行政院國家科學委員會專題研究計畫 成果報告
EGFR tyrosine kinase 抑制劑單獨或合併抗癌化學藥物對人 體膀胱癌細胞之毒殺與生長抑制之研究
計畫類別: 個別型計畫
計畫編號: NSC91-2314-B-006-148-
執行期間: 91 年 08 月 01 日至 92 年 07 月 31 日 執行單位: 國立成功大學醫學系泌尿科
計畫主持人: 蔡宗欣
報告類型: 精簡報告
處理方式: 本計畫可公開查詢
中 華 民 國 92 年 10 月 27 日
NSC-91-2314-B-006-148 成果報告
多種膀胱癌細胞株對 Iressa, 一種表皮 生長因子接受體酪酸酶抑制劑的敏感性:
與 EGFR-HER2/neu 共同表現相關
Differential Sensitivity of Bladder Cancer Cell Lines to Epidermal Growth Receptor-Tyrosine Kinase Inhibitor (Iressa): Correlation with Co-expression of EGFR and HER-2/neu
研究主持人:蔡宗欣
國立成功大學醫學院泌尿學科
中文摘要
在膀胱移行上皮細胞癌中,約有七、八十%為容易復發的表淺型膀胱癌。臨床上,在 接受內視鏡膀胱癌切除手術後會輔以膀胱內灌注化學藥物或免疫促進劑。其一年內復發 的機率仍約有三、四十%之多。而效果較好的藥物像 BCG 或 mitomycin C 也易引起一些副 作用。在先前我們的研究指出膀胱移行上皮細胞癌的病人中約有七、八十%會有表皮生長 因子接受體(EGFR, HER2/neu or both)的表現。因此,我們嘗試來研究一種新的表皮生
長因子接受體酪酸酶抑制劑 (Iressa, ZD1839, AstraZenck)是否可用當作膀胱癌術後
膀胱灌注的藥劑。Iressa,是一種可口服,分子量約 446.9 (介於 doxorubicin (M.W.544) 與 mitomycin C (M.W. 334)之間),口服後大部分經由膽汁排出,尿液中僅發現約不到 0.5%.目前已被美國食品藥物管理局通過可用於非小細胞的肺癌的病人,副作用大部分輕
微,像紅疹,青春痘等,約有 0.5-2%會有致命的間質性肺炎產生。因此,使用 Iressa
來當作膀胱癌術後膀胱灌注的藥劑或許可減少其副作用的產生而且保持有其抑制癌細胞 生長的作用。
我們首先以北方墨點法(western blotting)來決定表皮生長因子接受體家族成員 (EGFR, HER2/neu, erbB3)在多種的膀胱癌細胞株(MBT2, RT4, TSGH8301, TCCSUP, J82,
T24 cells)的表現量,並且以β-actin 來當作內部控制,利用影像分析的方式(ImagePro
plus 4.0),分別算出各個細胞的表皮生長因子接受體家族成員對β-actin 表現量比率,
其中,EGFR 以 TCCSUP cells 表現最多,HER2/neu 以 MBT2cells 表現最多;ErbB3 也以 TCCSUP cells 表現最多,而老鼠的膀胱癌細胞株(MBT2 cells)則只有 HER2/neu 的表現。
在抑制細胞生長方面,分別以不同濃度及不同藥物培養時間來進行 MTT Assay,其結果 呈現與藥物濃度及作用時間成相關的生長抑制情行;像在 100µM 的濃度作用下,一、二 及二十四小時的作用時間分別可達 4-49%,13-54% 及 24-65%。有趣的是此一生長抑制的 情形與 EGFR-HER2/neu 共同表現有統計學上的相關 (p=0.007, r2=0.8697),而與
EGFR,HER2/neu,ErbB3 或其它組合無關 (p=0.340 or 0.967).
從我們的研究結果顯示出多種的膀胱癌細胞株對 Iressa的敏感性與藥物濃度和作
用時間有關。在某些細胞株在一小時的作用時間就呈現很好的生長抑制情形。此種生長 抑制情形與與 EGFR-HER2/neu 共同表現有關。未來,在體內原位膀胱癌動物模式下有關 膀胱灌注治療或預防的效用與毒性研究將是需要的。
Differential Sensitivity of Bladder Cancer Cell Lines to Epidermal Growth
Receptor-Tyrosine Kinase Inhibitor (Iressa): Correlation with Co-expression of EGFR and HER-2/neu
Tzong-Shin Tzaia, Yuh-Shyan Tsaief, Chao-Liang Wub, Ai-Li Shiauc, Nan-Hua Chowd, Shin- Tzu Tsaia
Department of Urologya, Biochemistryb, Microbiology & Immunologyc, and Pathologyd, National Cheng Kung University Medical College and Hospital, Tainan, Taiwan
Department of Urology e, Tainan General Hospital, Department of Health, Executive Yuan, Tainan, Taiwan
Institute of Clinical Medicinef, National Cheng Kung University Medical College, Tainan, Taiwan
Running title: Sensitivity of bladder cancer cell lines to Iressa
Correspondence: Professor Tzong-Shin Tzai
Chief, Department of Urology, National Cheng Kung University Medical College & Hospital
138, Sheng Li Road, Tainan, 70428, Taiwan Tel: 886-6-2353535 ext. 5251
Fax: 886-6-2383678
E-mail: [email protected]
ABSTRACT
Purpose: To explore whether Iressa(ZD1839), a tyrosine kinase inhibitor of epidermal growth receptor, is an efficient intravesical agent for bladder cancer, we determined the expression status of EGFR, HER2/neu and erbB3 in several bladder cancer cell lines, investigated the differential sensitivity of these cancer cell to Iressa, and then mesaured the relationship between expression status of EGFR family and response to Iressa.
Materials and Methods: Fiver human bladder cancer cell lines (RT4, TSGH8301, T24, J82 and TCCSUP) and one murine bladder cancer cell line (MBT2) were obtained or purchased.
Total 50 µg protein from each cell lysate was obtained for Western blotting. The expression ratio of individual EGFR family member (EGFR, HER2/neu, erbB3)-to-β-actin were also calculated with image analysis (Image-Pro Plus 4.0). The growth inhibitory effect of Iressa in all cells was determined by MTT assays with 1, 2 and 24 hours of incubation time. The correlation between expression ratio and drug sensitivity was analyzed using a linear regression.
Results: From western blotting, all five human bladder cancer cre positive for EGFR and HER2/neu. ErbB3 was only expressed in TCCSUP and TSGH8301. MBT2 is only positive for HER2/neu, but negative for EGFR and ErbB3. From MTT assay, a dose-dependent and
time-dependent growth inhibitory effect were found in all cancer cells. The growth inhibitory effect at a 100 µM of Iressa for 1 hour, 2 hours and 24 hours were 4-49 %, 13-54% and 24-65%, respectively. Co-expresssion of EGFR and HER2/neu is strongly correlated with drug sensitivity (p=0.007, r2=0.8697), but not EGFR or HER2/neu alone (p=0.340 or 0.967), or other combination.
Discussion: Although the growth inhibitory effect of Iressa on several bladder cancer cells is
dose-or time-dependent, the effect in certain cancer cells (such as T24 cell) may be almost 50% at 1 hour of incubation time, which is the potential for intravesical therapy. In addition, the drug sensitivity significantly correlated with the co-expression of EGFR and HER2/neu, but not with the individual EGFR member alone or other combinations. In future, studies about the efficacy and toxicity in vivo should be considered in the orthotopic bladder cancer model.
Key words: Bladder neoplasm, EGFR, tyrosine kinase inhibitor, Iressa
INTRODUCTION
From natural history of transitional cell carcinoma (TCC) of the urinary bladder, about 70-80% tumors are superficial at diagnosis and easy to recur within a few years [1]. Many therapeutical modalities have been utilized for the prevention of recurrence, such intravesical instillation of chemotherapeutical agents, such as thiotepa, epirubicin or mitomycin-c, agents for enhancing local immunity, such as BCG, or 5-aminolevulinic acid for photodynamic therapy [2,3,4]. Despite that intravesical instillation with BCG or mitomycin-C may decrease recurrence rate as high to 30-40 %, there were also some severe adverse events, such as cystitis-like symptoms and systemic disseminated tuberculosis, caused by BCG instillation, or pelvic pain related to mitomycin-C extravasation [3,5]. Although there were less side effects associated with epirubin, and the reduction rate for recurrence was also less satisfactory (about 10-20%). In addition, thiotepa was not an ideal agent for intravesical instillation because of lower moelecular weight, which cause bone marrow suppression because of the potential of absorption into the bloodstream [6]. Therefore, it is necessary to search new ideal agents for intravesical instillation.
Our previous study has shown the high frequency of EGFR family expression in bladder cancer [7,8]. Using immunohistochemical staining, individual expression of EGFR, erbB2 (HER-2/neu), erbB3 and erbB4 receptors was detected in 72.2, 44.5, 56.3, and 29.8 % of bladder cancer caases. Overall, about four fifth of bladder cancer has expression of EGFR, erbB2, or both receptors. Furthermore, co-expression of EGFR and ErbB2, or EGFR, erbB2 and ErbB3 correlated with disease recurrence. In addition, co-expression of HER2/neu and p53 also contributed to increased number of lumph node metastasis [9]. With these results, many strategies to target EGFR family expression for cancer therapy have developed and revealed some excellent results, such as humanized monoclonal antibody, DNA vaccine, single chain antibodies, tyrosine kinase inhibitors of EGFR [10,11].
Iressa (‘ZD1839’) is an orally active, selective epidermal growth factor receptor tyrosine kinase inhibitor (EGFR-TKI) that blocks signal transduction pathways implicated in the proliferation and survival of cancer cells and other host-dependent processes promoting cancer growth [12]. Not only for EGFR, Iressa has also inhibited the growth in
HER-2-overexpressing breast cancer cells mediated Akt signal transduction pathways [13-15].
‘Iressa’ is a trademark of the AstraZeneca group of companies. It exhibits a broad spectrum of antitumour activity against many human solid tumour xenografts of various origins including breast, pancreas, lung, colorectal and head and neck [16]. ZD1839 has shown promising clinical effectiveness against a range of solid tumours, most importantly in non-small-cell lung cancer [17]. On May 5, 2003, Iressa received accelerated approved by the U.S. Food and Drug Administration as monotherapy treatment for patients with locally advanced or metastatic non-small cell lung cancer after failure of platinum-based and Docetaxol
chemotherapies. There were some adverse effects reported, including diarrhea, rash, acne, dry skin, nausea and vomiting, or even fatal interstital lung disease (about 1%, 0.3%-2%),
associated with this oral agents [18]. In addition, pharmacokinetics study demonstrated that there was a low urinary recovery after oral intake of Iressa, indicating that this was not a major route of elimination [19].
Therefore, this study was conducted to investigate whether Iressa is an efficient intravesical agent for bladder cancer, we determined the expression status of EGFR,
HER2/neu and erbB3 in several bladder cancer cell lines, detected the differential sensitivity of these cancer cell to Iressa with various incubation time, and explored the correlation between expression status EGFR family and drug response.
MATERIALS AND METHODS Materials
Iressa (ZD1839) was kindly provided by AstraZenca (Macclesfield, UK). Stock
solutions were prepared in DMSO and stored at-20 °C. The drugs was dulted in freshed media before each experiment. In all experiments, the final DMSO concentration was less than 0.1%.
Cell lines and culture condition
MBT2 cells was a murine bladder cancer cell line. RT4 cells was derived from low grade human bladder cancer, perchased from Center of Food scientific research center, Taiwan.
TSGH-301 was derived from a grade I, superficial, transitional cell carcinoma (TCC) of the urinary bladder. T24 cells was derived from invasive bladder cancer. TCCSUP was derived from an undifferentiated, Grade IV, metastatic TCC of human bladder. J82 was derived from a poorly differentiated, invasive, transitional-cell carcinoma, Stage T3 of human bladder. MBT2, TSGH8301, T24, TCCSUP and J82 cells were obtained from Professor Wu CL and Shiau AL, Department of Bochemostry and Microbiology and Immunology, National Cheng Kung University Medical Collwege (Tainan, Taiwan). All the cancer cell lines were maintained in Dulbecco's modified Eagle's medium (DMEM) containing 10% fetal bovine serum, 2 mM glutamine and 50µg ml-1 gentamicin in a 5 % CO2 humidified atmosphere at 37 °C, and harvested for analysis at 80-90 % confluency. Subconfluent cultures were expandedby treatment with 0.25% trypsin/0.1% EDTA.
Western Blotting
Western blots were performed by harvesting total cellular lysates in lysis buffer [10 mM sodium phosphate (pH 7.2), 150 mM NaCl, 0.1% SDS, 1% NP-40, 1% sodium deoxycholate, and protease inhibitors], separating 50 µg of each lysate by SDS-PAGE, and transferring to membrane. Immunoblot analyses were performed using antibodies specific for EGFR (Santa cruz, 1005), erbB2 (Santa cruz, C18), erbB3 (Santa cruz, C17) and β-actin, and visualized by
enhanced chemiluminescence and autoradiography. Utilizing the of β-actin expression as an internal control, quantitative analysis of their expression was performed by imaging the
autoradiograms in white light and quantitating relative band densities using Image-Pro Plus 4.0 software. A complte digital image of each cell sample was captured and measured as
integrated optical density (IOD is equal to averge density × area). All IOD values of EGFR, erbB2, erbB3 and β-actin were measured for each cellline and expressed as ratios of individual EGFR family member to β-actin.
Growth Inhibition assay
For growth inhibtion assays, cells were seeded in 96-well clusters at 500–1500 cells/well.
Later (24 h), the cells were placed in fresh medium containing various concentrations of ZD1839 and allowed incubation of the drug for 1-24 hours. When control wells were near 80-90 % of the confluence, cells viabilty was assayed using MTT assay. Briefly, 100 µl of MTT (1 mg/ml) were added to each well for 4 hours at 37 °C to allow MTT to form formazan crystals by reacting with metabolically active cells. When the MTT incubation was completed, the supernatants were removed. 100 µl dimethyl sulfoxide (DMSO) was added to each well.
The A value of each well was measured with a microplate reader at 570 nm 10 min later. The percentage cell growth was calculated by comparison of the A570 reading from treated versus control cells. All experiments were performed in triplicate.
Statistical Analysis
The correlation between the effect of iressa on growth inhibition and ratios of EGFR family to β-actin was measured by using a linear regression analysis. The result was considered as significant while p value is less than 0.05.
RESULTS
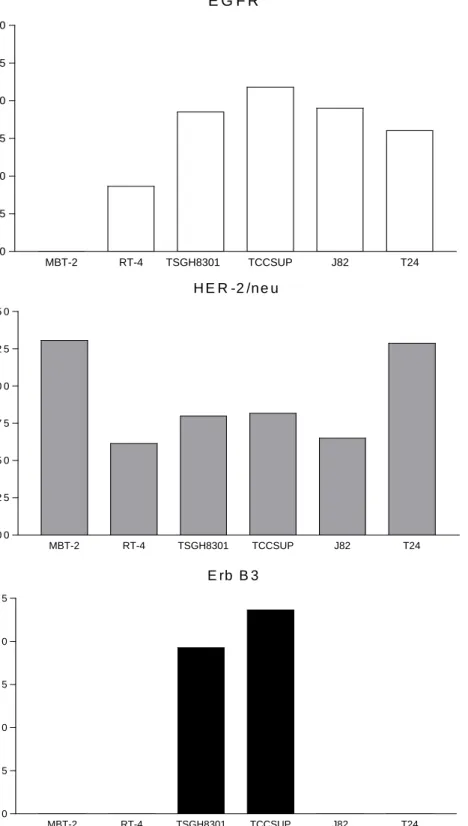
Expression status of EGFR, HER-2/neu and erbB3 in bladder cancer cell lines We first evaluate the expression of EGFR, HER-2/neu, and ErbB3 in a series of five human bladder cancer cell lines (RT4, TSGH8301, TCCSUP, J82 and T24) and one murine bladder cancer cell line (MBT2). Figure 1 showed the result of wesrtern blotting. With image analysis, the ratios of EGFR, HER-2/neu and erbB3 receptors to β-actin were determined. As for EGFR, the highest cell was TCCSUP, followed by J82, TSGH8301, T24 and RT4. There was no EGFR expression in MBT2 cells. As for HER-2/neu receptor, the highest cell was MBT2, followed by T24, TCCSUP, TSGH8301, J82 and RT4. As for erbB3, there were only two positive-expressing cells, including TCCSUP and TSGH8301.
Growth inhibition of bladder cancer cell lines to Iressa
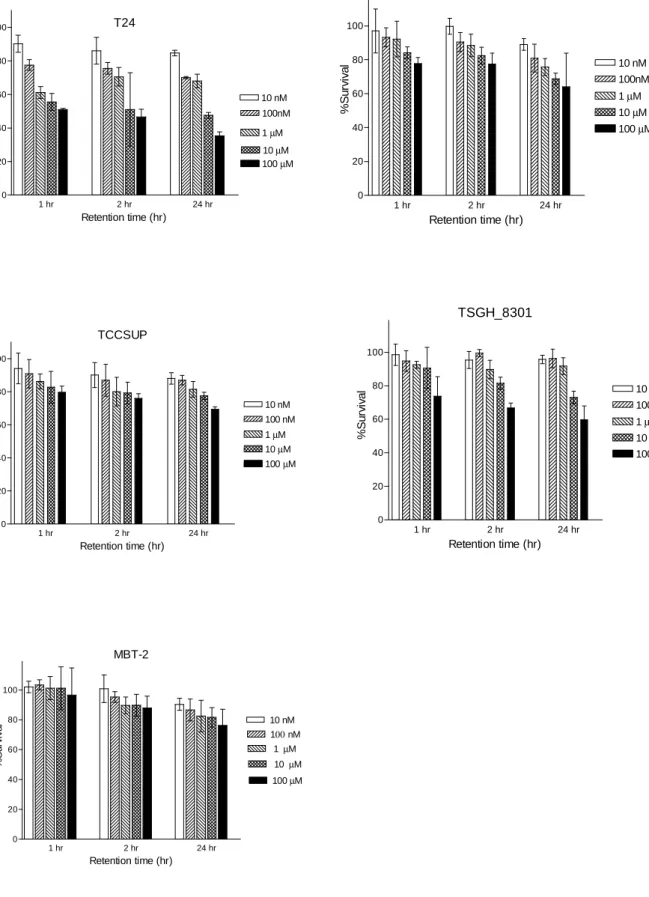
To determine whether Iressa is an efficient agent for bladder cancer via intravesical instillation, we evaluate the growth inhibition assay of these cancer cells with various incubation time (1, 2, and 24 hours) of this drug, mimicking with the retention time of chemotherapeutic agents for intraviscial instillation. Figure 2 and 3 showed the results of growth inhibition assay in T24, TSGH8301, TCCSUP, J82 and MBT2. Although a dose-dependent and time-dependent growth inhibitory effect were found in all cells; the growth inhibitory effect at a 100 µM of Iressa for 1 hour, 2 hours and 24 hours were 4-49 %, 13-54% and 24-65%, respectively. Among these bladder cancer cells, T24 cells has the best inhibitory growth effect and MBT2 cells has worst inhibitory effect.
The correlation between growth inhibition and EGFR family expression
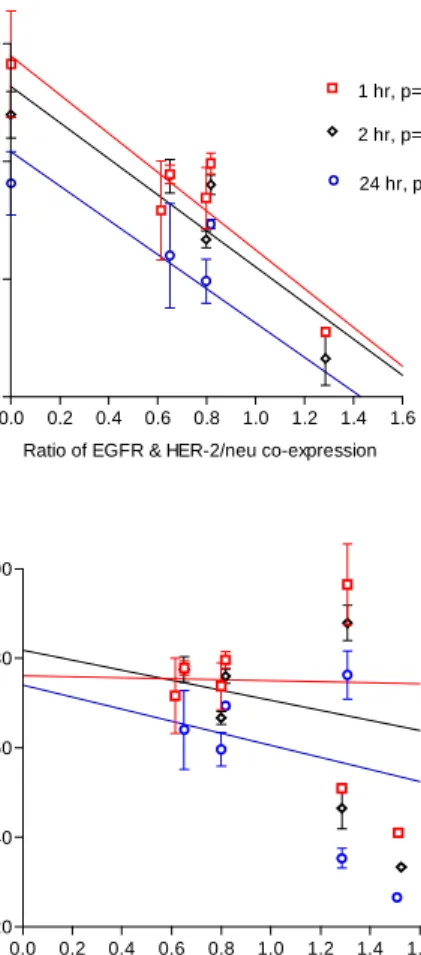
To determine whether sensitivity of bladder cancer cells to Iressa depends on the expression status of EGFR, HER-2/neu and erbB3, we measure the relationship between both by using a linear regression analysis. Figure 4 showed that the growth inbibtory effect of
Iressa is dependent on the coexpression status of EGFR and HER-2/neu co-expression, but not on EGFR, HER-2/neu or erbB3 expression. This correlation seem to be more significant at 1 hour of incubation time than at 2 hours or 24 hours of incubation time (pvalues, 0.007 versus 0.031 and 0.058, respectively; r2, 0.8697 versus 0.8320 and 0.7498).
DISCUSSION
Intravesical chemotherapy of superficial bladder cancer has been in routine use since the introduction of thiotepa in 1961 [20]. Since then, many chemotherapeutic or immnotherapeutic agents were utilized, such as thiopeta, epirubicin, doxorubincin, mitomycn-C, BCG,
interferon-alpha. For the prophylaxis of recurring disease, the recurrence rate eeither
chemptherapeutic agents or with immunotherapeutic agents is lower than with contros, but no effect on the risk of disease progression has been verified. Therefore, some trials with
combinations of both agents were also used [2].
The bladder lining is a poorly permeable membrane, but changes caused by tumours, inflammation and surgical scars can affect permeability profoundly. The diffusion of drugs across the bladder epithelium decreases in a linear fashion with increasing depth [21]. Ideally, low systemic absorption can avoid systemic toxicity; in contrast, deeper parts, such as deep growing tumor, are less exposed to drugs given by instillation, which easily casues the risk of disease progression. Factors within the bladder cavity also have a large impact on absorption.
These include the administered dose, volume of instillate, residual urine, urine production and the duration of the drug in the bladder. In addition, there are other variables of the drug
properties influencing absorption, such as molecular weight and lipid solubility [22]. Low molecular weight and high lipid solubility favour penetration of the bladder wall. For example, higher probability of bone marrow suppression occurred in patients receiving intravesical instillation of thiotepa than did other agents, because of lower molecular weight (M.W., 189.22).
Iressa is a orally active, low-molecular weight (M.W. 446.9), selective epidermal growth factor receptor-tyrosine kinase inhibitor that blocks signal transduction pathways implicated in proliferation and survival of cancer cells. On May 5, 2003, it was approved by F.D.A. in patients with non-small cell lung cancer after failure with docetaxol or cisplatin-based
chemotherapy. It inhibits the EGFR kinase in vitro with an inhibitory concentration 50% (IC50) of around 0.02 µM and requires a dose almost 200-fold higher to inhibit HER2/neu (3.7
µM).[23] Preclinical studies with Iressa have shown antitumor activity in a variety of cultured tumor cell lines and in human tumor xenografts, both as a single agent and in combination with chemotherapy and radiation therapy.[23-26] Interestingly, cultured breast cancer cells that express extremely high levels of HER2, even in the presence of a low number of EGFRs, are exquisitely sensitive to Iressa at concentrations that do not suppress HER2 tyrosine kinase activity[13-15]. Pharmocokinetically, the bioavailability of Iressa in human is approximately 60%, yet around 86% of orally administered Iressa is excreted in the faeces.
Biliary excretion is the major route by which absorbed drug leaves the human system. Urinary recovery of Iressa was less than 0.5%. A a pharmacokinetics study of Iressa in vitro, the data also showed that it is metabolised by the cytochrome P450 isoenzyme CYP3A4 and may inhibit activity of the related cytochrome P450 isoenzyme CYP2D6, indicating that some possible interactions between Iressa and other drugs, such as rifampicin (a CYP3A4 inducer);
itraconazole(a CYP3A4 inhibitor); and metoprolol (a CYP2D6 substrate) [19, 27-28]. Despite that no effects were judged likely to significantly alter the safety profile of the 250 mg daily dose, taken togethetr, it prompted us to investigate whether Iressa is an ideal agent of intravesical agent for superficial bladder cancer. Therefore, we first investigated the growth inhibitry effect in vitro in several bladder cancer cell lines with various expression profile of EGFR, HER-2/neu and erbB3 and mimicked with intravesical therapy by reducing incubation time short to 1 hour. In addition, we also seek the relationship between drug sensitivity and EGFR family expression.
100 µM ranged from 4% to 49 % at 1 hour of incubation time, from 13% to 54 % at 2 hours, and from 24% to 65 % at 24 hours. Our data is similar to previous ‘washout’ study in KB cells that sustained inihibition of autophosphorylation by Iressa can be persisted for 24 hours after exposure for 2 hours and replacement with culture medium without drug [12]. This
phenomenon implies that Iressa has the potential to be an efficient agent of intravesical instillation for bladder cancer in consideration with exposure time of the drug.
Although Iressa is a specific EGFR-tyrosinse kinase inhibitor, we found the growth inihibitory effect is dependent on the coexpression of EGFR and HER2/neu, but not on individual EGFR, HER2/neu, erbB3 alone or other combination. Ciardiello et al.has
demonstrated that tumor cell regression occurred in vitro, regardless of the degree of EGFR overexpression [16]. ZD1839 induce regression of tumors with either high or low EGFR expression in combination with other chemotherapeutical agents, such as taxane [24]. In addition, in some cultutred breast cancer cells that express extremely high levels of HER2, even in the presence of a low number of EGFRs, are exquisitely sensitive to Iressa [13-15].
Therefore, our data might indicate that Iressa inbihits the activity of tyrosine kinase on EGFR while heterodimerization with HER-2/neu, but less efficient while heterodimerization with other members or homodimerization of the indiviual receptor. However, it remained still about how the formation of homodimers or heterodimers occurs or about their underlying roles on the subsequent signal transduction [29].
In conclusion, our data demonstrated that the growth inhibitory effect in vitro occurred at a incubation time short to 1 or 2 hours, which is the potential for intravesical instillation for bladder cancer. The drug sensitivity is dependent on the co-expression of EGFR and
HER-2/neu, but not on EGFR, HER2/neu or erbB3 alone, or other combination. In future, the studies about the efficacy and toxicity in vivo orthotopic bladder cancer models are necessary.
ACKNOWLEDGEMENT
This study was supported by the National Science Council of Taiwan (grant NSC-91-2314-B-006-148).
REFERENCES
1. Messing EM, and Catalona W: Urothelial tumors of the urinary tract, in Walsh PC, Retik AB, Vaughan ED, and Wein AJ (Ed): Campbell's Urology, 7th ed., Philadelphia, W.B SAUNDERS Company, 1998, pp2348-2349.
2. Malmstrom PU. Improved Patient Outcomes with BCG Immunotherapy vs.
Chemotherapy –Swedish and Worldwide Experience. Eur Urol 2000; 37: 16–20
3. Alexandroff AB, Jackson AM, O’Donnell MA, James K. BCG immunotherapy of bladder cancer: 20 years on. Lancet 1999; 353: 1689–1694.
4. Berger AP, Steiner H, StenzlA, Akkad T, Bartsch G, Holtl L. Photodynamic therapy with intravesical instillation of 5-aminolevulinic acid for patients with recurrent superficial bladder cancer: A single-center study. Urology. 2003; 61: 338-341.
5. Nieuwenhuijzen JA, Bex A, Horenblas S. Unusual complication after immediate postoperative intravesical mitomycin C instillation. Euro Urol. 2003; 43: 711-712.
6. Badalament RA, Farah RN: Treatment of superficial bladder cancer with intravesical che-motherapy. Semin Surg Oncol 1997; 13: 335–341.
7. Lee SE. Chow NH. Chi YC. Tzai TS. Yang WH. Lin SN. Expression of c-erbB-2 protein in normal and neoplastic urothelium: lack of adverse prognostic effect in human urinary bladder cancer. Anticancer Research. 1994; 114: 1317-1324.
8. Chow NH, Chan SH, Tzai TS, Ho CL, Liu HS: Expression Profiles of ErbB Family Receptors and Prognosis in Primary Transitional Cell Carcinoma of the Urinary Bladder.
Clin Can Res 2001; 7: 1957-1962.
9. Tsai YS, Tzai TS, Chow NH, Yang WH, Tong YC, Lin JS, Chang CC, Cheng HL, Lin YM. Prognostic values of p53 and HER-2/neu co-expressions in invasive bladder cancer in Taiwan. Urol Int. 2003; 71:262-270.
10. Dancey JE, Freidlin B. Targeting epidermal growth factor receptor—are we missing the
mark? Lancet 2003; 362: 62–64.
11. Mendelsohn J, Baselga J. Status of Epidermal Growth Factor Receptor Antagonists in the Biology and Treatment of Cancer. J Clin Oncol. 2003; 21: 2787-2799.
12. Wakeling AE, Guy SP and Woodburn JR. ZD1839 (Iressa):An orally active inhibitor of epidermal growth factor signaling with potential for cancer therapy. Can Res. 2002; 62:
5749-5754.
13. Moulder SL, Yakes FM, Muthuswamy SK, Bianco R, Simpson JF, Arteaga CL.
Epidermal Growth Factor Receptor (HER1) Tyrosine Kinase Inhibitor ZD1839 (Iressa) Inhibits HER2/neu (erbB2)-overexpressing Breast Cancer Cells in Vitro and in Vivo. Can Res.2001; 61: 8887–8895
14. Moasser MM, Basso A, Averbuch SD, Rosen N. The Tyrosine Kinase Inhibitor ZD1839 (“Iressa”) Inhibits HER2-driven Signaling and Suppresses the Growth of
HER2-overexpressing Tumor Cells. Can Res. 2001; 61: 7184–7188.
15. Christensen JG, Schreck RE, Chan E, Wang X, Yang C, Liu L, Cui J, Sun L, Wei J, Cherrington JM, Mendel DB. High Levels of HER-2 Expression Alter the Ability of Epidermal Growth Factor Receptor (EGFR) Family Tyrosine Kinase Inhibitors to Inhibit EGFR Phosphorylation in Vivo.Clin Can Res. 2001; 7: 4230–4238.
16. Ciardiello F, Caputo R, Bianco R, et al: Antitumor effect and potentiation of cytotoxic drugs activity in human cancer cells by ZD-1839 (Iressa), an epidermal growth factor receptor-selective tyrosine kinase inhibitor. Clin Cancer Res 2000; 6: 2053-2063.
17. Fukuoka M, Yano S, Giaccone G, et al. Final results from a phase II trial of ZD1839 (Iressa) for patients with advanced non-small cell lung cancer (IDEAL 1) [abstract]. Proc
19. Swaisland H, Laight A, Stafford L, et al: Pharmacokinetics and tolerability of the orally active selective epidermal growth factor receptor tyrosine kinase inhibitor ZD1839 in healthy volunteers. Clin Pharmacokinet 2001; 40: 297-306.
20. Jones HC, Swinney J: Thiotepa in the treatment of tumours of the bladder. Lancet 1961; ii:
615–620.
21. Badalament RA, Farah RN: Treatment of superficial bladder cancer with intravesical chemotherapy. Semin Surg Oncol 1997; 13: 335–341.
22. Wientjes MG, Badalament RA, Au JL: Use of pharmacologic data and computer
simulations to design an efficacy trial of intravesical mitomycin C therapy for superficial bladder cancer. Cancer Chemother Pharmacol 1993; 32: 255–262.
23. Woodburn JR, Barker AJ, Gibson KH, et al: ZD1839, an epidermal growth factor tyrosine kinase inhibitor selected for clinical development. Proc Am Assoc Cancer Res.
1997; 38: 4521, 1997 (abstr).
24. Sirotnak FM, Zakowsky MF, Miller VA, et al: Efficacy of cytotoxic agents against
human tumor xenographs is markedly enhanced by co-administration of ZD1839 (‘Iressa’) an inhibitor of tyrosine kinase. Clin Cancer Res. 2000; 6: 4885-4892.
25. Woodburn J, Kendrew J, Fennell M, et al: ZD1839 (Iressa), a selective epidermal growth factor receptor tyrosine kinase inhibitor (EGFR-TKI): Inhibition of c-fos mRNA, an intermediate marker of EGFR activation, correlates with tumor growth inhibition. Proc Am Assoc Cancer Res 2000; 41: 2552. (abstr).
26. Ciardiello F, Caputo R, Bianco R, et al: Inhibition of growth factor production and angiogenesis in human cancer cells by ZD1839 (‘Iressa’), a selective epidermal growth factor receptor tyrosine kinase inhibitor. Clin Cancer Res 2001; 7: 1459-1465.
27. Swaisland HC, Ranson M, Smith R, et al. Ann Oncol 2002; 13 (Suppl. 5): Abs. 97.
28. Laight A, Swaisland HC, Partridge EA, et al. Ann Oncol 2002; 13 (Suppl. 5): Abs. 95.
29. Schlessinger J. Ligand-Induced, Receptor-Mediated Dimerization and Activation of EGF Receptor. Cell 2002; 110: 669-672.
FIGURE LEGENDS
Figure 1. A. Expression of EGFR, HER2/neu and erbB3 in several bladder cancer cell lines using western blotting. B. With the aid of image analysis, the ratio of individual EGFR member-to-β-actin were calculated. Among these cells, TCCSUP has the highest EGFR expression, followed by J82, TSGH8301, T24, and RT4. There was no detected EGFR expression in MBT2 cells. As for HER2/neu expression, MBT2 has the highest expression, followed by T24, TCCSUP, TSGH8301, J82 and RT4. There were only TCCSUP and TSGH8301 cells with erbB3 expression.
Figure 2. Differential sensitivity of bladder cancer cell lines to Iressa at various concentrations and incubation time. The growth inhibitory effect showed a dose- and time-dependent phenomenon.
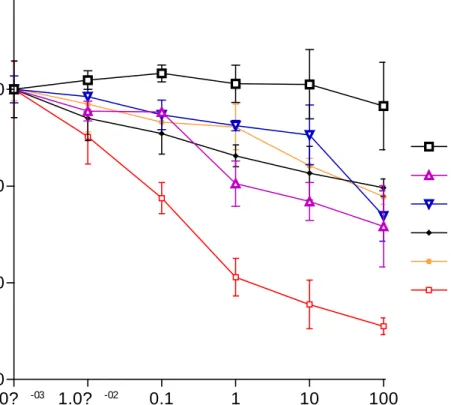
Figure 3. Growth inhibition curve of several bladder cancer cell lines at various concentration of Iressa with 1 hr-incubation time.
Figure 4. Correlation of drug sensitivity to the ratio of individual EGFR member- or EGFR-HER2/neu coexpression-to-β-actin in several bladder cancer cell lines. The result showed co-expresssion of EGFR and HER2/neu is strongly correlated with drug sensitivity (p=0.007, r2=0.8697), but not EGFR , HER2/neu, erbB3 alone (p=0.340 or 0.967), or other combinations (data not shown).
Figure
Figure 1A.
Figure 1B
E G F R
MBT-2 RT-4 TSGH8301 TCCSUP J82 T24
0 .0 0 .5 1 .0 1 .5 2 .0 2 .5 3 .0
EGFR/β-actin ratio
H E R -2 /n e u
MBT-2 RT-4 TSGH8301 TCCSUP J82 T24
0 .0 0 0 .2 5 0 .5 0 0 .7 5 1 .0 0 1 .2 5 1 .5 0
HER-2/neu /β-atin ratio
E rb B 3
MBT-2 RT-4 TSGH8301 TCCSUP J82 T24
0 .0 0 0 .2 5 0 .5 0 0 .7 5 1 .0 0 1 .2 5
ΗΕΡ−3/β-actin ratio
Figure 2.
MBT-2
1 hr 2 hr 24 hr
0 20 40 60 80 100
100 µM 10 µM 1µM
100nM 10 nM
%Survival
T24
1 hr 2 hr 24 hr
0 20 40 60 80 100
10 nM 100nM 1µM 10µM 100µM
Retention time (hr)
%Survival
J82
1 hr 2 hr 24 hr
0 20 40 60 80 100
10 nM 100nM 1µM 10µM 100µM
Retention time (hr)
%Survival
TCCSUP
1 hr 2 hr 24 hr
0 20 40 60 80 100
10 nM 100 nM 1µM 10µM 100µM
Retention time (hr)
%Survival
TSGH_8301
1 hr 2 hr 24 hr
0 20 40 60 80 100
10 nM 100 nM 1µM 10µM 100µM
Retention time (hr)
%Survival
Figure 3.
1.0? -03 1.0? -02 0.1 1 10 100 40
60 80 100
MBT-2 RT-4
TSGH8301 TCCSUP J82 T24
Iressa Conc. (µM)
%Survival
Figure 4.
0.0 0.2 0.4 0.6 0.8 1.0 1.2 1.4 1.6 40
60 80 100
2 hr, p=0.031, r2=0.8320
24 hr, p=0.058, r2=0.7498 1 hr, p=0.007, r2=0.8697
Ratio of EGFR & HER-2/neu co-expression
% Survival
0.0 0.5 1.0 1.5 2.0
25 50 75 100
1 hr, p=0.340, r2=0.2261 2 hr, p=0.470, r2=0.1853 24 hr, p=0.562, r2=0.1235
Ratio of EGFR expression
% Survival
0.0 0.2 0.4 0.6 0.8 1.0 1.2 1.4 1.6 20
40 60 80 100
2 hr, p=0.670, r2=0.0688 1 hr, p=0.967, r2=0.0005 2 hr, p=0.773, r2=0.0482
Ratio of HER-2/neu expression
% Survival
0.0 0.5 1.0 1.5 2.0
25 50 75 100
1 hr, p=0.845, r2=0.0104 2 hr, p=0.933, r2=0.0028 24 hr, p=0.702, r2=0.0559
Ratio of HER-3 expression
% Survival