to study the physiological, proteomic, and genomic changes beginning with normal, deviating to grossly abnormal, and in most cases, return to the normal state. This scenario does not exist in any of the populations mentioned above.
Therefore, there is a strong likelihood that causal relationships between injury and changes in gene expression will be discovered in the field of inflammation and the host response in injury. First, those who suffer from injury begin as normal healthy individuals. Most survive the injury and return to a normal physiological and genomic state. However, the most attractive feature of this phenomenon is that the exact moment of the perturbation for these normal individuals is known, and that very dramatic physiological changes in the host response occur in a temporally related sequence. The phenotypic expression of these changes can be profound and tissue specific. For example, cardiac index, oxygen consumption, and resting energy expenditure may increase twofold. Furthermore, this response is tissue-specific. The energy requirement of the liver, heart, and wound may be increased threefold or more whereas skeletal muscle and brain remain at or below their normal requirements for energy. There are similarly dramatic changes in the acute phase and immuno- inflammatory response after injury.
[Injury and Functional Genomics]
Functional genomics is to describe the regulatory relationships between genes and their programs of expression, as reflected by changes in mRNA abundance and protein levels. 75-76Critically ill or injured patients frequently die of incompletely understood conditions such as septic shock, acute respiratory distress syndrome, and ultimately multiple system organ dysfunction or failure. Activation of host inflammatory pathways causes tissue injury and thereby acts as a major pathogenic mechanism in these syndromes.
The application of genomic technology to the study of sepsis will yield important new insights into the regulatory networks underlying pathogenic mechanisms relevant to treatment of infection- and inflammation-induced organ dysfunction. At a basic level, the clinical and biological manifestations of host responses are determined by quantitative and qualitative changes in gene expression. Therefore, organ injury syndromes might be defined by their associated patterns of altered gene expression. From paired samples of cells or tissues, cDNA microarrays can measure relative changes in mRNA levels for thousands of genes simultaneously.77
Further, cDNA microarrays can be used to detect genetic polymorphisms that affect outcome and to identify new gene targets for drug development. Because cDNA microarrays generate huge data sets even from relatively simple experiments, difficulties with validating and conceptually handling this quantity of information need to be resolved. Clustering data from genes with shared characteristics, developing software to aid in the interpretation of results, and rapidly making results widely available are some potential approaches to these problems. Data derived from microarrays will allow for the first time a truly global, integrated view of the adaptive response to injury.
[Gene Expression Profiles of Septic Mice]
Cobb et al. 78 use the cecal ligation and puncture (CLP) in a murine septic model, and examined two organs of interest, spleen (sensitive to stress-induced apoptosis) and liver (resistant to stress-induced apoptosis). By using Clontech Atlas (Clontech, Palo Alto, CA) microarray technology, they found that the sepsis-induced changes in expression of the 588 murine genes studied were organ specific.79 The changes in liver gene expression at 24 hrs of sepsis in this model were largely at the level of membrane proteins and receptors. In contrast, changes in the expression of a much larger number of spleen genes were observed, most of which are associated with signaling cascades, cell death pathways, and cytokine production. Recently Chung et al.80 also reported that they can determine not only changes in the murine sepsis transcriptome, but also which of these changes are associated with antibiotic treatment and, thereby, survival vs. death after cecal ligation and puncture.
[Hormonal Modulation as the Intervention for Trauma-Hemorrhage]
There have been several hormonal modulators, including estrogen, flutamide and metoclopramide, studied for the intervention to traumatic hemorrhagic shock.
Flutamide (FTM) is an androgen-receptor antagonist. Previous studies have shown that administration of flutamide up-regulated estrogen receptor (ER) expression in males following trauma-hemorrhage. Flutamide also normalizes the depressed immune and cardiac function in males after trauma hemorrhage. The mechanism of the salutary effect of flutamide on cardiac function after trauma-hemorrhage is thought to be mediated via an estrogen-dependent pathway through upregulation of PGC-1.84-85
Prolactin is involved in the regulation of immune functions under normal and pathological conditions. Recent studies have shown that administration of the anterior pituitary hormone, prolactin, after hemorrhage restored the depressed immune responses. Metoclopramide (MCP), a synthetic substituted benzamide, is a dopamine-receptor antagonist, an antiemetic, and a stimulant of upper gastrointestinalmotility. The increase in prolactin secretion is apparently the result of MCP's antagonism of dopamine receptors in the anteriorpituitary gland. Dopamine is produced in the arcuate and paraventricularnuclei of the hypothalamus and then released by nerve terminalsin the median eminence, where it enters the portal circulationand reaches the anterior pituitary. Dopamine inhibits prolactinrelease via interaction with pituitary D2 receptors.86 Drugs that are dopamine antagonists, such as MCP, therefore increase prolactin levels by blocking the inhibitory effects of dopaminein the anterior pituitary. Some studies also revealed that the depressed splenic and peritoneal macrophage IL-1 and IL-6 release after severe hemorrhage was restored with MCP treatment in mice. Further evidence for the importance of neuroendocrine factors in the response to trauma-hemorrhage came from studies with female rodents during different stages of the reproductive cycle. In this regard, studies have shown that females in the proestrus state, a state in which plasma prolactin levels are found to be the highest, have enhanced immune and cardiovascular responses after hemorrhage as opposed to decreased responses in males. According to Chaudry86, MCP administration, which increases prolactin secretion, appears to be a useful adjunct for improving cardiovascular and hepatocellular responses and downregulating inflammatory cytokine release after trauma and hemorrhagic shock.
Of the above mentioned hormonal modulators, estrogen and flutamide have more adverse effects and are seldom used clinically. On the other hand, metoclopramide is clinical available, low price with little adverse effect. Therefore, we suggest that MCP might be a useful adjuvant in the treatment of the trauma hemorrhagic shock-induced immunosuppression.86
[Summary of First Year Study] A. Purpose:
Under the application of microarray technology, we can have a global understanding of the pattern and difference of immune restoration and gene expression following traumatic hemorrhagic shock in the male and female rats. We also want to correlate these observed gene expressions with cellular change and clinical parameters such as hormone levels and serum cytokine concentrations.
In our study, mature Sprague-Dawley rats with half for each sex, will be divided into three groups, each group having 12 rats. Group I: control group (sham operation). Group II:hemorrhagic group (sham operation + shock). Group III:resuscitative group (sham operation + shock+ resuscitation). Hemorrhagic shock will be induced by withdrawing 2.5 mL blood/kg body weight for 10 minutes. After shock, animals are resuscitated with the shed blood and lactated Ringer’s (RL) solution (2 times the shed blood volume, 5 mL/kg/h). The animals will be sacrificed by euthanasia at 4 hrs after the finish of experiment to obtain the liver and whole blood. The liver sample will be harvest and frozen rapidly in liquid nitrogen(-196℃) and storage at refreezer(-70℃)until microarray and pathological analysis. The cytokines including TNF-α,IL-1β,IL-6 及 IL-10, as well as 17β-estradiol will be measured through the blood samples. C. Results:
The 4-hour survival rates of group I and group III were 100%. However, in group II (hemorrhagic group), the 4-hour survival rate was 33% in male sub-group, and 50% in female sub-group. In regard to 17-βestradiol, plasma levels in females were significantly higher than those in males (p<0.001). However, the variation of plasma levels of 17-βestradiol among females were significant. Regardless of sexes, group II had the highest and group I had the lowest plasma levels of TNF-α,IL-1β,IL-6 and IL-10. As compared with sham operation group (group I), the plasma levels cytokines following traumatic hemorrhagic shock (group II) increased 5.7-fold (male) and 2.3 fold (female) for TNF-α, 18.1-fold (male) and 2.8-fold (female) for IL-1β, 15.9-fold (male) and 2.6-fold (female) for IL-6, and 1.9-fold (male) and 4.0-fold (female) for IL-10 respectively. On the other hand, as compared with shock group, levels of cytokine in plasma following resuscitation decreased 85.8% (male) and 60.2% (female) for TNF-α, 92.5% (male) and 61.8% (female) for IL-1β, 91.8% (male) and 57.8% (female) for IL-6, and 46.% (male) and 72.2% (female) for IL-10 respectively. In the microarray study, the GeneChip® revealed 3.0% (944/31099) of assessed genes were altered in which 415 genes up regulated and 286 genes down regulated in male sub-group, 203 genes up regulated and 73 genes down regulated during the hemorrhagic shock. The regulated activities of significant up-regulated genes during traumatic hemorrhagic shock include protein phosphatase type 1 regulator, prostaglandin transporter, negative regulator of basal transcription, cholesterol 7-alpha-monooxygenase, hydroxymethylglutaryl-CoA reductase (NADPH), glycerol-3-phosphate dehydrogenase (NAD+), glycine N-acyltransferase, [pyruvate dehydrogenase (lipoamide) ] kinase, pyruvate kinase, ATP citrate synthase etc. in male sub-group; and L-omithine transporter ,cAMP-dependent protein kinase inhibitor ,transmembrane receptor protein tyrosine kinase activator, ErbB-2 class receptor binding, receptor tyrosine kinase binding, cAMP response element binding protein binding , carbonate dehydratase, searoyl-CoA 9-desaturase, X-Pro aminopeptidase, Hsp27 protein, cAMP response element binding protein binding, MAP kinase phosphatase etc. in female sub-group.The regulated activities of significant down-regulated genes include basic amino acid permease, translation activator, retinoic acid 4-hydroxylase, NAD(P)H oxidase, asparagine synthase (glutamine-hydrolyzing, granzyme A, NAD+ nucleosidase, 2’,3’-cyclic-nucleotide 3’-phosphodiesterase, spermidine synthase etc. in male sub-group; and diphosphomevalonate decarboxylase , glycerol-3-phosphate O-acyltransferase , C-4 methylsterol oxidase , ianosterol synthase, isopentenyl-diphosphate delta-isomerase etc. in female sub-group.
As compared with shock group, the GeneChip® revealed 4.1% (1288/31099) of assessed genes were altered in which 617 genes up regulated and 441 genes down regulated in male sub-group, 126 genes up regulated and 148 genes down regulated after resuscitation. The regulated activities of significant up-regulated genes during traumatic hemorrhagic shock include citrate transporter, myo-inositol: sodium symporte), U-plasminogen activator receptor , ciliary neutrophic factor receptor binding , unfolded protein binding, TPR domain binding, heat shock protein binding, unmethylated CpG binding, stromelysin 1, stromelysin 2, phosphoserine phosphotase, phosphotidylinositol 3-kinase, camitine O-octanoyltransferase, steroid 17-alpha-monooxygenase, tryptophan-tRNA ligase, asparagine synthase (glutamine-hydrolyzing), etc in male sub-group; and proton-dependent oligopeptide transporter, insulin-like growth factor binding, heparanase , phosphoserine transamine, phosphoglycerate dehydrogenase, asparagine synthase (glutamine-hydrolyzing) etc. in female sub-group. The significant down-regulated genes included Prostaglandin transporter, Chemokine activity, Chemokine receptor binding, Interleukin-1, type I receptor binding, Phosphopantetheine binding, ATP citrate synthase, Squalene monooxygenase, Sterol 14-demethylase, Cholesterol 7-alpha-monooxygenase, Hydroxymethylglutaryl-CoA reductase, Glucose-6-phosphate 1-dehydrogenase, Hydroxymethylglutaryl-CoA reductase, Formyltetrahydrofolate dehydrogenase , Sarcosine dehydrogenase, Steroid delta-isomerase, Isopentenyl-diphosphate delta-isomerase, Famesyl-diphosphate famesyltransferase, Enoyl-[acyl-carrier protein] reductase (NADPH, B-specific), Glycerone kinase, Phosphomevalonate kinase, Pyruvate kinase, 3-oxaloacyl-[acyl-carrier protein] reductase, 3-oxaloacyl-[acyl-carrier protein] synyhase, Myristoyl-[acyl-carrier protein] hydrolase, Oleoyl-[acyl-carrier protein] hydrolase, Glucose-6-phosphate 1-dehydrogenase, X-pro aminopeptidase, Palmitoyl-[acyl-carrier protein] hydrolase etc. in male sub-group; and transmembrane receptor protein tyrosine kinase activator , MHC class I receptor , receptor tyrosine kinase binding (9), ErbB-2 class receptor binding, Hsp27 protein binding, stearoyl-CoA 9 desaturase, L-serine ammonia-lyase, threonine ammonia-lyase, X-Pro aminopeptidase, glycine N-methyltransferase, ornithine carbamoyltransferase , aspartate carbamoyltransferase , glycine N-acyltransferase, ketohexokinase, [pyruvate dehydrogenase (lipoamide)] kinase, glutathione transferase, D-amino-acid oxidase, sterol 12-alpha-hydroxylase, alpha-methylacyl-CoA racemerase etc. in female sub-group.
D. Discussion:
According to the results of our reperiment,,the mortality rates were zero in all except the shock group. In shock group (group II), the mortality was 66.7% in male sub-group and 50% in female sub-group. Amongthe mortality rats, male rats had shorter mean survival time than females did (81.3 min. vs. 123 min.). In regard to pro-inflammatory cytokines,TNF-α,IL-1β and IL-6,the plasma levels following traumatic hemorrhagic shock increased more predominantly in male subgroups as compared with those in female sub-groups. On the other hand, levels of anti-inflammatory cytokine, IL-10 in plasma following traumatic hemorrhagic shock increased more significantly in females as compared with those in males. The current data of mortality and plasma levels of cytokines in group II suggesting that females have more protective from traumatic hemorrhagic shock than males do. The protective effect may be due to the modulation of sex hormone, 17β-estradiol in particularly. The regulation of
17β-estradiol for the release and function of cytokines and the protection of the body in traumatic hemorrhagic shock have been widely discussed and proven. The contention is further supported in our experiment. In resuscitation groups, all of the studied cytokines were decreased significantly as compared with those in shock groups (p<0.001), but they showed no significant differences between sham operation group and resuscitation group. From this detrimental hemorrhagic shock model in the rat, we understand the gene expression is different from sepsis model. Most of the molecular activities of significant regulated genes are energy producing and metabolically related genes, and some are signal transduction, transporter and transcription regulator. In contrast with the lipopolysaccharide (LPS) induced septic model, their pattern of gene expression is exaggerated in the signaling networks and cytokine actions.
E. Conculsion:
Estrogen play an important role on modulation for systemic inflammatory response following traumatic hemorrhagic shock and resuscitation, therefore, reduce the early mortality of the injuried rats. Through the finding of up-regulated and down-regulated genes via microarray technology, we can further understand the miscellaneous responses after traumatic hemorrhagic shock, which can yield important new insights into the basic study for ongoing related research.
[Significance and Aim of this Study]
We plan to use the more detrimental hemorrhagic shock in the rat model and followed by resuscitation. And based on the above hypothesis, we intended (1) to introduce of hormonal modulators (metoclopramide) and to verify its therapeutic effects in affecting the hormone, immunology, and functional genomics in the hemorrhagic shock of rat. Through the two-year studies, we anticipate the miscellaneous hormonal, immunological, and genomic responses of rats can yield important new insights into the clinical resuscitation on severely injured patients with hemorrhagic shock and achieving an improved outcome in the future trauma resuscitation.
z Materials and Methods [Animal preparation]
Sprague-Dawley rats (body weight, male:300-350 g; female:200-300 g), with half for each sex, average age 8-12 weeks old, were housed in the animal facility at constant room temperature in a 12-hour light-dark cycle. They were allowed to acclimatize to laboratory conditions for at least 3 days before use. The experiments described conform to the current guidelines for care and use of laboratory animals as established by the Animal Care Committee of Chinese Medical University. All animals received rat chow and water ad libitum throughout the acclimatization period and until the time of operation.
Twenty-four rats were randomized into two groups with each groups of twelve rats, Group I: Control group (hemorrhagic shock+resuscitation); Group II: Metoclopramide intervention group (100 μg/100 g body weight, subcutaneously). Each group was further divided into two sub-groups: male and female (each sub-group contains 6 rats). Sprague-Dawley rats will be anesthetized with intraperitoneal injections of citosol (25-40 mg/kg) till adequate anesthesia. Polyethylene tubes (PE-50) were placed into the right jugular vein to administer drugs or fluids and continuously monitor central venous pressure (CVP) by a Cardiomax -II model 85 (Columbus Instruments International Co., Ohio, USA). The right femoral artery was cannulated (PE-50) to monitor blood pressure (BP) by a Cardiomax -II model 85 (Columbus Instruments International Co., Ohio, USA). The left femoral artery was cannulated (PE-50) for blood withdraw and replacement. All rats received a basic infusion of lactated Ringer’s solution (RL) (10 mL/kg/h) to replace evaporative losses, and are allowed to stabilize for 15 minutes after preparation. Body temperature is kept at 37 ± 0.5 °C by a heating device.
[Hemorrhagic Shock and Resuscitation Model]
The hemorrhagic shock and resuscitation model was used in the current study is a well-established model of fixed-pressure hemorrhage. In Group I and II, hemorrhagic shock was induced by withdrawing 2.5 mL blood/kg body weight for 10 minutes and maintaining MABP at 50+5 mm Hg for 60 minutes by withdrawing or replacing blood.
After this shock interval, animals were followed the following resuscitation as previous assigned groups: (I) resuscitation without metoclopramide intervention ; (II) metoclopramide intervention before resuscitation. During resuscitation, the shed blood (2.5 mL blood/kg body weight) will be returned and lactated Ringer solution (2 times the shed blood volume, 5 mL/kg/h) will be infused over 10 minutes to provide adequate fluid resuscitation. In metoclopramide intervention group, metoclopramide 100μg/100g body weight will be injected subcutaneously before resuscitation. After resuscitation, the animals will be allowed awake after the catheters removed and vessels ligated. All the animals were sacrificed 4 hours later.
[Procedure] Time(min.) 0 15 25 Gr. I A B C D E Gr. II A B C D E A1 B1 C1 D1 E1 F1 85 95 Metoclopramide intervention
A1: Start celiotomy: ventral incision from sub-xiphoid to pubic symphysis , bowel manipulation and then close the wound by silk.
A: Prepared period (90 minutes): Includes celiotomy、cannulation (right jugular vein and bilateral femoral arteries), monitor setting and tubes connection. The experiment will be start if all the above procedures are completed.
B1: Start experiment
B: Stabilization period (15 minutes): C1:Start blood withdraw
C: Shock inducing period (10 minutes): withdraw 2.5 mL blood/kg body weight for 10 minutes to maintain MABP at 50+5 mmHg
D: Shock maintaining period: maintaining MABP at 50+5 mmHg for 60 minutes by withdrawing or replacing blood.
E1: Start resuscitation:
E: Resuscitation period (10 minutes):
a、 replace the shed blood that was previously withdrawn.
b、 IV fluid challenge(Lactated Ringer solution :5ml/kg body weight)
Time(min.) 95 335
Gr. I F
Gr. II F
F1 G1 F1: Remove catheters、vessels ligation and animal awake
F: Recovery period (4 hours):
G1: The experiment was stopped at 335th min.(4 hours after the end of resuscitation period) or any time if the animals were dead during recovery period. The animals were sacrificed immediately after the experiment was stopped. The blood was withdrawn by cardiac puncture and the liver tissues were harvested thereafter.
[Animal Plasma Collection and Storage]
Whole blood will be sampled by cardiac puncture after rats were sacrifice. Plasma will be separated by centrifugation in pyrogen-free microcentrifuge tubes and samples are immediately frozen and stored (-70°C) until assayed.
A. Assessment of 17β-Estradiol and Cytokine Concentrations
17β-estradiol plasma concentrations were determined using a commercially available enzyme-linked immunosorbent assay as described by the manufacturer (Cayman Chemical Company, USA ).
Summary of assay procedure:
1. Allow all reagents to reach room temperature. Arrange and label required number of strips.
2. Pipet 50 ul of sample diluent (as zero standards), standards, control, and serum samples into anti-Mouse IgG coated wells in duplicate. Add 100 ul of Estradiol Enzyme
Conjugate solution into each well. Cover the plate and incubate at room temperature for 60 mins on a plate shaker.
3. Aspirate and wash the plate three times with wash buffer.
4. Pipet 150 ul of HRP substrate (TMB) into each well, mix gently (blue color denelops), cover the wells, and incubate at room temperature for 10 min.
5. Pipet 50 ul of stopping solution into each wells and mix gently (blue color turns yellow). Measure absorbance at 450 nm.
B. Assessment of TNF-α
Activity of TNF- α will be determined by enzyme-linked immunosorbent assay according to the manufacturer’s recommendations (R&D Systems, Inc.).
Summary of assay procedure74:
1. prepare reagents, standard curve dilutions, and samples as directed by the previous sections.
2. Remove excess microplate strips from the plate frame, return them to the foil pouch containing the desiccant pack, reseal.
3. Add 50uL of Assay Diluent RD1-41 to the center of each well.
4. Add 50uL of Standard, Control or sample* per well. Mix by gently tapping the plate frame for one minute. Cover with the adhesive strip provided. Incubate for 2 hours at room temperature. Plate layouts are provided to record standards and samples assays.
5. Aspiration each well and wash, repeating the process four times for a total of five washes. Wash by filling each well with Wash Buffer (400uL) using a squirt bottle, multi-channel pipette, manifold dispenser or autowasher. Complete removal of liquid at each step is essential to good performance. After the last wash, remove any remaining Wash Buffer by aspirating or decanting. Invert the plate and blot it against clean paper towels.
6. Add 100 uL of rat TNF-α Conjugate to each well. Cover with a new adhesive strip. Incubate for 2 hours at room temperature.
8. Add 100 uL of substrate Solution to each well. Incubate for 30 minutes at room temperature. Protect from light.
9. Add 100 uL of Stop Solution to each well. Gently tap the plate to ensure thorough mixing. 10. Determine the optical density of each well within 30 minutes, using a microplate reader set to
450 nm. If the wavelength correction is available, set to 540 nm or 570 nm. If wavelength correction is not available, subtract readings at 540 nm or 570 nm from the readings at 450 nm. This subtraction will correct for optical imperfections in the plate. Readings made directly at 450 nm without correction may be higher and less accurate.
C. Assessment of IL-1β
Activity of IL-1β will be determined by enzyme-linked immunosorbent assay according to the manufacturer’s recommendations (R&D Systems, Inc.).
Summary of assay procedure74:
1. prepare reagents, standard curve dilutions, and samples as directed by the previous sections.
2. Remove excess microplate strips from the plate frame, return them to the foil pouch containing the desiccant pack, reseal.
3. Add 50uL of Assay Diluent RD1-21 to each well.
4. Add 50uL of Standard, Control or sample* per well. Mix by gently tapping the plate frame for one minute. Cover with the adhesive strip provided. Incubate for 2 hours at room temperature. Plate layouts are provided to record standards and samples assays.
5. Aspiration each well and wash, repeating the process four times for a total of five washes. Wash by filling each well with Wash Buffer (400uL) using a squirt bottle, multi-channel pipette, manifold dispenser or autowasher. Complete removal of liquid at each step is essential to good performance. After the last wash, remove any remaining Wash Buffer by aspirating or decanting. Invert the plate and blot it against clean paper towels.
6. Add 100 uL of rat IL-1β Conjugate to each well. Cover with a new adhesive strip. Incubate for 2 hours at room temperature.
7. Repeat the aspiration/wash as step 5.
8. Add 100 uL of substrate Solution to each well. Incubate for 30 minutes at room temperature. Protect from light.
9. Add 100 uL of Stop Solution to each well. Gently tap the plate to ensure thorough mixing. 10. Determine the optical density of each well within 30 minutes, using a microplate reader
set to 450 nm. If the wavelength correction is available, set to 540 nm or 570 nm. If wavelength correction is not available, subtract readings at 540 nm or 570 nm from the readings at 450 nm. This subtraction will correct for optical imperfections in the plate. Readings made directly at 450 nm without correction may be higher and less accurate. D. Assessment of IL-6
Activity of IL-6 will be determined by assessing the 72-hour proliferation of the IL-6-dependent murine hybridoma 7TD1 stimulated by serial dilutions of plasma or supernatant, as described previously.
1. Bring all reagents to room temperature. Prepare reagents and samples as instructed. Return unused components to storage temperature as indicated in the instructions.
2. Add 50uL of Assay Diluent RD1-54 to each well.
3. Add 50uL of Standard, Control or sample* to each well. Tap plate gently for one minute. Cover the plate and incubate for 2 hours at room temperature.
4. Aspirate and wash each well for five times.
5. Add 100 uL of rat IL-6 Conjugate to each well. Cover the plate and incubate for 2 hours at room temperature.
6. Aspirate and wash each well for five times.
7. Add 100 uL of Substrate Solution to each well. Incubate for 30 minutes at room temperature. Protect from light.
8. Add 100 uL of Stop Solution to each well.
9. Read Optical, Density at 450 nm (correction wavelength set at 540 nm or 570 nm) E. Assessment of IL-10
Concentrations of IL-10 will be determined by enzyme-linked immunosorbent assay according to the manufacturer’s recommendations (Pharmingen, San Diego, CA).
Summary of assay procedure77:
1. Bring all reagents to room temperature. Prepare reagents and samples as instructed. Return unused components to storage temperature as indicated in the instructions.
2. Add 50uL of Assay Diluent RD1-21 to each well.
3. Add 50uL of Standard, Control or sample* to each well. Tap plate gently for one minute. Cover the plate and incubate for 2 hours at room temperature.
4. Aspirate and wash each well for five times.
5. Add 100 uL of rat IL-10 Conjugate to each well. Cover the plate and incubate for 2 hours at room temperature.
6. Aspirate and wash each well for five times.
7. Add 100 uL of Substrate Solution to each well. Incubate for 30 minutes at room temperature. Protect from light.
8. Add 100 uL of Stop Solution to each well.
9. Read Optical, Density at 450 nm (correction wavelength set at 540 nm or 570 nm) [Animal Liver Tissue Harvest]
The harvest of rat liver was performed through a midline ventral incision from pubis to xiphoid process. One segment (weight > 1 g) of middle lobe of liver is excised and hemostasis is done by ligation with 3-0 silk at the proximal part of middle lobe. The liver sample will be frozen rapidly in liquid nitrogen. The tissue will be kept in a -70oC freezer until microarray analysis.
[Microarray & Technique81,82] A. Introduction
Expression of liver RNA was analysed by microarray technique using GeneChip®Probe Arrays (Affymetrix, Inc.). GeneChip probe arrays are manufactured using technology that
combines photolithography and combinatorial chemistry. Up to 1.3 million different oligonucleotide probes are synthesized on each array. Each oligonucleotide is located in a specific area on the array called a probe cell. Each probe cell contains hundreds of thousands to millions of copies of a given oligonucleotide.
During the laboratory procedure described in this manual, biotin-labeled RNA or DNA fragments referred to as the “target” are hybridized to the probe array. The hybridized probe array is stained with streptavidin phycoerythrin conjugate and scanned by the GeneChip® Scanner 3000, or the GeneArray® Scanner. The amount of light emitted at 570 nm is proportional to the bound target at each location on the probe array.
B. GeneChip® Expression Analysis 1. RNA Preparation
Total RNA was isolated from rat liver tissue samples and electrophoresed on a 1% agarose-formaldehyde gel to determine the integrity of the RNA preparation. All RNA samples should meet assay quality standards to ensure the highest quality RNA is hybridized to the gene expression arrays. A 260/280 absorbance reading should be obtained for both total RNA and biotinylated cRNA. Acceptable A260/280 ratios fall in the range of 1.8 to 2.1. Ratios below 1.8 indicate possible protein contamination. Ratios above 2.1 indicate presence of degraded RNA, runcated cRNA transcripts, and/or excess free nucleotides. Then double-stranded cDNA is synthesized from total RNA isolated from rats’ liver tissue. An in vitro transcription (IVT) reaction is then done to produce biotin-labeled cRNA from the cDNA. The cRNA is fragmented before hybridization. The use of gel electrophoresis will aid in quality control following the sample from step to step in the assay and hybridization protocol. Gel electrophoresis can be performed after cDNA synthesis (if using poly-A mRNA as starting material), after cRNA synthesis, and after fragmentation. This will be helpful in estimating quantity and size distribution of the labeled sample. During this phase of technical evaluation, cRNA yield from a standard total RNA sample is another simple and effective method to assess consistency.
2. Gene microarray hybridization
A hybridization cocktail is prepared, including the fragmented target, probe array controls, BSA, and herring sperm DNA. It is then hybridized to the probe array during a 16-hour incubation. The hybridization process is described in the respective sections for the different probe array types.
3. Fluidics Station Setup
Specific experimental information is defined using Affymetrix® Microarray Suite or GeneChip Operating Software (GCOS) on a PC-compatible workstation. The probe array type, sample description, and comments are entered and saved with a unique experiment name. The fluidics station is then prepared for use by priming with the appropriate buffers.
4. Probe Array Washing and Staining
Immediately following hybridization, the probe array undergoes an automated washing and staining protocol on the fluidics station.
Once the probe array has been hybridized, washed, and stained, it is scanned. Each workstation running Affymetrix Microarray Suite or GCOS can control one scanner. The software defines the probe cells and computes an intensity for each cell. Each complete probe array image is stored in a separate data file identified by the experiment name and is saved with a data image file (.dat) extension.
6. Data analysis
The .dat image is analyzed for probe intensities; results are reported in tabular and graphical formats. Information on data analysis is provided in the enclosed GeneChip® Expression Analysis: Data Analysis Fundamentals booklet (P/N 701190).
C. Gene expression comparison
The liver tissues are prepared for RNA as described by the manufacturer as above. The target so generated was hybridized with cRNA probes on the Atlas array in accordance with the manufacturer’s instructions. Changes in expression were measured for more than 30000 known RNA sequences rat genes and send for cRNA microarray study using GeneChip®Probe Arrays. The differences of gene expression in three groups (control, shock and resuscitation) between male and female liver will be compared (total 12 GeneChip®, two for each sub-groups).
Gene expression was defined as coordinately increased or decreased relative to control (sham laparotomy) if there was concordance of all above analytical methods. A simple statistical test (sampling without replacement) was used to indicate the relative level of significance of the observed changes in gene expression, expressed as the number of genes that would be expected to be consistently increased or decreased by chance. The expression of a gene was called “increased” or “decreased” if 75% of the matrix showed a ratio reflecting a two-fold change (i.e., >2 or <0.5).Those previous significant expression genes related to sepsis and shock were compared between Group I (control) and Group II (hemorrhagic shock). And those genes expression difference after resuscitation were studied between the Group II (hemorrhagic shock) and Group III (resuscitation) to determine the effect of resuscitation on hemorrhagic shock.
[Statistical analysis]
Group analyzed using one-way analysis of variance (ANOVA). Statistical analysis of differences between groups was determined by post hoc Student Newman Keuls test. Comparisons between different periods of hemodynamic data in the animal were analyzed using the paired Student’s t test. Data are presented as means + standard error of means (SEM). Significancewas achieved when p<0.05. Statistical analysis was performed using commercially available software (SPSS13.0 for window).
z Results
[Age versus Body Weight]
There were no significant differences in age between two groups, but the body weights in male rats were significantly greater than those in female rats (p<0.05, Table 1).
Table 1:
Control Metoclopramide intervention Group IM (n=6) IF (n=6) IIM (n=6) IIF (n=6) Age (wks) 9-12 9-12 9-12 9-12 Wt (kg) (range) 338.2+19.8 (306-360) 285.2+22.3* (253-305) 353.7+47.8 (288-408) 278.5+26.9# (252-326) p value *0.008 vs male subgroup #<0.001 vs male subgroup
[Hemodynamic Change]
In regard to mean central venous pressure (MCVP) levels, there were no significant differences among four subgroups during stabilization period, shock peiod or resuscitation period. But the MCVP in resuscitation period were significant greater than those in stabilization and shock periods in female sub-groups (p<0.05) (Fig. 1 and Table 2).
<Fig.1>
MCVP in different periods between two groups
2.5* 3.8 2.0 1.4@ 1.5 3.7*# 1.6 1.9 2.6$ 0.0 0.5 1.0 1.5 2.0 2.5 3.0 3.5 4.0 B D E
M
C
V
P
(mmH
g)
IM IIM IF IIF ※ : B※ p value: *<0.001 vs stabilization period, #<0.001 vs shock pe : stabilization period; D: shock period; E: resuscitation period
riod in Sub-group IF ※ p value: $<0.001 vs shock period in Sub-group IIF
Table 2:
Control Metoclopramide intervention Group IM (n=6) IF (n=6) IIM (n=6) IIF (n=6) (range) 2.5+1.3 (1.5-5.0) 1.4+1.1 (-0.5-2.5) 1.6+0.7 (0.5-2.5) 1.4+0.7 (0.5-2.0) (cmH2O (range) 1.9+10.5 (1.6-3.0) 1.5+0.6 (0.7-2.1) 1.5+1.7 (-0.1-4.7) 1.5+0.2 (1.1-1.8) MCVP (cmH2O) in D (range) 3.8+2.6* (2.0-9.0) 3.7+0.8#$ (2.0-4.0) 2.0+1.8 (-0.5-5.0) 2.7+1.0& (1.5-4.0) P value *<0 -group I scitation riod D)
roup IF .05 vs sub IM in resu period (pe
#<0.05 vs sub-group II
F in resuscitation period (period D) $<0.001 vs stabilization (B) and shock (C) periods in sub-g &0.031 vs shock period (C) in sub-group II
F
MCVP (cmH2O) in B
MCVP ) in C
MABP in different periods among three groups
119.2 51.9* 119.3 115.4 53.7$ 119.8 118.7 53.2# 119.4 117.4 54.1& 113.3 0.0 20.0 40.0 60.0 80.0 100.0 120.0 140.0 B D E MA B P (mmH g
)
IM IF IIM IIF※ B: stabilization period; D: shock period; E: resuscitation period.
ith regard to mean arterial blood pressure (MABP) levels, there were no significant diffe
<
※ *p<0.001 vs stabilization (B) and shock (C) period in Sub-group IM F W
rences as compared with the corresponding sub-groups in stabilization, shock or resuscitation periods. Regardless of sexes, shock period had significant lowest MABP (p<0.05, Fig. 2 and Table 3).
Fig.2>
※ #p<0.001 vs stabilization (B) and shock (C) period in Sub-group I ※ $p<0.001 vs stabilization (B) and shock (C) period in Sub-group IIM ※ &p<0.001 vs stabilization (B) and shock (C) period in Sub-group IIF
Tab intervention le3: Control Metoclopramide roup G IM (n=6) IF (n=6) IIM (n=6) IIF (n=6) MABP in B (range) 119.2+9.1# (101.0-125.5) 5.4+ 11 119.4+18.5# 113.3+ (89.0-136.5) 9.1# (102.5-124.5) MABP in C (range) 51.9+2.5* (47.6-54.7) 53.7+2.2# (51.0-57.1) 53.2+1.0$ (52.0-54.7) 54.1+1.9& (51.1-56.7) MABP in D (range) 118.7+10.1 (103.0-130.0) 119.3+7.3 (112.0-128.0) 119.8+4.4 (114.5-125.0) 117.4+5.3 (114.0-124.0) *#$ tabiliza shock (C) period in the corresponding su
p value *<0.001 vs s tion (B) and b-group del] 8.8# (102.5-126.0) 20.6 15.9 141.7#$ 88.4* 0.0 50.0 100.0 150.0 200.0 250.0 Group I Group II C o nc .( pg /m l) Male Female
p=0.005 vs male in group I (control group)
p<0.001 vs male in group II (metoclopramide intervention group)
Plasm a levels of 17-beta estradiol
[Mortality of Mo
All rats were alive 4 hours after traumatic hemorrhagic shock ( 4-hour survival
Plasma Levels of 17β-estradiol]
he male sub-groups had the significantly lower plasma levels of 17β-estradiol than group had significantly highe ※ * ※ # rate=100% ) [Alteration in T
those in females. In female, the metoclopramide intervention
sub-r plasma levels of 17β-estsub-radiol, howevesub-r, thesub-re wesub-re no significant diffesub-rences between male sub-groups (p<0.05, Fig.3 and Table 4) .
<Fig.3>
※ $