An Experimental Study of Embedded Teaching Concerning Knowledge Sharing of
Health Technology and Learning Career for Students in Technological and Vocational
Colleges
Chin-Mou Cheng
College of Humanities and Management, Fooyin University, Kaohsiung, Taiwan
Abstract:
The purpose of this research was to carry on the experimental study of embedded teaching. The revised Solomon’s design of nonequivalent pretest-posttest control group consisted of two expe2imental groups (120 participants) and two control groups (125 participants). One of the experimental groups and control groups accepted respectively the pretest, and the experimental groups accepted the embedded teaching experiment of health technology and the control groups accepted non-experiment process. After 12 weeks, each group would accept the posttest to confirm the effectiveness of embedded teaching. The result discovered that the experimental groups and the control groups showed no significant difference in the pretest. The students who received the embedded knowledge sharing of health technology were superior to the students who did not receive the embedded knowledge sharing of health technology, regardless of behavioral norm, sharing attitude, sharing intention, sharing behavior and behavioral control. And there was no interactional effect between pretests and experimental treatment, and it was precisely proved through the experimental treatment and achieved an anticipatory effect. Finally, implication, conclusions and suggestions were advanced, such as taking more care for career types than learning styles, transactional platform of knowledge sharing in health technology, the health liberal teaching, enhancing the cooperation between industries and institutes, and helping the government draw up a technological policy.Key Words: professional and vocational colleges, health technology, knowledge sharing, learning styles, career types, embedded teaching
1 Introduction
Along with the approach in knowledge-based economy times and in facing the volatile and competitive environment, the knowledge sharing and learning type of health technology had become the sharp weapon with which we reached a target and created a competitive ability. Though knowledge sharing could be a principal axis of the knowledge-based economy, the decisive mission was learning before knowledge sharing. The knowledge had to come from learning and modified and renewed continuously. Through the learning, we could continuously promote the ability of the organization members, and in the meantime, make the organizational skill accelerate promptly, strengthen the organization operation day by day, and can also have more flexibility to respond to the fast changeable environment through the knowledge sharing. In order to respond to the "challenging Taiwanese digital modern eras planning in 2008", the learners had to hold a characteristic of large multidimensional learning. At present if college students had individually a learning style, for example they used the digital tool to obtain the digital teaching material through the wired or wireless network and carried out an activity of on-line or off-line digital learning or electronical learning, then they could easily obtain the knowledge needed. The learning which facilitated knowledge innovation could raise the industry value about fundamental scientific knowledge of colleges and reach the target of "national science technique development project"(2005-2008) to cultivate the talented persons of technology who emphasized learning curriculum and matched the industry needs and let them have the career vision. The educators established the fortress of happy learning, and let the learners leisurely visit the treasure house of information to share learning fun. The learners could appropriately control the approach of digital times, learning type of more multidimensional and getting away from the restriction of time and space. The digital technology
brings convenience for learning, then enhances the double effectiveness of knowledge created by sharing and embraces together each other a happy digital learning life. As the content of digital teaching material of "healthy medical learning net" let the people know Chinese herbal medicine, and convert theories of abstruse traditional medicine into reasonable and easy to get along with life experience and knowledge, including the understanding of physique, choosing food, especially healthy medicine food, and apply the healthy knowledge of the book to an actual life. All these knew clearly that the health technology knowledge came from learning, and learned happily the healthy knowledge related to personal learning style.
Learning styles or types meant the students were engaged in learning activities in the changeable environment of technology, and their apparent behaviors express the learning hobby with the individual difference through the mental process of their consciousness, remember, and thinking, etc. Learn styles, such as the factors of cognition, affection, society and physiology had the particularity, stability and consistency. By understanding the learning style, we could improve teaching and also help with the career development for students. The educational circles using classified theories of numerous learning styles most frequently was a Kolb learning type. The learning scale developed by Kolb combined the theoretical foundation of Jung, Levin, Dewey and Piaget, became a simple and strong model, and supported his theory with a complete statistical data. The students of learning styles could be divided into four groups: diverger, assimilator, converger, and accommodator. The students who must actually operate or experiment in the professional and vocational colleges could be contrasted with classified learning styles. Compared with the practice degree of lifelong learners, the different learning styles of learners could check the personal mastery, improving mental models, building shared vision, team learning, and systems
thinking (Senge, 1990). All the enterprise, administrative, educational and school organizations tried diligently inducing the related principles of the learning-based organization to apply widely (http://colkm.ccu.edu.tw/).The aim of this study was to solve the problems concerning the relationship between the students knowledge pursuing, management and sharing and their learning styles and practice degree, and whether they could learn from the multidimensional viewpoint to carry on knowledge sharing in professional and vocational colleges.
In the technological surroundings, college students of the present age should take into consideration how technology makes an impact on their health (Steinemann, 2000) and whether the knowledge sharing of health technology should have any kind of learning style and career type or not. Now there was not any kind of developed scale based on theories to measure the knowledge sharing of health technology and learning type for college students. This research searches first to inquire the related theories before developing a scale. In recent twenty years, bountiful are the academic papers on health technology interpreted by the behavior theories of social psychology and behavioral science, such as theory of planning behavior, social cognitive theory(Wigglers, 2005), innovative diffusion theory((Milner, Estabrooks, Humphrey, 2005), technology acceptance model(Kukafka, Johnson, Linfante, Allegrante, 2003), and health belief model to expect to build up a model of health technology knowledge and multidimensional learning.
In recent years, with a rapid increase of the number of technological and professional colleges, and in order to survive the inter-school competition, the colleges have made every effort to develop their own features to cultivate the students’ innovative capability to obtain competitive advantage. The White Paper about science and technology of my country- prospect and strategy of technological development (2003-2006) strove to head into a knowledge and creative technological development. Technological knowledge was the key factor of competitive ability. In the century of innovation and competitiveness, the prosperity of a nation comes from its competitiveness, that is, its innovative capability (Porter, 2001).
The enterprises thought widespreadly that for the current college students they lacked an innovation in working ability. The students were the important participants of technological innovation process, and they could bring the newness of their creativity into classroom, laboratory, factory, and enterprise of the new generation. The students were cultivated to develop their creative ability, could more availably display their creativity, and then created a new industry and work opportunity. Technology could be regarded as an innovative action adopted by people to solve a problem. Technology was the principal axis of social culture, and innovation was the engine that aroused the technological development. The invention steadily brought in more innovation, and innovation demanded the elemental technology ability. Through the good education of technology literacy, the college students were cultivated in proper order with fundamental technology literacy, and they had innovative ability in great quantities enough to expand. This research tried to make use of embedded teaching of health technology to inspire the potential of innovative learning and strengthen the competition ability for students.
The researcher taught the related subjects of technology literacy in professional and vocational colleges, and understood the
knowledge sharing and learning condition of students with the research interest in health technology, and then contributed with humble efforts to the general teaching. Owing to general subjects of liberal education, most of the traditional teaching methods could hardly arouse student's interest. The researcher developed a model about knowledge sharing and learning of health technology, which was an embedded teaching which could motivate students to learn health technology. Through the teaching process used by factors of interaction teaching, imagination, experience, scenario, attitude, curricular design, and pilot knowledge and what not, we let the students know how to handle well technology, cultivate the technology literacy, and promote a whole person's health. For challenging the job competition and taking preventive measures and forsaking a traditional burden, we displayed the effectiveness of powerful teaching to let the students be able to respond to future needs. Because this kind of research still belonged to an embryonic stage, and the researcher often paid more attention to healthy technology education in recent years and had a chance to participate in the teaching planning of liberal education curriculum, such as "medical caring", "health promotion", which took healthy concern as a focal subject of liberal education. Therefore the researcher kept often in mind a principle of health technology, and carried out the embedded teaching of health technology to identify the model about students' knowledge sharing and learning of health technology in professional and vocational colleges.
2 Research Objectives
In consideration of the fact that the students, despite being situated in the surroundings of technology, frequently ignore technological impact on their own health, this study focuses on the investigation about the condition of knowledge sharing and learning of health technology. Furthermore, the model of knowledge sharing and learning of health technology will be constructed, and the measuring scale of knowledge sharing and learning of health technology will be well developed and then carry out the embedded teaching of health technology. Accordingly, the objectives are stated as follow.
Carrying out the embedded teaching experiment of health technology to identify the result of model concerning the knowledge sharing and learning of health technology.
3 Literature Review
3.1 Reviewing the related theories
This research were mainly based up theoretical standpoints, such as Theory of Planned Behavior, Technology Acceptance Model, Innovates Diffusion Theory, Health Belief Model, and Social Cognitive Theory, to inquire into knowledge sharing and learning types of health technology for the students in professional and vocational colleges.
3.11 Theory of Planned Behavior
According to the theory of planned behavior( TPB), human action is guided by three kinds of considerations: beliefs about the likely outcomes of the behavior and the evaluations of these outcomes (behavioral beliefs), beliefs about the normative expectations of others and motivation to comply with these expectations (normative beliefs), and beliefs about the presence of factors that may facilitate or impede performance of the behavior and the perceived power of these factors (control beliefs). In their respective aggregates, behavioral beliefs produce a favorable or unfavorable attitude toward the behavior; normative beliefs result
in perceived social pressure or subjective norm; and control beliefs give rise to perceived behavioral control. In combination, attitudes toward the behavior, subjective norm, and perception of behavioral control lead to the formation of a behavioral intention. As a general rule, the more favorable the attitude and subjective norm, and the greater the perceived control, the stronger should be the person’s intention to perform the behavior in question. Finally, given a sufficient degree of actual control over the behavior, people are expected to realize their intentions when the opportunity arises. Intention is thus assumed to be the immediate antecedent of behavior. However, because many behaviors pose difficulties of execution that may limit volitional control, it is useful to consider perceived behavioral control in addition to intention. To the extent that perceived behavioral control is veridical, it can serve as a proxy for actual control and contribute to the prediction of the behavior in question.
Attitudes and subjective norms shape an individual’s intention and thus determine his behavior. Perceived behavioral control means how one perceives the difficulty of engaging in a beneficial behavior, that is, self –effectiveness. This will directly influence the intention of behavior. What directly or indirectly influences knowledge sharing is subjective norm, attitude intention, and perceived behavioral control (Ryu, Ho, Han, 2003). The more capability, skill, time, resources, or opportunities one has in engaging in some behavior, the more perceived knowledge he has. And thus his behavior intention will become stronger. (Ajzen, 1985) The relation between behavioral intention and actual act will become steadier.. In this study, the mutual relation among components of knowledge sharing of health technology literacy is based on the theory. Since 1975, the TPB theory (Fishbein & Ajzen, 1975) has made a study of relations among belief, attitude, intention, behavior, perceived behavior control, self-effectiveness, control propensity, and TPB (Ajzen, 2002). And it also explains how attitude influences behavior (Ajzen, & Fishbein, 2005). TPB has been widely applied to medical treatment behavior, environmental protection, life-long learning, reading literacy, sports health, tax reporting on the Internet, reasonable decision making, and information system, and this research will be applied to knowledge sharing and learning of health technology.
3.12 Innovative Technology Acceptance Model
Technology Acceptance Model (TAM) and Innovates Diffusion Theory (IDT) are combined to develop an Innovative Technology Acceptance Model. Technology acceptance model is designed to provide a basis used to research how outside factors influence users’ inner belief, attitude and intention, and how they influence the usage of the information system (Davis, 1989). According to this model, belief can influence attitude, which can influence behavioral intention, which in turn has a positive impact on practical usage. This model is widely used to explain or predict the influencing factors of information technology usage. When using technology, perception of the easiness of using new technology will influence its utility. In addition, both will influence the attitude of use; the perception of utility and the attitude toward use will further influence the behavior of use (Kukafka, Johnson, Linfante, Allegrante, 2003). In 1995, Everett Rogers formally presented the Innovation Diffusion theory. According to his theory, innovation diffusion in a social system depends on a condition that when users reach a certain rate of the total population, the diffusion process will sustain itself (Rogers, 1995). In a few studies, the diffusion process can be divided into
the stage of initial use, the stage of acceptance and adjustment, and the stage of continuous use. The related influencing factors include innovative features, organizational features, mission features, individuals’ features, and surrounding features. We attempt to understand how the stage of innovation diffusion of the knowledge management system is related to certain influencing factors. In addition, in terms of the innovation diffusion of national development, management and life cycle are stressed (Wonglimpiyaratat, Yuberk, 2005).
3.13 Health Belief Model
Health belief is mainly composed of perceived susceptibility, perceived severity, perceived benefits, and perceived barriers. Perceived susceptibility indicates an individual's assessment of their risk of getting the condition. Perceived severity indicates an individual's assessment of the seriousness of the condition, and its potential consequences. Perceived barriers indicate an individual's assessment of the influences that facilitate or discourage adoption of the promoted behavior. Perceived benefits indicate an individual's assessment of the positive consequences of adopting the behavior. HBM can revise the structure of teaching in order to improve health behaviors like giving up smoking (Kinzie, 2005). It can also be applied to the study of SARS (severe acute respiratory syndrome) (Wong, Tang, 2005). So, TAM, TPB, and IDT are combined to develop a more suitable model to examine the acceptability of health careers under the condition of PDA (Yi, et al.2006).
3.2 Embedded teaching
At present the universities and colleges compete keenly and must innovate teaching feature for the sustainable management. We could adopt a tangible teaching feature which is the new trend of learning and teaching and team teaching mingled with cooperative learning. The development of team teaching is influenced by cooperative learning and integrative curriculum from 1980s. However the team and cooperative teaching had the restriction, so the researcher picked the spirit of team cooperation and developed the teaching controlled by himself/herself of embedded teaching(Cheng, 2004). Then we try to construct a model of knowledge sharing and learning of health technology, and embedded it to a general education curriculum which healthily related as "healthy ability", "lifelong learning and knowledge management", and "sociology" teaching, and compared it with non- embedded teaching of knowledge sharing and learning of health technology to identify the effect of embedded teaching of health technology.
Embedding certain topics or subjects into main teaching units was more simple, and easer by making use of in the teaching situation at random, therefore the research chance which adopted infusing teaching as topics was abundant, such as the knowledge management integrated into the programming research of teaching organization, the planning study of combining knowledge management with teaching organization, the research of information seeding school pedagogy teams’ knowledge sharing, the effects of infusing history of physics into instruction on senior high school students' scientific epistemological views and learning approaches, the study of the information technology into Chinese instruction, the experimental study of integrating information technology on music instruction, a quasi-experimental study of infusing technological literacy into school curriculum, and infusing content of life education into science course and come up with an
integrated curriculum.
Integrating teaching which made the student participate properly in on-line learning through the curriculum is effective. The researcher once embedded the innovative humanities spirit of health technology into the general education teaching, usage teaching strategy, guided student's thinking, and made student's impression deep and lasting (Cheng, 2004, 2008). The health information could embed a clinical curriculum (Murphy, et. al, 2004). The related research of integrating teaching through searching Electronic Theses and Dissertations System in Taiwan discovered there were 564 articles up to April 3, 2009 and there was not an article on embedded teaching. When we searched the full text electronics periodical database of SDOS of Elsevier and there were 286 articles of integrated teaching, 99 articles of infusion teaching, and 65 articles of embedded teaching. Therefore we focus the research on developing embedded teaching model concerning knowledge sharing of health technology and learning career.
4 Research Methodology
4.1 Main Methods
4.11 .Documentary Review
We carried out documentary review to construct the basis of theories which knowledge sharing of health technology and learning of students in technological and vocational colleges, and the indicators and scale of measurement. When we reviewed the related documents, we searched the related articles from Electronic Theses and Dissertations System in Taiwan and electronics periodical of SDOS of Elsevier, including health technology, knowledge sharing, learning style, career type and health technology teaching, etc. Through the documentary analysis, we developed a questionnaire, acquired the quantitative data, and analyzed a statistical result. This research reviewed the related factor of health technology, and showed that the theories of basis, such as theory of planned behavior, social cognitive theory, innovative diffusion theory, technology acceptance model and health belief model. Then we drew up a scale with which the content was manufactured according to the related factor or indicators and appropriately described
4.12 Survey Research
In sampling investigation, cluster and stratified random sampling is adopted. Sampled 2-3 colleges students according to the each region in the north, central, south and east, each school sampled 60-150 people, and anticipated 1200-1500 people. The carried on a scale pretest. After testing, we built up the college student's norm concerning knowledge sharing of health technology and learning to explain the result.
4.13 Quasi-experimental Research
Experimental research method is a method which can really test the related hypothesis of cause and effect. In experimental research the independent variable was an experimental variable which was a reason or characteristic that was enough to cause difference as teaching method etc., and the dependent variable was a result of research. Because in actual teaching scenario, the real experimental research assigned randomly participants to the experimental group and the control group could not easily be implemented, we adopted a quasi-experimental design according to the way of purposive sampling and carried on Solomon's four groups of teaching experiment(Chang, 2003). So the revised Solomon’s design of the nonequivalent pretest-posttest control
group which consisted of two experimental groups and two control groups was extracted from the teaching classes of the researcher. This design of four groups which adopted non-random sampling and assigned participants to experimental treatment was combined pretest-posttest and only posttest control design, and was more rigorous than three groups for increasing one control group to become two experimental groups and two control groups.
Two experimental groups accept the same experimental treatment; and each of experimental groups and control groups accepts pretest. The groups accepted pretests are examined by a scale of knowledge sharing of health technology and learning. While experimental treatment will be over, four groups all accept posttest and carry out a scale test of knowledge sharing of health technology and learning. The researcher extracts four classes from the students whose optional subjects are concerning the related health teaching of general curriculum in professional and vocational colleges, such as” healthy ability" and "sociology". Then we select randomly a class as experimental group E1, another class as experimental group E2, and two experimental groups will accept an embedded teaching; and a class as control group C1, another class as control group C2, two control groups will accept a traditional teaching, and thus carry on a quasi-experimental research of nonequivalent pretest-posttest control group. The advantage of quasi- experimental research is a possible effect that can measure pretest, and its weakness isn't like a real experimental method assigned randomly.
The beginning of experimental treatment is at the 2nd semester of Taiwan Academic Year 96, within the limit of 12 weeks. The experimental treatment is over before the ending of this semester, carries on protest to test again a scale of college student's knowledge sharing of health technology and learning career, and compare the difference between experimental group and control group to identify the hypotheses. In order to make sure "experiment treatment", "pretest experience" and "the interaction of pretest and experimental treatment " these three kinds of effect, we adopt 2(pretest) × 2(experimental treatment) method concerning Analysis of Variance. The experimental period of embedded curriculum teaching of knowledge sharing of health technology and learning from 25 Feb 2008 to 24 May 2008. After 12 weeks, each group would accept the posttest to confirm the effectiveness of embedded teaching.
4.2 Research Participants
4.21 Quasi-experimental Subjects
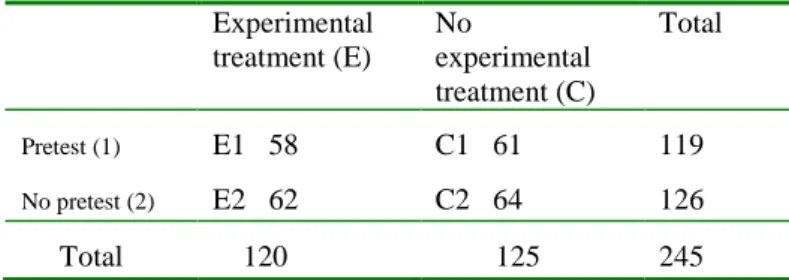
The numbers of subjects of quasi-experimental research are sampled as shown in Table 1, Table 2 and Table 3.
Table 1 Groups numbers of experimental treatment and pretest Experimental treatment (E) No experimental treatment (C) Total Pretest (1) E1 58 C1 61 119 No pretest (2) E2 62 C2 64 126 Total 120 125 245
Table 2 Numbers of learning styles in quasi-experimental research
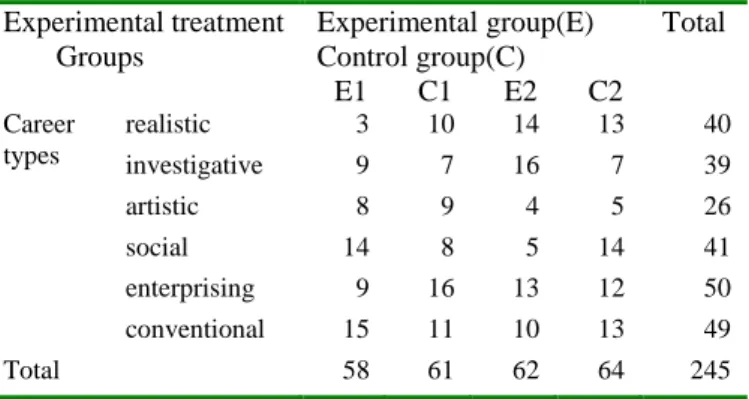
Table 3 Numbers of career types in quasi-experimental research
4.3 Research Measurement
The researcher constructed a scale concerning knowledge sharing of health technology and learning career which integrated 18 items of knowledge sharing of health technology literacy scale for students in professional colleges (Cheng, 2007,2008), 12 choice items about Kolb Learning Style Inventory, version 3 (http://www.learningfromexperience.com/images), and 60 items about career interest inventory (Test Publisher, 1994). This scale could test the degree of knowledge sharing of health technology and learning career for college students who placed themselves in technological environments, and understand what their learning styles and career types belonged to and the relationship with one another to promote the college students’ abilities of knowledge sharing of health technology and learning career and competitive ability.
4.4 Research Hypothesis
The research hypotheses are derived from above-mentioned theories and the related literature review mentioned above, and the hypothesis is listed as follow:
There is no significant difference between accepting embedded teaching of health technology and accepting not embedded teaching of health technology.
5 Result and Discussion
5.1 Quasi-experimental result analysis
The hypothesis mentioned above was identified by independent-sample t-test and two-way(pretest, embedded teaching) analysis of variance, and tested the difference of four
kinds of means as follows: (1) the means difference of pretest and posttest of E1(M3-M1), (2) the means difference of posttest of E1 and C1(M3-M4), (3) the means difference of posttest of E2 and C2 (M5-M6), and (4) the means difference of pretest of E1 or C1 and posttest of E2(M5-M1 or M5-M2).
5.11 The means difference of pretest and posttest of E1(M3-M1)
The result showed that there was no significant difference that was that the difference testing of pretest and posttest of experimental group reached not significant level and indicated that the pretest effect was very small.
5.12 The means difference of posttest of E1 and C1(M3-M4), as Table 6.
Table 6 the means, standard deviations and difference testing of posttest of E1(N=58) and C1(N=61)
** p <.01, * p<.05
From the table 6 showed that the means comparison of posttest of E1 and C1 all variables reached a significant level. That was that the students who received the embedded knowledge sharing of health technology were superior to the students who did not receive the embedded knowledge sharing of health technology, regardless of behavioral norm, sharing attitude, sharing intention, sharing behavior and behavioral control. Therefore the hypothesis was proven.
5.13 The means difference of posttest of E2 and C2 (M5-M6) as Table 7.
Table 7 the means, standard deviations and difference testing of posttest of E2(N=62) and C2(N=64)
** p <.01, * p<.05
From the table 7 it was shown that the means comparison of posttest of E2 and C2 all variables reached a significant level. That was that the students who received the embedded knowledge sharing of health technology were superior to the students who did not receive the embedded knowledge sharing of health technology, regardless of behavioral norm, sharing attitude, sharing intention, sharing behavior and behavioral control. Therefore the hypothesis was establishing. This matched the standpoint of the related research(Hinostroza & Mellar, 2001).
Experimental treatment Groups Experimental group(E) Control group(C) Total E1 C1 E2 C2 Learning styles diverging 11 17 15 17 60 assimilating 15 14 9 15 53 converging 9 12 23 22 66 accommodating 23 18 15 10 66 Total 58 61 62 64 245 Experimental treatment Groups Experimental group(E) Control group(C) Total E1 C1 E2 C2 Career types realistic 3 10 14 13 40 investigative 9 7 16 7 39 artistic 8 9 4 5 26 social 14 8 5 14 41 enterprising 9 16 13 12 50 conventional 15 11 10 13 49 Total 58 61 62 64 245 variable Mean posttest Std. Deviation posttest Std. Error Mean posttest t-test M5 M6 M5 M6 M5 M6 t Sig. norm 18.98 17.09 3.059 3.531 .389 .441 3.207 .002** attitude 14.94 13.41 2.126 2.980 .270 .372 3.307 .002** intention 18.56 17.33 2.838 3.546 .360 .443 2.157 .033* behavior 18.26 16.59 2.586 3.235 .328 .404 3.183 .002** control 13.03 11.94 2.283 2.678 .290 .335 2.466 .015* Total 83.77 76.36 11.135 14.14 1.41 1.77 3.263 .001** variable Mean posttest Std. Deviation posttest Std. Error Mean posttest t-test M3 M4 M3 M4 M3 M4 t Sig norm 18.81 17.30 2.825 2.716 .371 .348 2.983 .003** attitude 15.12 13.77 2.348 2.163 .308 .277 3.265 .001** intention 18.79 17.18 3.178 2.778 .417 .356 2.952 .004** behavior 17.97 16.51 3.184 2.675 .418 .342 2.708 .008** control 13.16 12.10 2.455 2.454 .322 .314 2.347 .021* Total 83.84 76.85 11.839 9.844 1.555 1.260 3.510 .001**
5.14 The means difference of pretest of E1 or C1 and posttest of E2(M5-M1 or M5-M2)
The result showed that there was no significant difference that was that the difference testing of E1 pretest and E2 posttest of experimental group reached not significant level and indicated that the pretest effect was no effect.
The means, standard deviations and difference testing of C1 pretest and E2 posttest was shown as in Table 8.
Table 8 Means, standard deviations and difference testing of C1(N=61) pretest and E2 (N=62) posttest
** p <.01,
From the table 8 showed that the means comparison of C1 pretests and E2 posttest all variables reached significant level.
The result showed that there was no significant difference that was that the difference testing of C1 pretest and C2 posttest of control group reached not significant level and indicated that the pretest effect was no effect.
By testing the difference of four kinds of means as above, we could find that the experimental result of two experimental groups in which one had pretest and the other one had no pretest was consistent, and it was precisely proved through the experimental treatment and achieved an anticipatory effect.
5.15 quasi-experimental teaching tested hypotheses by two-way analysis of variance
The result discovered that the experimental groups and the control groups showed no significant difference in the pretest, that is that the pretest reached not significant level on the variables of knowledge sharing of health technology and indicated that the pretest effect was no effect.
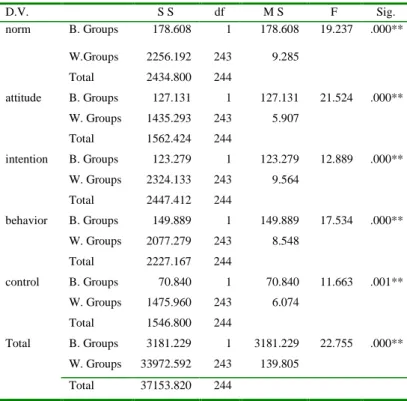
The result of experimental treatment was shown as in Table 9 and Table 10.
Table 9 Mean and standard deviation of experimental group and control group on knowledge sharing of health technology
From Table 9 and Table 10, we could discover that the students who received the embedded knowledge sharing of health technology were superior to the students who did not receive the
embedded knowledge sharing of health technology, regardless of behavioral norm, sharing attitude, sharing intention, sharing behavior and behavioral control. And it was precisely proved through the experimental treatment and achieved an anticipatory effect. Therefore, the hypothesis was establishing.
The result showed that there was no interactional effect between pretest and experimental treatment.
The statistical analysis discovered that for students belonging to any of the four learning styles, that is, diverging, accommodating, converging and assimilating, there was no significant difference in knowledge sharing of health technology.
The career types of students belonged to one of six types—the realistic type, the investigative type, the artistic type, the social type, the enterprising type, and the conventional type; and in addition to behavioral norm, behavioral control and knowledge sharing were significant differences, there was no significant difference in knowledge sharing of health technology, such as sharing attitude, sharing intention and sharing behavior. This could match the standpoints of the related researches(Cheng, 2005; Jang, 2008).
Table 10 Analysis of variance of experimental group and control group on knowledge sharing of health technology
** p <.01,
5.2 Discussion and Implication
In the experimental study of embedded teaching, the revised Solomon’s design of nonequivalent pretest-posttest control group which consisted of two experimental groups and two control groups was a suitable design. One of the two experimental groups and two control groups accepted respectively the pretest, and the experimental groups accepted the embedded teaching experiment of health technology and the control groups accepted non-experiment process. After 12 weeks, each group would accept the posttest to confirm the effectiveness of embedded teaching. The result discovered that the experimental groups and the control
treatment norm attitude intention behavior control Total E. group Mean 18.90 15.03 18.68 18.12 13.09 83.81 N 120 120 120 120 120 120 S D 2.937 2.228 2.996 2.882 2.359 11.432 C. group Mean 17.19 13.58 17.26 16.55 12.02 76.60 N 125 125 125 125 125 125 S D 3.149 2.609 3.182 2.963 2.562 12.188 Total Mean 18.03 14.29 17.95 17.32 12.54 80.13 N 245 245 245 245 245 245 SD 3.159 2.530 3.167 3.021 2.518 12.340 variable Mean posttest Std. Deviation posttest Std. Error Mean posttest t-test M5 M2 M5 M2 M5 M2 t Sig. norm 18.98 17.08 3.059 3.373 .389 .432 3.277 .001** attitude 14.94 13.43 2.126 2.572 .270 .329 3.549 .001** intention 18.56 16.80 2.838 2.682 .360 .343 3.536 .001** behavior 18.26 15.92 2.586 3.127 .328 .400 4.526 .000** control 13.03 11.41 2.283 2.479 .290 .317 3.776 .000** Total 83.77 74.59 11.135 11.88 1.41 1.52 4.424 .000** D.V. S S df M S F Sig. norm B. Groups 178.608 1 178.608 19.237 .000** W.Groups 2256.192 243 9.285 Total 2434.800 244 attitude B. Groups 127.131 1 127.131 21.524 .000** W. Groups 1435.293 243 5.907 Total 1562.424 244 intention B. Groups 123.279 1 123.279 12.889 .000** W. Groups 2324.133 243 9.564 Total 2447.412 244 behavior B. Groups 149.889 1 149.889 17.534 .000** W. Groups 2077.279 243 8.548 Total 2227.167 244 control B. Groups 70.840 1 70.840 11.663 .001** W. Groups 1475.960 243 6.074 Total 1546.800 244 Total B. Groups 3181.229 1 3181.229 22.755 .000** W. Groups 33972.592 243 139.805 Total 37153.820 244
groups showed no significant difference in the pretest. The students who received the embedded knowledge sharing of health technology were superior to the students who did not receive the embedded knowledge sharing of health technology, regardless of behavioral norm, sharing attitude, sharing intention, sharing behavior and behavioral control. There was no interactional effect between pretest and experimental treatment, and it was precisely proved that through the experimental treatment could achieve an anticipatory effect. In other words the hypothesis of embedded teaching was supportable. So we could apply this experimental design to the related researches.
Then there was no effect in knowledge sharing of health technology regardless of any of the four learning styles and there were some effects in six career types, so we should take more care for career types than learning styles in knowledge sharing of health technology.
6 Conclusion and Suggestions
6.1 Conclusion
The result showed that the pretest effect was no significant difference. We discovered that the experimental groups and the control groups showed no significant difference in the pretest, that is that the pretest reached not significant level on the variables of knowledge sharing of health technology and indicated that the pretest effect was no effect.
The result of quasi-experimental study of embedded teaching with the revised Solomon’s design of nonequivalent pretest- posttest control group consisted of two experimental groups (120 participants) and two control groups (125 participants) was that the experimental groups and the control groups showed no significant difference in the pretest. The students who received the embedded knowledge sharing of health technology were superior to the students who did not receive the embedded knowledge sharing of health technology, regardless of behavioral norm, sharing attitude, sharing intention, sharing behavior and sharing control. And there was no interactional effect between pretest and experimental treatment, and it was precisely proved through the experimental treatment could achieve an anticipatory effect and attain the research goal.
The statistical analysis discovered that for students belonging to any of the four learning styles, that is, diverging, accommodating, converging and assimilating, there was no significant difference in knowledge sharing of health technology. In other word there was no effect in knowledge sharing of health technology regardless of any of the four learning styles.
The career types of students belonged to one of six types—the realistic type, the investigative type, the artistic type, the social type, the enterprising type, and the conventional type; and in addition to behavioral norm, behavioral control and knowledge sharing were significant differences, there was no significant difference in knowledge sharing of health technology, such as sharing attitude, sharing intention and sharing behavior. In other word there was some effects in six career types.
6.2 Suggestions
1.In a rapid development of information technology, the college students’ health of body and mind were widespreadly subject to impact. Therefore, we will build up a knowledge sharing piping or platform of health technology to share their health belief
or exchange their opinion and experience, and it will be a necessity and adequacy.
2.The research discovered that the embedded teaching of knowledge sharing of health technology better than traditional teaching, therefore the related healthy subject of general teaching could be consulted and deliberate to embedded teaching method and strengthen the belief of health technology sharing to remind the students of paying attention to technological knowledge management.
3.The industry of health technology is doubtlessly one of new industries. The result of the related health technology research could provide the reference to develop a new product in industries. The related industry organization of government and citizen could provide a garden area of academic research, then could optimistically construct a cooperative bridge of industry and college.
4.The theories and scale of knowledge sharing of health technology and students learning career in professional and vocational colleges could provide a reference for teacher to research the related technology learning theories and establishment of scale.
5.The result of this research about college students’ knowledge sharing of health technology and learning career could provide a reference for the government to draw up a policy of health technology and bring benefit to the youthful mind and body.
Acknowledgements
This is part of a larger study on knowledge sharing of health technology and learning that has been financially supported by the National Science Council of Taiwan (NSC 96-2516-S-242-002).
References
Ajzen, I. (1991). The theory of planned behavior. Organizational Behavior and Human Decision Processes, 50, 179-211. Ajzen, I. (2002). Perceived behavioral control, self-efficacy, locus
of control, and the theory of planned behavior. Journal of Applied Social Psychology, 32, 665-683.
Ajzen, I., & Fishbein, M. (1980). Understanding attitudes and predicting social behavior. Englewood Cliffs, NJ: Prentice-Hall.
Ajzen, I. (2005). Attitudes, personality, and behavior (2nd. Edition). Milton-Keynes, England: Open University Press / McGraw-Hill.
Ajzen, I., & Fishbein, M. (2005). The influence of attitudes on behavior. In D. Albarracín, B. T. Johnson, & M. P. Zanna (Eds.), The handbook of attitudes (pp.173-221). Mahwah, NJ: Erlbaum.
Arthur, D., Pang, S., Wong, T.( 2001),the effect of technology on the caring attributes of an international sample of nurses, International Journal of Nursing Studies, 38, 37-43.
Barak, M.; Rafaeli, S. (2004). On-line question-posing and peer-assessment as means for web-based knowledge sharing in learning. Int. J. Human-Computer Studies. 61, 84–103. Broberg, O., Hermund, I. (2004), The OHS consultant as a
‘political reflective navigator’ in technological change processes, International Journal of Industrial Ergonomics, 33, 315-326.
Chang Yu-Shan. (2003). A Study on Creativity of Virtual Teams. The Dissertation of Department of Industrial technology Education, National Taiwan Normal University.
Cheng, Chin-Mou. (2004). The Humanities Caring of Health Technological Innovation Embedded to Liberal Teaching. College of Humanisties and Society, Fooyin University. Cheng, Chin-Mou. (2007). A Content Construction of Health
Technology Literacy for Students of Technology Universities: An Empirical Study. The Dissertation of Department of Industrial technology Education, National Kaohsiung Normal University.
Cheng, Chin-Mou. (2008). An Empirical Study on Constructing the Innovation Model of Health Technology Literacy and Quasi-experiment Embedded Teaching: for Students of Technological and Professional Colleges. Taipei: New Wun Ching Developmental Publishing Co.
Cheng, Shein-Yung (2005). Learning and diagnosis of individual and class conceptual perspectives: an intelligent systems approach using clustering techniques. Computers and Education, 44, 3, 257-283.
Chu, L. F. & Chan, B. K. (1998), Evolution of web site design: implications of medical education on the Internet, Computers in Biology and Medicine, 28, 459-472.
Colea, I. J., & Kelsey, A. (2004). Computer and information literacy in post-qualifying education, Nurse Education in Practice, 4, 190-199.
Cousineau, T. M., Franko, D. L., Ciccazzo, M., Goldstein, M., Rosenthal, E. (2006).Web-based nutrition education for college students: Is it feasible? Evaluation and Program Planning .29. 23–33.
Cutler, D. M. (2003), Technological development and medical productivity: the diffusion of angioplasty in New York state, Journal of Health Economics, 22, 187-217.
Farnaz, H. ; Galvin, K. (2003). Action learning groups: can they help students develop their knowledge and skills? Nurse Education in Practice. 3, 49–55.
Fishbein, M., & Ajzen, I. (1975). Belief, attitude, intention, and behavior: An introduction to theory and research. Reading, MA: Addison-Wesley
Hinostroza, J. E. & Mellar, H. (2001), Pedagogy embedded in educational software design: report of a case study, Computer & Education, 37, 27-40.
Holland , J. L. (1973). Making Vocational Choice:A Theory of careers. Englewood Cliffs , NJ:Prentice-Hall.
Holland, J. L. (1985). Making vocational choices (2nd ed.). Englewood Cliffs, NJ: Prentice-Hall.
Holland, J.L.(1997). Making Vocational Choices: A Theory of Vocational Personalities and work environments. Psychological Assessment Resources, Inc.
Jang, Syh-Jong(2008)
.
The effects of integrating technology, observation and writing into a teacher education method course. Computers & Education, 50, 3, 853-865.Johnson, B. C., Ersland, J. J. (1999), Development of a Strategic Planning for ulti-Department Management in a Medical Center, Journal of the American Dietetic Association, 99, pp.A31
Kolb, D.(1985). Learning style inventory: Self-scoring inventory and interpretation booklet. Boston: Mcber and Company. Kuhn, G. & Krome, R. L. (1997), Career planning and
development for emergency medicine faculty, Journal of Emergency Medicine, 15, 381-385.
Logan, J. R., & Price, S. L. (2004). Computer science education for medical informaticians, International Journal of Medical
Informatics, 73, 139-144.
Murphy, J.; Stramer, K.; Clamp, S.; Grubb, P.; Gosland, J.; Davis, S.(2004). Health informatics education for clinicians and managers—What’s holding up progress? International Journal of Medical Informatics. 73, 2, 205-213.
Nambisan, S. & Wilemon, D.( 2003), A global study of technology programs, Technovation, 23, 949-962.
Porter, M. E. 2001. Strategy and the internet. Harvard Business Review. (March): 63-78.
Ryu, S., Ho, S. H., Han, I. (2003). Knowledge sharing behavior of physicians in hospitals, Expert Systems with Applications, 25, 113–122.
Senge, P. (1990) The Fifth Discipline: The Art and practice of Learning Organization. N.Y: Dubleday /Currency.
Test Publisher. (1994). Career Interest Inventory(College version). Taipei: Test Publishers.
Thomas, C. (1999), Health Status, Technological Innovation, and Health Care Expenditure, Brandeis University, Background Paper.
Tsai, Chin-Chung & Lin, Sunny (2001). Analysis of attitude toward computer networks and internet addiction of Taiwanese adolescents. Cyberpsychology & Behavior. 4(3). 373-376.
Yi, M.Y., Jackson, J. D., Park, J. S., Probst, J. C.(2006). Understanding information technology acceptance by individual professionals: Toward an integrative view. Information & Management. 43. 350–363.
Zhang, Li-fang (2004).Learning approaches and career personality types: Biggs and Holland United. Personality and Individual Differences. 37, 65–81.