建置電子健康照護服務之績效評量架構 - 政大學術集成
44
0
0
全文
(2) Assessing the Performance of e-Health Service ABSTRACT This study develops quality evaluation criteria that consider both service provider satisfaction and patient perspective in assessing e-Health services; additionally, it evaluates the impact of these criteria on the performance of e-Health services. Utilizing data from the Tele Care Center in National Taiwan University Hospital (NTUH), one of the largest hospitals in Taiwan, this research framework extends the service-profit chain by integrating service triangle concept and emphasizing the relationships among three stakeholders: the firm, the customer, and the employee. The results suggest that the positive relationships among hospital’s business value, physicians’ value, and patients’ value can contribute to customer retention. In sum, this study expects to contribute to literature by providing an e-Health service performance assessment framework, which systematically develops a scale to evaluate e-Health service quality that concerns multiple stakeholders’ perspectives.. 立. 政 治 大. ‧. ‧ 國. 學. Keywords: e-Health service, internal service quality, external service value. n. er. io. sit. y. Nat. al. Ch. engchi. i. i n U. v.
(3) CONTENTS CHAPTER 1 – INTRODUCTION ............................................................................. 1 CHAPTER 2 – LITERATURE REVIEW ................................................................. 3 2.1 INTERNAL SERVICE QUALITY ................................................................................ 3 2.1.1 BUSINESS VALUE OF FIRMS ............................................................................ 4 2.1.2 EMPLOYEE VALUE .......................................................................................... 5 2.2 EXTERNAL SERVICE VALUE ................................................................................... 9 2.2.1 CUSTOMER VALUE ......................................................................................... 9 CHAPTER 3 – RESEARCH MODEL AND HYPOTHESES ............................... 13 3.1 THE DELIVERY OF FIRMS’ BUSINESS VALUE ........................................................ 13 3.2 THE DELIVERY OF EMPLOYEE VALUE.................................................................. 14 3.3 THE DELIVERY OF CUSTOMER VALUE AND RETENTION ....................................... 15. 治 政 CHAPTER 4 – RESEARCH METHODOLOGY ................................................... 16 大 立 4.1 C B ........................................................................................... 17 ASE. ACKGROUND. ‧. ‧ 國. 學. 4.2 SYSTEM BACKGROUND ....................................................................................... 18 4.3 MEASUREMENT ................................................................................................... 19 4.4 DATA COLLECTION .............................................................................................. 21 4.5 FRAMEWORK APPLICATION ................................................................................. 22. io. sit. y. Nat. CHAPTER 5 – RESULTS AND DISCUSSION ...................................................... 26 5.1 SUMMARY ........................................................................................................... 26 5.2 FINDINGS ............................................................................................................ 27. n. al. er. CHAPTER 6 – CONCLUSION ................................................................................ 29 6.1 CONCLUSION ....................................................................................................... 29 6.2 LIMITATIONS AND IMPLICATIONS OF FUTURE RESEARCH..................................... 29. Ch. engchi. i n U. v. REFERENCES........................................................................................................... 30 Appendix A – Complete Questionnaire for Physicians of “Tele Care Center” in e-Health Service ......................................................................................................... 33 Appendix B – Complete Questionnaire for Case Managers of “Tele Care Center” in e-Health Service ..................................................................................................... 34 Appendix C – Complete Questionnaire for Patients of “Tele Care Center” in e-Health Service ......................................................................................................... 35 Appendix D – Question List of the Group Interview (Chinese) ............................ 36 Appendix E – Interview Contents and Framework Application for Patients’ Value (Chinese) ........................................................................................................... 37. ii.
(4) TABLE CONTENTS Table 2-1 Comparison of the Employee Value Classification ………………... 08 Table 2-2 Comparison of the Customer Value Classification ………………… 12 Table 4-1 Description of The Three Service Categories in This Case ………... 18 Table 4-2 Measuring Construct of the Delivery of Firms’ Business Value ……19 Table 4-3 Measuring Construct of Employee Value Delivery ………………... 20 Table 4-4 Measuring Construct of Customer Value and Retention …………... 20 Table 4-5 The List of Samples ……………………………………………...… 21. 政 治 大. Table 4-6 Summary of Analysis Results …………………….………………... 22. 學. ‧ 國. 立. FIGURE CONTENTS. ‧. Figure 2-1 The Links in the Service-Profit Chain ……………………………. 03. sit. y. Nat. Figure 3-1 Research Framework ……………………………………………… 13. io. er. Figure 4-1 Research Process Map ……………………………………………..16. al. Figure 4-2 The Structure of Case Management in NTUH e-Health Service …. 17. n. v i n C h Flow ....…………………………………. e-Health Service System 19 engchi U. Figure 4-3. Figure 5-1 Summary of Case Analysis ………………..……………………… 26 Figure 5-2 Result of after Reviewing Research Model …………………….… 28. iii.
(5) CHAPTER 1 – INTRODUCTION ―E-Health‖ refers to a new system of health-related electronic services that offers a wide range of content, medical device connectivity, and improved clinical care (Maheu 2001; Lankton 2007; Hamid 2008). As a result of increased cost efficiencies and greater patient satisfaction (Lankton 2007), e-Health has become widely adopted worldwide; between 1999 and 2002 alone, the number of e-Health adopters has shown an increase of 788% (Hsu 2005). For adopters, it is important to develop performance metrics as a means for health care organizations to assess the likelihood of success of the these e-Health services (Lankton 2007). Traditionally, healthcare services are evaluated based on clinical statistics such as mortality and morbidity rates, which take into account only the clinician’s perspective; oftentimes, the more subjective, customer-oriented quality assessment is ignored (Dagger 2007). A good performance assessment, however, should consider the viewpoints of a variety of stakeholders (Lanseng 2007). For instance, to a hospital manager, quality service could mean having no adverse publicity; to clinicians, quality is tied to medical outcomes; to marketers, quality is a. 立. 政 治 大. ‧. ‧ 國. 學. er. io. sit. y. Nat. measured by patient satisfaction (Turner 1995). Moreover, value assessments from different perspectives may be highly interrelated. Past literature has found that service provider satisfaction and patient perception of care have a strong, positive correlation. In contrast, service provider dissatisfaction has an adverse, negative effect on patient loyalty, hospital profitability, and quality of care (Atkins 1996).. al. n. v i n C h assessmentsUare now even more important, Such multi-perspective performance engchi because e-Health, through information technology (IT), has developed a new. relationship between patients and service providers that differs from general health care services. For example, service providers can now educate patients using online resources and encourage patient-to-patient sharing via e-Health system platforms (Eysenbach 2001). While few published articles have addressed both patient and service provider perceptions in the context of e-Health, the main aim of this study is to develop quality evaluation criteria that consider both service provider satisfaction and patient value perspective in assessing e-Health services and to evaluate the impact of these criteria on the performance of e-Health services. Specifically, the key objectives are to (a) provide an e-Health performance assessment framework, (b) to develop a scale that evaluates e-Health service quality, while considering multiple perspectives, and (c) to 1.
(6) demonstrate the strong relationship between service provider and patient value perspectives in e-Health.. 立. 政 治 大. ‧. ‧ 國. 學. n. er. io. sit. y. Nat. al. Ch. engchi. 2. i n U. v.
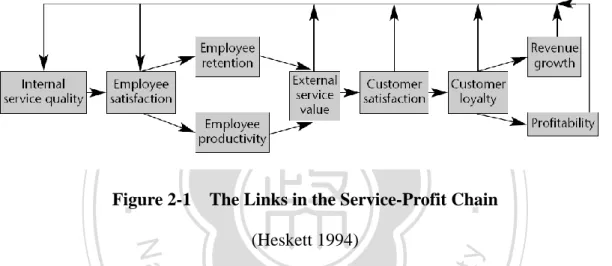
(7) CHAPTER 2 – LITERATURE REVIEW To explain the relationship between profitability, service value, and service quality, Heskett et al. (1994) developed a theory and business model, known as the service-profit chain. The links in the chain are as follows: Profit and growth are both affected by customer loyalty, which is largely influenced by customer satisfaction. Customer satisfaction is a direct result of service value, which is created by employees’ productivity and performance. Employee satisfaction is a result from high-quality support services and policies. (See Figure 2-1). 立. 政 治 大. ‧. ‧ 國. 學. Figure 2-1. The Links in the Service-Profit Chain. y. sit. Nat. (Heskett 1994). n. al. er. io. We can infer from Figure 2-1 that the internal service quality indirectly impacts the external service value through the service delivery system; the external service value then directly influences customer satisfaction and indirectly changes customer intention. Therefore, to understand the relationship between service value delivery and service performance, we should start by looking at the internal service quality and external service value components.. Ch. engchi. i n U. v. 2.1 Internal Service Quality Although internal service quality has been extensively studied over the past two decades, it is still an important factor in assessing service performance. In relevant literature, quality is viewed as an overall assessment of the gap between the customer’s expectations and their perception of the service; it is usually measured by the following factors: tangibles, reliability, responsiveness, assurance, and empathy (Parasuraman 1988). 3.
(8) In previous years, research has focused only on two service roles when considering service quality: the service receiver and service provider (Heskett 1994; Kumar 2008). Teboul (2006) has extended the two-role model to come up with the service triangle and redrawn the relationships so that the firm is placed at the top of the triangle, and customers and employees are placed on an equal level at the bottom. The firm sells the service to those who are going to provide it, the employees deliver and market services, and the customers participate through consumption and co-creation. The service triangle model highlights the process by which people (employees and customers) play an important part in service delivery. Other important internal service quality elements include the business and employee values (Teboul 2006), which will be discussed in the section below. Customer value, which is an important part of external service value, will be discussed in section 2. 2.. 治 政 大 2.1.1 Business Value of Firms 立 ‧ 國. 學. ‧. In recent years, companies have emphasized the idea of value creation within the firm. Many studies of business value impacts examine the link between IT investments and the output measures of firm value (Mooney 1996); however, few studies analyze the. er. io. sit. y. Nat. impact of IT on intermediate innovation services, which is unfortunate because this would generate considerable insight into the creation of business value of IT from a service perspective. Additionally, some research suggests that business value may be captured away by trading partners or competitors; and, ultimately, be refined by customers in the form of lower prices and better quality (Bresnahan 1986; Hitt 1996).. al. n. v i n Venkatraman et al. (1986) C have h classified i Uapproaches to the measurement e n g cseveral h of business performance in strategy research and found that in order to understand. what drives business value, managers must to incorporate information from all aspects of business systems, not just the financial performance. The Balanced Scorecard system (Kaplan 1992), for example, has applied this concept well and is implemented by many contemporary firms; it is recognized as one of the most popular performance measurement systems today (Bryant 2004). Since its development in 1990 by Robert Kaplan and David Norton, the Balanced Scorecard has been implemented at the corporate, strategic business unit, departmental, shared-service, and individual levels at hundreds of organizations worldwide, including those in the business and healthcare sectors (Voelker 2001). The Balanced Scorecard incorporates both financial and nonfinancial measures using four hierarchical perspectives: learning and growth, internal business processes, customer, and financial perspectives. The learning and growth perspective is considered the lowest level in the hierarchy and the 4.
(9) financial perspective, the highest (Bryant 2004). The four perspectives can be explained as follows: . Financial Perspective. The financial perspective focuses on measures of importance to the shareholder, such as return-on-capital-employed, project profitability, and cash flow.. . Customer Perspective. The customer perspective reflects the factors that really matter to customers, including waiting time, quality, performance, and cost.. . Internal Business Perspective. Internal business perspective emphasizes the excellence of critical internal operations, such as processes, decisions, and actions already undertaken.. 政 治 大 firms to innovate, improve, and learn. Examples of this include: launching 立 new products or services, creating more value for customers, and improving. Learning and Growth Perspective. This perspective stresses the ability of. ‧ 國. 學. operating efficiencies on a long term scale.. (Kaplan 1992). ‧. n. al. er. io. sit. y. Nat. The Balanced Scorecard thus effectively combines the financial and operational measures needed to achieve customer satisfaction, efficient internal processes, and innovative and improved business techniques. For this reason, we will utilize the Balanced Scoreboard method to measure the business value of firms in this study.. 2.1.2 Employee Value. Ch. engchi. i n U. v. Getting employees to become customer-oriented and to work as part of the firm’s team is the best way to improve service quality (Joseph 1996). The company should make the process of attracting, developing, motivating, and retaining qualified employees a priority; however, understanding the needs of the employee goes beyond simply promoting a good work environment (Benson 2003). In the healthcare sector, for example, employees have to face the challenges, including advances in technology and changes in the demographics and diversity of the workforce; thus, to achieve the highest value of customer satisfaction, employers must strive to satisfy their employees’ needs by enhancing job value (Berry 1991). According to Joseph (1996), co-opting good employees in healthcare should be considered a mutual investment by both the employees and the heads of the 5.
(10) organization. To accomplish this, he proposes the implementation of the following three policies: ―use of financial rewards,‖ ―expanded career paths,‖ and ―support for diverse employee lifestyles‖. Kalleberg (1977) examines the relationship between employee satisfaction and the work values associated with six dimensions of work— “ intrinsic‖,. ―convenience‖,. ―financial‖,. ―co-worker. relationship‖,. ―career. opportunity‖ and ―resource adequacy‖. The ―intrinsic‖ dimension refers to the characteristics of the task itself, whether it generates intellectual interest, motivates learning, or encourages improved performance. ―Convenience‖ refers to job characteristics that provide solid creature comforts that include, but are not limited to adequate time to accomplish the task, work environment, and amount of workload. The ―financial‖ dimension concerns what employees get, including salary, financial well-being, and job security. ―Co-worker relationship‖ includes factors such as whether the job allows chances to make friends, whether the co-workers are friendly, and whether those o-workers take a personal interest in him or her. ―Career opportunity‖ regards work promotion and whether those chances are fair and achievable. The final dimension is ―resource adequacy,‖ which is about satisfying the worker’s needs for adequate information and equipment to effectively complete the. 立. 政 治 大. ‧ 國. 學. ‧. task. In 1959, Herzberg published the two-factor theory that generalized employee motivation into two factors—“hygiene‖ and ―motivator‖. Later on, upon analyzing. io. sit. y. Nat. the content of employee’s perception of job value, Nathan King found that the motivator was dominated by the intrinsic aspects of the job, while hygiene was dominated by the extrinsic factors (King 1970).. n. al. er. Maslow (1970) suggests that human motivation should be arranged according to five hierarchies of needs. Physiological needs form the base of the hierarchy, followed by ―security‖, ―belongingness‖, ―esteem‖, and ―self-actualization‖ needs in ascending order. In order to understand and motivate health care employees, Benson and Dundis (2003) have applied Maslow's hierarchy of needs theory to training and technology. According to their research, the hierarchy of needs theory is explained as follows:. Ch. engchi. i n U. v. . Basic needs. Basic needs must be met with wages, which in turn provide shelter, food, water, heat, clothing, etc.. . Security. Safety on the job includes not only physical, but mental safety. A secure working environment can also mean decreased anxiety produced by adequate benefits, union contracts, etc.. . Belongingness. Employees seek pleasant working relationships with co-workers, peers, and others in the hierarchy. 6.
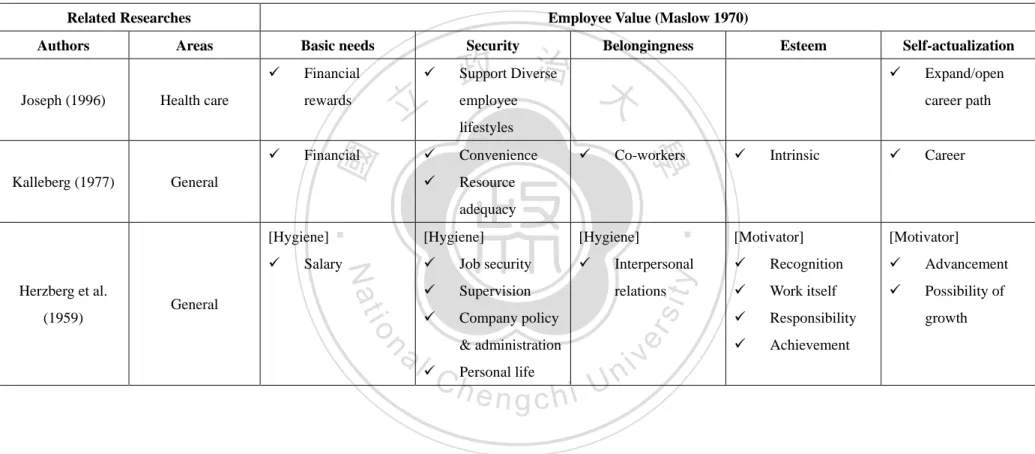
(11) . Esteem. Self-esteem in the organization is generally based on the individual’s successful performance appraisals, incentives, rewards received, and recognitions obtained, all which enhance self-confidence.. . Self-actualization. To develop one’s potential, to learn new things, to take risks, and to feel more confident in what one does. (Benson 2003). Considering suitability and integrality of the classification scale (See Table 2-1), the study adopts the Maslow’s model for measuring the employee value in e-Health services.. 立. 政 治 大. ‧. ‧ 國. 學. n. er. io. sit. y. Nat. al. Ch. engchi. 7. i n U. v.
(12) Table 2-1 Comparison of the Employee Value Classification Related Researches Areas. Basic needs . Health care. lifestyles. . Convenience. . Resource. . Co-workers. [Hygiene]. . . Job security. . . Supervision. . Company policy. n. & administration. y. Interpersonal. sit. relations. n C hPersonal life engchi U. . 8. ‧. [Hygiene]. al. Expand/open career path. 學. General. Self-actualization . [Hygiene]. Salary. Esteem. 治 Support Diverse 政 大 employee. adequacy. io. (1959). General. Financial. Nat. Herzberg et al.. 立. rewards. Kalleberg (1977). . Financial. Belongingness. er. Joseph (1996). Security. ‧ 國. Authors. Employee Value (Maslow 1970). iv. . Intrinsic. . Career. [Motivator]. [Motivator]. . Recognition. . Advancement. . Work itself. . Possibility of. . Responsibility. . Achievement. growth.
(13) 2.2 External Service Value Service management literature discusses the relationship between service quality and service value, which can be explained by the following excerpts: . There has been a convergence of opinion that favorable service quality perceptions lead to improved satisfaction and value attributions and that, in turn, positive value directly influences satisfaction…(Cronin 2000)(p. 195). . Service value should be treated as a ratio with service quality as the numerator and sacrifice as the denominator…(Cronin 1997)(p. 376). These studies have posited that service quality positively influences service value.. 治 政 Other studies consider customer perception and attitude, 大 which are summarized by the following excerpts. 立 It is found that customer perceived service quality may influence behavior intentions of customers indirectly by affecting customer value and customer satisfaction…(Wang 2004)(p. 337). . Customers' assessments of service value are positively related to their evaluations of service quality…(Bolton 1991)(p. 383). ‧. ‧ 國. 學. . sit. y. Nat. n. al. er. io. According to these studies, we find that service quality is the result of a customer’s perception of the service value received in a relationship. Behavior intentions of customers may be impacted by customer feeling during service delivery. In this study, external service value is measured by customer perceived service quality, or customer value.. Ch. engchi. i n U. v. 2.2.1 Customer Value Due to intense competition, rapid technological changes, and variable demands of customers, more and more companies are looking for new ways to achieve, preserve, and enhance competitive advantage. Being customer-oriented is the best method for achieving competitive advantage; thus, many firms continually strive to achieve superior customer value delivery (Woodruff 1997; Wang 2004). As some researchers have concluded, customer perceived service value indirectly influences customer behavior intentions (Cronin 2000; Wang 2004). 9.
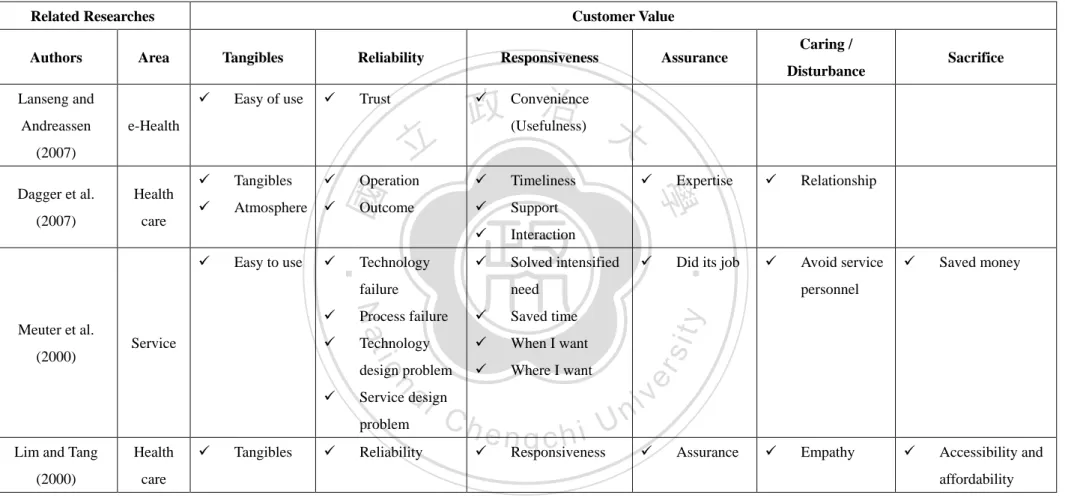
(14) Several models aiming to understand customer perceived service quality and satisfaction have evolved from health care settings. Lanseng and Andreassen (2007) used the Technology Acceptance Model (TAM) theory to explore the impact of“ease of use‖ and ―convenience‖ and their relationships with ―trust‖ in the context of e-Health. In this study, customer satisfaction was measured using nine items derived from Dagger, Sweeney et al.’s (2007) satisfaction scale, namely: interaction, relationship, outcome, expertise, atmosphere, tangibles, timeliness, operation, and support. Another model, SERVQUAL, measures the gap between customer expectations and experiences and has been widely accepted in literature (Rashid 2009). Proposed by Parasuraman et al. (1988), this scale provides five dimensions for measuring service quality. These dimensions are:. 政 治 大. . Tangibles. Physical facilities, equipment, and appearance of personnel.. . Reliability. Ability to perform the promised service dependably and accurately.. . Responsiveness. Willingness to help customers and provide prompt service.. . Assurance. Knowledge and courtesy of employees and their ability to inspire trust and confidence.. . Empathy. Caring, individualized attention that the firm provides its customers.. 立. ‧. ‧ 國. 學. n. er. io. sit. y. Nat. al. Ch. engchi. i n U. v. (Parasuraman 1988). Customer perception of value is equal to the perceived service quality relative to the price and customer acquisition costs (Hallowell 1996). Zeithaml (1988) suggested that customer value should be assessed by the customer’s perceptions of what is received (quality) and what is given (sacrifice). Customer value is something perceived by customers, and those perception processes typically involve a trade-off between customers ―get‖, such as quality, benefits, and utilities, and what they ―give‖, such as price, opportunity cost, and maintenance and learning cost (Wang 2004). To understand customer satisfaction with technology-based service encounters, Meuter et al. (2000) collected a survey of data from several customers with the following criteria for evaluating the service: "solved intensified need", "easy to use", "avoid service personnel", "saved time", "when I want", "where I want", "saved money", "did its job", "technology failure", "process failure", "technology design problem", and "service design problem". After an empirical study done by Lim and 10.
(15) Tang (2000), utilizing the feedback received from the Meuter survey, the final questionnaire rephrased an additional dimension, "affordability." Since these previous studies have focused on customer value in a service environment, we will combine these dimensions together with those specified by SERVQUAL and add ―sacrifice‖ as the sixth dimension to estimate customer value (See Table 2-2).. 立. 政 治 大. ‧. ‧ 國. 學. n. er. io. sit. y. Nat. al. Ch. engchi. 11. i n U. v.
(16) Table 2-2 Comparison of the Customer Value Classification Related Researches Area . Easy of use. Reliability . 立. (2007) Tangibles. . Operation. . Timeliness. . Atmosphere. . Outcome. . Support. . Interaction. . Solved intensified. Easy to use. . Technology failure. . Service. Process failure. . Saved time. Technology. . When I want. . Where I want. io. (2000). design problem. al. n. . Service design problem. Lim and Tang. Health. (2000). care. . Tangibles. . Expertise. . Relationship. . . Avoid service. Did its job. need. Nat. Meuter et al.. . Reliability. Ch. engchi. . . Saved money. . Accessibility and. personnel. y. . ‧ 國. care. Sacrifice. Disturbance. ‧. (2007). . 學. Health. Caring /. Assurance. Convenience 治 政 (Usefulness) 大. Trust. e-Health. Dagger et al.. Responsiveness. sit. Lanseng and Andreassen. Tangibles. er. Authors. Customer Value. i n U. Responsiveness. v. . Assurance. . Empathy. affordability. 12.
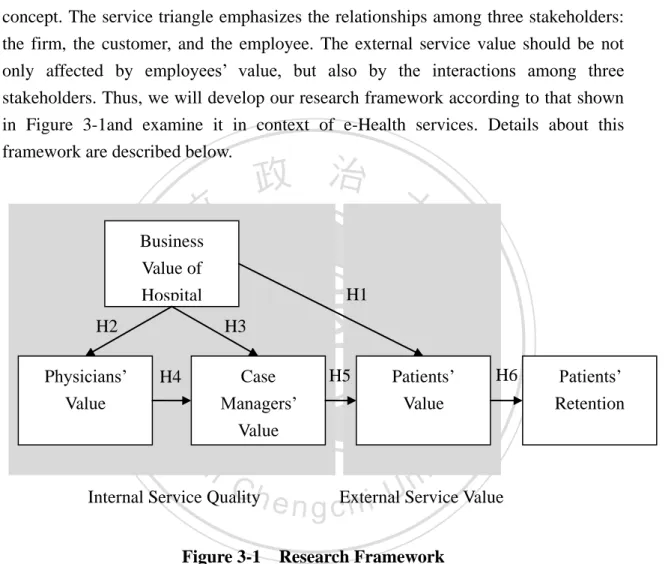
(17) CHAPTER 3 – RESEARCH MODEL AND HYPOTHESES The service-profit chain uses a linear method to explain relationships between internal service quality (i.e. employee value) and external service value (i.e. customer value). In this study, we will extend the service-profit chain by integrating service triangle concept. The service triangle emphasizes the relationships among three stakeholders: the firm, the customer, and the employee. The external service value should be not only affected by employees’ value, but also by the interactions among three stakeholders. Thus, we will develop our research framework according to that shown in Figure 3-1and examine it in context of e-Health services. Details about this framework are described below.. 政 治 大. ‧ 國. ‧. H3 H5. Patients’ Value. H6. Patients’ Retention. er. io. sit. Case Managers’ Value. H4. Nat. Physicians’ Value. 學. H2. H1. y. 立. Business Value of Hospital. al. n. v i n C Internal Service Qualityh e h i UService Value n g cExternal Figure 3-1 Research Framework. 3.1 The Delivery of Firms’ Business Value In general, firms advertise their business value to customers through mass communication, speeches, brochures and/or newsletters (Teboul 2006). Therefore, since hospitals have the potential to increase their business value to potential customers through service marketing of e-Health, we propose that: H1: Business value of hospital is positively related to patient value in e-Health services. 13.
(18) However, any campaign for a new service must be targeted equally towards employees as well as external customers, because employees play an essential part in promoting the service (Teboul 2006); companies need to ensure that employees fully understand the value of their roles and are willing to act as required. Therefore, it is necessary to sell the service to employees before any external marketing takes place--this is known as internal marketing. Through rules or communications, firms offer incentives among service providers to get employees to adopt the marketing concept of customer orientation and to encourage them to become part of the company's team (Joseph 1996). It is important to first enhance the employees’ value before attaining further business value. Although services mostly depends on the experience from front-line service providers, it is still necessary for backstage employees to prepare products and components or process information (Teboul 2006). Thus, in relation to e-Health, we propose that hospitals convey business value to both physicians (backstage staffs) and case managers or nurses (front-line staffs) through internal marketing.. 政 治 大. 立. ‧ 國. 學. H2: Business value of hospital is positively related to physician value in the context of e-Health service.. ‧. H3: Business value of hospital is positively related to case manager value in the context of e-Health service.. n. Ch. engchi. er. io. al. sit. y. Nat. 3.2 The Delivery of Employee Value. iv n stage U (Teboul. Back-stage activities exist to support the front 2006); therefore, front-line and backstage employees act in a cooperative relationship and should be observed as a team. For example, a restaurant waiter cannot accept meal orders without backup support from employees in the kitchen. Furthermore, we predict that backstage employees who have acquired high value from the service will be more willing to cooperate with front-line employees. In context of e-Health, case managers who receive better support from physicians will be more able to deliver services to patients and will thus hold a higher value for the e-Health service and themselves. We hypothesize that: H4: Physician value is positively related to case mangers value in the context of e-Health service. On the other hand, service marketing is not just for the front-line employees; it is just as important that these employees deliver service quality to ultimate consumers 14.
(19) (Joseph 1996). Customers today are strongly value oriented, so while the firm may advertise value through mass communication, brochures or newsletters, the front-line employees are ultimately the ones who directly interact with the customers and prove that they offer quality service. For this reason, we believe that the extent of value held by the front-line employees directly affects the value that is delivered to customers. Teboul (2006) believed that the relationship between frontline staff and customers becomes predominant. In e-Health service, patients were shown real service content through a caring and FAQ process from case managers. Consequently, we propose that case managers’ value has a positive relationship with patient value. H5: Case manager value is positively related to patient value in the context of e-Health service.. 治 and Retention 政 Value 3.3 The Delivery of Customer 大. 立. ‧. ‧ 國. 學. Customers who have already experienced the service have some power over the business-customer relationship, because they can decide whether or not to repurchase or advocate the service (Teboul 2006). In fact, when referrals are added to the economics of customer retention and repeat purchases of related products, the lifetime. n. al. er. io. sit. y. Nat. value of a loyal customer may be astronomical (Heskett 1994). According to Reichheld and Sasser’s (1990) estimation, a 5% increase in customer loyalty can increase profit from 25% to 85%. However, a customer’s intention to stay with a particular business is usually determined by the value they receive in relation to the total costs. In terms of e-Health, the quality of healthcare received and medical outcome may influence a patient’s intention to remain loyal. Based on this, we hypothesize that there is a positive relationship between patients’ value and patient retention in the context of e-Health services.. Ch. engchi. i n U. v. H6: Patient value is positively related to patient retention in the context of e-Health services. The above hypotheses can be tested empirically by calculating the significant path coefficients. In the following section, we will elaborate on the methodology which is going to be used in this study.. 15.
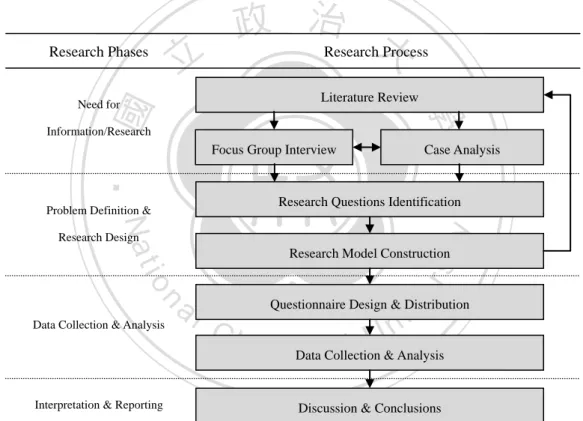
(20) CHAPTER 4 – RESEARCH METHODOLOGY The first step in this study was to review all relevant literature on performance assessments and e-Health services in order to create an overview of performance evaluation approaches and to have a better understanding of e-Health (Figure 4-1). During the course of the focus group interview, we discovered that different stakeholders contribute valuable, individual viewpoints; as a result of this, we researched different theories relating to value assessments by different individuals and developed a research model that explains how each stakeholder’s value assessment impacts another’s perceptive value. Through case data analysis, we developed several hypotheses that demonstrate the relationship between different stakeholders.. 立. Research Phases. 政 治 大 Research Process Literature Review. ‧ 國. 學. Need for. Information/Research. Focus Group Interview. Case Analysis. ‧. Research Questions Identification. Problem Definition &. y. Nat. Research Model Construction. n. al. er. io. sit. Research Design. Data Collection & Analysis. Interpretation & Reporting. i n U. v. Questionnaire Design & Distribution. Ch. e n gDatacCollection h i & Analysis Discussion & Conclusions. Figure 4-1 Research Process Map. 16.
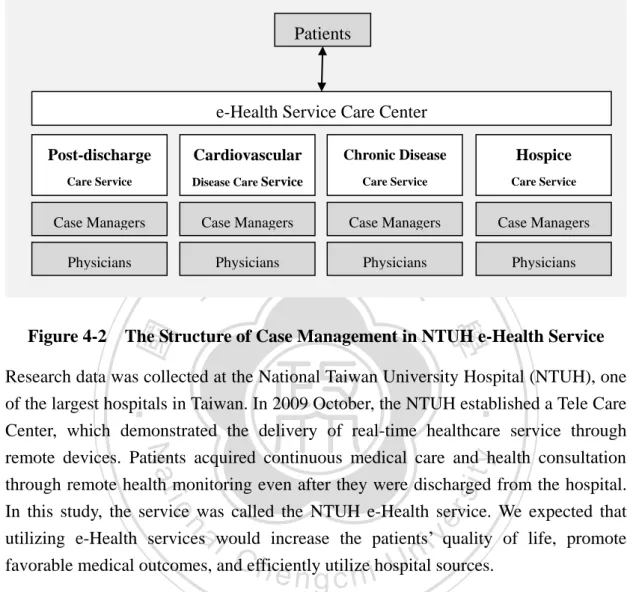
(21) 4.1 Case Background. Patients. e-Health Service Care Center Post-discharge. Cardiovascular. Chronic Disease. Hospice. Care Service. Disease Care Service. Care Service. Care Service. Case Managers. Case Managers. Case Managers. Case Managers. Physicians. Physicians. Physicians. ‧ 國. 學. Figure 4-2. 立. 政 治Physicians 大. The Structure of Case Management in NTUH e-Health Service. ‧. Research data was collected at the National Taiwan University Hospital (NTUH), one of the largest hospitals in Taiwan. In 2009 October, the NTUH established a Tele Care. n. al. er. io. sit. y. Nat. Center, which demonstrated the delivery of real-time healthcare service through remote devices. Patients acquired continuous medical care and health consultation through remote health monitoring even after they were discharged from the hospital. In this study, the service was called the NTUH e-Health service. We expected that utilizing e-Health services would increase the patients’ quality of life, promote favorable medical outcomes, and efficiently utilize hospital sources.. Ch. engchi. i n U. v. Depending on different medical situations, the e-Health service generally comprised of four service categories. Each care service had its own case managers who monitored the patient health and provided urgent consultation, while patients uploaded daily health information and called in for help. Physicians supported the care service by providing professional medical suggestions and arranging the outpatient services if necessary (please refer to Figure 4-2). Because of the different diseases and degree of illness, each care service offered similar but not identical service content. The summarized descriptions of these service categories are listed in Table 4-1.. 17.
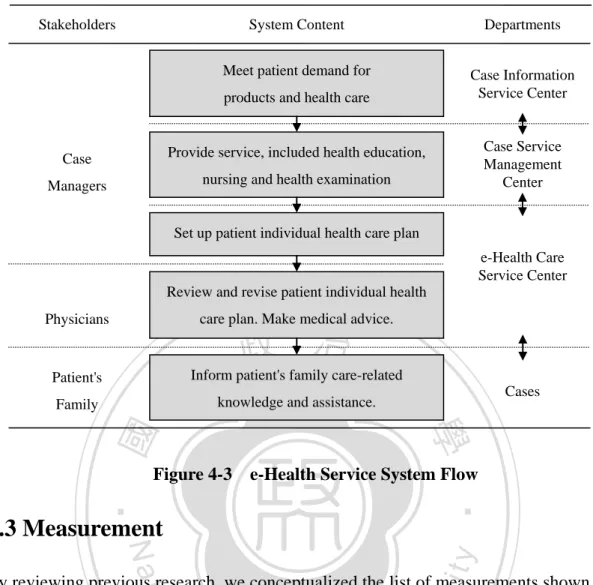
(22) Table 4-1 Description of The Three Service Categories in This Case Service Categories. Post-discharge Care Service. Cardiovascular Disease Care Service. Main Diseases. Respiratory and thoracic disorders, organ recession, and liver cirrhosis About 08:00-24:00. Cardiopathy. Diabetes and hypertension. Terminal cancer. 24hours. 24hours. 24hours. Free. NT$5000 per month (first months for free). Supplied Devices. Non (self-provided). Baby Bat (multiple function device). NT$100 per day (first months for free) Big Eyes (One-Way Live Video Equipment). Service Provider Service Content. 3 Physicians & 8 Case Managers Tele-monitoring (5 calls one month) Tele-consultation. 3 Physicians & 9 Case Managers Tele-monitoring (more than 2 calls per week) Tele-consultation. NT$400 per month (first three months for free) Specific glucose meter & Blood Pressure Monitor 5 Physicians & 11 Case Managers Tele-monitoring (3 or 4 calls per week) Tele-consultation. Need for Data. . . 政 治 大. Blood Pressure Blood Sugar. n. Ch. 4.2 System Background. engchi. 3 Physicians & 5 Case Managers Tele-monitoring (5 calls per week) Tele-consultation Tele-diagnosis Lifetime Health Non-fixed. sit. y. ‧. io. al. Blood Pressure Blood Sugar Weight Body Temperature Peak Flow Reading Electrocardiogram Oxyhemoglobin Saturation. 學. Nat. Blood Pressure Blood Sugar Weight Abdominal Circumference. Hospice Care Service. er. 立. ‧ 國. Service Time Service Charge. Chronic Disease Care Service. i n U. v. IT in e-Health service promoted the development of a new relationship between patients and service providers that differed from general health care services. The combination of case relationship management and communication integration platforms in e-Health is called ―U-Care‖. Used mainly for health consultation, patient referral, and case closing management, U-Care also integrates and stores record of interaction, disease diagnosis, and health planning. The system flow is presented in Figure 4-3.. 18.
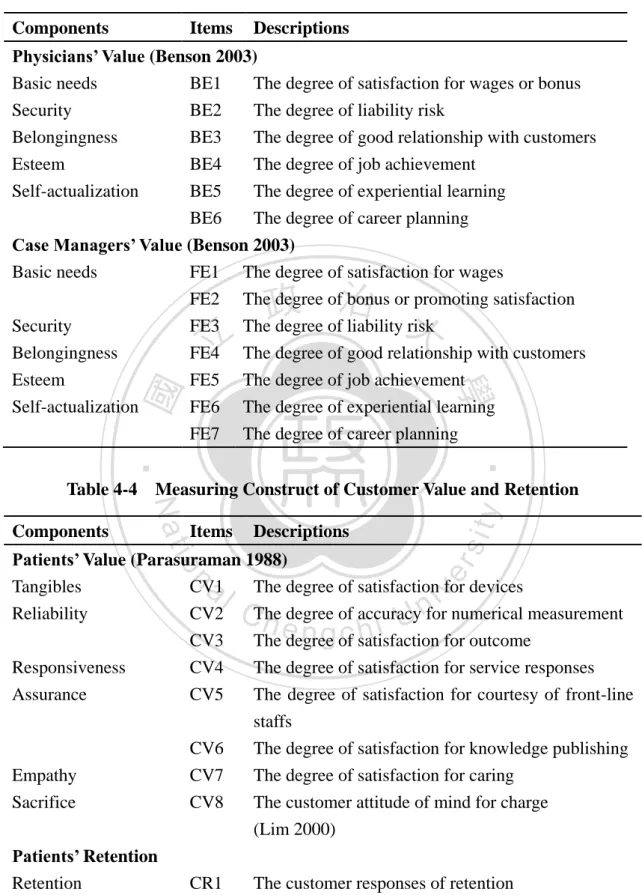
(23) Stakeholders. System Content. Departments. Meet patient demand for. Case Information Service Center. products and health care. Case. Provide service, included health education,. Managers. nursing and health examination. Case Service Management Center. Set up patient individual health care plan e-Health Care Service Center Review and revise patient individual health care plan. Make medical advice.. Physicians. 政 治 大 patient's family care-related 立Informknowledge and assistance.. Patient's. Cases. 學 Figure 4-3 e-Health Service System Flow. ‧. ‧ 國. Family. 4.3 Measurement. sit. y. Nat. n. al. er. io. By reviewing previous research, we conceptualized the list of measurements shown in Table 4-2 to 4-4. The proposed model in total has 25 evaluation components with at least 4 components in each one of five dimensions, resulting in an initial pool of 32 criteria. Sample questions for each item were presented using a five-point Likert scale with verbal anchors ranging from strongly disagree (1 point) to strongly agree (5 points), and patient retention was measured using true or false questioning. The completed questionnaires can be found in Appendices A through C for the different subjects (physicians, case managers, and patients).. Ch. engchi. i n U. v. Table 4-2 Measuring Construct of the Delivery of Firms’ Business Value Components. Items Descriptions. Business Value of Hospital (Kaplan 1992) Financial BV1 The degree of firm’s financial performance Customer Internal business Learning and growth. BV2 BV3 BV4 BV5. The degree of customer satisfaction The degree of good outcome for customers The degree of firm’s internal process The degree of firm’s reputation 19.
(24) Table 4-3 Measuring Construct of Employee Value Delivery Components. Items. Descriptions. Physicians’ Value (Benson 2003) Basic needs BE1 The degree of satisfaction for wages or bonus Security BE2 The degree of liability risk Belongingness BE3 The degree of good relationship with customers Esteem BE4 The degree of job achievement Self-actualization BE5 The degree of experiential learning BE6 The degree of career planning Case Managers’ Value (Benson 2003) Basic needs FE1 The degree of satisfaction for wages FE2 The degree of bonus or promoting satisfaction Security FE3 The degree of liability risk Belongingness FE4 The degree of good relationship with customers Esteem FE5 The degree of job achievement Self-actualization FE6 The degree of experiential learning FE7 The degree of career planning. 立. 政 治 大. ‧. ‧ 國. 學. y. Items. sit. Components. Nat. Table 4-4 Measuring Construct of Customer Value and Retention Descriptions. n. al. er. io. Patients’ Value (Parasuraman 1988) Tangibles CV1 The degree of satisfaction for devices Reliability CV2 The degree of accuracy for numerical measurement CV3 The degree of satisfaction for outcome Responsiveness CV4 The degree of satisfaction for service responses Assurance CV5 The degree of satisfaction for courtesy of front-line staffs CV6 The degree of satisfaction for knowledge publishing Empathy CV7 The degree of satisfaction for caring Sacrifice CV8 The customer attitude of mind for charge (Lim 2000) Patients’ Retention Retention. CR1. Ch. engchi. i n U. v. The customer responses of retention. 20.
(25) 4.4 Data Collection In order to discover the value of e-Health service, this study collected data by the survey in two steps. First, through focus group discussions regarding e-Health service at NTUH (Please see Appendix D for original Chinese interview questions), we collected a significant amount data from six physicians and eight case managers (please refer to Table 4-5 for the related list,). Second, after analyzing the data collected from the focus groups, we sent questionnaires to the physicians, case managers, and patients involved in e-Health service at NTUH. However, while we were surveying this four service categories, the cardiovascular disease care service closed their e-Health program, thus we had to rely on the other three service categories for our research subjects.. 政 治 大. Moreover, due to the fact that patient information is highly confidential data, the hospital didn’t want to interfere with patients and their families. Thus, we adopted the following two methods of analysis: questionnaire analyses and case studies. The questionnaire analysis method was used to measure the internal service quality of e-Health, focusing on the relationship between the business value of hospital, physicians’ value, and case managers’ value. We sent questionnaires to 10 physicians. 立. ‧. ‧ 國. 學. n. al. er. io. sit. y. Nat. and 16 case managers (the related list, please refer to Table 4-5), and received 100% replies. The case study was a detailed analysis of patient value from the focus group transcript that was adopted to discover external service value. As for patient retention, because the e-Health care service program was actually implemented for only less than a year and the service charge was calculated on a day-today basis due to the frequency of dying patients, we found it too difficult to accurately calculate. Consequently, we referred to meeting records of the NTUH e-Health service program and calculated the rate of case growth from January 2011 to May to instead of finding patient retention.. Ch. engchi. i n U. v. Table 4-5 The List of Samples Focus Group Interviews. Service Category. Physicians. Case Managers. Questionnaire Survey Physicians. Case Managers. Post-discharge Care Service Cardiovascular Disease Service. 2 2. 3 3. 3 0. 5 0. Chronic Disease Care Service Hospice Care Service. 1 1. 1 1. 5 2. 7 4. Total. 6. 8. 10. 16. 21.
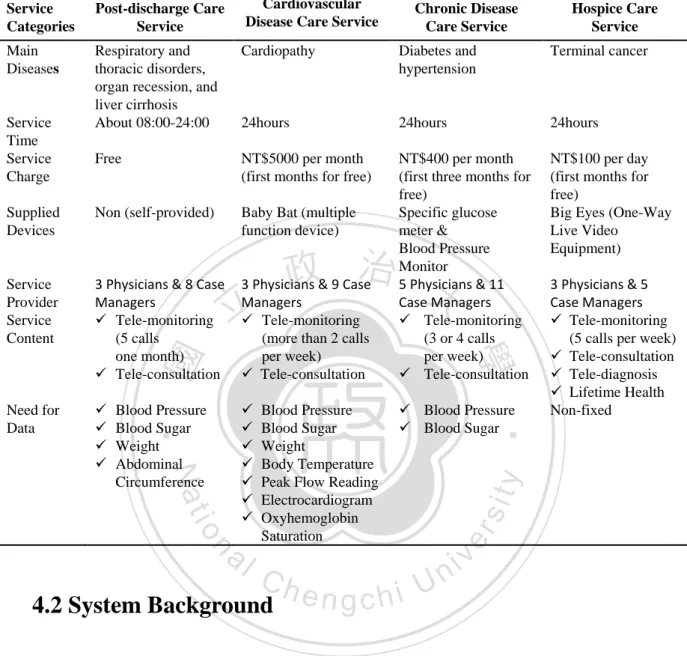
(26) 4.5 Framework Application Using these three e-Health service designs and providers, can internal service value deliver value to external service quality? What’s the influence relationship between stakeholders in e-Health? In this section, we will show a summary of the questionnaire analyses and the result of the case interpretations based on research framework we proposed on Table 4-6. Table 4-6 Summary of Analysis Results Post-discharge Care Service. Components. Business Value of Hospital 3.88. Cardiovascular Chronic Disease Hospice Care Disease Care Care Service Service Service X. 3.95. 5.00. 3.67. Customer. 3.83. Internal business. 4.33. X. 4.00. 5.00. Learning and growth. 3.67. X. 4.20. 5.00. Physicians’ Value. 3.07. X. 3.10. 5.00. X. 2.60. 0.67. X. 2.20. 3.50. 3.67. X. 3.80. ‧. 3.33. X. 3.40. y. 4.00. 2.67. X. 3.50. sit. 政 XX 治 大3.40 4.20. Financial. 4.25. X. 3.39. Self-actualization. Nat. Esteem. io. Case Mangers’ Value. al. n. Basic needs. 4.10 3.70. Security. 4.00. Belongingness. 4.40. Esteem. Ch. X. e nX g c h i. i n U3.00. 2.36. 4.35 5.00. er. Belongingness. ‧ 國. Security. 5.00. 學. Basic needs. 立. 5.00. v. 5.00. 3.08 1.88 2.50. X. 4.29. 3.50. 4.20. X. 3.43. 3.25. Self-actualization. 4.20. X. 3.86. 4.25. Patients’ Value. Low-medium. Medium-high. Medium. High. Tangibles. Low. High. Medium. Medium. Reliability. High. Low. Medium. High. Responsiveness. Low. High. Medium. Medium. Assurance. Medium. High. Low. High. Empathy. Low. Medium. Medium. High. Sacrifice*. Low. High. Low. Medium. Rate of Case Growth. 77%. 117%. 212%. 300%. Note1: Scoring features: 1: Strongly disagree, 2: Disagree, 3: No opinion, 4: Agree, 5: Strongly agree Note2: * reverse component 22.
(27) Business Value of Hospital Some of physicians in the case took a stance on program implementation; from their responses, the results suggest that financial, customer, internal business, and learning and growth are all of equal importance. In addition, their responses reflect that hospice care service has the highest business value within the hospital, in comparison to post-discharge care and chronic disease care. We considered that hospice patients paid charges on a daily basis, which would directly affect quality of performance. E-Health care service would also be the most helpful for patients in hospice care, especially if they had required home care; additionally, it would raise the reputation of hospital and improve internal operations. Physicians’ Value. 政 治 大. Referring to Table 4-5, the questionnaire results displayed that ―belongingness‖ is the highest perceived value by physicians and ―security‖ is the lowest. It could be explained that e-Health care led to a closer relationship between the physician and patient, but it consequently brought physicians more responsibility and risks. On the other hand, hospice care physicians also felt the highest value in comparison to post-discharge care and chronic disease care. This might mean that physicians in hospice care felt that their patients could be well taken care of using e-Health care. 立. ‧. ‧ 國. 學. services, which would’ve indirectly helped their jobs and increased confidence.. y. Nat. io. sit. Case Managers’ Value. n. al. er. After analyzing the questionnaire, we found that case managers tended to believe that ―basic needs‖ had the lowest value out of choices: basic needs, security, belongingness, esteem and self-actualization. This result could be explained by the fact that case managers commonly aren’t satisfied with their wages. On the other hand, after comparing the three services, including post-discharge care, chronic disease care, and hospice care, we found that case managers’ value of hospice care service was the lowest between the three sectors. This situation will be discussed in the next chapter.. Ch. engchi. i n U. v. Patients’ Value (for original Chinese content of interviews, see Appendix E) Tangibles. In the case, the accessible tangibles that the patients came in contact with were: the hospital indoor environment, medical devices, and case managers/nurses. Among them, medical devices affect patients’ value the most. According to case managers, e-Health care service is an innovative services for patients so that they worried whether the device is easy to operate. Out of the three different e-Health service categories that had similar conditions and the same number of service providers, only cardiovascular disease care services supplied devices had different 23.
(28) functions and interfaces; cardiovascular care facilities require highly complex medical devices for data measurements, such as blood pressure, blood sugar, weight, body temperature, peak flow reading, electrocardiogram readings, and oxyhemoglobin saturation. Chronic disease care service and hospice care service offered only the basic equipment (see Table 4-1). Additionally, post-discharge care service did not provide any equipment and encouraged patients to provide these measuring devices themselves. Hence, the degree of patient perceptive value degrees can be easily differentiated by analyzing the function complexity of medical devices. Accordingly, services offering more complex devices such as cardiovascular disease care resulted in a ―high‖ value of tangibles, whereas services that offered minimally complex devices such as chronic disease care and hospice care had ―medium‖ and ―low‖ ratings, respectively, Post-discharge care service had the lowest ratings for tangibles.. 政 治 大. Reliability. Each of the four types of disease conditions needed tele-monitoring services to make optimize patient health care planning; these monitoring systems played an important role in delivering e-health service. As the case managers mentioned, ―when measuring devices were inaccurate or monitoring system was unstable, patients worried greatly and called the e-Health service care center to confirm whether the information had been correctly delivered.‖ Using this case, we made an estimation of ―reliability‖ based on patient anxiety in response to device. 立. ‧. ‧ 國. 學. n. al. er. io. sit. y. Nat. dependency. Comparing these four service categories, post-discharge care, cardiovascular disease care, and hospice care had higher device dependency than chronic disease care service. Cardiovascular disease care service, in particular, had many equipment failures and out of order issues that made patients feel anxious. As a result post-discharge care and hospice care had ―high‖ values of reliability, chronic disease care had ―medium‖ values, and cardiovascular disease care had ―low‖ values.. Ch. engchi. i n U. v. Responsiveness. Tele-consultation service in this study offered a channel for patients or their family to call for help; in this situation, case managers would try their best to answer the patient’s and/or their family’s question. One case manager has commented that ―patients feel satisfied about this service, because they can call-in for help besides regular office hours.‖ Although these four service categories all had tele-consultation service, they were not all in real time. Therefore, we could easily make an estimate regarding the ―responsiveness‖ value by analyzing whether the patients received prompt responses from the e-Health care service center. Service time for post-discharge care service was only available from about 8 a.m. to 12 p.m. (refer to Table 4-1). In contrast, the other three service categories had 24 hours service, with the chronic disease care service and hospice care service only providing basic consultations during daytime working hours due to their night shift on call policy. We 24.
(29) found that ―responsiveness‖ remained ―high‖ with cardiovascular disease care, ―medium‖ with chronic disease care and hospice care, and ―low‖ with post-discharge care service. Assurance. Different diseases require different expertise, but some diseases are so common in the nation that many people have some knowledge about how to control it. However, if patients or their families do not know how the disease develops and how to control it; they would lose confidence and trust. For instance, a case manger in hospice care said ―patients' families were anxious about follow-up caring after discharge, but they became more relieved while they joined in e-Health service.‖ Therefore, we could measure ―assurance‖ through extent of knowledge provided by case managers or physicians. Cardiovascular disease and hospice care tend to be difficult to diagnose and unstable and tend to present a knowledge barrier for most people. Chronic diseases need long-term control and are easier to obtain related care information compared to other diseases. For these reasons, the ―responsiveness‖ value is ―high‖ for cardiovascular disease care, ―medium‖ for chronic disease care and hospice care, and ―low‖ for post-discharge care service.. 立. 政 治 大. ‧ 國. 學. ‧. Empathy. Active caring through phone calls is a direct expression of empathy to patients in e-Health cases. One case manager commented that the call-out services are. n. al. er. io. sit. y. Nat. especially beneficial to elderly patients who live alone; they feel cared for when they receive phone calls from the center.‖ Caring service is often carried out in different frequencies in each service category (see Table 4-1), so we’ve use caring frequency as a symbol of ―empathy‖ degree. Hospice care service had the most frequent caring; cardiovascular disease care and chronic disease care service had similar frequencies, which were both higher than that exhibited by post-discharge care service. Thus, the result of ―empathy‖ value was ―high‖ with hospice care, ―medium‖ with cardiovascular disease care and chronic disease care, and ―low‖ with post-discharge care service.. Ch. engchi. i n U. v. Sacrifice. One physician has commented about the service fee. He believed that a large portion of patients might not afford the service and would be very possible to discontinue the service after free-trial. Although we could easily sort degree of ―sacrifice‖ by service charge (see Table 4-1), patients also needed to prepare the device by themselves in some cases, as with post-discharge service. Hence, we included both service price and patient acquisition costs as adequate measures of patient ―sacrifice‖. The result of ―sacrifice‖ value was ―high‖ with cardiovascular disease care, ―medium‖ with hospice care, and ―low‖ with post-discharge care and chronic disease care service. 25.
(30) CHAPTER 5 – RESULTS AND DISCUSSION 5.1 Summary Figure 5-1 summarizes the case analysis. Hospice care service has the highest perceptive value from the viewpoints of the hospital, physicians, and patients; similarly, hospice care service performance also had the rate of case growth. Chronic disease care and post-discharge care services, on the other hand, were ranked second and third, respectively, in terms of case growth rate and value determined by hospital, physicians, and patients. As a result, we became aware of the positive relationship between business value of hospital, physicians’ value, patients’ value and the rate of case growth for these four dimensions. Case managers’ value, however, was non-positively related to hospital, physicians’ value, patients’ value and rate of case growth. In sum, the result of these case analyses supports hypothesis of H1, H2 and H6, but notH3, H4, and H5. In next section, we will discuss and analyze the results of research model.. 立. 政 治 大. Case Mangers’ Value. Patients’ Value. n. er. io. al. sit. Rate of Case Growth. y. ‧. ‧ 國. 學. Physicians’ Value. Nat. Business Value of Hospital. Ch. engchi. i n U. v. 5. High. 212% 3.95 3.39 3.1. 4.1 3.88 3.07. 300%. 4.35 3.08. Medium. 77% Low-medium. Post-discharge Care Service. Chronic Disease Care Service. Hospice Care Service. Figure 5-1 Summary of Case Analysis 26.
(31) 5.2 Findings After reviewing the research model and testing the hypotheses we proposed, we discussed the results and summarized four findings in the case, shown below. The results of our after-review research model are displayed in Figure 5-2. Business value of hospital could be positively delivered to patients by promotion specialists and activities in e-Health service. In the case, the four care services all implemented promotions with free trial in order to increase their number of patients (see Table 4-1). Through trial experience and message communicating, e-Health service value could deliver to patients more quickly and thus increase patient value. In the interview, some of physicians thought e-Health service needed promotion specialists to deliver virtual value to patients, as well to dispel any doubts that patients might have about e-Health being useless or untrustworthy.. 立. 政 治 大. ‧ 國. 學. ‧. Physicians benefit from the business value of the hospital and are able to positively deliver value to patients using e-Health service.. n. al. er. io. sit. y. Nat. Physicians have a special and important role in e-Health. Because several major physicians took charge in planning and executing this e-Health service center program, these physicians can directly understand and adapt the target business value of hospital. On the other hand, physicians are also like promotion specialists in that they can encourage patients to join e-Health service and explain its value to their patients. When physicians meet patients who decided to use e-Health services during clinic, patient might directly ask about the disease situation or e-Health, in which case the physician could give some suggestions or care. Through this, patients would have more confidence and trust in e-Health. Accordingly, physicians would then positively deliver value to patients in e-Health service.. Ch. engchi. i n U. v. The relationship between physicians and case managers’ does not support a positive relation in e-Health service. Case managers consider their job to be similar to a nurse’s, though without a clear job position or professional training. Case managers say they need complete e-Health care professional training, but all the service processes and expertise end up being built by cumulative experience. Furthermore, case managers were not able to perceive value from hospital value delivery, because their job exposure to e-Health services was relatively shorter than that of a nurse’s, and because they received a lower salary on 27.
(32) average; for this reason, case managers did not deliver positive value to patients. In the case, we found that the values of ―security‖, ―belongingness‖ and ―esteem‖ perceived by case managers are not positively related in comparison to those values perceived by physicians (refer to Table 4-5). We thought that if physicians give more support to case managers and took on more duties, then case managers would feel more secure. On the other hand, if physicians change belongingness and the patient becomes better, then the physician’s greater sense of accomplishment might negatively affect the case manager sense of being and achievement. The most telling reason for this is that there aren’t adequate, real-time communication channels between physicians and case managers. Usually, case managers are only able to ask physicians questions at weekly meetings; inter-departmental communication should be improved so that case managers would be fully supported by physicians.. 政 治 大. Patient value decides the rate of case growth in the context of e-Health.. 立. ‧. ‧ 國. 學. It’s a simple idea that patients’ value is positively related to rate of case growth in the context of e-Health service. When the patients’ perceptive value was raised, patients were more willing to participate in e-Health care service, which provided the simplest way to assess e-Health performance.. y. Nat. sit H1(+). n. al. H2(+) Physicians’ Value. H4 (?). Ch. H3 (?). engchi H5. Case Managers’ Value. (?). er. io. Business Value of Hospital. i n U. v. Patients’ Value. H6 (+). (+) Internal Service Quality. External Service Value. Figure 5-2 Result of after Reviewing Research Model. 28. Rate of Case Growth.
(33) CHAPTER 6 – CONCLUSION. 6.1 Conclusion This study aimed to provide quality evaluation criteria that consider the value perspectives of multiple stakeholders involved in a service triangle relationship of an e-health service—namely, the hospital, case managers, physicians, and patients. After analyzing our results, we found that hospitals and physicians positively affect the value of patient perspective and that case managers do not. Case managers, in terms of e-Health services, have not been to establish a unique work position, so they have not been able to discover their job value. We suggest that case managers should be given the complete professional training for e-Health care and established certification in the future to boost morale and thus improve service quality. In addition, the most important thing is to ensure smooth and real-time communication between case managers and physicians. In the past, few published articles have addressed the issue of multiple value perspective interactions in an e-Health service setting. In the study, we reviewed. 立. 政 治 大. ‧. ‧ 國. 學. n. al. er. io. sit. y. Nat. several value components of performance and redefined them for suiting the context of e-Health care service. Therefore, this study contributed to literature by providing an e-Health service performance assessment framework, which systematically developed a scale for evaluating e-Health service quality in terms of the value perspectives of multiple stakeholders and their interactions.. Ch. engchi. i n U. v. 6.2 Limitations and Implications of Future Research Although we proposed that performance assessment should include the values of multiple stakeholders, our study was limited in that we couldn’t collect patients’ actual data and that there were too few samples. In the future, with the development of e-Health care, there will be more organizations that will supply e-Health care services with more service content. Future research could include the studies of promotion specialists in e-Health service and expanding the case studies that out of hospital to include nursing home and communities.. 29.
(34) REFERENCES Atkins, P. M., Marshall, B.S., Javalgi, R.G. (1996). "Happy employees lead to loyal patients. Survey of nurses and patients shows a strong link between employee satisfaction and patient loyalty." Journal of Health Care Marketing 16(4): 14-23. Benson, S. G., Dundis, S.P. (2003). "Understanding and motivating health care employees: integrating Maslow's hierarchy of needs, training and technology." Journal of nursing management 11(5): 315-320. Berry, L. L., Ed. (1991). Marketing services: Competing through quality Free Press. Bolton, R. N., Drew, J.H. (1991). "A Multistage Model of Customers' Assessments of Service Quality and Value." Journal of consumer research 17(4): 375-384. Bresnahan, T. F. (1986). "Measuring the Spillovers from Technical Advance: Mainframe Computers in Financial Services." American Economic. 立. 政 治 大. ‧ 國. 學. Review 76(4): 742-755. Bryant, L., Jones, D.A., Widener, S.K. (2004). "Managing value creation within the firm: An examination of multiple performance measures." Journal of. ‧. management accounting research 16(1): 107-131. Cronin, J. J., Brady, M.K., Brand, R.R, Hightower, Jr.R., Shemwell, D.J. (1997). "A cross-sectional test of the effect and conceptualization of service value.". y. Nat. sit. n. al. er. io. Journal of Services Marketing 11(6): 375-391. Cronin, J. J. J., Brady, M.K., Hult, G.T.M. (2000). "Assessing the effects of quality, value, and customer satisfaction on consumer behavioral intentions in service. Ch. i n U. v. environments." Journal of Retailing 76(2): 193-218. Dagger, T. S., Sweeney, J.C., Johnson, L.W. (2007). "A Hierarchical Model of Health Service Quality: Scale Development and Investigation of an Integrated. engchi. Model." Journal of Service Research 10(2): 123-142. Eysenbach, G. (2001). "What is e-health?" Journal of Medical Internet Research 3(2): e20. Hallowell, R. (1996). "The relationships of customer satisfaction, customer loyalty, and profitability: an empirical study." International Journal of Service Industry Management 7(4): 27-42. Hamid, A., Sarmad, A. (2008). "Evaluation of e-health services: user's perspective criteria." Transforming Government: People, Process and Policy 2(4): 243-255. Herzberg, F., Mausner, B., Snyderman, B., Ed. (1959). The motivation to work. New York, Wiley. 30.
(35) Heskett, J. L., Jones, T.O., Loveman, G.W., Sasser, W.E.Jr., Schlesinger, L.A. (1994). "Putting the service-profit chain to work." Harvard Business Review 72: 164-174. Hitt, L. M., Brynjolfsson, E. (1996). "Productivity, Business Profitability, and Consumer Surplus: Three Different Measures of Information Technology Value." MIS Quarterly 20(2): 121-142. Hsu, J., Huang, J., Kinsman, J., Fireman, B., Miller, R., Selby, J., Ortiz, E. (2005). "Use of e-Health services between 1999 and 2002: a growing digital divide." Journal of the American Medical Informatics Association 12(2): 164-171. Joseph, W. B. (1996). "Internal marketing builds service quality." Journal of Health Care Marketing 16(1): 54-59. Kalleberg, A. L. (1977). "Work Values and Job Rewards: A Theory of Job Satisfaction." American Sociological Review 42(1): 124-143. Kaplan, R. S., Norton, D. P. (1992). "The Balanced Scorecard–Measures That Drive. 政 治 大 Performance." Harvard Business Review 70(1): 71-79. 立 King, N. (1970). "Clarification and evaluation of the two-factor theory of job. ‧ 國. 學. ‧. satisfaction." Psychological Bulletin 74(1): 18-31. Kumar, V., Smart, P.A., Maddern, H., Maull, R.S. (2008). "Alternative perspectives on service quality and customer satisfaction: the role of BPM." International. sit. y. Nat. Journal of Service Industry Management 19(2): 176-187. Lankton, N. K., Wilson, E.V. (2007). "Factors Influencing Expectations of e-Health Services within a Direct-Effects Model of User Satisfaction." e-Service. n. al. er. io. Journal 5(2): 85-111. Lanseng, E., J., Andreassen, T.W. (2007). "Electronic healthcare: a study of people's readiness and attitude toward performing self-diagnosis." International Journal. Ch. engchi. i n U. v. of Service Industry Management 18(4): 394-417. Lim, P. C., Tang, N.K.H. (2000). "A study of patients' expectations and satisfaction in Singapore hospitals." International Journal of Health Care Quality Assurance 13(7): 290-299. Maheu, M., Whitten, P., Allen, P. (2001). E-Health, Telehealth, and Telemedicine. San Francisco, CA, Jossey-Bass. Maslow, A. H., Ed. (1970). Motivation and Personality. New York, Harper & Row Meuter, M. L., Ostrom, A.L., Roundtree, R. I., Bitner, M.J. (2000). "Self-service technologies: Understanding customer satisfaction with technology-based service encounters." The Journal of Marketing 64(3): 50-64. Mooney, J. G., Gurbaxani, V., Kraemer, K.L. (1996). "A process oriented framework for assessing the business value of information technology." Database for Advances in Information Systems 27(2): 68-81. 31.
(36) Parasuraman, A., Zeithaml, V.A., Berry, L.L. (1988). "SERVQUAL: A Multiple-Item Scale For Measuring Consumer Perception of Service Quality." Journal of Retailing 64(1): 12-40. Rashid, W. E. W., Jusoff, H.K. (2009). "Service quality in health care setting." International Journal of Health Care Quality Assurance 22(5): 471-482. Reichheld, F. F., Sasser, W.E. Jr. (1990). "Zero defections: quality comes to services." Harvard Business Review 68(5): 105-111. Teboul, J., Ed. (2006). Service is front stage: positioning services for value advantage, Palgrave Macmillan. Turner, P. D., Pol, L.G. (1995). "Beyond patient satisfaction. Broaden the scope of quality measurement by integrating the marketing view with other perspectives." Journal of Health Care Marketing 15(3): 45-49. Venkatraman, N., Ramanujam, V, (1986). "Measurement of business performance in strategy research: A comparison of approaches." Academy of Management. 立. 政 治 大. ‧ 國. 學. Review 11(4): 801-814. Voelker, K. E., Rakich, J.S., French, G.R. (2001). "The Balanced Scorecard in Healthcare Organizations: A Performance Measurement and Strategic. ‧. Planning Methodology." Hospital Topics 79(3): 13-24. Wang, Y., Lo, H.P., Yang, Y. (2004). "An integrated framework for service quality, customer value, satisfaction: Evidence from China's telecommunication. sit. y. Nat. industry." Information Systems Frontiers 6(4): 325-340. Woodruff, R. B. (1997). "Customer Value: The Next Source for Competitive. n. al. er. io. Advantage." Journal of the Academy of Marketing Science 25(2): 139-153. Zeithaml, V. A. (1988). "Consumer perceptions of price, quality, and value: a. Ch. i n U. v. means-end model and synthesis of evidence." Journal of Marketing 52(2): 2-22.. engchi. 32.
(37) Appendix A – Complete Questionnaire for Physicians of “Tele Care Center” in e-Health Service 台大醫院遠距照護醫生意見調查表 醫師編號:. 本問卷採不記名方式,請放心填答. 項目. 題. 目. 5. 4. 3. 2. 第一部分:遠距照護服務 BE1. 對加入遠距照護的醫生,醫院有提供合理的獎勵制度. BE2. 加入遠距照護服務使醫師增加了額外的工作風險責任. BE3. 遠距照護服務會促進醫師與病人之間的良好關係. BE4. 加入遠距照護服務讓我很有成就感. BE5. 治 政 加入遠距照護服務對於自我的學習成長有幫助大 立 加入遠距照護服務對我未來職涯規劃是有幫助的 ‧ 國. 學. BE6 第二部分:醫院整體價值 BV2. 我認為醫院提供遠距照護可以提升病人的滿意度. BV3. 我認為醫院提供遠距照護可以提升病人的治癒率. BV4. 我認為醫院提供遠距照護可以有效改善醫療照護流程. BV5. 2.5 我認為醫院提供遠距照護可以提升醫院的社會觀感. sit. y. ‧. 我認為醫院提供遠距照護可以增加收益. Nat. BV1. n. al. er. io. 註:計分原則:「5 分」表示非常同意;「4 分」表示同意;「3 分」表示普通; 「2 分」表示不同意;「1 分」表示非常不同意。. Ch. engchi. 33. i n U. v. 1.
(38) Appendix B – Complete Questionnaire for Case Managers of “Tele Care Center” in e-Health Service 台大醫院遠距照護個管師意見調查表 個管師編號:. 本問卷採不記名方式,請放心填答. 項目. 題. 目. 5. FE1. 以工作量來看,我滿意目前的薪資水準. FE2. 我滿意目前的獎懲及留任制度. FE3. 這份工作需要擔負的風險和責任是在合理範圍之內. FE4. 與護理人員相較,這份工作更易與病患建立良好關係. FE5. 這份工作讓我很有成就感. FE6. 個管師的工作經驗對自我的學習成長有幫助. FE7. 政 治 大 這份工作對我未來職涯規劃是有幫助的 立. 4. 3. 2. 1. ‧. ‧ 國. 學. 計分原則:「5 分」表示非常同意;「4 分」表示同意;「3 分」表示普通;「2 分」 表示不同意;「1 分」表示非常不同意。. n. er. io. sit. y. Nat. al. Ch. engchi. 34. i n U. v.
(39) Appendix C – Complete Questionnaire for Patients of “Tele Care Center” in e-Health Service 台大醫院遠距照護個案滿意度調查表 個案編號:. 受訪時間:. 醫生編號:. 個案連繫不到 拒訪電話無人接聽其他 項目. 題. 目. 5. 4. 3. 2. 1. 第一部分:個案對於儀器設備之滿意度 CV1. 使用「相關儀器、設備」之滿意程度. CV2. 「相關儀器、設備」量測數據準確度之滿意程度. CV3. 參與服務後,對於病情的控制或改善程度是否滿意. CV6. 對於所提供之健康照護知識是否滿意. ‧ 國. CV4. 學. CV5. 治 政 對於各項問題及時回應及處理的狀況是否滿意大 立 對於遠距照護服務人員服務態度是否滿意. CV7 對於病患的關注程度是否滿意 第二部分:個案對於照護服務之參與態度. ‧. 目前,由於經濟部補助計畫,此項服務有免費試用。但在未來沒有計畫補 助下,可能要改採收費的方式,您的態度是: 若要付費,即不會使用即使要付費,也會使用. CR1. 3.1 未來我對使用此項服務之態度: 不會持續使用會持續使用本人會持續使用外,並會讓家人或友人一起 來使用. n. al. er. io. sit. y. Nat. CV8. Ch. engchi. i n U. v. 註:第一部分計分原則:「5 分」表示非常滿意;「4 分」表示滿意; 「3 分」表示普通;「2 分」表示不滿意;「1 分」表示非常不滿意。. 35.
(40) Appendix D – Question List of the Group Interview (Chinese) Physicians: 1. 現在參與遠距醫療系統計畫的醫師人數?通常是哪些層級和科別? 2. 遠距醫療照護系統對於門診的回診情況有實際影響(回診率降低或提高診斷 準確程度)嗎?而遠距醫療系統的報告會做為門診診斷的參考嗎?有和台大醫 院其他系統做整合(資料同步)嗎? 3. 對於病人的遠距醫療系統報告會醫師會主動固定追蹤參考嗎?還是經由個 管師主動告知病人的特殊狀況?每位個管師會固定和同一個醫生報告嗎? 如何分配? 4. 遠距醫療系統會增加醫師的工作負擔嗎?例如:需要多花時間看病人的報 告。 5. 初步的問題狀況是交由個案師來判斷嗎(例如上傳資料不正常)?到了什麼 樣的層級才需要報告給醫師知情? 6. 醫生對系統介面功能會有操作不易的情況嗎? 7. 醫生在遠距醫療系統扮演了病情諮詢和推廣系統的角色,會不會加重原本就 吃緊的業務,如果會的話,您會希望系統或流程方面應該做什麼樣的改進?. 立. ‧. ‧ 國. 學. 病患需要量測什麼儀器和取得什麼資料嗎?. Nat. y. 8.. 政 治 大. sit. n. al. er. io. Case Managers: 1. 您的病患是否有特別需要哪些遠距醫療儀器或功能?而哪些儀器特別要求 數據必須有高準確性? 2. 您的病患透過遠距醫療服務與您聯繫中有哪些地方特別注意的? 3. 遠距醫療服務的系統介面或報表以哪種方式呈現對病患比較易於理解? 4. 目前的遠距醫療服務的系統介面功能是否有助於病患資料管理?而您還希 望需要有哪些功能? 5. 目前的遠距醫療服務對於工作流程是否有幫助?而您希望如何改進? 6. 目前的遠距醫療服務的報告(報表)或系統介面呈現方式是否容易瞭解和操 作?而您希望如何改進? 7. 在有限的人力之下進行遠距醫療服務是否會產生人力配置上的困難?要怎 麼去應付? 8. 在服務產品推廣上,面對顧客的推廣,要如何的說服病人及家屬相信及願意 購買這項服務?. Ch. engchi. 36. i n U. v.
數據
+7
相關文件
Thus, both of two-dimensional Kano model and IPGA mode are utilized to identify the service quality of auto repair and maintenance plants in this study, furthermore,
The prevalence of the In-service Education is making the study of In-service student satisfaction very important.. This study aims at developing a theoretical satisfaction
Through literatures relevant to service quality, service value, customer satisfaction and customer loyalty, this research conducts study on the five aspects of the theme
This paper presents a Knowledge Value-Adding Model (KVAM) for quantitative performance evaluation of the Community of Practice (CoP) in an A/E consulting firm.. The
This study aims to explore whether the service quality and customer satisfaction have a positive impact on the organizational performance of the services and whether the
Lee's (2007) "Study of Long Stay Destination Evaluation Indicators for Japanese Pensioner Tourists in Taiwan" as research dimension, to analyze the grading
Hoping that the results of this study can provide suggestions for educational authorities and supplement schools to elevate the quality of elementary supplement schools.. The
A model of service quality perceptions and health care consumer behavior. Measurement and evaluation of satisfaction processes in
