科技部補助專題研究計畫成果報告
期末報告
長期運動介入對失智症家族與輕微認知障礙老人的認知神經生
理與生化表現效果(第3年)
計 畫 類 別 : 個別型計畫
計 畫 編 號 : MOST 105-2410-H-006-050-MY3 執 行 期 間 : 107年08月01日至108年07月31日 執 行 單 位 : 國立成功大學體育健康與休閒研究所
計 畫 主 持 人 : 蔡佳良 共 同 主 持 人 : 白明奇
計畫參與人員: 碩士級-專任助理:劉賓亘 碩士級-專任助理:鄭篁郁
碩士班研究生-兼任助理:莊智堯 碩士班研究生-兼任助理:黃伊瑩 碩士班研究生-兼任助理:甘育嘉
報 告 附 件 : 出席國際學術會議心得報告
中 華 民 國 108 年 10 月 21 日
中 文 摘 要 : 1. 老化時期會出現血液中神經成長因子濃度減少、低程度發炎、與 神經認知功能降低, 這些現象都與神經退化性疾病(例如:阿茲海默 症)有所關聯,不過,運動能改善這些老化現象,進而避免神經退化 性疾病的發生。本研究目的在了解有氧與肌力運動是否能對神經保 護成長因子、發炎指標、和神經認知表現產生不同的效果,進而了 解這些分子生物指標改變是否與神經認知改變有所關聯。55位輕微 認知障礙老年人被隨機分成有氧組、肌力組或控制組,所有研究參 與者執行轉換作業任務時的神經認知表現(例如:行為和大腦事件相 關位)、和周邊血液中的神經保護成長因子(例如:腦衍生成長因子
、類胰島素成長因子-1、血管增生指標)與發炎指標(例如:TNF-α, IL-1β, IL-6, IL-8, and IL-15)濃度,在16週運動介入前後皆被 量測。結果發現:規律從事有氧和肌力運動能部份地改善輕微認知 障礙老年人執行作業轉換認知作業時的神經認知表現(例如:在轉換 情境時的反應時間與正確率、腦波 P3振幅),但P2成分波與P3潛時 則未產生改變;在血液生化指標方面,規律16週運動雖無法改變血 管增生指標(VEGF和FGF-2)和部分發炎指標(例如:IL-1β、IL-6和 IL-8),但有氧運動能顯著提升腦衍生成長因子濃度並降低TNF-α和 IL-15濃度,而阻力訓練則顯著提升類胰島素成長因子-1並降低IL- 15濃度。血液生化指標與神經認知表現的改變兩者達到接近顯著的 關聯性。這些研究發現暗示有氧和阻力運動皆能明顯改善與失智症 有關的輕微認知障礙族群之神經滋養因子與發炎指標濃度,並促進 神經認知表現。不過,這兩種運動型態似乎是藉由不同的分子機制 來達到提升神經認知表現的效果。
2. 本研究在探討有失智症家族史的族群中,ApoE-4基因型是否會對 其血液中分子生物指標與神經認知功能產生影響,進而了解這兩種 依變項與身體適能的關聯性。110位有失智症家族史的研究參與者透 過基因篩檢後,其中16位帶有ApoE-4基因型,經施測他們的視覺空 間工作記憶力與血液分子生物指標後,和另外16位有失智症家族史 但無ApoE-4基因型的控制組進行比較。結果發現兩組的血液生化指 標(例如:IL-1β、IL-6、IL-8、BDNF、Aβ1-40、Aβ1-42)都無組 間差異,但部分神經認知表現(例如:只有在記憶力負荷較高情境下 出現較低正確率和較差的神經震盪表現),其中行為表現與最大攝氧 量達顯著關聯性。這些結果說明有失智症家族史伴隨有ApoE-4基因 型的族群,此時期僅有一些神經認知障礙,提高心肺功能或許能改 變他們未來惡化成失智症問題。
中 文 關 鍵 詞 : 有氧運動; 阻力運動; 認知; 分子調節; 輕微認知障礙; 阿茲海默 家族史; 神經震盪; 發炎指標; 乙型澱粉漾蛋白; 腦衍生成長因子;
身體適能; 載脂蛋白ε4等位基因
英 文 摘 要 : 1: The purposes of the present study included investigating whether both aerobic and resistance exercise produce
divergent effects on the neuroprotective growth factors, inflammatory cytokines, and neurocognitive performance, and further exploring whether changes in the levels of these molecular biomarkers are associated with alterations in neurocognitive performance. Fifty-five older adults with amnestic MCI (aMCI) were recruited and randomly assigned to
an aerobic exercise (AE) group, a resistance exercise (RE) group, or a control group. The assessment included
neurocognitive measures during a task-switching paradigm, as well as circulating neuroprotective growth factors and inflammatory cytokine levels at baseline and after either a 16-week aerobic or resistance exercise intervention program or a control period. The results showed that aerobic and resistance exercise could effectively partially facilitate neurocognitive performance [e.g., accuracy rates (ARs), RTs during the heterogeneous condition, and ERP P3 amplitude]
when the participants performed the task switching paradigm although the ERP P2 components and P3 latency could not be changed. In terms of the circulating molecular biomarkers, the 16-week exercise interventions did not change some parameters (e.g., VEGF, FGF-2, IL-1β, IL-6, and IL-8).
However, the peripheral serum BDNF level was significantly increased, and the levels of insulin, TNF-α, and IL-15 levels were significantly decreased in the AE group, whereas the RE group showed significantly increased IGF-1 levels and decreased IL-15 levels. The relationships between the changes in neurocognitive performance (AR and P3 amplitudes) and the changes in the levels of
neurotrophins (BDNF and IGF-1)/inflammatory cytokines (TNF- α) only approached significance. These findings suggested that in older adults with aMCI, not only aerobic but also resistance exercise is effective with regard to increasing neurotrophins, reducing some inflammatory cytokines, and facilitating neurocognitive performance. However, the aerobic and resistance exercise modes likely employed divergent molecular mechanisms on neurocognitive facilitation.
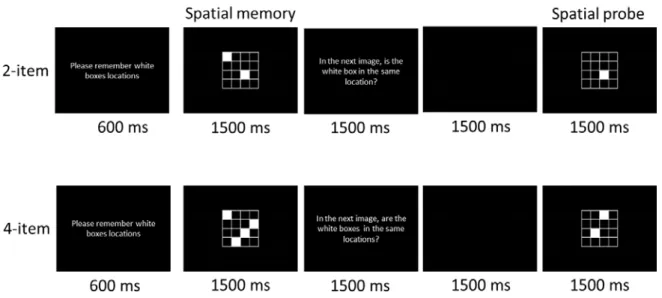
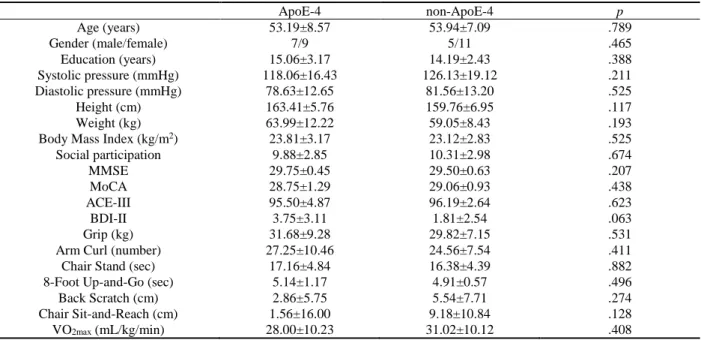
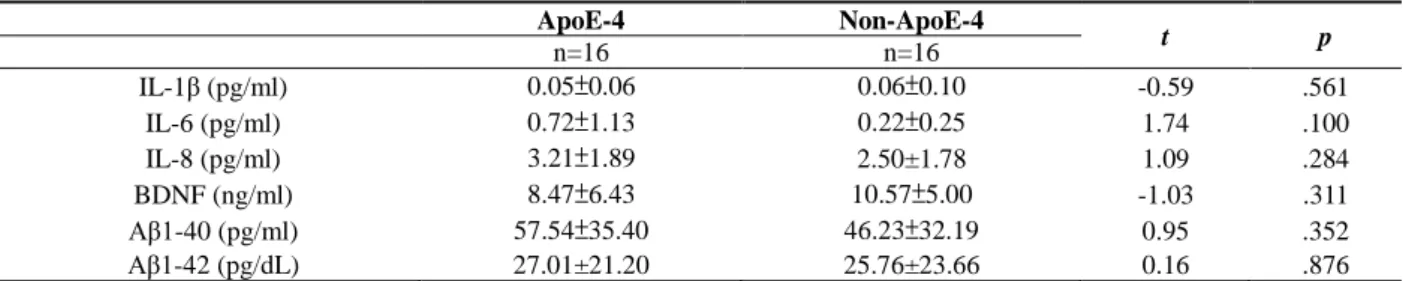
2: The primary purpose of this study was to determine whether ADFH individuals with the ApoE-4 genotype show deviant brain event-related neural oscillatory performance and cognitively-related molecular indices. A secondary purpose was to examine the interactive effects on physical fitness. Blood samples were provided from 110 individuals with ADFH to assess molecular biomarkers and the ApoE genotype for the purpose of dividing them into an ApoE-4 group (n=16) and a non-ApoE-4 group (n=16) in order for them to complete a visuospatial working memory task while simultaneously recording electroencephalographic signals.
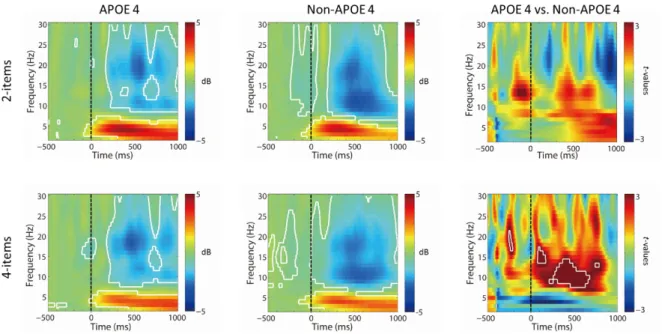
They also performed a senior functional physical fitness (SFPF) test. While performing the cognitive task, the ApoE- 4 relative to non-ApoE-4 group showed worse accuracy rates (ARs) and brain neural oscillatory performance. There were no significant between-group differences with regard to any molecular biomarkers (e.g., IL-1β, IL-6, IL-8, BDNF, Aβ1-
40, Aβ1-42). VO2max was significantly correlated with the neuropsychological performance (i.e., ARs and RTs) in the 2-item and 4-item conditions in the ApoE-4 group and across the two groups. ADFH individuals with the ApoE-4 genotype only showed deviant neuropsychological (e.g., ARs) and neural oscillatory performance when performing the
cognitive task with a higher visuospatial working memory load. Cardiorespiratory fitness potentially played an important role in neuropsychological impairment in this group.
英 文 關 鍵 詞 : Aerobic exercise; resistance exercise; cognition; molecular mediators of exercise-induced response; mild cognitive impairment; Alzheimer's disease of family history; neural oscillation; inflammatory cytokines; amyloid-β; BDNF;
cognition; physical fitness; APOE-4
科技部補助專題研究計畫成果報告
( □期中進度報告/█期末報告)
長期運動介入對失智症家族與輕微認知障礙老人的認知神經生理與
生化表現效果
計畫類別: █個別型計畫 □整合型計畫
計畫編號: MOST 105-2410-H-006-050-MY3
執行期間:105 年 8 月 1 日至 108 年 7 月 31 日
執行機構及系所:成功大學管理學院體育健康與休閒研究所
計畫主持人:蔡佳良
共同主持人:白明奇
計畫參與人員:劉賓亘、鄭篁郁、莊智堯、黃伊瑩、甘育嘉
本計畫除繳交成果報告外,另含下列出國報告,共 1 份:
□執行國際合作與移地研究心得報告
█出席國際學術會議心得報告
□出國參訪及考察心得報告
Part 1: Pages 1-36
Part 2: Pages 37-54
中 華 民 國 108 年 10 月 21 日
1
Pat 1
Abstract
Decreased levels of the neuroprotective growth factors, low-grade inflammation, and reduced neurocognitive functions during aging are associated with neurodegenerative diseases, such as Alzheimer’s disease. Physical exercise modifies these aging phenomena while a sedentary
lifestyle promotes them, thus contributing to neurodegeneration. The purposes of the present study included investigating whether both aerobic and resistance exercise produce divergent effects on the neuroprotective growth factors, inflammatory cytokines, and neurocognitive performance, and further exploring whether changes in the levels of these molecular biomarkers are associated with alterations in neurocognitive performance. Fifty-five older adults with amnestic MCI (aMCI) were recruited and randomly assigned to an aerobic exercise (AE) group, a resistance exercise (RE) group, or a control group. The assessment included neurocognitive measures [e.g., behavior and event-related potential (ERP)] during a task-switching paradigm, as well as circulating
neuroprotective growth factors (e.g., BDNF, IGF-1, VEGF, and FGF-2) and inflammatory cytokine (e.g., TNF-α, IL-1β, IL-6, IL-8, and IL-15) levels at baseline and after either a 16-week aerobic or resistance exercise intervention program or a control period. The results showed that aerobic and resistance exercise could effectively partially facilitate neurocognitive performance [e.g., accuracy rates (ARs), RTs during the heterogeneous condition, global switching cost, and ERP P3 amplitude] when the participants performed the task switching paradigm although the ERP P2 components and P3 latency could not be changed. In terms of the circulating molecular biomarkers, the 16-week exercise interventions did not change some parameters (e.g., leptin, VEGF, FGF-2, IL-1β, IL-6, and IL-8). However, the peripheral serum BDNF level was significantly increased, and the levels of insulin, TNF-α, and IL-15 levels were significantly decreased in the AE group, whereas the RE group showed significantly increased IGF-1 levels and decreased IL-15 levels. The relationships between the changes in neurocognitive performance (AR and P3 amplitudes) and the changes in the levels of neurotrophins (BDNF and IGF-
1)/inflammatory cytokines (TNF-α) only approached significance. These findings suggested that in older adults with aMCI, not only aerobic but also resistance exercise is effective with regard to increasing neurotrophins, reducing some inflammatory cytokines, and facilitating neurocognitive performance. However, the aerobic and resistance exercise modes likely employed divergent molecular mechanisms on neurocognitive facilitation.
Keywords: aerobic exercise, resistance exercise, cognition, molecular mediators of exercise- induced response, mild cognitive impairment
2
Introduction
Alzheimer’s disease (AD)-related neuropathological characteristics are associated with reduced circulating peripheral and cerebrospinal fluid (CSF) levels of neuroprotective growth factors, such as brain-derived neurotrophic factor (BDNF) [1-3], insulin-like growth factor-1 (IGF-1) [4], vascular endothelial growth factor (VEGF) [5], and fibroblast growth factor-2 (FGF- 2) [6, 7]. In human post-mortem brain tissue, decreased BDNF gene mRNA and protein levels have been found in the hippocampus and neocortex of AD patients [8-10]. Serum BDNF levels were found to be reduced in patients with early or late onset AD compared to age-matched healthy controls [11]. Even in the earliest, prodromal stages of dementia [i.e., mild cognitive impairment (MCI)], the levels of BDNF precursor and mature BDNF in the specific brain regions are
significantly reduced [12], which is associated with a decline in executive functions [13]. Low serum IGF-1 has been reported to be associated with increased amyloid-β (Aβ) accumulation [14]
and age-related brain amyloidosis [15]. Higher serum IGF-1 could enhance clearance of the brain Aβ [14]. Angiogenic trophic factors VEGF and FGF-2 are markedly reduced with aging, which could be one potential cause of a dramatic decline in dentate gyrus neurogenesis/astrocyte activity in the aging hippocampus [7], contributing to learning and memory impairment [6,7]. AD has been suggested to be an angiogenesis-dependent disorder [16], and patients with AD have been found to show a significant decrease in serum VEGF as compared to patients with vascular dementia and healthy elderly individuals [5]. In addition, cerebrovascular alterations are often observed in patients with MCI [17]. It may soon be confirmed that aberrant secretion of
neuroprotective growth factors could play an important role in the pathogenesis and progression of AD neuropathology.
Cytokines play a central role in neuro-immune-endocrine processes and influence cognition via diverse mechanisms [18]. Neuroinflammation is suggested to contribute to AD pathogenesis [11,19]. Higher levels of pro-inflammatory cytokines have been proposed as independent, strong predictors of increased risk of progression from MCI to AD [20, 21]. Interleukin-1-beta (IL-1β), IL-6 and IL-8, which are the most potent inflammatory cytokines, are products of activated microglia and astrocytes and are up-regulated in AD brains [22, 23]. Most studies on this topic have observed elevated serum IL-6 levels in AD patients [22, 24, 25]. Similar conditions (i.e., higher serum levels of IL-1β, IL-6, and IL-8) have also been reported in patients with MCI or AD [22, 26-28]. In addition, IL-15 is elevated in the CSF of patients with AD and is associated with frontotemporal degeneration [29]. Lombardi et al. [30] and Gezen-Ak et al. [11] reported that serum levels of proinflammatory cytokine TNF-α are significantly increased in patients with early or late onset AD relative to healthy controls. Higher serum TNF-α levels have also been found in patients with MCI [11, 27, 31, 32]. Importantly, high TNF-α levels during aging and in AD may contribute to amyloidosis [14, 33, 34]. Also, in terms of new genetic risk factors for AD that are associated with inflammation, elevated levels of inflammatory biomarkers, including complement
3
proteins, reflect the polygenic risk scores in AD. This clearly suggests a link between genetic risk and circulating disease predictors/biomarkers that could be used for the screening stratification of AD patients [35]. Genome Wide Association Studies identified several candidate genes involved in inflammation and immune responses that could also be used to predict risk of late onset Alzheimer’s disease. These include TREM2 (triggering receptor expressed on myeloid cells 2 protein, which is involved in the regulation of immune response/cytokine production), IL-6, IL-1β, IL-10, and a few other inflammatory markers [36-38]. It can be assumed that, similar to other diseases resulting “from physical inactivity” [39], neurodegenerative processes in AD are modulated by the interaction of genetic predisposition and a sedentary lifestyle, which can promote inflammation both at a systemic level as well as in the brain. Collectively, the
abnormalities of circulating levels of these inflammatory cytokines likely represent a very early or preclinical stage of AD pathogenesis.
Although no curative pharmacotherapy currently exists for dementia at present, a growing number of studies have documented significant benefits of long-term, regular exercise on normal cognitive aging, dementia risk/progression, and perhaps AD-related pathological biomarkers (e.g., reducing amyloid-β 42 and tau phosphorylation) [40-43]. Since circulating peripheral levels of neuroprotective growth factors and inflammatory cytokines have been suggested to be associated with AD-type brain pathology, as mentioned above, the identification of a means of modulating the levels of neuroprotective growth factors and pro-inflammatory cytokines represent important advances in the treatment AD [11]. Skeletal muscle has the capacity to express and release several cytokines/myokines, including IL-6, IL-8, IL-15, BDNF, and FGFs [44]. Regular physical exercise has been recommended as an effective non-pharmacological intervention capable of enhancing the expression/concentrations of neuroprotective growth factors [41, 45-53] and positively modulating pro-inflammatory/anti-inflammatory pathways [27, 54-56], which have been proposed as putative markers/mediators of exercise-induced benefits on both the brain and cognition [57, 58].
Nevertheless, divergent molecular mechanisms that facilitate cognition seem to be, at least to a certain extent, exercise-mode dependent (e.g., aerobic and resistance exercise) [51, 59]. Although a resistance exercise mode has also been demonstrated to be effective with regard to improving neurocognitive functions in the elderly [45, 60-62], until now, most previous clinical trials have focused on investigating the effects of long-term aerobic exercise in MCI/dementia [41, 63], so only limited information exits on the adaptive response to resistance exercise [64, 65], especially as it relates to neuroprotective and neuroinflammatory biomarkers. Therefore, an investigation of the distinct effects of different exercise modes on the neurocognitive and molecular indices in MCI seems warranted.
MCI, which is a transitional stage from normal aging to dementia [66], is a clinical syndrome with a high-risk rate (i.e., 10 to 54%) of developing into dementia or AD on an annual basis [67, 68]. Since cognition can be preserved or even improved in the MCI stage [69, 70], it is worth finding strategies for prevention and/or delay of the progression of MCI into dementia/AD.
4
Individuals with MCI have been demonstrated to exhibit abnormalities in neurocognitive
performance during the task-switching paradigm [71, 72], which is likely associated with reduced cardiorespiratory fitness [72]. A growing number of clinical studies have reported physical- activity/exercise-related impacts on behavioral [e.g., accuracy rate (AR) and reaction time (RT)]
and electrophysiological [e.g., event-related potential (ERP) P3 component] outcomes of the task- switching paradigm among elderly subjects [43, 62, 73, 74]. Physical exercise has been
demonstrated to be effective with regard to improving logical memory and reducing whole brain cortical atrophy in older adults with amnestic MCI (aMCI) [75, 76]. Thus far, no studies have explored whether there are different effects of aerobic and resistance exercise interventions on neurocognitive performance (i.e., behavior and ERPs) and neuroprotective (e.g., BDNF, IGF-1, VEGF, and FGF-2) and inflammatory (e.g., TNF-α, IL-1β, IL-6, IL-8, and IL-15) biomarkers in patients with aMCI. Therefore, the purpose of the present study was to investigate whether aerobic and resistance exercise produce divergent effects on these molecular biomarkers and
neurocognitive performance in older individuals with aMCI. We hypothesized that a 16-week aerobic or resistance exercise intervention could effectively improve neurocognitive performance, potentially through divergent molecular factors (e.g., neuroprotective growth factors and
cytokines) in patients with aMCI where exercise-induced neurocognitive changes could be associated with changes in these peripheral bioactive molecules.
Methods Participants
Fifty-five older adults with amnestic MCI (aMCI) aged 60-85 years were recruited through the Alzheimer’s Disease Research Center, National Cheng Kung University Hospital, following a clinically standardized inclusion criteria [77-79]: (1) objective memory impairment for age, (2) subjective memory complaints confirmed by family members, (3) an absence of dementia, (4) a Clinical Dementia Rating of 0.5, (5) absence of significant levels of impairment in other cognitive domains (e.g., language, orientation, attention, and abstraction), as assessed by the Cognitive Abilities Screening Instrument [80], (6) Mini-Mental State Examination (MMSE) scores > 24, (7) largely intact functional activities of daily living, (8) no brain abnormalities (e.g., malignant brain tumors or stroke) via structural MRI scans, and (9) the Beck Depression Inventory, 2nd edition (BDI-II) scores < 13 [81]. Structural brain examinations via computed tomography and functional examinations via single photon emission computed tomography and were performed when more information was needed to confirm the diagnosis. All participants had no history of other
significant neurological disorders, significant cerebrovascular disease, current psychiatric illnesses, musculoskeletal impairment, use of anti-dementia medicine, or substance abuse or addiction. The Edinburgh Handedness Inventory [82] assessed all participants as right-handed.
They had normal (or corrected to normal) vision based on the minimal 20/20 standard and had not regularly participated in exercise activities in the prior two years. An informed consent form,
5
approved by the local Institution Ethics Committee, was read and signed by all the participants.
Experimental procedure
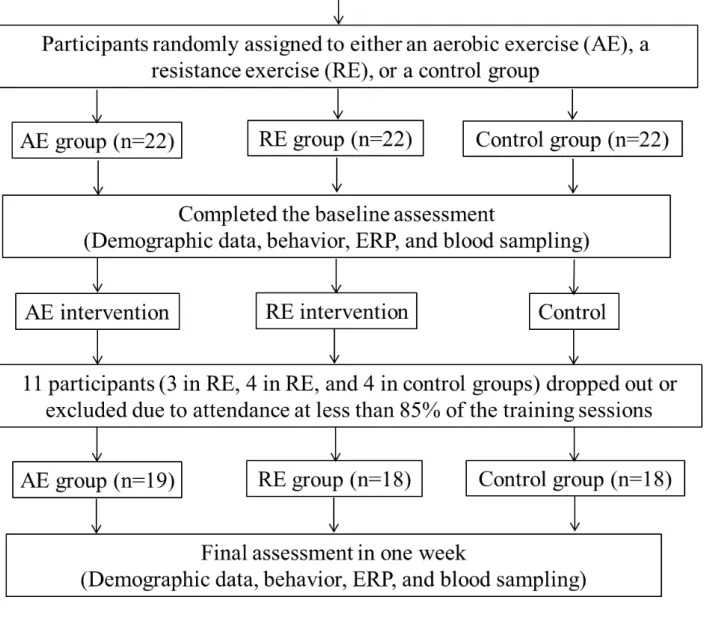
The Consolidated Standards of Reporting Trials (CONSORT) flowchart outlining the number of participants from the first contact to study completion is shown in Figure 1. The original
participants comprised 66 sedentary older adults with aMCI who were randomly divided into three groups by drawing an envelope with the intervention assignment enclosed: an aerobic exercise (AE) group, a resistance exercise (RE) group, and a control group. After a sixteen-week exercise intervention, eleven participants dropped out or were excluded due to attendance at less than 85%
of the exercise sessions. The remaining 55 participants (AE: n=19; RE: n=18; Control: n=18) were included in the current study. The three groups did not significantly differ in terms of any of the characteristics at baseline (see Table 1).
The participants were asked to visit the cognitive neurophysiology laboratory for two
separate sessions before the formal exercise intervention. During the first session, each participant completed an informed consent form, a handedness inventory, the basic information form (e.g., a demographic questionnaire, a medical history, the DBI-II, the MMSE, a social participation questionnaire [83], and the digit span component of the Wechsler-IV Adult intelligence test [84]) to assess the working memory span. The Physical Activity Readiness Questionnaire (PARQ) [85]
and a seven-day physical activity recall questionnaire (7-day PAR) [86] were used to examine the participants’ previous levels of physical activity to lower potential risk factors before the 16-week physical exercise intervention. Their height and weight were also measured to calculate their BMI [Body Mass Index, weight (kg)/height (m)2]. Two certified fitness instructors then completed all senior functional physical fitness assessments [87] and hand grip for each participant. The
participants’ cardiorespiratory fitness was assessed using the Rockport Fitness Walking Test [88], which is a low-risk, low-cost, non-exercise estimate of cardiorespiratory fitness with high
validation in low-activity older adults [89]. The volunteers were required to walk one mile as quickly as possible, with heart rate (HR) being continuously recorded using a Polar heart rate (HR) monitor (RX800CX, Finland). One repetition maximum (1-RM) and peak muscle power were assessed for each participant in the RE group to determine the exercise intensity [90] when performing biceps curls, triceps extensions, bench presses, leg presses, leg extensions, and vertical butterflies.
On a separate day in the same week, each participant was required to refrain from strenuous exercise for at least 24 hours, and caffeine, food, and alcohol intake were also prohibited for at least 12 hours since these factors can be associated with electrophysiological signal performance [91, 92] and biochemical markers [93]. They were asked to arrive at the laboratory, which had an acoustically shielded room with dimmed lights, between 8:30 and 9:30 am to control for circadian influences. When arriving at the laboratory, each participant was asked to sit in an adjustable chair in front of a computer screen (width = 43 cm), with the viewing distance being approximately 75cm. Then, an electrocap and electro-oculographic (EOG) electrodes were attached to the
6
subject’s scalp and face. After the practice trials to determine whether the participants had become familiar with the rules of the cognitive task, blood was drawn, and then the formal cognitive test was immediately administered, with concomitant electrophysiological signals (i.e., ERPs) being recorded.
After a sixteen-week exercise intervention, the participants were also asked to visit the laboratory within one week for two separate sessions to complete the pre-intervention procedure.
Compliance with the prescribed exercise protocol was high (> 95%) during the intervention period.
Interventions
The effects of this type of intervention on the cognition and fitness of individuals with MCI have already been reported in previous studies [55, 94].
Aerobic exercise (AE) group
Participants in the AE group attended three supervised exercise sessions per week for 16 consecutive weeks on either a bicycle ergometer or a motor-driven treadmill (Medtrack ST55, Quinton Instrument Company, United States) according to the participant’s lower-extremity function, with the exercise intensity corresponding to 50-60% of the individual target heart rate reserve (HRR, HRmax-HRresting) during the first two weeks and 70-75% of the HRR for the remainder of the program. Each aerobic exercise session involved a 5-minute warm-up period, followed by 30 minutes of continuous bike riding or brisk walking/jogging at an intensity that would maintain the heart rate within the assigned training range, followed by 5 minutes of cool- down. A Polar HR monitor (RX800CX, Finland) was used to monitor each participant’s heart rate during the exercise.
Resistance exercise (RE) group
The participants in the RE group also attended three supervised exercise sessions per week for 16 weeks with the use of free weights and bodybuilding machines, with exercise intensity corresponding to 60-70% of the individual target 1RM during the first two weeks and 75% of their target 1RM for the remainder of the program. Each resistance exercise session involved a 5-
minute warm-up period (e.g., slow-paced walking and active mobility exercises for the joints of the four limbs), followed by 30 minutes of core content, followed by 5 minutes of cool-down. The core RE content consisted of the following circuit-exercise schedule: biceps curls, vertical
butterflies, leg presses, seated rowing, hamstring curls, and calf raises. The participants performed the resistance exercise at the target intensity for three sets of 10 repetitions with a 90-second rest between sets, and a two-minute interval between each apparatus.
Control group
To control for placebo effects [95] and to rigorously make the variables (i.e., social interactions, motivation, and schedule) as similar as possible to the AE and RE groups [43, 48, 96], participants in the control group were also asked to visit the laboratory three times a week for 16 weeks. They performed static stretching exercises with an instructor and videotape guidance.
7
However, this exercise mode did not provide a load on their cardiorespiratory and musculoskeletal system, such as occurred during the aerobic and resistance training, respectively [48, 97]. Every class included a 5-min warm-up period, core content, and a 5-min cool-down period. To maintain the participants’ interest, different stretching and balancing techniques were used with various types of equipment (e.g., balance boards and fitness balls).
Cognitive task
The task-switching paradigm employed in the present study was adopted from one previously used by Tsai et al. [72] used in older adults with aMCI to show deficits in neurocognitive
performance as compared to healthy cohorts. The task switching paradigm included two tasks (low/high and odd/even tasks) using the same numeric stimuli. The white stimuli (digits 1–9, excluding 5) were presented focally in the center of a computer screen on a black background after counting down in reverse order, 3, 2, and 1. The participants had to judge whether the digit was greater or less than five (low/high task), or whether it was odd or even (odd/even task), when the digit was surrounded by a solid or broken square, respectively. The task-switching paradigm involved two homogeneous conditions and one heterogeneous condition and consisted of six blocks of stimuli, with a brief rest period in the middle of each block. The first two blocks were the homogeneous conditions in which only one task (i.e., less/more than 5 or odd/even task) with 64 trials was performed, which were counterbalanced across participants. Blocks 3-6 were the heterogeneous conditions with 256 trials (64 trials×4 blocks), in which two equiprobable task sets (i.e., less/more than 5 and odd/even tasks) were alternated randomly, with seven consecutive trials as the maximum number performed repeatedly for each task. The participants were thus required to switch between two tasks on some trials and to repeatedly perform the same task during trials in other cases in the heterogeneous block. The participants were asked to use their left index finger to press the X button on the keyboard when the digit was less than five or odd. In contrast, when the digit was greater than five or even, the participants were asked to use their right index finger to press the M button. The participants were instructed to press the response button as quickly and accurately as possible. Digits were presented on the screen for 200ms, with a 2000ms response- stimulus interval. Participants were given the task instructions, and each block (e.g., single-task as well as task-switch trials) was preceded by a series of practice trials before the formal test to familiarize the participants with the rules.
Electrophysiological recording and analysis
Electroencephalographic (EEG) activity was recorded from 18 electrode sites (F3, F4, Fz, F7, F8, C3, Cz, C4, T3, T4, T5, T6, P3, Pz, P4, O1, Oz, and O2) using an elastic electrode cap (Quik- Cap, Compumedics Neuroscan, Inc., El Paso, TX) designed for the International 10-20 System.
Additional ocular electrodes were placed on the supero-lateral right canthus and infero-lateral to the left eye to monitor horizontal and vertical EOG (i.e., HEOG and VEOG) activity for eye movements. Scalp locations were referred to linked mastoid electrodes, while a ground electrode was placed on the mid-forehead on the Quik-Cap. All electrode impedances were below 5kΩ.
8
EEG data acquisition employed an A/D rate of 500 Hz/channel, a band-pass filter of 0.1-50 Hz, and a 60 Hz notch filter, with continuous writing to hard disk for off-line analysis using SCAN4.3 analysis software (Compumedics Neuroscan, Inc., El Paso, USA).
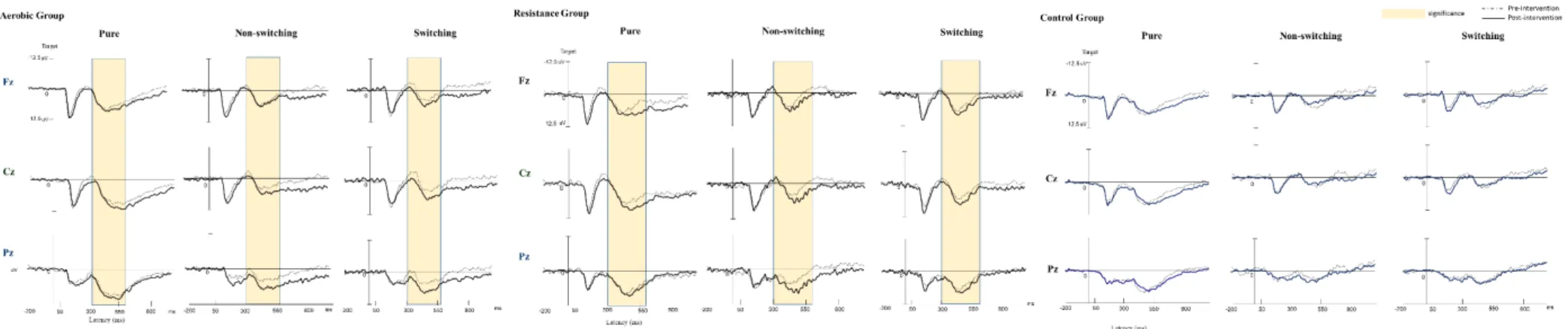
ERP analysis epochs extracted off-line consisted of segments from -200ms of pre-stimulus activity to 1000ms of post-stimulus activity. All trials with response errors and blink artifacts (i.e., VEOG, HEOG, and electromyogram exceeding ±100 μV) were excluded offline. The remaining effective ERP data were averaged across epochs according to the different trial types. When an individual performs a visual task-switch paradigm, ERP P2 and P3 components are evoked simultaneously to respectively represent the target for a unique component of cognitive control regarding the switching cost or task-set activation (i.e., ERP P2), as well as the task-set updating processes and attentional resources allocated to the updating of working memory (i.e., ERP P3) [72]. Since a cognitive task relies on a set of separate components implicating a fronto-to-parietal network of brain areas [71], in the present study, the two stimulus-locked ERP components, P2 and P3, in the three electrodes (Fz, Cz, and Pz) were thus identified in artifact-free trials followed by correct responses and analyzed to quantify the effects of the physical exercise intervention and stimulus type [72]. Two types of ERP variables (i.e., amplitudes and latencies) were measured.
ERP P2 and P3 mean that amplitudes were calculated within 150-300ms and 300-650ms latency windows, respectively. Latencies were defined as the time point of the maximal amplitude within the latency window for every participant, and the results were equivalent for the ERP elicited by all conditions and participants.
Blood sampling and analysis
A 10-mL blood sample was obtained by a qualified phlebotomist from the antecubital vein prior to and after the exercise intervention. The blood samples were drawn for the analysis of serum insulin, leptin, neuroprotective growth factors (e.g., BDNF, IGF-1, VEGF, and FGF-2), and cytokine (e.g., TNF-α, IL-1β, IL-6, IL-8, and IL-15) levels. The blood samples were kept at room temperature to allow for clotting (BD Vacutainer Plus) and then were centrifuged at 3000 rpm for 15 minutes at 4°C (Hettich Mikro 22R, C1110). The serum was aliquoted and stored at –80°C for further marker assays. The levels of serum insulin, leptin, neuroprotective growth factors (e.g., BDNF, IGF-1, VEGF, and FGF-2), and inflammatory cytokines (e.g., TNF-α, IL-1β, IL-6, IL-8, and IL-15) were analyzed using Human Cytokine Antibody-Immobilized Magnetic beads (Millipore, Billerica, MA, USA). Measurements were performed on a Luminex 200 analyzer (Luminex, Austin, TX, USA). The entire procedure for the determination of the molecular markers was performed by the same person to avoid inter-operator bias. The pre- and post-samples were analyzed using the same assay kit, with the intra-assay variability between 2-10%.
Data processing and statistical analysis
Accuracy rates (ARs) and reaction times (RTs) were measured and analyzed to determine behavioral performance. Individual trials with RTs shorter than 100ms and longer than 2400ms were excluded from further analyses. Two types of switching cost (i.e., the global switching cost
9
and the local switching cost) were respectively determined by subtracting the mean RT between homogeneous and heterogeneous conditions and by subtracting the mean RT between switching and non-switching trials during the heterogeneous condition. When an individual performs the task-switching task, global switching cost and local switching cost represent two cognitive
processing abilities (i.e., to maintain the two task sets where the individual must alternate between the working memory and reconfiguring actions from trial to trial, according to the relevant task sets) [72]. Three trial types were subjected to behavior (i.e., ARs and RTs) and
electrophysiological (i.e., ERP P2 and P3 latencies and amplitudes) statistical analyses: a “pure”
trial in the homogeneous condition and “non-switching” and “switching” trials in the heterogeneous condition [72].
A one-way analysis of variance (ANOVA) was used to analyze the differences in the demographic backgrounds (except sex, for which a Pearson’s chi-squared test was used) of the participants in the AE, RE, and control groups. The ARs and correct-trial RTs were submitted separately to a 3 (Group: AE vs. RE vs. Control) × 2 (Time: pre-exercise vs. post-exercise) × 3 (Trial types: pure vs. non-switching vs. switching) mixed repeated measures analysis of variance (RM-ANOVA). P2 and P3 latencies and amplitudes from ERP recordings were submitted
separately to a 3 (Group: AE vs. RE vs. control) × 2 (Time: pre-exercise vs. post-exercise) × 3 (Trial types: pure vs. non-switching vs. switching) × 3 (Electrode: Fz vs.Cz vs. Pz) RM-ANOVA.
All biochemical markers were submitted separately to a 3 (Group: AE vs. RE vs. Control) × 2 (Time: pre-exercise vs. post-exercise) RM-ANOVA. The homogeneity and normality of variance assumptions were confirmed with the Levene and Lilliefors test and the Kolmogorov-Smirnov test, respectively. When the RM-ANOVAs revealed significant effects due to the simple main effects and interactions, posterior comparisons of the mean values were carried out through appropriate multiple comparisons (adjusted using the Bonferroni correction). Whenever the RM- ANOVA detected a major violation of the sphericity assumption, the Greenhouse-Geisser (G-G) correction adjusted the significance levels of the F ratios. A partial eta squared (ηp2) was adopted to calculate effect sizes for significant main effects and interactions, with the following
conventions used to determine the magnitude of mean effect size: 0.01-0.059 representing a small effect size, 0.06-0.139 a medium effect size, and ≧0.14 a large effect size [98]. Pearson product- moment correlations were used to examine (1) changes in the neurocognitive performance and biochemical markers and (2) changes in the cardiorespiratory (i.e., the estimated VO2max) and muscular (i.e., the hand grip and chair stand) fitness, as well as the neurocognitive and
biochemical indices prior to and after the exercise intervention. Significance was set at p <.05 for all analyses.
Results
Characteristics of the study population
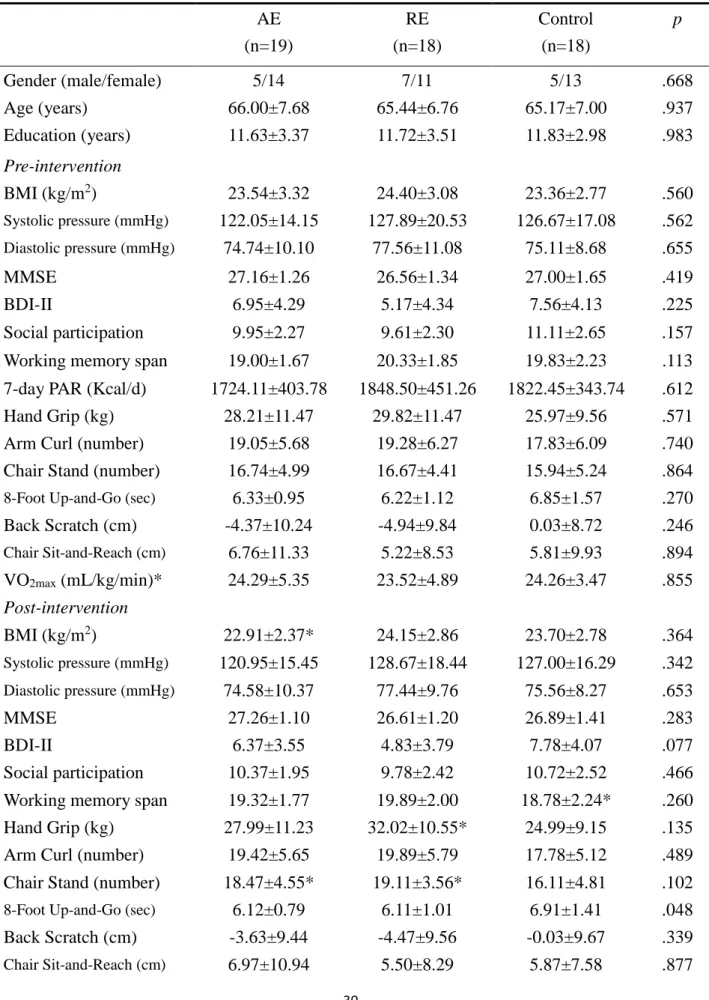
Table 1 presents an overview of the pre- and post-intervention characteristics of the
10
participants. At baseline, there were no significant differences (all ps>.05) at the group level with regard to any demographic characteristics, confounding factors (e.g., years of education, BMI, blood pressure, social participation, working memory span, global cognitive function, depression, and cardiorespiratory fitness) in relation to cognition, or with regard to the tests of senior
functional physical fitness in the AE, RE, and control groups. Paired t tests showed that, compared to pre-intervention, the AE group had significantly lower BMI and improved scores for the chair stand test and cardiorespiratory fitness (i.e., estimated VO2max) after the intervention; the results for the RE group showed that the scores for the hand-grip dynamometry and chair stand test were significantly improved, and the control group was significantly worse in working memory span and cardiorespiratory fitness performance. At the post-intervention, there were significant differences at the group level with regard to the scores for the 8-Foot Up-and-Go test and
cardiorespiratory fitness among the three groups. Post hoc only showed that the AE group showed significantly higher levels of cardiorespiratory fitness compared to the RE and control groups (AE vs. RE: p=.017; AE vs. Control: p=.010).
Neuropsychological performance Accuracy rate (AR)
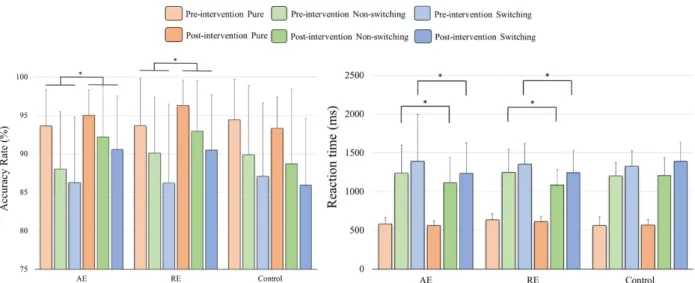
As seen in Figure 2, the RM–ANOVA performed on the ARs for the task-switching paradigm revealed the main effects of Time [F(1,52)=6.34, p=.015, ηp2=0.11] and Trial [F(2,104)=55.25, p<.001, ηp2=0.52], with a higher AR for post- (91.7%) than pre-intervention (89.9%), and with the following trial gradient: pure (94.4%) > non-switching (90.3%) > switching (87.8%). The
interaction between Time × Group [F(2,52)=4.18, p=.021, ηp2=0.14] was also significant. The post-hoc analysis showed that, relative to the pre-intervention, the AE and RE groups exhibited significantly higher ARs [AE: F(1,18)=6.02, p=.025, ηp2=0.25; RE: F(1,17)=5.64, p=.030, ηp2=0.25] across the three trials after the intervention.
Reaction time (RT)
The RM–ANOVA performed on the RTs for the task-switching paradigm revealed the main effects of Time [F(1,52)=12.28, p=.001, ηp2=0.19] and Trial [F(2,104)=305.41, p<.001, ηp2=0.86], with faster RTs for post- (1002.04ms) as compared to pre-intervention (1059.48ms) and with the following trial gradient: pure (586.47ms) < non-switching (1182.46ms) < switching (1323.35ms).
The interactions between Time × Group [F(2,52)=6.42, p=.003, ηp2=0.20] and Time × Group×
Trial [F(4,104)=2.49, p=.048, ηp2=0.09] were also significant. The post-hoc analysis for the Time
× Group × Trial interaction showed that the AE group exhibited significantly faster RTs in the non-switching [F(1,18)=6.92, p=.017] and switching [F(1,18)=4.80, p=.042] trials and approached significance in the pure trial [F(1,18)=4.04, p=.059] post- as compared to pre-intervention. It also showed that the RE group exhibited significantly faster RTs in the non-switching [F(1,17)=13.99, p=.002] and switching [F(1,17)=6.66, p=.019] trials post- as compared to pre-intervention.
In terms of RT switching costs, the RM–ANOVA performed on the global switching cost revealed the main effects of Time [F(1,52)=6.12, p=.017, ηp2=0.11], with a smaller effect for post-
11
(633.25ms) as compared to pre-intervention (699.62ms). The interactions between Time × Group [F(2,52)=3.36, p=.043, ηp2=0.11] were also significant. The post-hoc analysis showed significant differences in global switching cost pre- and post-exercise in the AE (614.3ms vs. 731.7ms, p=.047) and RE (552.5ms vs. 666.5ms, p=.005) groups. However, no significant main effects for Group and Time or other significant interactions were obtained on the local switching cost.
Neurophysiological performance P2 latency
As shown in Figure 3, the RM–ANOVA performed on the P2 latency revealed the main effects of Trial [F(2,104)=5.96, p=.004, ηp2=0.10] and Electrode [F(2,104)=21.06, p<.001,
ηp2=0.29]. The post hoc analyses indicated that P2 latency was obtained significantly earlier in the pure trials (201.03ms) as compared to in the non-switching (209.65ms) and switching (210.91ms) trials and was significantly longer for the Pz electrode (215.65ms) than for the Fz (203.88ms) and Cz (202.06ms) electrodes. The interaction between Trial × Electrode [F(4,208)=2.92, p=.022, ηp2=0.05] was also significant. However, no significant main effects of Group and Time or other significant interactions were obtained.
P2 amplitude
The RM–ANOVA performed on the P2 amplitude revealed the main effects of Trial
[F(2,104)=7.96, p=.001, ηp2=0.13] and Electrode [F(2,104)=109.59, p<.001, ηp2=0.68]. The post hoc analyses indicated that the P2 amplitude was significantly larger in the pure trials (9.02μV) than in the non-switching (7.39μV) and switching (7.32μV) trials and was significantly smaller for the Pz electrode (5.51μV) than for the Fz (9.19μV) and Cz (9.03μV) electrodes. The interaction between Trial × Electrode [F(4,208)=6.17, p<.001, ηp2=0.11] was also significant. However, no significant main effects of Group and Time or other significant interactions were obtained.
P3 latency
The RM–ANOVA performed on the P3 latency revealed the main effect of Electrode [F(2,104)=5.71, p=.004, ηp2=0.10]. The post hoc analyses indicated that P3 latency was obtained significantly earlier for the Fz electrode (504.18ms) than for the Cz (521.08ms) and Pz (518.61ms) electrodes. The interaction between Trial × Electrode [F(4,208)=3.13, p=.016, ηp2=0.06] was also significant. However, no significant main effects of Group and Time or other significant
interactions were obtained.
P3 amplitude
RM-ANOVA performed on the P3 amplitudes showed the main effects of Time
[F(1,52)=11.22, p=.002, ηp2=0.18] and Trial [F(2,104)=15.88, p<.001, ηp2=0.23]. The post-hoc analysis indicated that the P3 amplitude was significantly larger post- (7.62μV) as compared to pre-exercise (6.27μV) and was significantly larger for the pure (9.03μV) electrode than for the non-switching (5.56μV) and switching (6.25μV) trials. The interactions of Time × Group
[F(2,52)=6.29, p=.004, ηp2=0.20], Time × Electrode [F(2,104)=10.35, p<.001, ηp2=0.17], Trial × Electrode [F(4,208)=21.39, p<.001, ηp2=0.29] and Time × Trial × Electrode [F(4,208)=5.76,
12
p<.001, ηp2=0.10] were also significant. The post-hoc analysis for the Time × Group interaction showed that the P3 amplitudes were significantly larger post- as compared to pre-exercise across trials and electrodes in the AE [F(1,18)=38.50, p<.001, ηp2=0.68) and RE [F(1.17)=7.62, p=.013, ηp2=0.31) groups.
Biochemical markers
There was a significant effect of Time × Group [F(2,52)=7.86, p=.001, ηp2=0.23) on insulin levels. The post-hoc analyses revealed that post- relative to pre-intervention, the serum insulin level decreased significantly in the AE group (p=.009), and there was an approaching significant decrease in the RE group (p=.055) and an approaching significant increase in the Control group (p=.060), while no significant main effects of Group and Time or other significant interactions were obtained on levels of leptin.
Neuroprotective growth factors
It can be clearly seen in Figure 4 that there was a significant effect of Time × Group [F(2,52)=3.28, p=.046, ηp2=0.11) on BDNF levels. The post-hoc analyses revealed that, post- relative to pre-intervention, the serum BDNF level increased significantly in the AE group (p=.016).
In addition, there was a significant effect of Time × Group [F(2,52)=3.19, p=.049, ηp2=0.11) on IGF- 1 levels. The post-hoc analyses revealed that, post- relative to pre-intervention, only the serum IGF- 1 level approached significance in the RE group (p=.052). There were no significant main effects of Group and Time or other significant interactions obtained on levels of VEGF and FGF-2.
Cytokines
There was a significant effect of Time × Group [F(2,52)=11.30, p<.001, ηp2=0.30) on TNF-α levels. The post-hoc analyses revealed that, post- relative to pre-intervention, the serum TNF-α level decreased significantly in the AE group (p=.004) and increased significantly in the Control group (p=.032), and there was an approaching significant decrease in the RE group (p=.052). In addition, there was a significant effect of Time × Group [F(2,52)=4.75, p=.013, ηp2=0.16) on IL-15 levels, and the post-hoc analyses revealed that, post- relative to pre-intervention, the serum IL-15 level decreased significantly in the AE (p=.013) and RE (p=.010) groups. However, no significant main effects of Group and Time or other significant interactions were obtained on the levels of IL- 1β, IL-6, and IL-8.
Correlation analysis
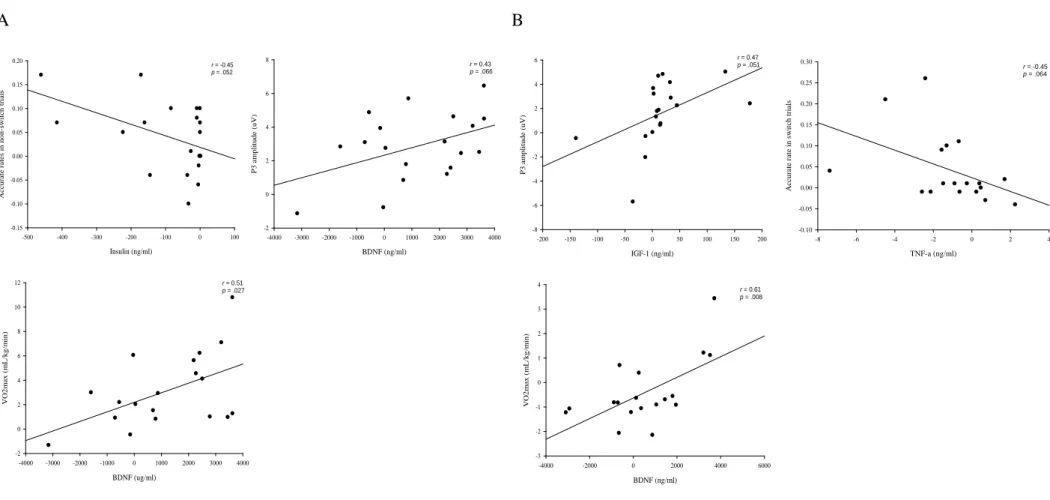
As shown in Figure 5, for the AE group, the correlations between changes in insulin levels and the ARs in the non-switching trials (r=-0.45, p=.052) and between changes in BDNF levels and P3 amplitudes (r=0.43, p=.066) prior to and after the intervention approached significance. For the RE group, the correlations between changes in IGF levels and P3 amplitudes (r=0.47, p=.051) and between changes in TNF-α levels and ARs in the switching trials (r=-0.45, p=.064) approached significance. In addition, the changes prior to and after intervention between BDNF levels and estimated VO2max were significantly correlated in both the AE (r=0.51, p=.027) and RE (r=0.61, p=.008) groups.
13
Discussion Main findings
The present study was aimed at investigating whether different exercise modes produce divergent effects on the neurocognitive performance related to executive function and circulating levels of biochemical markers in older adults with aMCI as well as on determining associations between changes in neurocognitive performance and peripheral levels of molecular biomarkers prior to and after an exercise intervention. The results showed that the 16-week aerobic exercise intervention significantly improved BMI, lower body strength, and cardiorespiratory fitness in older adults with aMCI; resistance exercise significantly enhanced muscular strength on the upper and lower limbs. The AE relative to the RE and control groups showed significantly higher
cardiorespiratory fitness after the 16-week exercise intervention. Both aerobic and resistance exercise were shown to effectively increase ARs across three trials, to facilitate RTs during the heterogeneous condition, and to decrease global switching cost when the participants performed the task switching paradigm. Although the ERP P2 components and P3 latency were not changed, P3 amplitudes were significantly increased after both exercise interventions. The serum BDNF level was significantly increased, and the levels of insulin, TNF-α, and IL-15 levels were
significantly decreased in the AE group, whereas the RE group showed significantly decreased IL- 15 levels, pointing at a distinct regulation of the molecular biomarkers by the two exercise modes.
Contrarily, the control group exhibited increased TNF-α levels after 16 weeks, indicating a progressive inflammatory state. Training-induced changes in serum molecular biomarkers tended to correlate with P3 amplitude and behavioral (i.e., AR) performance in both the AE and RE exercise groups, supporting their potential role as mediators of exercise benefits on the brain.
Neurocognitive parameters
Patients with aMCI typically demonstrate reduced perceptual/central as well as response- related neural processing when performing a cognitive task involving multiple components of executive control (e.g., task switching) [72]. Both aerobic and resistance exercise significantly improved ARs across trials, suggesting that these two exercise modes may successfully enhance executive control and task component processes related to encoding, stimulus evaluation, response selection, and response in individuals with aMCI. Aerobic and resistance training decreased RTs in the heterogeneous condition and reduced global switching costs, which are altered in individuals with aMCI [71,72], suggesting improved time efficiency related to the central processing of cognitive functions, especially with regard to the maintenance of potentially relevant task sets through the two exercise modes.
The neural networks involved in executive function are subject to age-related atrophy [99].
Older adults with MCI exhibit deficits in ERP P2 performance (e.g., prolonged P2 latency) as compared to healthy controls when performing a highly working memory demanding two-back task [100]. In the present study, physical exercise did not improve the P2 performance in the
14
individuals with aMCI when they were performing the task-switching paradigm, suggesting that cognitive control with regard to a shift in target modality and task-set activation is not affected via aerobic and resistance exercise interventions.
P3 latency, a potentially neuropathological characteristic of MCI, has been suggested to be a stable, sensitive biomarker that can be used to assess the cognitive functions of MCI patients and those who are transitioning from MCI to AD [101]. Tsai et al. [43] found that, as compared to the controls, elderly individuals with aMCI showed longer P3 latencies under both homogenous and heterogeneous conditions when performing the task-switching paradigm, suggesting decreased efficacy of perceptual and central processing time with regard to performing a cognitive task requiring frequent switching and updating of task sets. However, this problem seems not to be remedied via physical exercise. On the contrary, the P3 amplitude was significantly greater after 16-week aerobic and resistance exercise, demonstrating that neural activities involving task-set updating processes and attentional allocation to focal stimuli in the service of updating the working memory [102] can be facilitated via both exercise modes. Consistent with previous studies indicating that cognitive functions of patients with MCI could benefit from physical exercise aimed to improve cardiorespiratory fitness [41,63], the present study suggests that both aerobic and resistance exercise modes have the potential to enhance the plasticity of brain networks of MCI patients.
Biochemical parameters Neuroprotective markers
Circulating BDNF, IGF-1, VEGF, and FGF-2 are putative neuroprotective markers and mediators of exercise-induced benefits to brain function [7, 52, 103]. In the present study, even though we found significant improvements in cardiorespiratory (i.e., estimated VO2max) and muscular (i.e., the hand grip and chair stand tests) fitness after aerobic and resistance exercise interventions in patients with aMCI, we did not find changes in the levels of serum angiogenic factors (e.g., VEGF and FGF-2). However, the two exercise modes produced divergent changes in circulating neurotrophin levels, with increased serum BDNF levels in the AE group and a
tendency toward increased serum IGF-1 levels in the RE group.
BDNF plays an important role in neuronal survival, differentiation, and synaptic plasticity in the central nervous system (CNS) [104]. BDNF participates in memory, learning, and behavior and can mediate rapid dephosphorylation of tau protein [105]. Previous studies have demonstrated that BDNF levels are significantly reduced in the brains of MCI and AD patients [10, 12, 106].
Regular aerobic exercise has been shown to increase circulating BDNF levels in young and older adults [49, 53], and hippocampal BDNF was found to be increased in several animal studies in response to physical exercise [59, 107]. Furthermore, BDNF is rapidly transported in both directions across the blood-brain barrier (BBB) [108], which together with its regulation by
physical exercise makes it an ideal candidate as a mediator of exercise-induced benefits both at the level of the brain and the periphery. One RCT (randomized controlled trial) study of patients with
15
MCI found that plasma BDNF levels tended to increase in men and were significantly reduced in women following six months of high-intensity aerobic exercise [41]. Similar to our observations, Nascimento et al. [55, 94] found that a 16-week exercise intervention aimed to stimulate aerobic metabolism effectively increased serum BDNF in patients with MCI, independently of the BDNF genotype. However, resistance exercise did not elevate circulating BDNF levels in aMCI patients, which was in agreement with previous studies [109, 110].
By contrast, 16 weeks of resistance (but not aerobic) exercise tended to increase (p=.052) circulating IGF-1 levels in the current study. Administration of IGF-I has been shown to improve hippocampal neurogenesis and cognitive performance, as well as to reduce apoptosis in animal models of age- and AD-related brain pathologies/disturbances [111, 112]. Moreover, levels of IGF-1 have been found to correlate positively with hippocampal volume [48], while low serum IGF-1 has been linked to increased Aβ accumulation, and higher serum IGF-1 to increased clearance of brain Aβ [14, 15]. Serum IGF-I is thus linked to AD-related physiological and
pathological brain aging. Schiffer et al. [113] found that long-term aerobic and resistance exercise significantly decreased plasma IGF-1 in young healthy athletes. In the present study, serum IGF-1 increased after 16 weeks of resistance exercise as opposed to aerobic exercise in aMCI patients. In other studies, long-term aerobic exercise was also found to fail to elevate circulating IGF-1 in young women [114], as well as long-term resistance exercise elevated serum IGF-1 in both adults [115] and the elderly [45]. However, Baker et al. [41] also observed that plasma IGF-1 increased after 6 months of aerobic exercise in men, but this was not the case in women with MCI. These findings suggest that a longer aerobic exercise intervention might still increase IGF-1 levels. It is worth noting that blood-borne IGF-I could potentially affect BBB permeability to Aβ carrier proteins and further induce clearance of brain Aβ [14]. The present finding of elevated peripheral IGF-1 levels with resistance exercise in the older adults with aMCI suggested that such an
exercise mode could also be an effective alternative to reducing the progression of MCI/AD neuropathology.
Greater baseline VEGF has been associated with greater exercise-induced increases in temporal lobe functional brain connectivity [52] and angiogenic effects [116]. Some studies have observed an increase in circulating VEGF in older individuals in response to combined or aerobic exercise [117, 118]. However, the present study did not show increased serum VEGF levels in the patients with aMCI after the 16-week aerobic exercise intervention, which is consistent with earlier studies in sedentary healthy older adults [48, 52] and in older adults with
peripheral/coronary artery diseases [119, 120]. Likewise, compatible with Ogawa et al.’s findings [121], levels of VEGF were not significantly increased via 16 weeks of resistance exercise in patients with aMCI in the present study. Increases in the vulnerability of the aging hippocampus to different types of neuronal loss/damage have been suggested to be related to decreased FGF-2 levels [7]. FGF-2 has been proposed to contribute to exercise-induced hippocampal neurogenesis [103] and, in animal studies, short-term physical exercise has been shown to enhance cognitive
16
function and to regulate FGF-2 expression [46, 47]. However, a lack of exercise-induced increases in serum FGF-2 was found in the present study. Further exploration is required to determine how to effectively increase the two angiogenic molecules (e.g., VEGF and FGF-2) via physical exercise and/or to determine the mechanisms by which they mediate exercise-induced adaptive responses in the human brain.
Inflammatory/anti-inflammatory markers
The pro-inflammatory cytokine, TNF-α, disrupts brain-barrier properties [122] and participates in the inflammatory process linked to age- and neurodegeneration-associated brain impairment [33, 34]. In addition, TNF-α blocks IGF-I, affecting several target cells, including neurons, and antagonizes other actions of IGF-I in the brain [123]. TNF-α blocks IGF-I-induced passage of albumin through choroid plexus (CP) barriers and counteracts the effects of systemic IGF-I on transport and production of transthyretin by CP, resulting in blockage of the stimulatory effects of IGF-I on Aβ clearance [14]. Although Mendham et al. [124] found that aerobic exercise did not significantly reduce the levels of TNF-α in sedentary middle-aged men, pro-inflammatory cytokine levels increased in the control group and decreased as a result of aerobic and resistance (trend) exercise in the present study. This finding concurred with the findings of earlier studies investigating the effects of 16 weeks of aerobic exercise on TNF-α in MCI patients [55] and 12 weeks of resistance exercise in frail elderly individuals [125], suggesting that aerobic and resistance exercise may effectively suppress TNF-α in aMCI patients.
IL-1ß is up-regulated in AD brains [126], and higher serum IL-1β has been reported in patients with MCI [30, 31]. In the present study, 16 weeks of aerobic or resistance exercise did not decrease serum IL-1β in patients with aMCI. Compatible with earlier studies [124,127], aerobic exercise might not be an effective way to significantly reduce the levels of IL-1β. However, it was found to be significantly decreased after resistance exercise in college-age male subjects [127] and after a 12-month combined aerobic and resistance training intervention in middle-aged and elderly patients with type 2 diabetes [128]. This evidence seems to point to the potential effects of
resistance exercise on IL-1β, which is worth exploring in individuals with aMCI via longer exercise periods.
Skeletal muscle has the capacity to express and release IL-6, IL-8, and IL-15 [129,130] in response to muscle contractions [56]. IL-6 increases lipolysis/fatty acid oxidation and insulin- stimulated glucose disposal in elderly humans [131], and it can suppress TNF-α production [132]
as a part of an anti-inflammatory response to exercise. The cytokine/chemokine IL-8 acts as a potent angiogenic factor [133] that is potentially involved in exercise-induced angiogenesis [56].
Resting serum IL-6 and IL-8 did not change following the 16-week aerobic or resistance exercise intervention in aMCI individuals in the present study. Nevertheless, Nascimento et al. [55] found that a 16-week aerobic exercise intervention effectively reduced serum IL-6 in patients with MCI, with a positive impact on cognition assessed using the MoCA. It is worth noting that muscle contractions can induce production and release of IL-6, which may further inhibit TNF-α-induced
17
insulin resistance [139]. Importantly, decreased insulin levels were observed in the present study after the exercise intervention. Since insulin promotes tau protein phosphorylation [134], and reduced IL-6 levels benefit the cognitive functions in MCI [55], further research is still warranted in this area, possibly examining effective interventions to attenuate chronic subclinical
inflammation and insulin resistance in aMCI patients.
Different exercise modes may induce the expression and release of cytokines belonging to distinct families that specifically modulate adaptive responses to different types of exercise. IL-15 is expressed predominantly in type 2 muscle fibers and is regulated mostly by resistance exercise [56]. Ostrowski et al. [135] found that plasma IL-15 protein did not change in response to
prolonged treadmill running, whereas Riechman et al. [136] and Pérez-López et al. [137] reported increased plasma/serum IL-15 levels immediately after an acute resistance exercise. In the present study, serum IL-15 levels were significantly decreased after 16 weeks of not only resistance but also aerobic exercise interventions in the aMCI patients. Up to the present, conflicting evidence has existed on the effects of regular exercise on circulating IL-15 levels. However, in line with the present finding, Riechman et al. [136] also showed a similar trend of decreased plasma IL-15 levels after 30 sessions of resistance exercise in young adults, and Pérez-López et al. [138] found that baseline serum IL-15 was reduced in physically active middle-aged adults.
Inflammatory processes are thought to contribute to the pathogenesis of AD in the brain [11, 19, 27]. Although some pro-inflammatory cytokines levels at baseline could not be changed after AE or RE exercise in the present study, such exercised modes could reduce circulating levels of TNF-α and IL-15 in patients with aMCI. Since the onset of the neurodegenerative process is preceded by low-grade inflammation [20, 21], the present findings suggest that regular physical exercise may reduce inflammation phenomena associated with aMCI, which could protect the CNS against damage from long-term exposure to chronically elevated inflammatory cytokines [55, 139].
The marginal trends in correlations between the changes in specific neurotrophins (IGF-1, BDNF)/cytokines (TNF-α) and neurophysiological markers (P3 amplitudes, ARs in the switching trials) suggest that higher levels of peripheral neurotrophins and lower levels of specific
circulating inflammatory cytokines (e.g., TNF-α) regulated by exercise might be related to better neurocognitive performance in patients with aMCI. Previous studies have demonstrated IGF-1 levels to be inversely correlated with the degree of cognitive impairment [4, 140]. Maass et al.
[48] found that changes in IGF-I levels after a 3-month aerobic intervention were positively correlated with hippocampal volume changes and late verbal recall performance. Changes in IGF- 1 levels correlated with changes in RT and P3b amplitude in healthy older adults after 1 year of a resistance exercise intervention [50]. Cardiorespiratory fitness has been shown to be associated with better preservation of gray matter volumes among patients with AD [141, 142], and increased serum BDNF levels were associated with hippocampal volume in a 1-year RCT of exercise in seniors [96]. Similarly, physical exercise has been demonstrated to improve cognitive functions
18
and additionally provide a reduction in peripheral levels of inflammatory markers [59]. Coupled with these previous findings, the trends from the present study indicate that changes in
neurotrophins and inflammatory cytokines induced by regular aerobic or resistance exercise could be related to neurocognitive improvements in aMCI.
Limitations
The present study extends current knowledge regarding the distinct effects of aerobic and resistance exercise interventions on peripheral neuroprotective growth factors, inflammatory cytokines, and neurocognitive performance in individuals with aMCI. However, there are limitations that must be acknowledged. First, the changes in neurocognitive performance only showed a trend toward correlations with the exercise-induced changes in insulin, BDNF, IGF-1, and TNF-α (see Figure 5). This is perhaps due to the fact that we examined patients with aMCI at an early developmental stage of the neurodegenerative disease. Thus, these findings must be taken with caution, and further work is needed to determine their significance on a larger sample size with the higher range of metabolic and cognitive abnormalities. However, the data was presented in order to illustrate the complexity of exercise induced-changes at both biochemical and
neurocognitive levels. Second, since peripheral neuroprotective growth factors (e.g., BDNF, IGF- 1, and VEGF) and inflammatory cytokines are strongly associated with the regulation of amyloid- beta deposits [14, 33, 34], we measured these biomarkers as indirect parameters of
neurodegenerative processes. However, the effects of long-term exercise on the level of amyloid- beta, which is actually going on within the aMCI/AD brain, must be investigated via CSF sampling.
Conclusions
Currently, no curative treatment for dementia exists. Identifying early neuroprotective and anti-inflammatory biomarkers could be an important approach to the prevention and treatment of AD. Regular moderate exercise at midlife or even later in life may significantly reduce subsequent risks of MCI, thus significantly lower risk of dementia. The present study showed that both
aerobic and resistance exercise modes effectively benefit neurocognitive (e.g., behavior and ERP P3 amplitude) and inflammatory/anti-inflammatory (e.g., TNF-α and IL-15) biomarkers and that it produces divergent effects on neuroprotective biomarkers (e.g., BDNF and IGF-1). These findings support the role of regular physical exercise in prevention and treatment of age-related aMCI and dementia. Importantly, not only aerobic exercise, as most previous clinical studies have suggested, but also moderate intensity resistance exercise should not be overlooked as an important
therapeutic strategy across the age spectrum since it may attenuate age-related loss of synapses and neuropils via a direct influence on neurodegenerative disease mechanisms with distinct mediators and pathways, and thus may significantly reduce the risk of progression from aMCI to AD.
References
19
[1] Laske C, Stellos K, Hoffmann N, Stransky E, Straten G, Eschweiler GW, Leyhe T. Higher BDNF serum levels predict slower cognitive decline in Alzheimer’s disease patients. Int J Neuropsychopharmacol 14: 399-404 (2011).
[2] Yasutake C, Kuroda K, Yanagawa T, Okamura T, Yoneda H. Serum BDNF, TNF-alpha and IL- 1beta levels in dementia patients: comparison between Alzheimer’s disease and vascular dementia. Eur Arch Psychiatry Clin Neurosci 256: 402-406 (2006).
[3] Yu H, Zhang Z, Shi Y, Bai F, Xie C, Qian Y, et al. Association study of the decreased serum BDNF concentrations in amnestic mild cognitive impairment and theVal66Met polymorphism in Chinese Han J Clin Psychiatry 69: 1104-1111 (2008).
[4] Murialdo G, Barreca A, Nobili F, Rollero A, Timossi G, Gianelli MV, et al. Relationships between cortisol, dehydroepiandrosteronesulphate and insulin-like growth factor-I system in dementia. J Endocrinol Invest 24: 139-146 (2001).
[5] Solerte SB, Ferrari E, Cuzzoni G, Locatelli E, Giustina A, Zamboni M, et al. Decreased release of the angiogenic peptide vascular endothelial growth factor in Alzheimer's disease:
recovering effect with insulin and DHEA sulfate. Dement Geriatr Cogn Disord 19: 1-10 (2005).
[6] Drapeau E, Mayo W, Aurousseau C, Le Moal M, Piazza PV, Abrous DN. Spatial memory performances of aged rats in the water maze predict levels of hippocampal neurogenesis. Proc Natl Acad Sci USA 100:14385-14390 (2003).
[7] Shetty AK, Hattiangady B, Shetty GA. Stem/progenitor cell proliferation factors FGF-2, IGF- 1, and VEGF exhibit early decline during the course of aging in the hippocampus: role of astrocytes. Glia 51: 173-186 (2005).
[8] Connor B, Young D, Yan Q, Faull RL, Synek B, Dragunow M. Brain-derived neurotrophic factor is reduced in Alzheimer’s disease. Brain Res Mol Brain Res 49: 71-81 (1997).
[9] Garzon D, Yu G, Fahnestock M. A new brain-derived neurotrophic factor transcript and decrease in brain-derived neurotrophic factor transcripts 1, 2 and 3 in Alzheimer’s disease parietal cortex. J Neurochem 82: 1058-1064 (2002).
[10] Holsinger RM, Schnarr J, Henry P, Castelo VT, Fahnestock M. Quantitation of BDNF mRNA in human parietal cortex by competitive reverse transcription-polymerase chain reaction:
Decreased levels in Alzheimer’s disease. Brain Res Mol Brain Res 76: 347-354 (2000).
[11] Gezen-Ak D, Dursun E, Hanağası H, Bilgiç B, Lohman E, Araz ÖS, et al. BDNF, TNFα, HSP90, CFH, and IL-10 serum levels in patients with early or late onset Alzheimer's disease or mild cognitive impairment. J Alzheimers Dis 37:185-195 (2013).
[12] Peng S, Wuu J, Mufson EJ, Fahnestock M. Precursor form of brain-derived neurotrophic factor and mature brain-derived neurotrophic factor are decreased in the pre-clinical stages of Alzheimer’s disease. J Neurochem 93: 1412-1421 (2005).
[13] Shimada H, Makizako H, Doi T, Yoshida D, Tsutsumimoto K, Anan Y, et al. A large, cross- sectional observational study of serum BDNF, cognitive function, and mild cognitive
![Figure 4. Changes in serum levels (mean±SE) of neuroprotective growth factors [brain-derived neurotrophic factor (BDNF), insulin-like growth factor 1 (IGF-1), vascular endothelial growth factor (VEGF), fibroblast growth factor 2 (FGF-2)] and inflammatory](https://thumb-ap.123doks.com/thumbv2/9libinfo/9039439.325297/40.1262.78.1152.150.583/changes-neuroprotective-derived-neurotrophic-vascular-endothelial-fibroblast-inflammatory.webp)