期末報告
接受生殖技術治療懷孕夫妻孕期性健康—性別差異與照護需求 (第二年)
計 畫 類 別 : 個別型計畫
計 畫 編 號 : MOST 106-2629-B-040-001- 執 行 期 間 : 106年08月01日至107年07月31日 執 行 單 位 : 中山醫學大學護理學系(所)
計 畫 主 持 人 : 李淑杏
共 同 主 持 人 : 黃正宜、應宗和
計畫參與人員: 碩士班研究生-兼任助理:李佳穎
報 告 附 件 : 出席國際學術會議心得報告
中 華 民 國 107 年 10 月 30 日
方法:研究設計為採縱貫式研究法(Longitudinal study
design),研究時間點為夫妻懷孕第一孕期(10-11週)、第二孕期
(20-21週)及第三孕期(30-31週)。研究組為接受人工生殖技術 治療懷孕夫與妻(study group)及自然受孕組自然受孕夫與妻
(control group)。結構式問卷,包括:夫妻的基本資料、女性性 功能量表(Female Sexual Function Index)、男性勃起功能品質 量表(International Index of Erectile Function; IIEF)等以 郵寄方式,請夫妻分別填答,再以回郵信封寄回。研究組及自然受 孕組各收案100對夫妻,最後研究組夫妻共72對(回收率72%),自 然受孕組共76對夫妻(回收率76%)納入研究。
結果:生殖技術懷孕組與自然懷孕組妻子之平均年齡為34.46歲 vs.31.35,生殖技術懷孕組與自然懷孕組先生之平均年齡為36.37歲 vs. 33.24歲。生殖技術懷孕組夫妻平均年齡顯著高於自然懷孕組夫 妻平均年齡。兩組個案其基本人口學資料在年齡、結婚年數、懷孕 胎數均有顯著差異(p<.05)。兩組婦女於孕期之性活動內容及頻率 依次為擁抱、接吻、愛撫、性交及自慰,且頻率隨孕期增加而減少
。生殖技術懷孕組婦女比自然受孕組於第一孕期性交次數顯著減少
(p<.05)。生殖技術懷孕組無論先生及妻子在三個孕期自行搜索性 健康資訊均顯著高於自然受孕組之先生及妻子(p<.05)。生殖技術 懷孕組先生在三個孕期有高於50%有問題,與自然懷孕組先生比並無 顯著差異(p>.05)。女性性功能指標量表中;生殖技術懷孕組在第 一孕期階段其「性興奮」、「陰道潤濕」、「高潮」、「滿意度」
、「疼痛」均顯著低於自然懷孕組(p<.05)。
結論與建議: 夫妻於孕期性健康資訊來源以自行搜尋居多、50%先生 於妻子懷孕階段可能有勃起功能問題、生殖技術懷孕婦女於孕期中 性功能滿意度普遍低,醫護人員應更積極提升自我在性健康照顧中 的角色與功能,於提供孕期健康照護時融入性健康照護內容,協助 夫妻瞭解懷孕階段彼此之需求,以健康態度共同面對。
中 文 關 鍵 詞 : 人工生殖技術、懷孕夫妻、性別、性健康、照護需求
英 文 摘 要 : Purposes: The purpose of this longitudinal study is to investigate the difference in sexual needs and responses during pregnancy between husbands and wives of couples with assisted reproductive technology (ART) and normal
conception.
Methods: This is a longitudinal study to investigate the sexual needs and responses at first trimester (10-11 gestational weeks), second trimester (20-21 weeks) and third trimester (30-31 weeks) during pregnancy. The
structured questionnaire for this study is designed by the research group based on the literature and experts'
opinions, comprising basic profiles of the couples, Female Sexual Function Index(FSFI), International Index of
Erectile Function (IIEF). The study group is composed of 100 previously infertile couples receiving ART, while 100
administered questionnaires.
Results: The response rate for study and control group was 72% (72 couples) and 76% (76 couples), respectively. The average age of ART and normal conception female was 34.46 and 31.35 years old, respectively, while that for their husbands was 36.37 and 33.24 years old, respectively. There were significant differences (p < .05) in age, years of marriage, and number of fetus. The leading sexual
activities during pregnancy for all pregnant women were holding, kiss, caring and masturbation in order, and the frequency of sexual activities was significant decreased with progress of the term of pregnancy (p < .05). Compared to couples of normal conception, both wives and husbands of ART group were more active in search of related sexual health information. More than 50% of husbands of ART group had sexual disturbance over three terms of wives’
pregnancy. On the other hand, wives of ART group
experienced a significantly lower satisfaction on orgasm, moisture, satisfaction and pain sensation than those of normal conception group.
Conclusion and Recommendation: The most common way to get sexual health information for previously infertile couples during all trimester is to search by themselves other than provided by doctors or nurses. Pregnant women with ART had a lower sexual satisfaction, especially during first
trimester, compare to pregnant women of normal conception which is one of tasks of health professionals to provide appropriate and timely health education on sexual health during pregnancy.
英 文 關 鍵 詞 : assisted reproductive technology, pregnancy, gender difference, sexuality, health needs
一、
前言
性是人類的基本需求之一(Maslow,1954),人類從出生開始即與性有關,性影響個 體生理、情緒、社會及認知表現,在人類整體經驗中佔有重要角色。夫妻於懷孕階段 其身體、心理、認知及社會等因素的改變都對夫妻間的性造成很大衝擊。多數的研究 顯示孕期及其健康狀態會改變夫妻的性慾與性反應週期,例如,懷孕時噁心、嘔吐、
乳房腫脹感及疲倦是最常影響婦女性趣的症狀,隨著胎兒逐漸長大孕婦體型改變,懷 孕婦女亦可能感受不適而造成性交的慾望降低(Bartellas, Grane, Daley, Bennett, &
Hutchens, 2000; Reamy, White, & Daniell, 1982; Elliott & Watson, 1985)。夫妻進行性行為 時可能有傷害胎兒的憂慮、擔心造成流產或早產,男性可能擔心性交時對胎兒造成傷 害(Bogren, 1991)。然而孕期也不完全對夫妻性健康造成負向影響;有些夫妻認為確 認懷孕後不必再刻意使用避孕措施,可以免除他們擔心懷孕的恐懼心理,夫妻會發現 懷孕時也能享受性的樂趣。
個人對於性的資訊與認知是影響性行為的重要因素,若懷孕夫妻瞭解有關性的生 理及情緒層面的正確資訊,則他們在享受性關係上就愈自在。然而加拿大 Bartellas 等 人(2000)的研究僅 29%婦女與醫師討論孕期性活動問題,49%由婦女提起,顯示孕 期婦女有性健康資訊的需求,而醫護人員在提供性健康資訊仍屬被動。西方社會如此,
而相形比較保守的華人社會更值得進一步探討。
許多研究顯示;不孕夫妻的性關係呈現壓力狀態(李淑杏、郭碧照、李孟智、李 茂盛,1995; Slade, Emery & Lieberman, 1997)。近年來有越來越多不孕夫妻尋求人工生 殖技術治療來達到懷孕的目的(國健署,2015;Gerris, 2002;Kremer, 2002;Olivius, Friden, Lundin, & Bergh, 2002)。然而昂貴醫療費用及一連串複雜且侵入的醫療措施亦使不孕夫 妻承受極大心理社會壓力,其中包括夫妻之性關係壓力(李淑杏、李孟智、郭碧照、
李茂盛,1991;李淑杏、郭碧照、李孟智、李茂盛,1995; Eugster &Vingerhoets, 1999; Greil, 1997; Slade, Emery & Lieberman, 1997)。夫妻一但成功懷孕,還需面對較高的孕期合併 症,以及因多胞胎而導致早產、低出生體重等較差嬰兒之出生結果(Poikkeus, Gissler, Unkila‐Kallio, Hyden‐Granskog, Tiitinen, 2007;Romoundstad, et al, 2006;Sunderam, et al, 2009)。
因懷孕的特殊性及較差的嬰兒出生結果,接受人工生殖技術治療夫妻其孕期性健 康與需求是否與自然受孕夫妻不同?且夫與妻孕期性健康反應及其需求是否不同,值 得進一步探討!因此本研究之目的即在針對接受生殖技術治療懷孕夫妻孕期性健康與 需求建立一個縱貫性的調查並瞭解夫妻之間的性別差異,期能提供未來醫護教育及臨 床照護之知識基礎與參考。
二、
研究目的
本研究計畫的目的如下:
1. 分析接受人工生殖技術治療懷孕夫妻第一孕期、第二孕期、及第三孕期夫與妻性健 康與照護需求之差異。
2. 比較接受人工生殖技術治療懷孕與自然受孕夫妻第一孕期、第二孕期、及第三孕期 夫與妻性健康與照護需求之差異。
三、研究方法
研究設計為採縱貫式研究法(Longitudinal study design)。研究時間點為夫妻懷 孕第一孕期(10‐11 週)、第二孕期(20‐21 週)及第三孕期(30‐31 週)。研究組為 接受人工生殖技術治療懷孕夫與妻(study group)及自然受孕組自然生懷孕夫與妻
(control group)。
1. 研究對象
研究對象選取條件為:(1)研究組:接受人工協助生殖技術治療初次懷孕之夫妻,
能閱讀中文並同意填寫問卷者,排除條件為已有生育小孩者。(2)自然受孕組:第 一胎自然受孕夫妻,能閱讀中文並同意填寫問卷者。
2. 研究場所
於中部某一生殖治療中心及中部某醫學中心婦產科門診為收案場所。研究組及 自然受孕組各收案 100 對夫妻,最後研究組夫妻共 72 對(回收率 72%),自然受孕 組共 76 對夫妻(回收率 76%)納入研究。
3. 研究步驟
通過 IRB 審查後(No.CS16047),符合研究對象之選取條件後進行如下:研究組:
於不孕症門診確認懷孕後,經由研究者說明研究目的,徵求夫妻之同意,並填寫知情 同意書後,於第一孕期(10‐11 週)、第二孕期(20‐21 週)及第三孕期(30‐31 週)時,
以郵寄問卷方式,請夫妻分別填答,完成後再以回郵信封寄回。自然受孕組:於一般 產科門診選取個案,經由研究者說明研究目的,徵求產後夫妻之同意,並填寫同意書 後,於第一孕期(10‐11 週)、第二孕期(20‐21 週)及第三孕期(30‐31 週)時,以郵 寄問卷方式,請夫妻分別填答,完成後再以回郵信封寄回。
4. 研究工具
本研究所採用之工具,為研究者參考國內外有關文獻、本團隊研究經驗、研究 領域專家建議及下列各標準量表加以編制成的結構式問卷,經測試信、效度後開始 施測,內容包括:
(1) 夫妻基本資料:
年齡、教育程度、經濟狀況、不孕原因、不孕時間及 ART 相關資料、懷孕週數、
懷孕合併症、懷孕前及各孕期性生活相關資料。
(2)女性性功能量表(Female Sexual Function Index ; FSFI):
本研究引用郭美璋等人(2004)翻譯 Female Sexual Function Index女性性功能指標量表 增訂項目之量表。量表共19題,分「性慾望」、「性興奮」、「陰道潤濕」、「高潮」、
「滿意度」、「疼痛」等六個次量表。採5 point likert scale,分數越高表示頻率越高、
滿意度越高、困難程度越低。
(3)男性勃起功能品質量表(International Index of Erectile Function; IIEF):
勃起功能量表,分成勃起時間、勃起持續時悶、射精、滿意度及整體品質等五項,採 5 point likert scale,分數越高表示滿意度越高。是國際標準化的分類方式及評估男性性功 能障礙的量表,目前亦作為臨床診斷與治療的重要依據,總分≧26分者為正常、18‐25 分者為輕度功能障礙、11‐17分為中度功能障礙、1‐10分為重度功能障礙,(郭美璋等 人,2004、2005)。
四、結果與討論
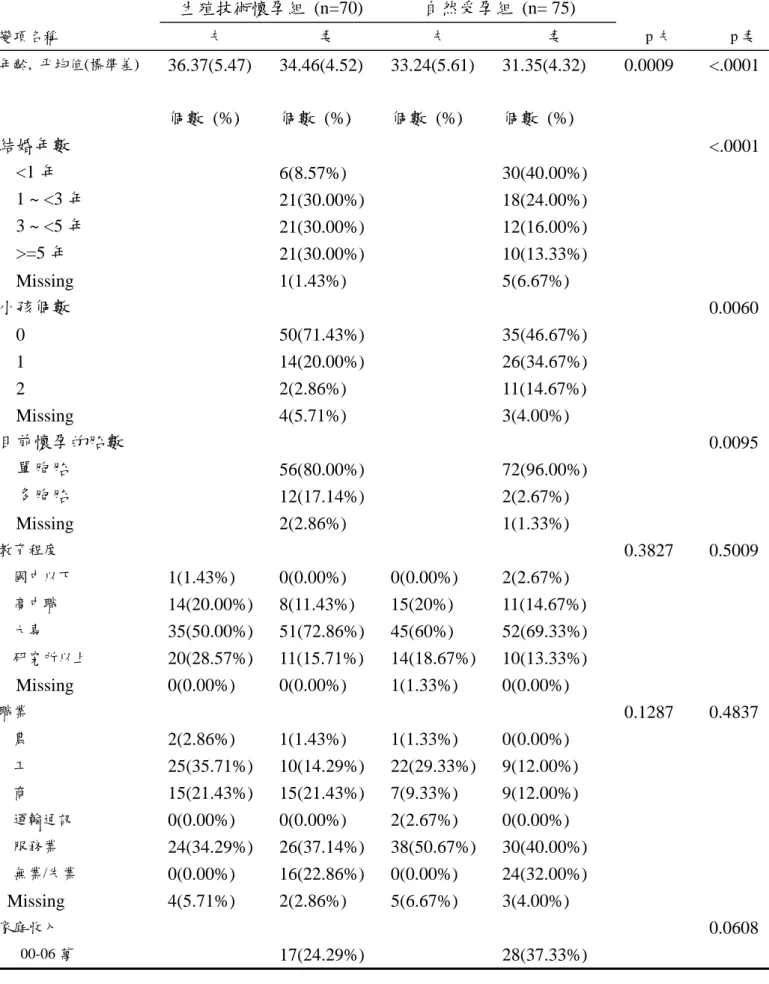
1.生殖技術懷孕組與自然懷孕組先生之平均年齡為 36.37 歲 vs. 33.24 歲,生殖技術懷孕組與 自然懷孕組妻子之平均年齡為 34.46 歲 vs.31.35。生殖技術懷孕組夫妻平均年齡顯著高於 自然懷孕組夫妻平均年齡。兩組個案其基本人口學資料在年齡、結婚年數、懷孕胎數均 有顯著差異(p<.05)(Table 1)。
2.生殖技術懷孕組在第一、二及三孕期之合併症(含腹痛、高血壓、陰道出血、羊水流出等) 分別為 29%、36% 及 31%。自然懷孕組在第一、二及三孕期之合併症(含腹痛、高血壓、
陰道出血、羊水流出等)分別為 35%、24%及 27%。二組未達顯著差異(p>.05)。
3.兩組婦女於孕期之性活動內容及頻率依次為擁抱、接吻、愛撫、性交及自慰,且頻率 隨孕期增加而減少。生殖技術懷孕組婦女比自然受孕組於第一孕期性交次數顯著減 少(p<.05)。
4.生殖技術懷孕組先生與妻子孕期性健康資訊來源其自行搜尋之比例均高於由醫師或護 理師提供。生殖技術懷孕組無論先生及妻子在三個孕期自行搜索性健康資訊均顯著高 於自然受孕組之先生及妻子(p<.05)。第一孕期由護理師提供生殖技術懷孕組妻子 之性健康資訊顯著高於自然受孕組妻子(p<.05);凸顯護理師於此部分所扮演之角色與 功能(Table2)。
5. 表三為男性勃起功能量表之嚴重度分布。生殖技術懷孕組先生在三個孕期有高於 50%
有問題,與自然懷孕組先生比並無顯著差異(p>.05)(Table3)。
6. 女性性功能指標量表中;生殖技術懷孕組在第一孕期階段其 「性興奮」、「陰道潤濕」、
「高潮」、「滿意度」、「疼痛」均顯著低於自然懷孕組(p<.05)(Table 4)。
結論與建議: 夫妻於孕期性健康資訊來源以自行搜尋居多、50%先生於妻子懷孕階段可 能有勃起功能問題、生殖技術懷孕婦女於孕期中性功能滿意度普遍低,醫護人員應更 積極提升自我在性健康照顧中的角色與功能,於提供孕期健康照護時融入性健康照護 內容,協助夫妻瞭解懷孕階段彼此之需求,以健康態度共同面對。
參考文獻
內政部統計處(2015)‧內政統計年報:育齡婦女生育率‧Retrieved January 17, 2015, from http://sowf.moi.gov.tw/stat/year/list.htm
李淑杏、李孟智、郭碧照、李茂盛(1991).接受人工生殖科技治療之不孕症婦女的 心理壓力及其相關因子.公共衛生,
18(2),148-163。
李淑杏、郭碧照、李孟智、李茂盛(1995).接受人工生殖科技治療的不孕症夫妻之 心理社會反應.台灣醫學會雜誌,
94(Suppl.1),S26-33。
郭美璋、許淳森、陳思銘、張景文、陳學修、張利中、江漢聲 (2004)•台灣婦產科門診 中婦女之性功能研究•臺灣性學學刊
, 10(1), 1‐12.
郭美璋、許淳森、陳思銘、張景文、陳學修、張利中、江漢聲 (2005)•台灣婦產科門診 婦女對性功能和性功能障礙認知之研究調查•臺灣泌尿科醫學會雜誌
, 16(2), 53‐59.
國健署(2015)‧民國
102
年台灣地區人工生殖施行結果分析報告‧台北:行政 院衛生署國民健康局。2016 年 1 月 17 日取自http://www.bhp.doh.gov.tw
Bartellas, E., Crane, J. M. G., Daley, M., Bennett, K. A., &Hutchens, D. (2000). Sexuality and sexual activity in pregnancy. British Journal of Obstetrics and Gynaecology, 107,964‐968.
Elliott, S. A. & Watson, J. P. (1985).Sex during pregnancy and the first postnatal year.
Journal of Psychosomatic Research, 29, 541‐548.
Eugster, A., &Vingerhoets, A. J. J. M. (1999).Psychological aspects of in vitro fertilization: a review. Social Science &Medicine, 48, 575‐589.
Gerris, J., DeNeubourg, D., Mangelschots, K., Van Royen, E., Vercruyssen, M., Barudy‐Vasquez, J., Valkenburg, M., & Ryckaert, G. (2002). Elective single day 3 embryo transfer halves the twinning rate without decrease in the ongoing pregnancy rate of an IVF/ICSI programme. Human Reproduction, 17, 2626–31.
Greil, A. L. (1997). Infertility and psychological distress: a critical review of the literature.
Social Science &Medicine,45, 1679‐1704.
Huang, C.Y., Tsai, L.Y., Liao, W.C.,& Lee, S. (2012). Nursing Interventions on Sexual Health:
Validation of the NISH Scale in Baccalaureate Nursing Students in Taiwan. International
Society for Sexual Medicine, 9, 2600‐2608.
Maslow, A. (1954). Motivation and personality. New York, NY: Harper.
Olivius, C., Friden, B., Lundin, K., & Bergh, C. (2002).Cumulative probability of live birth after three in vitro fertilization/ intracytoplasmic sperm injection cycles. Fertility& Sterility,
77, 505–510.
Poikkeus, Gissler, Unkila‐Kallio, Hyden‐Granskog, Tiitinen (2007). Obstetric and neonatal outcome after single embryo transfer. Human Reproduction, 22(4), 1073‐1079.
Reamy, k., White, S. E., Daniell, W. C, &, Le Vine, E. (1982).Sexuality and
pregnancy: a prospective study. Journal of Reproductive Medicine,27, 321‐327.
Romundstad, L.B., et al. (2006). Increased risk of placenta previa in pregnancies following IVF/ICSI; a comparison of ATR and non‐ART pregnancies in the same mother.Human
Reproduction, 21(9), 2353‐2358.
Slade, P., Emery, J., & Lieberman, B. A. (1997).A prospective, longitudinal study of emotions and relationships in‐vitro fertilization treatment. Human Reproduction, 12(1), 183‐190.
Sunderam, S., et al. (2009). Assisted reproductive technology surveillance: United States, 2006. MMWR Surveillance Summaries/CDC, 58(5), 1‐25.
Table 1 基本人口學變項
生殖技術懷孕組 (n=70) 自然受孕組 (n= 75)
變項名稱 夫 妻 夫 妻 p 夫 p 妻
年齡, 平均值(標準差) 36.37(5.47) 34.46(4.52) 33.24(5.61) 31.35(4.32) 0.0009 <.0001 個數 (%) 個數 (%) 個數 (%) 個數 (%)
結婚年數 <.0001
<1 年 6(8.57%) 30(40.00%)
1 ~ <3 年 21(30.00%) 18(24.00%) 3 ~ <5 年 21(30.00%) 12(16.00%)
>=5 年 21(30.00%) 10(13.33%)
Missing 1(1.43%) 5(6.67%)
小孩個數 0.0060
0 50(71.43%) 35(46.67%)
1 14(20.00%) 26(34.67%)
2 2(2.86%) 11(14.67%)
Missing 4(5.71%) 3(4.00%)
目前懷孕的胎數 0.0095
單胞胎 56(80.00%) 72(96.00%)
多胞胎 12(17.14%) 2(2.67%)
Missing 2(2.86%) 1(1.33%)
教育程度 0.3827 0.5009
國中以下 1(1.43%) 0(0.00%) 0(0.00%) 2(2.67%)
高中職 14(20.00%) 8(11.43%) 15(20%) 11(14.67%)
大專 35(50.00%) 51(72.86%) 45(60%) 52(69.33%)
研究所以上 20(28.57%) 11(15.71%) 14(18.67%) 10(13.33%) Missing 0(0.00%) 0(0.00%) 1(1.33%) 0(0.00%)
職業 0.1287 0.4837
農 2(2.86%) 1(1.43%) 1(1.33%) 0(0.00%)
工 25(35.71%) 10(14.29%) 22(29.33%) 9(12.00%)
商 15(21.43%) 15(21.43%) 7(9.33%) 9(12.00%)
運輸通訊 0(0.00%) 0(0.00%) 2(2.67%) 0(0.00%)
服務業 24(34.29%) 26(37.14%) 38(50.67%) 30(40.00%)
無業/失業 0(0.00%) 16(22.86%) 0(0.00%) 24(32.00%)
Missing 4(5.71%) 2(2.86%) 5(6.67%) 3(4.00%)
家庭收入 0.0608
00-06 萬 17(24.29%) 28(37.33%)
06-08 萬 29(41.43%) 19(25.33%)
08-10 萬 7(10.00%) 17(22.67%)
10-12 萬 8(11.43%) 5(6.67%)
12 萬以上 6(8.57%) 5(6.67%)
Missing 3(4.29%) 1(1.33%)
宗教信仰 0.1413 0.2451
佛教、道教 46(65.71%) 47(67.14%) 49(65.33%) 56(74.67%)
基督教 0(0.00%) 1(1.43%) 4(5.33%) 1(1.33%)
天主教 0(0.00%) 0(0.00%) 2(2.67%) 0(0.00%)
一貫道 2(2.86%) 3(4.29%) 1(1.33%) 0(0.00%)
其他 18(25.71%) 17(24.29%) 12(16%) 13(17.33%)
Missing 4(5.71%) 2(2.86%) 7(9.33%) 5(6.67%)
不孕原因
男方因素 8(11.43%)
女方因素 21(30.00%)
雙方因素 19(27.14%)
不明原因 20(28.57%)
Missing 2(2.86%)
p 夫: 兩組丈夫的人口學特徵比較檢定的 p value p 妻: 兩組妻子的人口學特徵比較檢定的 p value
Table2孕期性健康資訊來源
人數(%)
生殖技術懷孕組 自然受孕組 p 夫 p 妻
夫 妻 夫 妻
性資訊來源
第一孕期 61(87.14%) 64(91.43%) 60(80.00%) 57(76.00%) 0.3819 0.0136 第二孕期 58(86.57%) 60(89.55%) 61(88.41%) 59(84.29%) 0.5230 0.3617 第三孕期 44(81.48%) 46(85.19%) 51(85.00%) 49(81.67%) 0.6147 0.6147
醫師
第一孕期 20(28.57%) 17(24.29%) 18(24%) 12(16%) 0.5289 0.2535 第二孕期 8(11.94%) 11(16.42%) 19(27.54%) 15(21.43%) 0.0412 0.4547 第三孕期 11(20.37%) 12(22.22%) 11(18.33%) 12(20%) 0.7832 0.7714
護理師
第一孕期 17(24.29%) 19(27.14%) 10(13.33%) 6(8.00%) 0.1587 0.0049 第二孕期 8(11.94%) 9(13.43%) 7(10.14%) 6(8.57%) 0.5854 0.3623 第三孕期 5(9.26%) 11(20.37%) 8(13.33%) 6(10.00%) 0.4944 0.1206
媒體
第一孕期 10(14.29%) 11(15.71%) 8(10.67%) 9(12%) 0.5124 0.4617 第二孕期 8(11.94%) 15(22.39%) 14(20.29%) 10(14.29%) 0.2431 0.2197 第三孕期 9(16.67%) 14(25.93%) 12(20%) 8(13.33%) 0.6467 0.0889
自行搜尋
第一孕期 52(74.29%) 57(81.43%) 53(70.67%) 50(66.67%) 0.5859 0.0534 第二孕期 55(82.09%) 57(85.07%) 52(75.36%) 49(70.00%) 0.4434 0.0350 第三孕期 38(70.37%) 41(75.93%) 46(76.67%) 42(70%) 0.4459 0.4777 p 夫: 兩組丈夫的比較檢定的 p value
p 妻: 兩組妻子的比較檢定的 p value
Table 3 研究族群的 IIEF 嚴重度分布
生殖技術懷孕組 自然受孕組 p
第一孕期 Missing=3 Missing=3 0.7362
no ED (26<=IIEF) 37(52.86%) 46(61.33%) minimal ED (18-25) 25(35.71%) 22(29.33%) moderate ED (11-17) 4(5.71%) 4(5.33%) severe ED (1-10) 1(1.43%) 0(0%)
第二孕期 Missing=5 Missing=3 0.8137
no ED (26<=IIEF) 30(44.78%) 35(50.00%) minimal ED (18-25) 27(40.3%) 28(40.00%) moderate ED (11-17) 5(7.46%) 4(5.71%)
severe ED (1-10) 0(0%) 0(0%)
第三孕期 Missing=0 Missing=3 0.2711
no ED (26<=IIEF) 24(44.44%) 31(51.67%) minimal ED (18-25) 26(48.15%) 23(38.33%) moderate ED (11-17) 4(7.41%) 3(5%)
severe ED (1-10) 0(0%) 0(0%)
Table4 FSFI 分數, 平均值(標準差), 以無母數統計 (wilcoxon rank sum test and fisher exact test)進行檢定
生殖技術懷孕組 自然受孕組 p 第一孕期
Desire 2.75(1.18) 3.02(1.14) 0.1561 Arousal 1.81(2.09) 2.83(1.97) 0.0031 Lubrication 1.20(1.63) 2.09(1.80) 0.0022 Orgasm 1.4(1.85) 2.31(2.03) 0.0053
Satisfaction 2.19(2.61) 3.13(2.54) 0.0291
Pain 0.70(1.18) 1.33(1.40) 0.0045
FSFI 9.76(9.35) 14.72(9.81) 0.0024 FSD (%) 66(94.29%) 71(94.67%) 0.2619 第二孕期
Desire 3.01(1.14) 3.21(1.32) 0.3484 Arousal 2.24(2.14) 2.6(2.12) 0.3310 Lubrication 1.62(1.67) 1.83(1.79) 0.4983 Orgasm 1.75(1.87) 1.91(1.89) 0.6336 Satisfaction 2.49(2.56) 2.61(2.51) 0.7909 Pain 1.05(1.51) 1.26(1.49) 0.4156 FSFI 12.3(9.85) 13.60(9.94) 0.4537 FSD (%) 59(88.06%) 65(92.86%) 0.4698 第三孕期
Desire 2.65(1.06) 2.78(1.28) 0.5742 Arousal 1.67(1.84) 2.19(2.04) 0.1634 Lubrication 0.96(1.46) 1.50(1.71) 0.0823 Orgasm 1.06(1.67) 1.55(1.90) 0.1569 Satisfaction 1.70(2.43) 2.25(2.53) 0.2397 Pain 0.61(1.17) 1.09(1.48) 0.0598 FSFI 8.56(8.33) 11.34(9.79) 0.1114 FSD (%) 52(96.30%) 58(96.67%) 0.1338
科技部補助專題研究計畫出席國際學術會議心得報告
日期:107 年 7 月 30 日
一、 參加會議經過
ESHRE 是一個國際 non-profit organization;此組織之主要目標是針對不孕治療促進其生殖 科學與醫學的進步。ESHRE 是由 Robert Edwards 和 Jean Cohen 於 1984 年創立,其目的乃認為 歐洲須有一組織致力於生殖科技的發展,且有自己的期刊(Human Reproduction)及教育訓練 計畫,發展至今已有超過 6700 多名會員,其中歐洲會員占 6 成以上,其餘為世界各洲會員。
ESARE 在每年的會議上均有引領生殖科學的教育研究活動。
第 34 屆 2018 ESHRE 於西班牙加泰隆尼亞區 Barcelona 舉辦,此城市位於地中海岸,擁 有知名的人文歷史、藝術與建築,與會者置身城市中自然地享受人文的薰陶外,最重要的更有
計畫編號 MOST 106-2629-B -040 -001 -
計畫名稱 接受生殖技術治療懷孕夫妻孕期性健康—性別差異與照護需求 出國人員
姓名 李淑杏 服務機構
及職稱 中山醫學大學 護理學系 教授 會議時間 108 年 7 月 1 日至
108 年 7 月 4 日 會議地點 西班牙 巴塞隆納
會議名稱
(中文) 2018 歐洲生殖醫學會年會
(英文)
2018 ESHRE(European Society of Human Reproduction and Embryology)發表題目
(中文)以家庭為中心的照護介入對接受生殖技術治療夫妻產後憂鬱之 成效
(英文)
Effects of Family-centered postpartum care for Postpartum Depression in Previously Infertile Couples我投稿「Effects of Family-centered postpartum care for Postpartum Depression in Previously
Infertile Couples」此為科技部計畫(MOST 103-2410-H-040-001-SSS)獲大會接受以 e-poster 的方 式發表論文,著實榮幸。
二、 與會心得與建議
大會 Keynote lecture 題目為“Semen quality of young adult ICSI offspring - The first result. 探 討經由單一精蟲注射(ICSI)所生 54 位男性,在 young age(18~22 歲)時測量其精蟲狀況。因 採用 ICSI 之男性本身有較嚴重 male-factor,研究初步結果亦發現其子代的精蟲數量較少,但 因個案數少,Speaker 建議應繼續追蹤。
另外我參加下列 section,如“Before ART:Fertility awareness, assessment and preservation”、
“What about the child”、“Health risk in children born after ART”、“Female fertility preservation”、
“Endometriosis and endometrium clinical research”、“How to increase people’s fertility
awareness”、“Nurses/Midwives invited session”.這些主題多數與我的專長及研究領域有關,收穫 豐富。
比較特別的是近年於ESHRE會議有發表與生殖科技相關如疾病治療、實驗室品管及病人 心理社會照護等指引供醫療團隊於臨床與研究之參考。今年發表的主題是「多囊性卵巢症候群 評估與處置- 2018國際實證指引」(International evidence-based guideline for the assessment and management of polycystic ovary syndrome 2018)。這個由The Australian National Health and Medical Research Council (NHMRC) Centre for Research Excellence in Polycystic Ovary Syndrome (CREPCOS) (APP1078444)聯合全球相關組織完成指引,對於婦女在各生命階段 PCOS之篩檢、診斷、治療、危險評估及其對生活品質影響有完整詳細的介紹,提供臨床很好 的照護指引。
這是我初次參加 ESHRE 研討會,有非常多收穫,也有許多反思。例如:有些研究主題自 己早已有類似想法,但完成研究之進度上仍嫌緩慢,因此更期許自己應落實建構的研究主題以 與全球學者共同切磋。
三、 發表論文全文或摘要
Purpose: The purpose of this study was to develop and evaluate a family-centered postpartum care
(EPDS≧10 points, either husband or wife )checked 4 weeks after delivery. Experimental group will receive health education CD/booklet at the 5th week, and telephone consultation for 20 minutes during 6th-9th weeks after delivery. There were 180 couples recruited in the screening stage.
Forty-nine couples were randomized assign into two groups. The experimental groups consist 21 couples and the control groups consist 19 couples in the final stage. The self-administered questionnaire is composed of subjects’ profiles, Edinburgh postpartum depression scale, self-esteem questionnaire, Brief parenting stress questionnaire and social support questionnaire. Generalized estimating equation will be used for multi-variant time-series data analysis by SPSS/PC window 19.0 to evaluate the effects and difference of long-term change with the intervention.
Results: Even the experimental groups had a high demand for information of postpartum care during 3 to 6 months after delivery. The most helpful education method perceived by husbands in 3th and 6th months were booklet(86%) vs. telephone consultation(62%), booklet(62%), respectively. The most helpful education method perceived by wives in 3th and 6th months were telephone consultation(86%) vs. telephone consultation(72%), respectively. For husbands, the mean score of EPDS in the experimental groups had significantly lower than the control groups after intervention. But, for wives, the mean score of EPDS in the experimental groups had not significantly lower than the control groups after intervention.
Summary:Through this study, a family-centered postpartum care for postpartum depression among previously infertile couples model can be developed as a reference for care and policy.
Keywords: Family-centered, Intervention, Postpartum depression, Infertile couple, Assisted reproductive technology
四、攜回資料名稱及內容
International evidence-based guideline for the assessment and management of polycystic ovary syndrome 2018
計畫主持人:李淑杏 計畫編號:106-2629-B-040-001- 計畫名稱:接受生殖技術治療懷孕夫妻孕期性健康—性別差異與照護需求(第二年)
成果項目 量化 單位
質化
(說明:各成果項目請附佐證資料或細 項說明,如期刊名稱、年份、卷期、起 訖頁數、證號...等)
國 內
學術性論文
期刊論文 0
研討會論文 0 篇
專書 0 本
專書論文 0 章
技術報告 0 篇
其他 0 篇
智慧財產權 及成果
專利權 發明專利 申請中 0
件
已獲得 0
新型/設計專利 0
商標權 0
營業秘密 0
積體電路電路布局權 0
著作權 0
品種權 0
其他 0
技術移轉 件數 0 件
收入 0 千元
國 外
學術性論文
期刊論文 0
研討會論文 0 篇
專書 0 本
專書論文 0 章
技術報告 0 篇
其他 0 篇
智慧財產權 及成果
專利權 發明專利 申請中 0
件
已獲得 0
新型/設計專利 0
商標權 0
營業秘密 0
積體電路電路布局權 0
著作權 0
品種權 0
收入 0 千元
參 與 計 畫 人 力
本國籍
大專生 1
人次
參與研究歷程,學習研究設計、收案、
整理資料。
碩士生 1 參與研究歷程,學習研究設計、收案、
整理資料。
博士生 0
博士後研究員 0
專任助理 0
非本國籍
大專生 0
碩士生 0
博士生 0
博士後研究員 0
專任助理 0
其他成果
(無法以量化表達之成果如辦理學術活動
、獲得獎項、重要國際合作、研究成果國 際影響力及其他協助產業技術發展之具體 效益事項等,請以文字敘述填列。)