行政院國家科學委員會專題研究計畫 期中進度報告
兒童慢性 B 型肝炎病毒感染自然病程影響因子之長程研究:
病毒量及病毒全長基因變化之探討(1/3)
計畫類別: 個別型計畫 計畫編號: NSC93-2314-B-002-101- 執行期間: 93 年 08 月 01 日至 94 年 07 月 31 日 執行單位: 國立臺灣大學醫學院小兒科 計畫主持人: 張美惠 報告類型: 精簡報告 報告附件: 出席國際會議研究心得報告及發表論文 處理方式: 本計畫可公開查詢中 華 民 國 94 年 6 月 3 日
行政院國家科學委員會補助專題研究計畫
☑ 成 果 報 告
□期中進度報告
(計畫名稱)
兒童慢性 B 型肝炎病毒感染自然病程影響因子之長程研究:
病毒量及病毒全長基因變化之探討(1/3)
計畫類別:
☑
個別型計畫 □
整合型計畫
計畫編號:NSC 93-2314-B-002-101 -
執行期間: 93 年 8 月 1 日至 94 年 7 月 31 日
計畫主持人:張美惠教授
共同主持人:
計畫參與人員:
成果報告類型(依經費核定清單規定繳交):
☑
精簡報告 □完整報告
本成果報告包括以下應繳交之附件:
☑
赴國外出差或研習心得報告一份
□赴大陸地區出差或研習心得報告一份
□出席國際學術會議心得報告及發表之論文各一份
□國際合作研究計畫國外研究報告書一份
處理方式:除產學合作研究計畫、提升產業技術及人才培育研究計畫、
列管計畫及下列情形者外,得立即公開查詢
□涉及專利或其他智慧財產權,□一年□二年後可公開查詢
執行單位:台大小兒科
中 華 民 國 94 年 5 月 31 日
中文摘要 目的/背景:在 B 型肝炎病毒慢性感染之自然史中,急性肝功能惡化可能造成進行性肝傷害, 甚至肝衰竭。長程前瞻性研究以探討 B 肝病毒量在急性肝功能惡化之及後,e 抗原抗體轉變 是否具帶動角色,是很重要的,可惜這方面的研究極欠缺,尤其在兒童及年輕成人方面。 對象及方法:我們長程追蹤了 460 名慢性 B 型肝炎病毒的兒童。每半年檢驗一次肝功能及血 B 肝標記。其中 72 名最初年齡小於 15 歲,追蹤期間大於 10 年,而且未曾接受過治療者進入 本研究。共有 59 人在追蹤過程中發生 e 抗原抗體轉變,另 13 人則一直保持 e 抗原陽性。在 病人肝功能變化前後我們測量其血清病毒濃度,然後並與其性別年齡,基因型等作相關分析。 結果:發現 B 型肝炎濃度變化主要有三種型式:(一)在肝功能上升前,病毒濃度保持高水平, 經過一到數次的肝功能變化之後,病毒濃度便急速下降(>102 copies/ml ) (n=62) (二)在肝功能 上揚之前,病毒濃度也上升(n=5)。(三)在肝功能上揚之前,病毒濃度先下降(n=4)。另外有一 人無法歸類。在 e 抗原陰轉之前的病毒濃度明顯高於陰轉之後。在陰轉之前,肝功能上升下 降起伏變化的次數明顯等於陰轉之後,但是 B 型肝炎病毒濃度的上下起伏次數在陰轉前後都 並無改變。 結論:大多數 B 型肝炎帶原的兒童及青少年,他們身上的病毒濃度在 e 抗原陰轉之後才會真 正下降。在陰轉之前,肝功能上下起伏是常見,但不見得伴有 B 型肝炎病毒濃度的上下起伏。 所以病毒濃度並非啟動 e 抗原陰轉的主因,應另外思考其他因素,例如宿主與病毒間的免疫 反應。 關鍵詞: B 型肝炎病毒,B 肝病毒 e 抗原,B 肝病毒 DNA,實時間聚合酶鏈反應
ABSTRACT
Aim/Background: In the natural history of chronic hepatitis B virus (HBV) infection, the acute
exacerbation or alanine aminotransferase (ALT) flare-up episodes can lead to progression of liver
damage, and even liver failure. Long term prospective study to explore the role of HBV viral load
in the exact mechanism of acute exacerbation and its subsequent hepatitis B e antigen (HBeAg)
seroconversion is very important but lacking particularly in children and young adults. Subjects
and Methods: Totally 460 children with chronic HBV infection were long-term followed up for
liver function profiles and HBV serum markers every 6 months. We recruited 72 children who
were enrolled at the age <15 years, followed-up for more than 10 years, and without treatment.
Fifty-nine of them were tepatitis B e antigen (HBeAg) seroconverted during follow-up, while 13
remained HBeAg sero-positive. We measured serum HBV DNA levels by real time PCR before,
at, and after ALT flare-up was detected. Then we correlated viral levels with subsequent HBeAg
seroconversion, gender, age, genotype, and histological findings. Results: The temporal profiles
of HBV DNA, ALT, and HBeAg seroconversion can be divided into three major patterns among
these 72 patients: (1) Plateau of HBV DNA before ALT flare-up (>2x UNL) and decreasing viral
load (>102 copies/ml) (n=62). After one or several episodes of ALT flare-up, the viral load started to
decrease sharply. (2) Increased viral load (>102 copies/ml) before ALT flare-up (n=5). (3)
Decreased viral load (>102 copies/ml) before ALT flare-up (n=4). One patient was unclassified.
post-HBeAg seroconversion phase. While those of ALT flare-up are higher in the pre- HBeAg
seroconversion phase, the frequencies of HBV DNA fluctuations are not different between those
two phases. Conclusion: HBV viral load would not decline until they finally underwent HBeAg
seroconversion in the majority of HBV carrier children and young adults. Several episodes of ALT
flare-up were common in the natural course, yet they were not commonly accompanied by a surge
of HBV DNA level. Most Factor(s) other than the surge of viral load may plays the key role in the
initiation process of HBeAg seroconversion.
INTRODUCTION
Chronic hepatitis B virus (HBV) infection is a world wide health problem (1). In hyperendemic
areas such as Taiwan, most chronic HBV infection begins in infancy and early childhood (2,3).
HBV infection in infancy or early childhood usually leads to a chronic infection (4), and
subsequently more serious complications than adult–acquired HBV infection (5, 6). Although
complications of chronic HBV infection manifest mostly in adulthood, liver histological changes
begin early since childhood (7). After HBV acquisition in infancy or childhood, the virus
replicates actively in the first several years, an immune tolerance stage to HBV with high HBV
DNA and normal ALT levels. They gradually lose their tolerance to HBV and going into an
immune clearance stage to HBV, marked by episode(s) of acute exacerbation with elevation of ALT
levels and inflammation and /or fibrosis of the liver in histology examination (8).
The exact mechanism leading to acute exacerbation and subsequent HBeAg seroconversion is
an outcome of host-virus interaction. We recently also found that host factors may affect the
clinical course: such as HLA DRB1*14 predicts earlier HBeAg seroconversion with higher
aminotransferase levels, while HLA DRB1*11 predicts later HBeAg seroconversion during HBeAg
seroconversion (unpublished data). We also had reported the mutations of the precore gene (9),
basal core promoter (10), and core gene deletion (11), are accompanied with HBeAg seroconversion,
some with a severe form of liver diseases.
exacerbation (12). Our previous study, using the less sensitive hybridization method, has shown a
high ALT level and a low HBV DNA level correlated with an imminent clearance of HBeAg (8).
However, there are several pitfalls in most of the previous studies: (i) the blood sampling were
mostly done at the time points of elevated ALT levels, which often reflect the results of the viral
host interaction. (ii) the study subjects are biased by the diseased population, not the community
based population. (iii) previous methods to measure viral load was relatively insensitive.
It will be more revealing if this is a prospective cohort study recruiting large community-based
population starting from early childhood, which is far before the acute exacerbation episodes, as in
this study. With the help of real time polymerase chain reaction (PCR), we are thus able to well
correlate the HBV DNA levels with the episodes of acute exacerbation in our long-term follow-up
(more than 15 years) children with chronic HBV infection. The related information in this age
group is mostly lacking in the world literature natural history of HBV infection.
SUBJECTS AND METHODS
Totally 460 HBsAg children with chronic HBV infection, under parental consents, were followed
longitudinally every 6 months. These carrier children were enrolled from (1) the outpatient clinic
of the National Taiwan University Hospital in a prospective study starting around 23 years ago, (2)
a prospective screening program for carrier children of HBsAg seropositive mothers, and (3) four
1999 (13). At each visit, physical examination, blood test for liver function profiles and HBV
markers were studied.
Among these children, 72 of them were enrolled into this study according to the following
criteriae. We recruited children who fulfilled the following three criteria: (i) HBeAg positive at
enrollment, (ii) an initial age <15 years old, (iii) follow-up duration >10 years, (iv) underwent
HBeAg seroconversion during follow-up, (v) no antiviral treatment was intervened. Fifty-nine
children fulfilled those criteria and had adeguate blood samples for analysis. Another 13 patients
were age-matched with the 59 children while they were persistently seropositive for HBeAg during
follow-up. Their HBV DNA quantification by real time PCR was done at least once every five
years if ALT levels were normal at the previous check every 6 months. In case of ALT elevation >
2x upper limit of normal (ULN), that is defined as acute exacerbation, we would do blood sampling
every one to two months till at least one more month after ALT returns to normal. If ALT
elevation was between normal and 2xULN, we would follow-up the child every 3 months till ALT
returns to normal. The subjects would be excluded from this study if they received any antiviral
therapy and if their blood samples were inadegnate for study.
Liver function profiles and Serology studies. Liver function profile were checked by an
autoanalyzer Hitachi 736 (Tokyo, Japan). A level of ALT greater than 80Iu/L was regarded as
having a surge. HBV Markers (including HBsAg, anti-HBs, anti-HBc, HBeAg, anti-HBe) were
done by an autoanalyzer (Hitachi 7450, Tokyo, Japan).
HBV DNA Quantification by real time PCR. HBV DNA was extracted from 50 µl serum and
the nucleic acid was re-dissolved in 50 µl of H2O. The PCR reaction was prepared in a total
volume of 10 µl containing 2 µl of DNA template, 1 µl of LightCycler FastStart DNA Master
Hybridization Mixture (Roche Diagnostics Applied Science, Mannheim Germany), 0.8 µl of 25 mM
MgCl2, 0.3 µM of anchor and sensor probes, and 5 µM primers. The primers covered HBV
nucleotide position 1261-1279 and 1600-1580, and the anchor probe is nucleotide position
1552-1576 and the sensor probe is from nucleotide position 1533-1550 of HBV DNA. The
detailed nucleotide sequences were described previously (14). The PCR reaction was performed
as follows: initial hot start denaturation at 95℃ for 10 minutes, followed by 45 cycles of
denaturation at 95℃ for 5 seconds, annealing at 53℃ for 10 seconds, and extension at 72℃ for 20
seconds. Real time PCR monitoring was achieved by measuring the fluorescence at the end of the
annealing phase for each cycle. The measurement was performed by using LightCycler analysis
software 3.5 (Roche Diagnostics Applied Science, Mannheim Germany). The sensitivity of this
method was 102 copies/ml of HBV in serum. A change of the levels of HBV DNA greater than 100
fold was regarded to have an increase or decrease of the levels.
Subjects. The demographic data of the 72 patients were described in Table 1. All these patients
are still under followed-up currently and none of them showed any signs of liver cirrhosis,
decompensated liver diseases, or hepatocellular carcinoma.
Temporal profile of HBV DNA, ALT, and HBeAg seroconversion. If we focus on the HBV
DNA and the ALT flare-ups, we may divide the temporal profiles into four patterns among these 72
patients.[Patlern 1: plateau of HBV DNA before ALT surge] (1a) Plateau of HBV DNA followed by
up surge of ALT (>2x UNL) and decreasing viral load (>102 copies/ml) (n=46): The subjects had a
persistently high titer of HBV DNA and no sign of decreased viral load before the first data of ALT
elevation. After ALT flare-up, the viral load started to decrease sharply (Fig. 1a). Among these
46 patients, 39 of them underwent HBeAg seroconversion while the other 7 did not up to date. (1b)
Plateau of HBV DNA followed by first ALT flare-up. However, the viral load kept about the same
level through the first ALT flare-up (n=16). Among these 16 patients, 10 of them finally
underwent HBeAg seroconversion while 6 did not. We also observed that the viral load did
decrease more than 100 folds in the second or third flare-up in five seroconverters and only one
non-seroconverters (Fig. 1b). All viral loads decreased to a low level after HBeAg seroconversion
if it occurred. [Pattern 2. Increased viral load (>102 copies/ml) before ALT flare-up] (n=5): four of
the five patients in this group were seroconverters while one of them did not undergo HBeAg
(n=4): All of them were seroconverters (Fig. 3). [Pattern 4. Unclassified] One patient had
fluctuation of viral loads after HBeAg seroconversion and unclassified to the above categories.
HBV DNA and ALT changes before and after HBeAg seroconversion. If we focus on the 59
patients who underwent HBeAg seroconversion and take the levels of HBV DNA and ALT into
consideration in the time sequence of these events, we may characterize their patterns before and
after HBeAg seroconversion in Table 2. The frequencies of the episodes of HBV DNA fluctuation
(>100 folds in copies/ml) before and after HBeAg seroconversion is not different, however, the
frequencies of ALT surges (>80 U/L) did differ between the pre- and post- HBeAg seroconversion
phases.
DISCUSSION
Our previous study, using the less sensitive hybridization method, has shown a high ALT level
and a low HBV DNA level preceded an imminent clearance of HBeAg (8). Also, the small-scale
adult study demonstrated a viral load peak preceded the ALT in acute exacerbation (15). In this
study, we described the viral load, ALT, and HBeAg seroconversion in more details. The
conclusion drawn from our previous study, which was published 14 years ago, may need some
modification after this study.
This prospective large-scale study should well illustrate the natural course of HBV DNA and
children,gotally 86% (pattern 1) do not demonstrate a viral load fluctuation before an acute
exacerbation or HBeAg seroconversion. This is because most HBeAg carrier children have a high
viral load, and a drastic viral load change is not a prerequisite to initiate an acute exacerbation
and/or HBeAg seroconversion. Only 12.5% of the carrier children, that is patterns 2 and 3, had a
>100 folds change of viral load before acute exacerbation. Once the ALT started to surge, we
checked the blood viral level every month. Certainly, the interval of viral load check has a huge
impact in interpretation of the results. However, we believed we did not miss the viral load
changes too much at a monthly interval (15).
The changes of the magnitude of HBV DNA levels amy not be a major event which directly
affect the acute exacerbation in children and young adults. The pathogenesis of HBV-related
hepatitis is immune-mediated (16), Which is not necessarily viral dose-dependent. The clinical
consequences of HBV infection mainly depend upon the provoked host immune response (17), not
the surge of the viral load. The data in Table 2 also circumstantially support this idea. The HBV
DNA fluctuation frequency was not different between the pre- and post-HBeAg seroconversion
phase while ALT fluctuation frequency was indeed more in the pre-HBeAg seroconversion phase.
This means in the same period, the severity of liver damage was not determined by the fluctuation
of viral load, something else, The host immune response is more likely the key factor to decide the
It is obvious that, HBV DNA levels declined after HBeAg seroconversion. This fact is
compatible with the concept that host immune response, mainly through the CD8+ cells (18),
sweeps away most of the HBeAg-expressed and HBV harbored hepatocytes, thus lowering down
the viral load. If the host immune response is provoked to a lesser extent, the HBV DNA levels
would not go down. While there still would be several ALT flare-ups, as they reflected some
activation of host immune response, but not enough to initiate HBeAg seroconversion. Once the
host immune response is competent enough to clear the virus, HBeAg seroconversion would ensue
and HBV DNA would decrease. Such course was commonly observed in the pre-HBeAg
seroconversion phase in this study (Fig. land 2).
In conclusion, surge of HBV DNA levels are not necessarily the critical factors as the
harbinger of HBeAg seroconversion through our long-term follow-up study. Over 80% of the
carrier children reached a plateau of viral load in the immune tolerance phase and the viral load
would not decline until they finally underwent HBeAg seroconversion, although several episodes of
ALT flare-up were possible during the course. A further exploration in integrating the time
sequences of the host immune reaction, viral load, serum biochemical profiles, liver histological
examination, and HBeAg seroconversion may help to understand which is (are) the key
determinant(s) in the natural history of chronic HBV infection.
ACKNOWLEDGEMENT:
REFERENCES
1.Beasley RP, Stevens CE. Epidemiology of hepatitis B virus infection in Taiwan. In Sung JL, Yu JY,
Wang TH, eds. “Proceedings of the International Symposium on Hepatitis in Taipei”. Taipei,
Gastroenterologic Society of the Republic of China, pp. 1-10.
2. Hsu HY, Chang MH, Chen DS, et al. Baseline seroepidemiology of hepatitis B virus in children
in Taipei, 1984 : A study just before mass hepatitis B vaccination program in Taiwan. J Med Virol
1986; 18: 301-7.
3. Sung JL, Chen DS, Lai MY, et al. Epidemiological study on hepatitis B virus infection in Taiwan.
Chin J Gastroenterol 1984; 1: 1-9.
4. Stevens CE, Beasley RP, Tsui J, et al. Vertical transmission of hepatitis B antigen in Taiwan. N
Engl J Med 1975; 292:771-4.
5. Chu CM. Toward control of hepatitis B in the Asia –Pacific Region- Natural history of chronic
hepatitis B virus infection adults wit emphasis on the occurrence of cirrhosis and hepatocellular
carcinoma. J Gastroenterol Hepatol 2000; 15: E25-30.
6. Yuen MF, Lai CL. Toward control of hepatitis B in the Asia –Pacific region- Natural history of
chronic hepatitis B virus infection. J Gastroenterol Hepatol 2000; 15: E20-4.
7. Chang MH, Hwang LY, Hsu HC, Lee CY, Beasley RP. Prospective study of asymptomatic
HBsAg carrier children infected in the perinatal period : clinical and liver histologic studies.
8. Lee PI, Chang MH, Lee CY, et al. Changes of serum hepatitis B virus DNA and
aminotransferase levels during the course of chronic hepatitis B virus infection in
children. Hepatology 1990; 12: 657-660.
9. Chang MH, Hsu HY, Ni YH, Tsai KS, Lee PI, Chen PJ, et al. Preocore stop codon mutant in
chronic hepatitis B virus infection in children : Its relation to hepatitis B seroconversion and
maternal hepatitis B surface antigen. J Hepatol 1998;28: 915-922.
10. Ni YH, Chang MH, Hsu HY, Tsuei DJ. Longitudinal study on mutation profiles of core
promoter and precore regions of hepatitis B virus genome in children. Pediatr Res 2004;56:396-399.
11. Ni YH, Chang MH, Hsu HY, Chen HL. Long-term follow-up study of core gene deletion
mutants in children with chronic hepatitis B virus infection. Hepatology 2000;32:124-128.
12. Liaw YF, Pao CC, Chu CM. Changes of serum HBV-DNA in relation to serum transaminase
level during acute exacerbation in patients with chronic type B hepatitis. Liver 1988;8:231-5.
13. Ni YH, Chang MH, Huang LM, Chen HL, Hsu HY, Chiu TY, Tsai KS, Chen DS. Hepatitis B
virus infection in children and adolescents in a hyperendemic area: 15 years after universal hepatitis
B vaccination. Ann Intern Med 2001; 135:796-800.
14. Ni YH, Huang FC, Wu TC, Kong MS, Jeng YM, Chen PJ, Tsuei DJ, Chen HL, Hsu HY, Chang
MH. Lamivudine treatment in maternally transmitted chronic hepatitis B virus infection patients.
Pediatr Int 2005; 47: (in press).
characterizing full-length hepatitis B virus genomes during acute exacerbation. Gastroenterology
2003; 124:80-90.
16. Ganem D, Prince AM. Hepatitis B infection-Natural history and clinical consequences. N Engl J
Med 2004; 350:1118-29.
17. Rehermann B. Immune responsed in hepatitis B virus infection. Semin Liv Dis 2003;23:21-34.
18. Guidotti LG, Ishikawa T, Hobbs MV, et al. Intracellular inactivation of the hepatitis B virus by
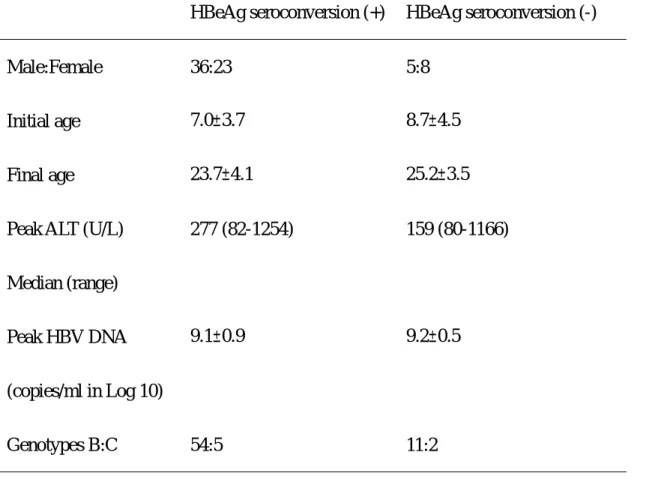
Table 1. The basic demographic data of the 59 children who underwent HBeAg seroconversion and 13 children who did not seroconverted during follow-up.
HBeAg seroconversion (+) HBeAg seroconversion (-)
Male:Female 36:23 5:8
Initial age 7.0±3.7 8.7±4.5
Final age 23.7±4.1 25.2±3.5
Peak ALT (U/L)
Median (range) 277 (82-1254) 159 (80-1166) Peak HBV DNA (copies/ml in Log 10) 9.1±0.9 9.2±0.5 Genotypes B:C 54:5 11:2
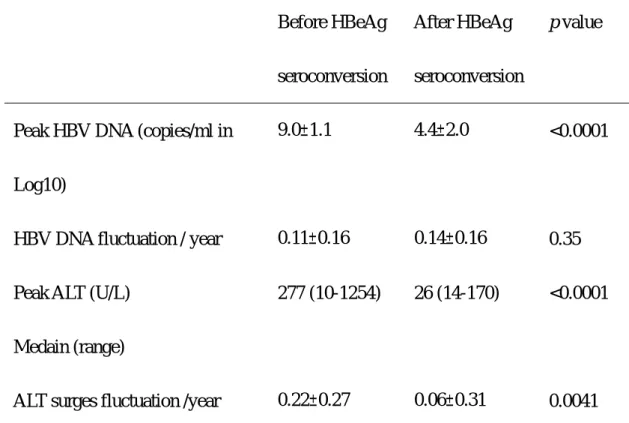
Table 2. The comparisons of before and after HBeAg seroconversion in 59 patients who underwent HBeAg seroconversion
Before HBeAg
seroconversion
After HBeAg
seroconversion
p value
Peak HBV DNA (copies/ml in
Log10)
9.0±1.1 4.4±2.0 <0.0001
HBV DNA fluctuation / year 0.11±0.16 0.14±0.16 0.35
Peak ALT (U/L)
Medain (range)
277 (10-1254) 26 (14-170) <0.0001
ALT surges fluctuation /year 0.22±0.27 0.06±0.31 0.0041
The age of HBeAg seroconversion: 17.2±5.8 years (mean ± standard deviation)
The definition of HBV DNA fluctuation is the episodes of the magnitude of HBV DNA levels
changes >102 copies/ml at two consecutive checks. In terms of its frequency before HBeAg
seroconversion, we divided such episodes by (the age of HBeAg seroconversion – the age at
enrollment). So is the calculation of its frequency after HBeAg seroconversion. The ALT surge
fluctuation is defined as the episodes of the magnitude of ALT levels changes >2XUNL, that is
usually 80 U/L at two consecutive blood samplings. The calculation of its frequency before and
after HBeAg seroconversion is the same as that of the HBV DNA.
Fig. 1a and 1b. (1a) Plateau of HBV DNA followed by up surge of ALT (>2X UNL) and
decreasing viral load (>102 copies/ml) (n=46): The subjects had a persistently high titer of HBV
DNA and no sign of decreased viral load before the first ALT increase. After ALT flare-up, the
viral load started to decrease sharply. The vertical line denotes the HBeAg seroconversion time.
(1b) Plateau of HBV DNA followed by first ALT flare-up. However, the viral load kept about the
same level through the first ALT flare-up (n=16). The viral load did decrease more than 100 folds
in the second or third flare-up in 5 of the 10 seroconverters while only one of the six
non-seroconverters. All viral loads decreased to a low level after HBeAg seroconversion if it
occurred. The vertical line denotes the HBeAg seroconversion time.
Fig. 2 Increased viral load (>102 copies/ml) followed by ALT flare-up (n=5): four of the five patients in this group were seroconverters while one of them did not undergo HBeAg
seroconversion. The vertical line denotes the HBeAg seroconversion time.
Fig. 3 Decreased viral load followed (>102 copies/ml) by ALT flare-up (n=4): All of them were seroconverters.
0 40 80 120 160 08/03 10/03 12/03 14/03 16/03 18/03 20/03 22/03 24/03 AGE (years) ALT (Iu/L) 0.00 1.00 2.00 3.00 4.00 5.00 6.00 7.00 8.00 9.00 10.00 HBV DNA Log1 0 0 10 20 30 40 50 60 02/02 04/02 06/02 08/02 10/02 12/02 14/02 16/02 18/02 AGE (years) ALT (Iu/L) 0.00 1.00 2.00 3.00 4.00 5.00 6.00 7.00 8.00 9.00 10.00 HBV DNA Log10 Fig 1 (a) Fig 1(b)
0 40 80 120 160 200 00/01 02/01 04/01 06/01 08/01 10/01 12/01 14/01 16/01 18/01 AGE (years) ALT (Iu/L) 0.00 2.00 4.00 6.00 8.00 10.00 12.00 HBV DNA Log10 Fig.2.
0 40 80 120 160 200 240 280 320 05 /0 4 06 /0 4 07 /0 4 08 /0 4 09 /0 4 10 /0 4 11 /0 4 12 /0 4 13 /0 4 14 /0 4 15 /0 4 16 /0 4 17 /0 4 AGE (years) A LT ( Iu/ L) 0.00 2.00 4.00 6.00 8.00 10.00 12.00 H B V DNA Lo g1 0 Fig.3.
行政院國家科學委員會補助國內專家學者出席國際學術會議報告
年 月 日 報告人姓名張美惠
服務機構 及職稱台大醫學院小兒科
時間 會議 地點 93 年 10 月 27 日至 11 月 4 日 美國波士頓 本會核定 補助文號 會議 名稱 (中文)美國肝臟醫學會(英文)American Association for the Study of Liver Diseases 發表
論文 題目
(中文)以大規模嬰兒大便卡篩檢膽道閉鎖之台灣經驗初報
(英文)A Mass Screening Program for Biliary Atresia By Stool Color Card in Taiwan-A Pilot Study
報告內容應包括下列各項:
一、 參加會議經過
(一)第一天(10 月 29 日): 本人先參加北美小兒肝臟學研討會,及大會之再教育課程 (共兩天之課程)。 北美小兒肝臟學研討會此次主題為 ”急性肝衰竭”.內容包含肝傷害及肝再生,美國 人急性肝衰竭之流行病學及預後, 肝腦病變之機轉及治療,胎兒及新生兒因鐵沉積症 引發之肝傷害, 藥物及毒物引發之肝傷害,兒童急性肝衰竭之藥物及過渡性治療等,接 著參加本日再教育課程內容涵括: (1) C 型肝炎之病毒生活史,宿主免疫反應,目前的治療,治療後以病毒動力學預測治療 之有效否及抗藥性,以及未來的新治療等。 (2) B 型肝炎的病毒學,宿主反應,及新藥發展, 病毒學檢驗法以偵測抗藥性,目前的治 療法,Pegylated interferon 治療,免疫調節劑,及其他新治療法。 另有很精采的 辯論有關是否免疫耐受期的 B 肝病人該被治療? 以目前的藥物治療看來,似乎因 效果不佳及抗藥性問題,應審慎選擇,儘量不治療此類病人。 (二)第二天(10 月 30 日):參加大會之再教育課程 本日內容涵括: (1)非酒精性脂肪肝病變(NASH)之診斷及臨床轉歸,其病理生理學,治療,及可能 以脂肪肝病變為表現之其他疾病(例如 C 型肝炎)。另有很有趣的辯論:酒精性脂 附 件 一肪肝病變(ASH)與非酒精性脂肪肝病變(NASH)是否是同一個病。 (2)肝纖維化及肝硬化之病理成因,抗纖維化治療之前景,肝內微循環及一氧化氮在門 脈高壓之角色,門脈高壓之新治療策略。 (3)肝細胞癌流行病學及自然史,致病機轉及治療新貌,並辯論是否肝癌應更積極的被 作肝移植。 (4)肝臟移植之病人選擇,受肝者對新肝之耐受性,Calcineurin 外之免疫抑制劑, HIV 感染及病毒性肝癌與肝移植,以及是否移植後之 C 型肝炎應被再移植之辯論等。 (三)第三天(10 月 31 日): 美國肝臟學會年會(1). 同一天有數個節目同時進行,本人參加:
(1)清晨研討會 ( 6:45AM-7:45 AM) : 主題為膽汁形成之分子機轉, 由 Richard M. Green 及 Michael Trauner 兩位教授主持此小型研討會, 主要討論膽汁之形成及 肝細胞內之膽汁運送系統,與其轉錄調控。
(2) 研究研討會( Research Workshop),主題為肝,脂肪,及脂肪毒性. 其內容涵括 a. 肝脂肪代謝之轉錄調控者之角色: 主要調控者 Sterol Response
Element-Binding Proteins(SREBP) , Carbohydrate-Response Element Binding Protein (ChREBP),及 Peroxisome Proliferator-Activated Receptors (PPARs) 之角色。
b. 肝脂肪內涵之調整 : 脂肪酸來源之調控影響肝脂肪化 ,Stearoyl-CoA Desaturase-1 (SCD-1) 在脂肪肝之調控角色。
c. 脂肪毒性 : 脂肪酸誘發細胞死亡通路,及 CYP2E1 經由不飽和脂肪酸及氧化與抗 氧化劑間之不平衡來導致細胞毒性。
(3) 發表我們的論文 : “ Screening for Biliary Atresia by Infant Stool Color Card in Taiwan”。 本文獲選為大會主席推薦之論文,本文報告我們在 2002 年三 月至 2003 年十二月,在台灣北中南東地區共 96 家醫療院所所執行之大規模嬰兒大 便卡計畫, 以推展膽道閉鎖之早期篩檢、診斷及手術,以提升手術成功率,增加存活 率。 在此期間合作醫院共生了 119,973 名嬰兒,我們共於此期間收集 78,183 張大 便卡(65.2%), 共通報 93 名嬰兒有異常大便顏色,共診斷了 27 名膽道閉鎖嬰兒, 其 中 25 名在出生後 60 天內被發現,2 名在 60 天以後才被發現 26 名嬰兒接受葛西手 術,其中 16 名(59.3%) 在生後 60 天以前接受手術, 另有一名嬰兒直接接受換肝手 術, 所以我們的嬰兒膽道閉鎖發生率為 2.33-3.45/10,000。 (4)小兒肝疾病論文發表會 : 內容涵括膽道閉鎖,膽汁滯留, 肝移植等 : 以膽道閉鎖之 Rhesus monkey 輪狀病毒 動物模式來評估免疫反應造成之膽道傷害; 肝臟 CD8 陽性淋巴球可調控實驗性膽道
閉鎖動物模式之膽道阻塞; 美國多中心 24 個月大膽道閉鎖兒之預後分析研究;全 靜脈營養所造成的膽汁滯留可能與黃豆脂肪溶液中之 stigmasterol 抑制膽酸活化 之 Bile Salt Export pump (BSEP) 有關;以選擇性 plasmapheresis 成功執行 ABO 血型不合兒童之肝移植 ; 以及用手術流通門脈血流可矯正原發性肝外門脈高壓, 引發無症狀之肝腦病變等。
(5) 參加 Liver International 之 主編會議. (四)第四天(11 月 1 日): 美國肝臟學會年會(2)
(1)清晨研討會 ( 6:45-7:45 AM) :
主題為肝臟疾病微陣列分析之缺點及好處.主持人為 Charles E.Rogler and Lislie Rogler 兩位教授。 討論其標本前處理與資料之分析方法。
(2) Presidential Plenary Session : (a) Session 1 : 內容函括 : 膽道上皮細胞產生的 endothelin -1 是造成肝肺徵候群之機轉 ; C 型肝炎病毒肝肺體外產出模式; C 型肝炎病毒複製體之動態展現; 骨髓細胞所形 成的肌纖維母細胞可產生膠原纖維(collagen), 但非經由細胞融合 ; IL6 引發之 RXRα 由核運出需 JNK 活化細胞訊息, 且與 serine 260 有關等. 於 HCV RNA 陽性之慢性 C 型肝炎病人 (b) Session 2: 內容函括 : 肝癌網路之初報 -美國肝細胞癌之流行病學與存活率; 西班牙多中 心隨機較長期用 Pegylated interferon alfa-2A (40 kd)( Pegasys) 及 Ribavirin 於 HCV RNA 陽性之慢性 C 型肝炎病人之最後報告; 調整體重與一般用法使用 Ribavirin 合併 Peginterferon alfa-2B 於非裔美人 C 肝病毒機銀型第一型病人 之比較; 體內過度表現 Peroxisome Proliferator-Activated Receptor
γ( PPARγ) 可抑制肝纖維化.
(3). Hyman Zimmermann State-of-Art Lecture :
主題為嚴重型藥物特異反應所造成的肝傷害,及其處置。其內容極具啟發性及實用 性。多中心之研究模式也很值得學習。
(4). 頒獎 :
a.傑出成就獎 : 頒給 Professor D. Montgomery Bissell b. 傑出服務獎 : 頒給 Professor R. Schiff.
內容函括 : 斑馬魚在胚胎發育時肝臟長出及肝腫大肝再生之基因機轉;
Plasminogen 缺乏造成成鼠肝修補時肝變胰臟細胞之轉變 ; 人類肝臟細胞植入 免疫不全鼠之型態學與生化學之辨識; CD39 與 RANBPM 作用後直接調控部分肝切 除後之 Ras 活化,肝細胞增生,及肝再生。
(6).參加參加美國肝臟學會年會節目評估委員會(Program Evaluation Committee, PEC)會議.
(五)第五天(11 月 2 日): 美國肝臟學會年會(3)
(1).清晨研討會 ( 6:45-7:45 AM) : 主題為 肝臟幹細胞, 由兩位大師級教授 Steward Sell 及 Neil D. Theise 主持.
(2).Presidential Plenary III :
內容涵括 : 懷孕末期使用 lamivudine 預防 B 型肝炎病毒母子傳染之多中心雙盲安 慰劑控制之研究; 隨機雙盲研究比較 adefovir dipivoxil (ADV) 加上
Emtricitabine (FTC) 與單用 ADV 於 e 抗原陽性慢性 B 型肝炎之效益及機轉 ; Adipokine 值可預測非酒精性脂肪肝病人之肝組織變化; Heteromeric Organic Solute Transporter ( OST) α 及 β 是迴腸表皮細胞基側膜膽酸運送者. (3).Leon-Schiff State-of-the Art Lecture :
主題為”受 HIV 感染的成人之肝病”, 由 professor David L. Thomas 演講. (4).病毒性肝癌之基礎科學研究 :
內容函括 : B 肝及 C 肝感染 UPA-免疫不權鼠之型態學及病毒學特質; B 肝病毒 ccc DNA 涉入在免疫不全鼠 hydrodynamic 注射裸露之 plasmid encoding B 肝病毒 DNA 後持續複製之機轉; B 肝病毒 lamivudine 抗藥性變種失去分泌 D 型肝炎病毒之能 力.
二、 與會心得
美國肝臟學會年會今年為第五十五屆, 歷史悠久, 是目前國際肝臟學術會議中學術 水準最高的會議. 每年年會均有大約五千人左右參加此會, 研討內容涵括與肝臟學 相關的基礎與臨床,內外兒科肝臟學之最新研究成果. 本人參加此會議有下列心得 : (一).了解國際肝臟學相關的基礎與臨床最新研究現況成果與趨勢,作為調整我們研究工作之重要參考,也啟發我們規劃新研究工作之動機。
(二)報告我们的研究成果,讓國際人士了解我們努力研究的水準,交換研究的心得。 (三)參加美國肝臟學會年會節目評估委員會(Program Evaluation Committee, PEC)會
議 : 本人任期 2004 至 2006 年。替此重要國際學會工作,促進國際交流。
(四)參加 SCI 期刊 Liver International 之編輯委員會:本人為此期刊之編輯(Editor)。 經由對此國際期列之工作貢獻,實際提昇我國的國際醫學之參與及影響力。