行政院國家科學委員會補助專題研究計畫期中進度精簡報告
多巴胺系統在妥瑞症合倂過過動與注意力不集中症之研究
Studies of Dopaminergic System in Tourette Syndrome Comorbid Attention
Deficit Hyperactivity Disorder
計畫類別:■ 個別型計畫
□ 整合型計畫
計畫編號:NSC 97-2314-B-039-018-MY3
執行期間:
97 年 08 月 01 日至 100 年 07 月 31 日
計畫主持人: 周宜卿 主治醫師
共同主持人: 蔡長海 教授
蔡輔仁 教授
藍先元 教授
李采娟 副教授
計畫參與人員:
成果報告類型(依經費核定清單規定繳交):■精簡報告
□完整報告
本成果報告包括以下應繳交之附件:
□赴國外出差或研習心得報告一份
□赴大陸地區出差或研習心得報告一份
□出席國際學術會議心得報告及發表之論文各一份
□國際合作研究計畫國外研究報告書一份
處理方式:除產學合作研究計畫、提升產業技術及人才培育研究計畫、
列管計畫及下列情形者外,得立即公開查詢
□涉及專利或其他智慧財產權,□一年□二年後可公開查詢
執行單位:中國醫藥大學
中
華
民
國
9
8年
0
6月
16日
Content
I. Preface
In our previous studies, we used single nucleotide polymorphisms (SNPs) as markers to study the association between dopamine regulators and TS in Taiwanese children. A total of 160 Taiwanese children with TS and 83 normal control subjects were included. We have identified that dopamine receptor D2 gene polymorphisms are associated in Taiwanese children with TS (10), and the dopamine receptor D1 gene polymorphism are not associated (39). This is consistent with animal and human studies showing an important role of dopamine in rewarding TS.
However, we examined the noradrenergic genes (ADRA2A, ADRA2C) and found no association (40). We also reported that genetic screening in the Slit and Trklike1 gene for the recently
identified mutations does not appear to be of utility in the diagnosis of TS (41). Base on these experiences, we will focus on neurobiological data that link the genetic variants to biological models that reflect dysfunction in the dopamine systems.Second, TS and ADHD are highly co-morbidity, and the neurobiologic relationship between TS and ADHD is not yet clear. In our experience, most of the TS patients we have tested fall into ADHD, and since we have also examined multiple sets of controls, we feel that this wide range of individuals will allow us to examine the role of the dopaminergic candidate genes in pure TS, pure ADHD and TS comorbid ADHD. We hypothesis that TS and ADHD are variant expressions of a common set of
vulnerability genes, with one subtype of ADHD being a variant expression of the underlying vulnerability genes for TS. Both conditions evolve from disturbances in a shared neural substrate, such as dysfunction of the basal ganglia. Therefore, we subclass three diagnostic groups in this study exploring the dopaminergic genes of TS only, TS with comorbid ADHD, and ADHD. This approach includes clinical symptoms, neuroimaging studies, and treatment response to
methylphenidate. Results from the study will be crucial in elucidating the pathogenesis of this condition.
II. Research Aim
Tourette’s Syndrome (TS) and attention deficit hyperactivity disorder (ADHD) are now recognized as a common neurophychiatric disorder with a spectrum of neurological, behavioral, and cognitive features. We aim to characterize affected individuals in patients with ADHD and TS. The neuropsychological function and comorbid disorders and of TS will be examined. We will further use the Yale Global Tic Severity Scale to compare the severity of TS with the single nucleotidepolyphisms (SNPs) markers. Four models of alterations in the central neurotransmitters have been suggested as a cause of TS and ADHD.
III. Background and Rationale
Tourette Syndrome Cormobid Attention Deficit Hyperactivity Disorder
Tourette syndrome (TS) and attention deficit hyperactivity disorder (ADHD) are common neuropsychiatric disorders found in children, and they frequently co-occur in the same individual (1, 2). Tic disorders are characterized by bouts of brief, involuntary or semivoluntary movements and sounds. Tic disorders are classified as either transient (present for less than one year), chronic (motor or vocal tics lasting longer than one year), or as TS, in which the presence of chronic motor and vocal tics endure beyond one year. It occurs in 1-3% of school-age children (1).
Attention deficit hyperactivity disorder (ADHD) is characterized by hyperactivity,
inattention, and impulsivity. The DSM-IV classification of ADHD distinguishes three subtypes: predominantly hyperactive, predominantly inattentive, and combined type, in which both
hyperactive and inattentive symptoms are present. The majority of studies report prevalence rate of 3-6% within a school-aged population (2).
The diagnosis and effective treatment of ADHD in a child with TS can be critical to their academic, social and interpersonal functioning. The school performance of a child with TS may
be impaired by various combinations of contributing factor (2). In a recent study of social and emotional adjustment in 72 children with TS, tic severity and frequency was not associated with social, behavioral, or emotional functioning even after controlling for the effects of medication. However, ADHD diagnosis was found to be highly correlated with those outcomes (2).
Genetics of Tourette Syndrome and Attention Deficit Hyperactivity Disorder
In the 1970s, investigators first demonstrated that TS shows a familial concentration. Susceptibility to TS was then demonstrated to be transmitted vertically from generation to generation, and studies of twin pairs confirmed a genetic influence. In 1986, Pauls and Leckman used segregation analysis of affected families to indicate that TS is inherited in an autosomal dominant pattern, with variable expression that also includes chronic tic disorder and
obsessive-compulsive disorder (OCD). This information raised hopes that the application of linkage analysis techniques to ascertained pedigree would identify a genetic marker linked to the disease. To date, the gene search in TS has been unsuccessful (4) and is illustrative of the many factors that can complicate genetic analysis of complex human traits.
ADHD is also highly hereditary, and the familial and twin studies estimate heritability at 80%–90% (2). It is estimated that 50-75% of children with TS will have cormorbid ADHD (2). The high rate of comorbidity between ADHD and TS is hypothesized to involve shared
pathophysiology of basal ganglia circuitry (3).
Neurobiolog Issues in Tourette Syndrome
There is general consensus from pathophysiological studies that TS represents a disorder localized to a series of parallel frontal subcortical circuits that link specific regions of the frontal cortex to subcortical structures (5). Although a variety of neurotransmitters are localized within these circuits, the possibility of a dopaminergic abnormality in TS continues to receive strong consideration. Evidence supporting the dopamine hypothesis includes the therapeutic response to dopamine antagonists and results from a variety of postmortem studies and nuclear imaging protocols (6). Postulated changes in dopamine synaptic transmission include: (A) variable
increases in the number of receptors (7); (B) elevated levels of transporters (8); and (C) increased intrasynaptic release (9).
Progress in Gene Location in Tourette Syndrome and Attention Deficit Hyperactivity Disorder Base on these evidence, candidate genes investigated to date in TS belong primarily to the dopaminergic system. In our previous study, the dopamine receptor 2 gene (DRD2) TaqI
restriction site locus has shown a possible association with TS (10) Besides, the 7-repeat allele of the dopamine receptor 4 gene (DRD4) (11) have also shown an association with TS. Several investigators have examined patients with both TS and ADHD (TS+ADHD) and shown positive associations for polymorphisms within the DRD2, DRD4, dopamine beta-hydroxylase (DBH), and acid phosphatase 1 (ACP1) genes (13). For example, the TaqI polymorphism of DBH, the enzyme responsible for the conversion of dopamine to norepinephrine, has been associated with an additive effect on continuous ADHD scores in TS patients (13). In a study evaluating
TS+ADHD, the frequency of non A alleles of the ACP*1A polymorphism was significantly increased in TS+ADHD cases (12). In 2007, Singer et al has identified a significant association between the presence of TS and a dopamine transporter, DAT1 DdeI polymorphism (14).
Involvement of the dopaminergic system has been also suggested in patients suffering from ADHD since the symptoms can be successfully treated with methylphenidate, a potent blocker of the dopamine transporter (DAT). ADHD is a very promising area for pharmacogenetic studies. Among the 15 ADHD pharmacogenetic studies in the literature (15, 16), 10 investigations addressed the dopamine transporter gene (DAT1). In a previous study, an association between homozygosity for the 10-repeat allele at DAT1 and worse response to methylphenidate (MPH) in a sample of 50 European-Brazilian patients (17), replicating previous results from Winsberg and Comings (18). Recently, Cheon et al. (19) also replicated this association. However, several others found different results (20-24). Five studies addressed the association between the 48-bp
VNTR polymorphism at the D4 dopamine receptor (DRD4) and response to MPH (19, 21, 25-27) found that patients presenting the 7-repeat allele at DRD4 (DRD4*7) required higher doses for symptom improvement. Cheon et al. (19) reported that children who were homozygous for the 4-repeat allele at the DRD4 presented a better response to MPH.
Imaging in Attention Deficit Hyperactivity Disorder and Treatment Response
In recent years, investigators have begun to focus on the possible neurobiological factors involved in ADHD by evaluating the functional activity of the brain through the use of newly available imaging techniques. These studies have reported on either brain metabolism (28) or perfusion (29, 30). Recently, animal and human studies have been published on a newly
developed and one of the first technetium-labelled ligands for imaging the dopamine transporter, [99mTc]TRODAT-1 (31-37). In the previous study, [99mTc]TRODAT-1 was used to assess the status of the DAT in adults suffering from ADHD in the newly diagnosed, untreated condition and after commencement of treatment with methylphenidate (38). They found that the decrease in available DAT binding sites under treatment with methylphenidate correlates well with the
improvement in clinical symptoms. [99mTc]TRODAT-1 may help to elucidate the complex dysregulation of the dopaminergic neurotransmitter system in patients suffering from ADHD and the effect of treatment with psychoactive drugs.
VI. Instruments
SNAP-IV
The Swanson, Nolan, and Pelham scale—version IV (SNAP-IV)—the primary outcome measure—is a revision of the Swanson, Nolan, and Pelham (SNAP) Questionnaire (43). Its subscales provide scores for inattention, hyperactivity, and oppositional symptoms. The scale is completed by the subjects’ parents and teachers. The Taiwanese version of ADHD evaluation scale was standardized by Gau, et al (44). Secondary outcome measures include the Clinical Global Assessment (45) and the Barkley’s Stimulants Side Effects Rating Scale (SERS) to assess stimulants side events (46).
YGTSS
Yale Global Tic Severity Scale (YGTSS), a semi-structured interview with multiple informants, was designed to elicit information concerning the specific character and anatomical distribution of tics observed during the course of 1-week interval before the clinical assessment (47). With number, frequency, intensity, complexity and interference, examiners rate these characteristics for motor and phonic tics independently to generate a total tic score, an overall impairment rating, a global severity score and there is also a checklist for specific types for the tics.
CY-BOCS
The Children’s Yale-Brown Obsessive-Compulsive Scale (CY-BOCS) is a 10 item clinician-administered scale for Obsessive-Compulsive Disorder (OCD) that represents a total scale as well as two subscales (obsessions and compulsions). Both subscales are identically structured, with five items assessing frequency, distress, interference, resistance, and control over either obsessions or compulsions. Each item is rated from 0 to 4, with higher numbers indicating severity of symptoms (49)
CPT II
Conner’s Continuous Performance Test II (CPT II) is an attention test widely used in ADHD research and clinical testing. Examiner measures response times, errors, change in reaction time speed and consistency according to Signal Detection Theory. The standard version of the test is a non-X- type presented visually for 14 minutes. The participants need to respond by pressing the space bar every time a letter (target) appear on the computer screen, expect the letter X
V. Methods
Include Taiwanese children with Tourette’s syndrome and ADHD patients (group 1; TS=200, ADHD=200, ADHD comorbid TS=200) and normal control subjects (group 2; n=200). This study was approved by the Ethics Committee of the China Medical College Hospital, Taichung, Taiwan. All parents signed informed consent before blood tests were performed. Cases were matched with controls according to age, sex, ethnicity and geographic location of origin. Diagnosis of TS and ADHD followed the criteria of the Diagnostic and Statistical Manual of Mental Disorders, 4th edition (DSM-IV). The severity of TS will be measured by the YGTSS, to
compare the severity of TS with the SNP markers; the attention data of ADHD patients will be measured by CPT and SNAP-IV. All cases were from unrelated kindred. The controls were healthy volunteers with no history of psychiatric treatment (Figure I).
All children will undergo peripheral blood sampling for genotype analyses. Genomic DNA was isolated from peripheral blood by mean of a DNA extractor kit (Genomaker DNA extraction kit; Blossom, Taipei, Taiwan). A total of 50 ng of genomic DNA was mixed with 20 pmol of each polymerase chain reaction (PCR) primer in a total volume of 25 ul containing 10mM
Tris-hydrochloride, pH 8.3; 50mM potassium chloride; 2.0mM magenesium chloride; 0.2mM each deoxyribonucleotide triphosphate; and 1 U of DNA polymerase (Amplitaq; Perkin Elmer, Foster City, Calif., USA). PCR primers were used to amplify the correlated gene. The subjects of this research are not required to have follow-up program. Allelic frequencies were expressed as a percentage of the total number of alleles. Genotypes and allelic frequencies polymorphisms in both groups were compared.
VI. International Cooperation
In March 2009, the National Institute of Neurological Disorders and Stroke hold a “Tourette Syndrome GWAS Replication Workshop” in Bethesda, Maryland. In the conference, Prof. David Pauls mentioned a global project for collecting and genotyping the TS GWAS samples to replication. In table I, there are TS samples contributed by each site. The project that they applied to NIH is build on a long-standing program of research conducted by the Tourette Syndrome
Group I: Pure Tourette Group II: Pure ADHD Group III:ADHD + TS Group VI: Control YGTSS + CY-BOCS SNAP-IV+CPT YGTSS+CY-BOCS+SNAP-IV+CPT
SPECT All ADHD patients
[99mTc] TRODAT-1 for DAT
MPH (All ADHD patients for 8 weeks)
SPECT All ADHD patients
[99mTc] TRODAT-1 for DAT
SNAP-IV+CPT
Physical Examination Exclude participants withPsychiatric history.
Association International Consortium on Genetics (TSAICG) that was formed to help clarify the genetics of Gilles de la Tourette Syndrome (GTS). We attend the group to advance the genetic research and become one of a member of GTS GWAS replication steering committee.
All individuals who will be included in the current project have signed informed consent for their DNA to be used in the studies. De-identified DNA samples and phenotypic information will be sent to the coordinating site at the Psychiatric and Neurodevelopmental Genetic Unit in the Center of Human Genetic Research at Massachusetts General Hospital in Boston. This replication/extension project will incorporate a case-control design. We are looking forward to this development.
Table I: Expected number of subjects contributed by each site
Site Ethnicity/ ancestry # of TS samples
TSAICG US/Canadian 328 TSAICG French Canadian 73 TS GeneSEE (Hungary) Hungarian 66 TS GeneSEE (Poland) Polish 20 TS GeneSEE (Greece) Greek 16 TS GeneSEE (Italy) Italian 50
Utrecht Dutch 20
Vienna, Austria Austrian 107
Essen German 107
Hannover German 98
Taiwan Han Chinese 91 Tel Aviv Israeli Jewish 28
NYU US 35 Cincinatti US 92 Hopkins US 250 Rutgers US 30 Paris French 127 TOTAL 1538
VII. Discussion
We’ve gathered 93 patients with TS or ADHD comorbid TS in the last year, and the male/ female ratio is about 1:5. Still there are subjects needed to follow up, so in the 1st year of this
three-year project, we’ve searched and developed instruments to perfect the data we want to collect and analyze from participants.
1. The cueing paradigm:
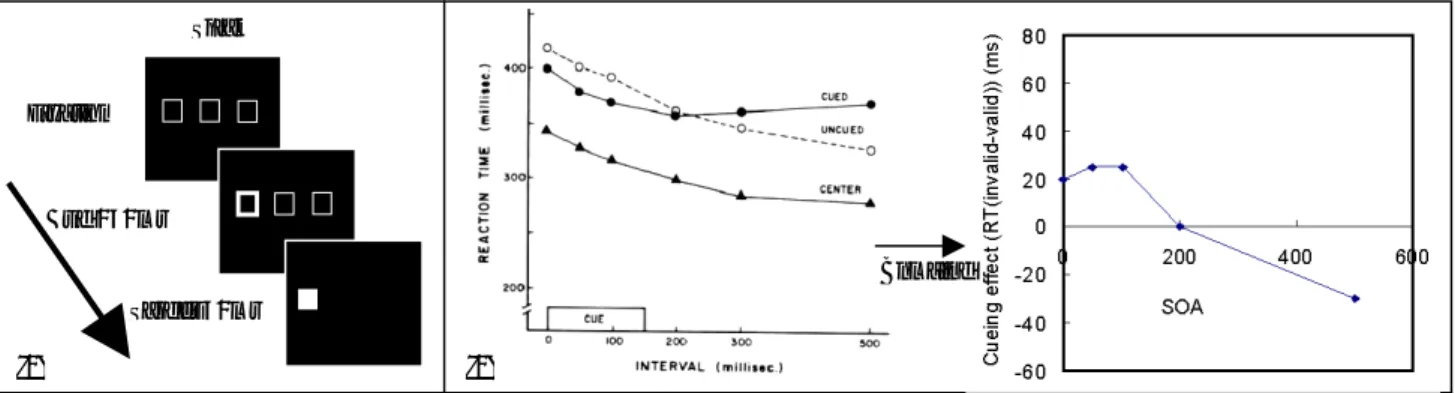
Thanks for Dr. Hsu, Li-Chuan and Dr. Tien, Yi-Min provide an incredible instrument- an idea- for ADHD patients to find out if they are different form normal people. Cohen and Posner (1984) had developed a paradigm for attention orientating (50). And other investigators (Bashinski & Bachrach, 1980; Jonides, 1981; Posner, 1980; Posner, Nissen, & Ogden, 1978) used central and peripheral cues to direct attention to various places in the visual fields and showed that even under the most austere conditions of empty visual fields and clear, bright stimuli, various dependent variables showed improved efficiency when subjects were cued to location of the event (51-54). The paradigm is (Figure II): Top panel is before a trial; subject fixates at central box; brightening of the outline of one peripheral box initiates a trial (middle panel); and a small but a bright target will appears in the center of one of the boxes to which a response is required.
According to results of Posner (1984)’s study, when SOA is 0, 50 and 100 ms, there is a Facilitation (curves of reaction time become lower) in this interval, means that when the time getting longer, participants will respond more correctly. But when SOA is between 300 to 500 ms, an Inhibition appears (the curves become higher); it means participants take more time to respond the target when SOA is getting longer in this field (Figure II).
The study is a 3*2*4 experimental design, 180 trials in total, manipulating the stimulus onset asynchrony (SOA) time (0, 50, 100 ms), cues (only appears at left or right side of the
three boxes) and targets (left, right, center and without targets). There are 15 ADHD patients and 13 control persons included. According to the results (figure III), there are two significances, “Valid” and SOA, in the normal group; for the accuracy, there is an interaction between SOA and “Valid” in ADHD group (figure VI). We may notice that in the normal group, even “valid” is significant, but the RT time seems the same at every different SOA. RT in ADHD group even shows no significant, but the “invalid” curve has the effect of Facilitation and both of “valid” and “invalid” curves shows the Inhibition. And even ADHD patients take more time to respond; there is a significant interaction for accuracy (0.62-0.80). For the research, we think probably the numbers of trails is not enough; the SOA time is not various, participants didn’t truly matched and most of all, sample is not big enough. So we’ll manipulate these variables for the further research to clarify the mechanism of attentional orienting on ADHD patients and develop the study to an effective assessment in clinic.
450 500 550 600 0 45 495 SOA R T invalid valid *Valid: 0.000 *SOA: 0.031 Valid*soa:0.067 Normal ADHD Valid: 0.269 SOA: 0.475 Valid*soa:0.688 Figure III. Validity of reaction time of Normal control group and ADHD patients.
0.8 0.85 0.9 0.95 1 1.05 1.1 1.15 1.2 0 45 495 SOA A C Y invalid valid Normal Valid:0.467 SOA: 0.440 Valid*soa:0.081 0.5 0.6 0.7 0.8 0.9 1 0 45 495 SOA A C Y invalid valid ADHD Valid:0.060 SOA: 0.496 *Valid*soa:0.018 Figure VI. Validity of accuracy of Normal control group and ADHD patients.
Trial Sequence Fixation 300ms Cue 150ms Target 50ms Ti m e
Figure II. Components of Visual Orienting: (1) study design; (2) valid curve is the cued curve and invalid curve is the un-cued one.
(Posner & cohen, 1984). Combine
2. Translating scales of YGTSS and CY-BOCS: We translate the scales to make the data collected more easier for the examiner. In further, we can form a Chinese-version tic severity scale to build a Taiwanese norm. CY-BOCS is an OCD assessment; we include this scale in the process to check if the participant is co-morbidity between OCD and TS. 3. Using the CPT to quantify the attention data: We use two instruments to assess the severity of ADHD patients. Use SNAP-IV to confirm the diagnosis at first and CPT to compare the difference from ADHD patients’ before and after medical therapy for ADHD.
VII. Self-assessment
First year of project
Subject Status Notification
YGTSS translation □Un finished □In processing ■Complete
CY-BOCS translation □Un finished ■In processing □Complete Will be completed in June, 2009 CPT sourcing □Un finished ■In processing □Complete Will be completed in June, 2009 The evaluation of attentional
orienting in patients with ADHD □Un finished ■In processing □Complete
The cueing system is replaced by CPT in this project, and for its further
research will keep going on by another project.
Case report form □Un finished ■In processing □Complete Will be completed in June, 2009 Participant-retrievals □Un finished ■In processing □Complete Will be completed in the 2nd year. International cooperation for TS □Un finished ■In processing □Complete For replicating the genetics of TS.
Reference
1. Kurlan R, ComoP, Miller B, et al. The behavioral spectrum of tic disorders: a community-based study. Neurol Clin 2002; 59:414-420
2. Carter A, O’Connell D, Schultz R, et al. Social and emotional adjustment in children affected with Gilles de la Tourette’s syndrome: associations with ADHD and family functioning. J Child Psychol Psychiatry 2000;41(2):215-223.
3. Mink J. Basal ganglia dysfunction in Tourette’s syndrome: a new hypothesis. Ped Neurol 2001; 25:190-198.
4. Paul DL. Update on the Genetics of Tourette syndrome. In: Cohen DJ, Goetz CG, Jankovic J, eds. Tourette Syndrome. Philadelphia: Lippincott Williams & Wklkins, 2001: 281-293.
5. Singer HS. Tourette’s syndrome: From behaviour to biology. Lancet Neurol 2005; 4(3):149–159.
6. Singer HS, Minzer K. Neurobiology of Tourette’s syndrome: Concepts of neuroanatomic localization and neurochemical abnormalities. Brain Dev 2003; 25 (Suppl. 1):S70–S84.
7. Wong DF, Singer HS, Brandt J, et al. D2-like dopamine receptor density in Tourette syndrome measured by PET. J Nucl Med 1997; 38(8):1243–1247.
8. Singer HS, Hahn IH, Moran TH. Abnormal dopamine uptake sites in postmortem striatum from patients with Tourette’s syndrome. Ann Neurol 1991;30(4):558–562.
9. Singer HS, Szymanski S, Giuliano J, et al. Elevated intrasynaptic dopamine release in Tourette’s syndrome measured by PET. Am J Psychiatry 2002;159(8):1329–1336.
10. Lee CC, Chou IC, Tsai CH, et al. Dopamine receptor D2 gene polymorphisms are associated in Taiwanese children with Tourette syndrome. Pediatr Neurol 2005;33(4):272–276.
11. Grice DE, Leckman JF, Pauls DL, et al. Linkage disequilibrium between an allele at the dopamine D4 receptor locus and Tourette syndrome, by the transmission-disequilibrium test. Am J Hum Genet 1996;59(3):644–652.
12. Bottini N, MacMurray J, Rostamkani M, et al. Association between the low molecular weight cytosolic acid phosphatase gene ACP1*A and comorbid features of Tourette syndrome. Neurosci Lett 2002;330(2):198–200.
genes (ADRA2a, ADRA2C, DBH) on attention-deficit hyperactivity disorder and learning disabilities in Tourette syndrome subjects. Clin Genet 1999;55(3):160–172.
14. Yoon DY. Dopaminergic polymorphisms in Tourette syndrome: association with the DAT gene (SLC6A3).Am J Hum Genet 2007;144B:605–610.
15. McGough JJ. Attention-Deficit/Hyperactivity Disorder pharmacogenomics. Biol Psychiatry 2005;57:1367–1373.
16. Polanczyk G, Zeni C, Genro JP, et al. Attention-deficit/hyperactivity disorder: Advancing on pharmacogenomics. Pharmacogenomics 2005;6:225–234.
17. Roman T, Szobot C, Martins S, et al. Dopamine transporter gene and response to methylphenidate in attention-deficit/hyperactivity disorder. Pharmacogenetics 2002;12:497–499.
18. Winsberg BG, Comings DE. Association of the dopamine transporter gene (DAT1) with poor methylphenidate response. J Am Acad Child Adolesc Psychiatry 1999; 38:1474–1477. 19. Cheon KA, Ryu YH, Kim JW, et al. The homozygosity for 10-repeat allele at dopamine
transporter gene and dopamine transporter density in Korean children with attention deficit hyperactivity disorder: Relating to treatment response to methylphenidate. Eur
Neuropsychopharmacol 2005;15:95–101.
20. Hamarman S, Ulger C, Fossella J, et al. Dopamine receptor 4 (DRD4) 7-repeat allele predicts methylphenidate dose response in children with attention deficit hyperactivity disorder:A pharmacogenetic study. J Child Adolesc Psychopharmacol 2004;14:564–574. 21. Kirley A, Lowe N, Hawi Z, et al. Association of the 480 bp DAT1 allele with
methylphenidate response in a sample of Irish children with ADHD. Am J Med Genet Part B
(Neuropsychiatr Genet) 2003;121B:50–54.
22. Lott DC, Kim SJ, Cook EH, et al. Dopamine transporter gene associated with diminished subjective response to amphetamine. Neuropsychopharmacology 2005;30:602–609 23. Stein MA, Waldman ID, Sarampote CS, et al. Dopamine transporter genotype and
methylphenidate dose response in children with ADHD. Neuropsychopharmacology 2005;30:1374–1382.
24. Van der Meulen EM, Bakker SC, Pauls DL, et al. High sibling correlation on
methylphenidate response but no association with DAT1-10R homozygosity in Dutch sibpairs with ADHD. J Child Psychol Psychiatry 2005;46:1074–1080
25. Winsberg BG, Comings DE. Association of the dopamine transporter gene (DAT1) with poor methylphenidate response. J Am Acad Child Adolesc Psychiatry 1999;38:1474–1477. 26. Ben Amor L, Grizenko N, Schwartz G, et al. 2004. Association between three
polymorphisms in the dopamine receptor D4(DRD4) gene and
Attention-Deficit/Hyperactivity Disorder (ADHD): A pharmacogenetic study. Abstracts for the XII World Congress of Psychiatric Genetics, Dublin, Ireland. p 92
27. Hamarman S, Ulger C, Fossella J, et al. Dopamine receptor 4 (DRD4) 7-repeat allele predicts methylphenidate dose response in children with attention deficit hyperactivity disorder:A pharmacogenetic study. J Child Adolesc Psychopharmacol 2004;14:564–574. 28. Zametkin AJ, Liebenauer LL, Fitzgerald GA, et al. Brain metabolism in teenagers with
attention-deficit hyperactivity disorder. Arch Gen Psychiatry 1993; 50: 333–340. 29. Amen DG, Carmichael BD. High-resolution brain SPECT imaging in ADHD. Ann Clin
Psychiatry 1997; 9: 81–86.
30. Sieg KG, Gaffney GR, Preston DF, et al. SPECT brain imaging abnormalities in attention deficit hyperactivity disorder. Clin Nucl Med 1995; 20: 55–60.
31. Ernst M, Zametkin AJ, Matochik JA, et al. High midbrain [18F]DOPA accumulation in children with attention deficit hyperactivity disorder. Am J Psychiatry 1999; 156: 1209–1215.
32. Ernst M, Zametkin AJ, Matochik JA, et al. DOPA decarboxylase activity in attention deficit hyperactivity disorder adults. A [fluorine-18] fluorodopa positron emission tomographic
study. J Neurosci 1998; 18: 5901–5907.
33. Pharmacological effects of dopaminergic drugs on in vivo binding of [99mTc]TRODAT-1 to the central dopamine transporters in rats. Eur J Nucl Med 1998; 25: 31–39.
34. Kung M-P, Stevenson DA, Plössl K, et al. [99mTc]TRODAT-1: a novel technetium-99m complex as a dopamine transporter imaging agent. Eur J Nucl Med 1997; 24: 372–380. 35. Kushner SA, McElgin WT, Kung M-P, et al. Kinetic modeling of [99mTc]TRODAT-1: a
novel compound for imaging the dopamine transporter. J Nucl Med 1999; 40: 150–158. 36. Mozley PD, Schneider JS, Acton PD, Barraclough ED, et al. Binding of [99mTc]
TRODAT-1 to dopamine transporters in patients with Parkinson’s disease and healthy volunteers. J
Nucl Med 2000; 41: 584–589.
37. Mozley PD, Acton PD, Barraclough ED, et al. Effects of age on dopamine transporters in healthy humans. J Nucl Med 1999; 40: 1812–1817.
38. Mozley P, Stubbs J, Plössl K, et al. Biodistribution and dosimetry of TRODAT-1: a technetium-99m tropane for imaging dopamine transporters. J Nucl Med 1998; 39: 2069–2076.
39. Chou I-C, Tsai C-H, Lee C-C, et al. Association analysis between Tourette’s syndrome and dopamine D1 receptor gene in Taiwanese children. Psychiatr Genet. 2004;14(4):219-21. 40. Chou IC, Tsai CH, Hsu YA, Lei W, Tsai FJ. Association Study Between Tourette’s
Syndrome and Polymorphisms of Noradrenergic Genes (ADRA2A, ADRA2C) Psychiatr
Genet 2007 accepted
41. Chou IC, Wan L, Liu SC, et al. Association of the SLITRK1 Gene in Taiwanese Patients with Tourette Syndrome. Pediatr Neurol. 2007 37(6):404-6.
42. Wang TM, Chang SY, Chang CG, Tsai CH, Shih C, Wang YH. Yunnan paiyao in established fractures: Therapeutic efficacy and possible mechanisms of action in rabbits.
Mid Taiwan J Med 2001;6(1):42-51
43. Tsai HY, Chu CL, Hsieh WT, Chen YF, Lee CC, Tsai CH. The Role of Nitric Oxide on EDTA-induced Vasoconstriction in isolated rabbit aorta. Mid Taiwan J Med 2001;6(1):22-9 44. Chen HY, Chen WC, Tsai HD, Hsu CD, Tsai FJ, Tsai CH. Relation of the estrogen receptor
α gene microsatellite polymorphism to bone mineral density and the susceptibility to
osteoporosis in postmenopausal Chinese Women in Taiwan. Maturitas 2001;40:143-50(SCI) 45. Chen HY, Tsai HD, Chen WC, Wu JY, Tsai FJ, Tsai CH. Relation of Polymorphism in the
Promotor Region for the Human Osteocalcin Gene to Bone Mineral Density and Occurrence of Osteoporosis in Postmenopausal Chinese Women in Taiwan. J of Clinical Laboratory
Analysis 2001;15:251-5(SCI)
46. Lin WD, Wu JY, Hsu HB, Tsai FJ, Lee CC, Tsai CH. Mutation Analysis of a Family with Hereditary Hemorrhagic Telangiectasia Associated with Hepatic Arteriovenous
Malformation. J Formos Med Assoc 2001;100(12):817-9(SCI)
47. James F. Leckman, Mark A. Riddle, Maureen T, Hardin, and et al. The Yale Blobal Tic Severity Scale: Initial Testing of a Clinician-Rated Scale of Tic Severity. J. Am. Acad. Child. Adolesc. Psychiatry, 1989, 28; 4: 566-573.
48. Renato Borgatti, Paolo Piccinelli, Rosario Montirosso, and et al. Study of Attentional Processed in Children With Idiopathic Epilepsy by Conners’ Continuous Performance Test.
J Child Neurol 2004; 19: 509-515.
49. Dean McKay, Scott Greisberg, John Piacentini, and et al. The Children’s Yale-Brown Obsessive-Compulsive Scale: Item Structure in an Outpatient Setting. Psychological Assessment 2003, 15(4): 578-581.
50. Posner M.I. & Cohen Y. (1984). Components of visual orienting. Chapter in Attention &
Performance X, (Bouma H. and Bouwhuis D., eds) pp 531-56, Erlbaum
51. Bashinki, H.S., & Bachrach, V. R. Enhancement of perceptual sensitivityy as the result of selectively attending to spatial locations. Perception and Psychophysis, 1980, 28, 241-248. 52. Junides, J. Voluntary versus automatic control over the mind’s eye. In J. Long & A.
Baddeley (Eds.), Attention and perforimance IX, Hillsdale, N. J.: Lawrence Erlbaum Associates, 1981.
53. Posner, M. I. Orienting of attention. The VIIth Sir Frederic Barlett Lecture, Quarterly
Journal of Experimental Psycholology, 1980, 32:3-25.
54. Posner, M.I., Nissen, M. J., and Ogde, W. C. Attend and unattended processing modes: The role of set for spatial location. In H. L. Pick & I.J. Saltzman (Eds.), Modes of perceiving and