行政院國家科學委員會專題研究計畫 成果報告
動情素與人類絨毛膜促性腺激素在調節血管內皮細胞生長
因子及其接受器基因表現的角色:對 OHSS 的重要性(3/3)
計畫類別: 個別型計畫 計畫編號: NSC91-2314-B-002-304- 執行期間: 91 年 08 月 01 日至 92 年 07 月 31 日 執行單位: 國立臺灣大學醫學院婦產科 計畫主持人: 陳欽德 報告類型: 完整報告 處理方式: 本計畫可公開查詢中 華 民 國 92 年 10 月 27 日
目 錄
頁次
中文摘要 II
英文摘要 III
報告內容
前言
1
研究目的 2
研究方法 3
結果
4
討論
6
結論
7
參考文獻 7
計畫成果自評 9
附錄
11
表格
18
中文摘要
關鍵詞:卵巢過度刺激症候群(0varian hyperstimulation syndrome, OHSS) 血管上皮生長因子(vascular endothelial growth factor, VEGF)
卵巢過度刺激症候群(OHSS)是刺激排卵所併發的後遺症。嚴重的 OHSS 會造成血壓下 降,電解質不平衡,肝腎功能受損,嚴重時甚至可能影響到病人的生命安全。致病機轉目 前尚不完全清楚,僅知卵巢和全身微血管通透性增加,造成大量腹水或胸水形成。
OHSS 都發生在胚胎植入後數天。人類絨毛膜促性腺激素(hCG) 是主要的誘因。血中 高濃度荷爾蒙也是原因之一。血管上皮生長因子(vascular endothelial growth factor, VEGF)
是一種很強的血管生成物,透過VEGF 專一接受器(KDR & flt-1),對血管上皮細胞有專一
的促進作用。血管增生的同時,血管通透性也隨之增加。
我們先前研究結果顯示OHSS 病患的胸腹水內 VEGF 濃度對臨床預後有極重要的指標
意義。而排卵前後至胚胎植入前的血清 IL-6,IL-8,TNF-α及 VEGF 濃度無法當作預測指
標。表示這些細胞動力素是以autocrine or paracrine 方式運作,不是以 endocrine 方式運作。
臨床上部份重度OHSS 是以胸部積水為唯一症狀,本身腹水很少。如果 VEGF 只來自卵巢
顆粒細胞(granulose cells),很難解釋這些以胸部積水來表現的 OHSS。覆蓋體腔的間質細胞 (mesothelial cells)以及其內的巨噬細胞(resident macrophage)即是很好的候選者。
假設VEGF 來源不限於卵巢顆粒細胞,那麼研究 OHSS 病患胸腹水內的間質細胞和巨
噬細胞VEGF 的基因調控情況將有助於瞭解 OHSS 病患以胸部積水為唯一症狀的機轉所在。
我們過去的研究,已經闡述細胞動力素在 OHSS 的角色。本次申請計畫,我們進一步
提出以下四種假說:
1. OHSS 病患胸腹水內的間質細胞以及巨噬細胞 VEGF mRNA 也發生過度表現,並且隨 著病程的改變而有所變化。
2. 上述細胞 VEGF mRNA 表現受到荷爾蒙(estradiol)及 hCG 的調控。
3. 我們假設 OHSS 病人,上述細胞比來自一般人的細胞更易受到刺激。也就是說排卵(取 卵)後,不同病人間上述細胞 VEGF mRNA 有不同表現。
4. 荷爾蒙和 hCG 增加微血管壁上 VEGF receptor (KDR and flt-1) mRNA 表現。 為了證實以上假說,我們提出本計畫以達成以下四點目標:
1. 以重覆胸腹水抽取治療 OHSS 病患,分析胸腹水內的間質細胞以及巨噬細胞 VEGF mRNA 表現的情形?OHSS 病程內不同時段抽取的變化又是如何?
2. 闡明荷爾蒙(estradiol)及 hCG 對上述細胞 VEGF mRNA 表現的調控情形。
3. 參與體外受精病患,上述細胞及卵巢顆粒細胞對荷爾蒙及 hCG 的刺激,其 VEGF mRNA 表現在不同病人間的差異性。
4. 闡明不同濃度及劑量的荷爾蒙及 hCG 對微血管壁上 VEGF receptor (KDR and flt-1) mRNA 表現的調控情形。
研究結果顯示腹水中的 VEGF 隨著病程的改善而逐漸下降,但是腹水細胞 VEGF mRNA 則無明 顯變化,顯示卵巢黃體化的顆粒細胞是腹水中 VEGF 的重要來源,並與預後有關。排卵前後 至胚胎植入前血清內 VEGF 無法預測卵巢過度刺激症候群的發生,但是來自卵泡數多的高危 險群的卵巢顆粒細胞受到動情素與人類絨毛膜促性腺激素刺激後,其VEGF 訊息核糖核酸 表現呈現劑量相關與時間相關,顯示刺激排卵的過程中,動情素與人類絨毛膜促性腺激素 為引發卵巢過度刺激症候群的重要物質,所產生的反應可能經由VEGF 媒介。卵巢過度刺 激症候群為從事人工生殖科技常見的併發症之一。研究可能致病機轉,提供預防卵巢過度 刺激症候群的臨床數據,可進一步提供臨床醫師對該病的認識,有助於預防及治療卵巢過 度刺激症候群,減少人工生殖科技的併發症,避免醫療源費。降低對卵巢的剌激並且設法 阻斷卵巢顆粒細胞產生大量 VEGF 是未來預防及治療卵巢過度刺激症候群需要努力的方向。
英文摘要
Keywords:ovarian hyperstimulation syndrome (OHSS), vascular endothelial growth factor (VEGF)
Ovarian hyperstimulation syndrome (OHSS) is a relatively common complication of ovarian stimulation and can be life threatening. In severe cases, a critical condition develops with massive ascites, marked ovarian enlargement, pleural effusion, electrolyte imbalance, and hypovolemia with hypotension and oliguria. The underlying mechanism responsible for the clinical manifestations of OHSS appears to be an increase in capillary permeability of the mesothelial surface with acute fluid shift out of the intravascular space.
OHSS always developed several days after embryo transfer. The increase in capillary permeability was thought to be mediated by a vasoactive substance(s) in response to human chorionic gonadotropin (hCG) administration. However, the exact factors responsible for this phenomenon are the subject of debate. Recent data imply a possible association between vascular endothelial growth factor (VEGF) and the evolution of OHSS. VEGF has been shown to play important roles in normal and pathological angiogensis. Angiogenesis always associated with the increase of vascular permeability.
Our previous study has shown that serial VEGF levels in ascites were inversely correlated with the clinical course of severe OHSS, suggesting that these cytokines may be involved in the resolution of OHSS, and therefore may also potentially serve as prognostic markers for this syndrome. However, measurements of serum VEGF from the day of HCG administration up to the day of embryo transfer are not predictive for this syndrome. This suggested that VEGF is worked as an autocrine or paracrine growth factor, but not as an endocrine manner. In addition, in some cases, they presented acute hydrothorax as the only symptom of OHSS. The exact pathogenesis of massive hydrothorax concurrently with minimal ascites remains a mystery. This raised a possibility that other cells, in addition to luteinized granulose cells, secreted VEGF. The mesothelial cells and the macrophages residented in peritoneal cavity and pleural space are the best candidates.
In our previous study, we have demonstrated the role of cytokines in the pathophysiology of OHSS. In this applied grant, we propose to test the following hypotheses:
1. In patients with severe OHSS, the mesothelial cells and the macrophages within peritoneal cavity and pleural space involved in the secretion of VEGF.
2. The expression of VEGF mRNA is regulated by the hormone (estradiol and hCG.)
3. We assume that difference do exist in the expression of VEGF mRNA in these cells between the high-risk patients and the normal control after ovulatory doses of hCG administration. 4. The hormone (estradiol and hCG) also involved in the regulation of the expression of VEGF in
human luteinized granulosa cells.
To test these hypotheses, we propose studies with the following aims:
1. To study the VEGF mRNA expression of resident cells in ascites and pleural effusion, which were obtained from repeated paracentesis or thoracentesis in the treatment of OHSS. We also study the time-course changes during the evolution of OHSS.
2. To determine in vitro effects of hormone and hCG on VEGF expression in these cells.
3. To determine the VEGF expression in cells from high-risk patients compared with cells from patients with normal ovarian response in our IVF program.
4. To study the in vitro effects of estradiol and hCG on the regulation of VEGF expression in human luteinized granulosa cells.
Serial VEGF concentrations in ascites were inversely correlated to the clinical course of OHSS. However, the expression of VEGF mRNA in the peritoneal macrophage did not change during the study period and was not different among the different severity of OHSS. This indicated that the ovary, but not peritoneal resident cells, may be the main source of VEGF in ascitis fluid in women with OHSS. Luteinized granulosa cells produce significant quantities of VEGF which is regulated directly by hCG. The degree of up-regulation of VEGF expression is dependent on the dose and type of gonadotropin employed, with hCG being the most effective in this regard. VEGF may represent a significant pathophysiological promoter for OHSS. It is hoped that awareness of the
pathophysiology of OHSS will soon provide opportunities to develop specific regimens for its treatment and prevention.
報告內容
1. 前言
The ovarian hyperstimulation syndrome (OHSS) comprises a series of iatrogenically induced complications which are relatively common and potentially life-threatening (Golan et al., 1989). It is associated with the use of exogenous gonadotropins to induce multiple ovulation in women undergoing different
therapeutic reproductive procedure. In severe cases, a critical condition develops with massive ascites, marked ovarian enlargement, pleural effusion, electrolyte imbalance, and hypovolemia with hypotension and oliguria (Golan et al., 1989). As the
indications for ovarian stimulation grow, so too will the absolute number of cases thus demanding an increased awareness of the possibility of this condition developing, and also knowledge of its prevention and treatment. The pathogenesis of OHSS remains poorly understood. There is a need for extensive studies of this important
iatrogenically induced complication.
The underlying mechanism responsible for the clinical manifestations of OHSS appears to be an increase in capillary permeability of the mesothelial surface with acute fluid shift out of the intravascular space (Haning et al., 1985; Polishuk & Schenker, 1969). It has been postulated that a vasoactive substance is released from the ovary in response to hormonal stimulation and causes increased vascular
permeability (McClure et al., 1994). Ovarian follicular fluid obtained from patients at risk for developing OHSS significantly augments in vitro permeability of endothelial cells (Goldsman et al., 1995).
The substance responsible for inducing the manifestations of this syndrome has not been conclusively identified. Recent data imply that VEGF is the follicular factor responsible for increased vascular permeability (McClure et al., 1994). This
glycoprotein was originally isolated as a vascular permeability factor (Senger et al., 1983) because it potently stimulates fluid transgression through endothelial cell tight junctions (Milton & Knutson, 1990). VEGF also is a mitogen for endothelial cells (Keck et al., 1989), contributing to neovascularization in the ischemic diabetic retina (Aiello et al., 1994) or tumor metastasis (de Vries et al., 1992; Kim et al., 1993; Millauer et al., 1994; Terman et al., 1992). VEGF is secreted by a variety of cells and binds to several transmembrane receptors expressed on endothelial cells, most
importantly Flt and KDR (or VEGFR-1 and –2) (de Vries et al., 1992; Terman et al., 1992). This growth factor is produced by normal and neoplastic human ovaries (Olson
et al., 1994), including ovarian granulose cells from women undergoing stimulation
for in vitro fertilization (IVF) (Yan et al., 1993).
In some cases of OHSS, they presented acute hydrothorax as the only clinical manifestation (Bassil et al., 1996; Hsieh et al., 1994; Jewelewicz & Vande Wiele, 1975; Kingsland et al., 1989; Man et al., 1997; Wood et al., 1998). The exact pathogenesis of massive hydrothorax concurrently with minimal ascites remains a mystery. The development hydrothorax may contribute by the increased pleural vascular permeability leading to the accumulation of fluid enriched in proteins, and to the recruitment of cells into the pleural space. Although pleural effusions are not uncommon in patients with severe OHSS, very little information is available on the inflammatory mechanisms that are involved in their development. As mention above that VEGF is worked as an autocrine or paracrine growth factor, but not in an
endocrine manner. For this reason, we postulate that other cells, in addition to ovarian granulose cells, secreted VEGF in response to the increased pleural and peritoneal vascular permeability. Candidates as the responsible cells include the resident cells of the peritoneal cavity and pleural space, the mesothelial cells and the macrophages
(Topley et al., 1996). To our knowledge, it has never been reported concerning the role of these cells in the regulation of VEGF expression in OHSS.
Peritoneal fluid bathes the peritoneal and ovarian surfaces. Elevated levels of VEGF are found in the peritoneal fluid of women with OHSS (Chen et al., 1999; Rizk
et al., 1997). VEGF is expressed by luteinized granulose cells (Doldi et al., 1997; Lee et al., 1997; Yan et al., 1998), but the major cellular constituents of peritoneal fluid
are macrophages, comprising between 82 and 99% of the total cell population (Eischen et al., 1994). These cells are involved in immune surveillance of the peritoneal cavity. They are also known to secrete a number of growth factors
including TNF-alpha, IL-1 beta, IL-1, IL-6 and INF-gamma, which may regulate the actions of leukocytes in the peritoneal fluid. The presence of mRNA encoding VEGF has been demonstrated in activated guinea pig peritoneal fluid macrophages (Shen et
al., 1993). However, the number and activation of these cells are not clear in OHSS.
Angiogenic effects of macrophages also have been isolated from ascitic fluid aspirated from women with ovarian cancer (Sheid, 1992).
OHSS always developed several days after embryo transfer (at early or late luteal phase), associated with elevated levels of serum estradiol and progesterone (Chen et
al., 1997). Because the administration of hCG is essential for the occurrence of the
syndrome (Neulen et al., 1995) and, we would thus postulate that under the action of hCG, the mesothelial cells and macrophage in peritoneal and pleural space, as well as ovarian granulosa cells, produce a large amount of VEGF that led to increased
vascular permeability. In-vitro studies examining these cells in culture following hCG and steroids stimulation would clarity our hypothesis. Moreover, if the overexpression of VEGF mRNA begins as early as in the embryo transfer period, these may be used to predict more specifically which patients will develop severe OHSS
In this applied grant, we propose to test the following hypotheses:
• In patients with severe OHSS, the mesothelial cells and the macrophage within peritoneal cavity and pleural space can express the mRNA of VEGF and its receptors.
• The expression of VEGF mRNA in these cells is up-regulated by the hormone (estradiol and hCG)..
• We assume that difference do exist in the expression of VEGF mRNA in these cells between the high-risk patients and the normal control after ovulatory dose of hCG administration
• The hormone (estradiol and hCG) also involved in the regulation of the expression of VEGF in human luteinized granulosa cells.
2. 研究目的
To test these hypotheses, we propose studies with the following Specific Aims: 1. To study the gene expression of VEGF and its receptors in the mesothelial cells
and macrophages in ascites and pleural effusion, which were obtained from repeated paracentesis or thoracentesis in the treatment of OHSS. We also study the time-course changes of the expression of VEGF and its receptors during the evolution of OHSS.
2. To determine in vitro effects of hormone and hCG on VEGF expression in these cells as well as in ovarian granulose cells.
3. To determine the VEGF expression in cells from high-risk patients in comparison with cells from patients with normal ovarian response in our IVF program. 4. To study the in vitro effects of estradiol and hCG on the regulation of VEGF
3. 研究方法 For specific aim 1
• To study the VEGF mRNA expression in mesothelial cells and macrophages in ascites and pleural effusion, which were obtained from repeated paracentesis or thoracentesis in the treatment of OHSS. We also study the time-course changes during the evolution of OHSS.
Subjects
We performed 266 IVF cycles between August, 2000 and May, 2001. Eleven women develop moderate to severe OHSS requiring hospitalization. Most patients present as massive ascites with or without pleural effusion. In all patients serial peripheral venous blood was drawn during the hospitalization. The blood was centrifuged and the supernatant was stored at -70°C before assay for cytokines and steroids. Five of 11 patients (45.4%) required either paracentesis (n = 5) or
thoracentesis (n = 1) or both (n = 1). Totally, 21 ascites samples and one pleural effusion sample were obtained. The diagnosis of severe OHSS was based on the classification proposed by Galon et al (1989). The use of paracentesis or thoracentesis was based on the clinical indications. We performed abdominal paracentesis for tense ascites and thoracentesis for massive pleural effusion. Ascites and pleural effusion samples were obtained from each abdominal paracentesis and thoracentesis
respectively. The samples were centrifuged for 10 minutes at 400 g and the cell-free supernatant was stored immediately at -70°C before cytokines assay. The cell pellet was re-suspended in medium for subsequent use.
VEGF production and VEGF expression in peritoneal (pleural) macrophages
Peritoneal (pleural) macrophages were isolated from ascites (pleural effusion) of OHSS patients after therapeutic abdominal paracentesis (throcentesis). Ascites
(pleural effusion) was kept at 4°C to prevent the adhesion of the macrophages to the plastic. After centrifugation at 200g for 10 minutes at 4°C, 105 cells per well were seeded on 96-well plates in their own ascitic fluid. After incubation for 90 minutes at 37°C in a humidified atmosphere (95% air and 5% CO2), the nonadherent cells were removed from the wells by three washed of 200µL of prewarmed Dulbecco’s
phosphate-buffered saline (DPBS), and the remaining adherent cells were incubated with phenol red-free RPMI 1640 medium (supplemented with 10% fetal calf serum, 2 mmol/L L-glutamine, 100 U/mL penicillin, and 100 mg/mL streptomycin). After 16 hours adherent cells were detached from the plastic with use of EDTA and seeded for the various experiments in tissue-culture round-bottom 5-mL tubes (Bibby, 1 x 106 cells/tube) in 1 mL of complete RPMI medium. The adherent cells were examined by flow cytometry analysis using macrophage-monocyte cell surface marker CD14. Viability was assessed by trypan blue exclusion. Total RNA was extracted from peritoneal macrophages by the RNA extraction kit. Reverse transcription of 1 µg total RNA was carried out. Relative quantification of VEGF mRNA will be performed on an ABI PRISM 7700 Sequence Detection System.
Serial concentration of VEGF in ascites in OHSS patients receiving repeated paracentesis or thracentesis
The serial concentration of VEGF will be determined with an enzyme-linked immunosorbent assay (ELISA) (Quantikine; R&D Systems, Minneapolis,MN). There are 56 serum samples and 22 ascites and pleural effusion samples are available for this assay.
For specific aim 2
To determine in vitro effects of hormone and hCG on VEGF expression in peritoneal resident cells, as well as in ovarian granulose cells in IVF patients at the time of oocyte retrieval and TET.
Total RNA was extracted from peritoneal resident cells and peritoneal
macrophages by the RNA extraction kit. Reverse transcription of 1 µg total RNA was carried out. Relative quantification of VEGF mRNA was performed on an ABI
PRISM 7700 Sequence Detection System. These data accompanied with data of serial concentrations of VEGF, estradiol, progesterone and hCG in plasma and ascites were analyzed. We collect plasma and body fluids from women with (1) severe OHSS required both pleurocentesis and paracentesis (n = 15), (2) severe OHSS only received paracentesis (n = 13) (3) severe OHSS received pleurocentesis (n = 7), (4 )Severe OHSS required hospitalization only ( n = 29), (5) control group with follicular fluid and plasma samples available ( n = 20). Assay of VEGF, estradiol, progesterone, and hCG to reveal the dynamic changes and to compare the differences between these groups. We also collected clinical data from coasting cases. These data are helpful for clinicians to prevent the development of OHSS.
For specific aim 3
• To determine the VEGF expression in cells from high-risk patients in comparison with cells from patients with normal ovarian response in our IVF program.
Time course and dose response of VEGF mRNA regulation by estradiol and hCG in human granulosa cells.
Luteinized granulosa cells and peritoneal macrophages were obtained from IVF patients (20 high responder patients and 20 low responder patients). Follicular fluids were centrifuged for 2 minutes at 50 x g. Pellets were repeatedly resuspended with phosphate-buffered saline (PBS) and centrifuged for 2 minutes to crudely eliminate contamination. Resulting pellets were incubated with 300 U/mL hyaluronidase for 10 minutes in PBS at 37℃. Cell clusters were separated by repeated aspiration through an Eppendorf blue-tipped pipette. Cell suspensions were then layered onto at 2.5 mL 50% Percoll and centrifuged for 10 minutes at 1,200 x g. Granulosa cells precipitated at the Percoll-PBS interphase were subsequently wash twice in PBS containing 1% (vol/vol) fetal calf serum and finally seeded in Falcon tissue culture dishes in Medium 199 supplemented with 1% fetal calf serum and 100 mg/L gentamycin 37℃, saturated humidity, and an atmosphere containing 5% CO2. Time course of VEGF mRNA regulation by estradiol and hCG in human geanulosa cells were treated with estradiol (1-10 ng/mL) or hCG (0.1-10 IU hCG/mL medium) or combined Estradiol and hCG, and total RNA was extracted from the cells at the indicated times (0, 1, 3, 5, 7 days). RNA was also extracted from control cells receiving vehicle but not estradiol or hCG.. Relative quantification of VEGF mRNA will be performed on an ABI PRISM 7700 Sequence Detection System. The conditioned media were removed and VEGF determined using a commercially available ELISA kit (R&D, Minneapolis, MN, USA).
4. 結果
VEGF production and VEGF expression in peritoneal macrophages
Serial VEGF concentrations in ascites were inversely correlated to the clinical course of OHSS. However, the expression of VEGF mRNA in the peritoneal macrophage did not change during the study period and was not different among the different severity of
OHSS. This indicated that the ovary, but not peritoneal resident cells, may be the main source of VEGF in ascitis fluid in women with OHSS.
Serial concentration of VEGF in ascites in OHSS patients receiving repeated paracentesis or thracentesis
Serial VEGF concentrations in ascites were inversely correlated to the clinical course of OHSS (VEGF: r = -0.351, P = 0.008). Changes of VEGF concentrations preceded improvement in clinical status. The distributions of various cytokine levels in pleural effusion were quite similar to those in ascites, although they were not correlated with the course of OHSS. The VEGF levels in pleural effusion were significantly lower than those in ascites and in control peritoneal fluid (P < 0.001). The results suggested that local cytokines may be involved in the resolution of severe OHSS.
Time course and dose response of VEGF mRNA regulation by estradiol and hCG in human granulosa cells
VEGF expression in granulosa cells was enhanced by increasing amounts of hCG. Amplification of VEGF expression by hCG was also shown to be time dependent. After three days of incubation with 10 IU hCG/mL medium, VEGF expression reached maximal values. More prolonged incubation (up to 7 days) did not result in further enhancement of VEGF mRNA expression. VEGF expression in granulosa cells with estradiol addition also showed similar pattern, although they did not reach significantly differences.
To compare the efficacy of coasting to prevent OHSS with intravenous albumin and to determine if different timing of gonadotropin coasting would affect the IVF outcomes.
The mean age (31.8 versus 32.2 years) and etiology of infertility did not differ between the coasting and the intravenous albumin groups. Although the mean number of oocytes retrieved was significantly higher in group 2 (21.3 ± 8.7 versus 24.6 ± 6.7; P = .009), fertilization rates (60.1% versus 57.1%, respectively) did not differ
significantly between the two groups. The mean number of embryos transferred was 5.0 ± 1.1 and 5.4 ± 0.9 in the coasting group and the intravenous albumin group,
respectively. The pregnancy rates per transfer was 35.5% in the coasting group versus 60.8% in the intravenous albumin group (P = .003). The implantation rate also was significantly lower in the coasting group (10.8% versus 16.6%, P = .047).
Five (9.8%) patients in the coasting group developed severe OHSS, where as 9 (9.3%) patients in the intravenous albumin group developed severe OHSS. Four (80%) of five patients with severe OHSS in the coasting group carried multiple pregnancies. Two required thoracocentesis and another two required repeated abdominal
paracentesis. The remaining non-pregnant woman with early-onset OHSS also required abdominal paracentesis. Eight (88.9%) of 9 patients with severe OHSS in the
intravenous albumin group conceived. Five (62.5%) of these eight pregnant patients carried multiple pregnancies. All patients with severe OHSS in the intravenous albumin group required repeated abdominal paracentesis. There was no significant difference in the rates of moderate OHSS between the two groups (19.6% in coasting group versus 15.5% in the intravenous albumin group).
The cycle characteristics between the early and late coasting subsets are shown in Table 2. The mean age (31.8 versus 31.8 years) and etiology of infertility did not differ between this two subsets. The days of coasting was significantly longer in the early coasting subset compared with the late coasting subset. The mean E2 level at start of coasting and the mean peak E2 values were significantly lower in the early coasting
subset compared with the late coasting subset. However, there were no significant differences between the two subsets in E2 on the day of hCG administration, total ampules of gonadotropin used, number of oocyte retrieved, fertilization rate, pregnancy and implantation rates. The incidence of moderate and severe OHSS did not differ statistically between the two subsets.
5. 討論
Our study has shown that serial VEGF levels in ascites were inversely correlated with the clinical course of severe OHSS, suggesting that these cytokines may be involved in the resolution of OHSS, and therefore may also potentially serve as prognostic markers for this syndrome. However, measurements of serum VEGF from the day of hCG administration up to the day of embryo transfer are not predictive for this syndrome. This suggested that VEGF is worked as an autocrine or paracrine growth factor, but not in an endocrine manner. The results suggested that local cytokines may be involved in the resolution of severe OHSS.
We postulate that the recovery of local capillary permeability and leakage of fluid from the ovaries may be responsible for the self-limiting of OHSS. The shutdown of capillary leakage from target tissues is reflected in the subsequent decrease of local angiogenic activators (e.g. VEGF). The progressive decrease of VEGF in ascites during the resolution of OHSS may indicate an attenuated stimulation of VEGF-producing cells and serial monitoring of these cytokine
concentrations may therefore have prognostic value. This suggests the ovary may be the main resource of mediators that work as the initiators of the changes and lead to the full appearance of OHSS.
Luteinized granulosa cells produce significant quantities of VEGF which is regulated directly by hCG. The degree of up-regulation of VEGF expression is dependent on the dose and type of gonadotropin employed, with hCG being the most effective in this regard. The positive effect of in-vitro exposure on VEGF expression after 7 days of culture is consistent with the exacerbation of the clinical course of OHSS in early pregnancy in response to circulating hCG. VEGF may represent a significant pathophysiological promoter for OHSS. It is hoped that awareness of the pathophysiology of OHSS will soon provide opportunities to develop specific regimens for its treatment and prevention.
When coasting was compared with intravenous albumin administration, no difference was found in the incidence of moderate and severe OHSS between the two groups, despite the fact that the pregnancy and implantation rates were significantly lower in the coasting group. Both coasting and intravenous albumin decrease the expected incidence of severe OHSS in these high-risk patients. Nevertheless, they do not completely prevent the development of OHSS.
It is of interest that significantly more oocytes were obtained among women in the intravenous albumin group, suggesting that some oocytes may be sacrificed during the coasting process. In addition, although the fertilization rates were not significantly different, the pregnancy and implantation rates were significantly lower in the
coasting group compared with the intravenous albumin group. These findings suggest that the oocytes quantity and embryo quality have been affected during the coasting process.
In the clinical situation of assisted reproduction, the three most important criteria are numbers of oocytes obtained after a course of ovarian stimulation, their
developmental competence, and the ability of implanted embryos to sustain viable fetal development. The proposed mechanism by which coasting may prevent OHSS
emphasizes that granulose cells and smaller follicles are more susceptible to gonadotropin withdrawal and atresia than are the developing oocytes, thereby reducing the risk of OHSS in this high-risk population. In a cow model, study has shown that the decreasing gonadotropin regimen allowed some follicles to enter atresia earlier, producing some oocytes and follicles at a more advanced stage of degeneration.
It has been assumed that only actively growing follicles would or could contain oocytes capable of supporting embryonic development following fertilization. Studies have shown that oocytes from follicles in early stage atresia is not necessarily
detrimental to oocytes and that early atretic follicles are more competent to support embryonic development in vitro than those from actively growing follicles. In one experiment designed to induce a form of early follicular atresia in vivo, animals were treated with exogenous gonadotropins followed by an abrupt cessation of treatment to reduce the follicle growth rate by gonadotropin starvation (coasting). Animals were coasted for 1, 2, or 3 days. Optimal oocyte developmental competence was achieved after 2 days of gonadotropin-free coasting.
The main concern of early coasting is that immature follicles may lack sufficient time and gonadotropin receptors to reach maturity during the coasting period.
Reduction of gonadotropin dose before coasting and prevent ‘prolonged coasting’ may be the keys to success in performing early coasting in patients with excessive ovarian follicular response. In conclusion, coasting is as effective as intravenous albumin in preventing OHSS in high-risk patients but yields inferior pregnancy rates. When compared with late coasting, start coasting before follicular maturation can be achieved successfully in reducing the incidence of OHSS with similar IVF outcome.
6. 結論
腹水中的 VEGF 隨著病程的改善而逐漸下降,但是腹水細胞 VEGF mRNA 則無
明顯變化,顯示卵巢黃體化的顆粒細胞是腹水中 VEGF 的重要來源,並與預後有 關。排卵前後至胚胎植入前血清內 VEGF 無法預測卵巢過度刺激症候群的發生, 但是來自卵泡數多的高危險群的卵巢顆粒細胞受到動情素與人類絨毛膜促性腺 激素刺激後,其VEGF 訊息核糖核酸表現呈現劑量相關與時間相關,顯示刺激排 卵的過程中,動情素與人類絨毛膜促性腺激素為引發卵巢過度刺激症候群的重要 物質,所產生的反應可能經由VEGF 媒介。降低對卵巢的剌激並且設法阻斷卵巢 顆粒細胞產生大量 VEGF 是未來預防及治療卵巢過度刺激症候群需要努力的方 向。 7. 參考文獻
Aiello, L.P., Avery, R.L., Arrigg, P.G., Keyt, B.A., Jampel, H.D., Shah, S.T., Pasquale, L.R., Thieme, H., Iwamoto, M.A., Park, J.E. & et al. (1994). Vascular endothelial growth factor in ocular fluid of patients with diabetic retinopathy and other retinal disorders [see comments]. N Engl J Med, 331, 1480-7.
Bassil, S., Da Costa, S., Toussaint-Demylle, D., Lambert, M., Gordts, S. & Donnez, J. (1996). A unilateral hydrothorax as the only manifestation of ovarian
hyperstimulation syndrome: a case report. Fertil Steril, 66, 1023-5.
Chen, C.D., Lu, H.F., Chen, H.F., Chen, S.U., Ho, H.N. & Yang, Y.S. (2000). Value of serum and follicular fluid cytokine profile in the prediction of moderate to severe ovarian hyperstimulation syndrome. Hum Reprod, 2000;15:1037-1042.
Chen, C.D., Wu, M.Y., Chao, K.H., Chen, S.U., Ho, H.N. & Yang, Y.S. (1997). Serum estradiol level and oocyte number in predicting severe ovarian hyperstimulation
syndrome. J Formos Med Assoc, 96, 829-34.
Chen, C.D., Wu, M.Y., Chen, H.F., Chen, S.U., Ho, H.N. & Yang, Y.S. (1999). Prognostic importance of serial cytokine changes in ascites and pleural effusion in women with severe ovarian hyperstimulation syndrome. Fertil Steril, 72, 286-92.
Chen CD, Chao KH, Yang JH, Chen SU, Ho HN, Yang YS. Comparison of coasting and intravenous albumin in the prevention of ovarian hyperstimulation syndrome. Fertil Steril 2003;80(1): 86-90.
de Vries, C., Escobedo, J.A., Ueno, H., Houck, K., Ferrara, N. & Williams, L.T. (1992). The fms-like tyrosine kinase, a receptor for vascular endothelial growth factor. Science, 255, 989-91.
Doldi, N., Bassan, M., Messa, A. & Ferrari, A. (1997). Expression of vascular
endothelial growth factor in human luteinizing granulosa cells and its correlation with the response to controlled ovarian hyperstimulation. Gynecol Endocrinol, 11, 263-7.
Eischen, A., Duclos, B., Schmitt-Goguel, M., Rouyer, N., Bergerat, J.P., Hummel, M., Oskam, R. & Oberling, F. (1994). Human resident peritoneal macrophages: phenotype and biology. Br J Haematol, 88, 712-22.
Golan, A., Ron-el, R., Herman, A., Soffer, Y., Weinraub, Z. & Caspi, E. (1989). Ovarian hyperstimulation syndrome: an update review. Obstet Gynecol Surv, 44, 430-40.
Goldsman, M.P., Pedram, A., Dominguez, C.E., Ciuffardi, I., Levin, E. & Asch, R.H. (1995). Increased capillary permeability induced by human follicular fluid: a hypothesis for an ovarian origin of the hyperstimulation syndrome [see comments]. Fertil Steril, 63, 268-72.
Haning, R.V., Jr., Strawn, E.Y. & Nolten, W.E. (1985). Pathophysiology of the ovarian hyperstimulation syndrome. Obstet Gynecol, 66, 220-4.
Hsieh, M.J., Tsao, T.C. & Cheng, P.J. (1994). Ovarian hyperstimulation syndrome with minimal ascites and massive pleural effusion: report of a case. J Formos
Med Assoc, 93, 882-4.
Jewelewicz, R. & Vande Wiele, R.L. (1975). Acute hydrothorax as the only symptom of ovarian hyperstimulation syndrome. Am J Obstet Gynecol, 121, 1121.
Keck, P.J., Hauser, S.D., Krivi, G., Sanzo, K., Warren, T., Feder, J. & Connolly, D.T. (1989). Vascular permeability factor, an endothelial cell mitogen related to PDGF.
Science, 246, 1309-12.
Kim, K.J., Li, B., Winer, J., Armanini, M., Gillett, N., Phillips, H.S. & Ferrara, N. (1993). Inhibition of vascular endothelial growth factor-induced angiogenesis suppresses tumour growth in vivo. Nature, 362, 841-4.
Kingsland, C.R., Collins, J.V., Rizk, B. & Mason, B.A. (1989). Ovarian
hyperstimulation presenting as acute hydrothorax after in vitro fertilization. Am J
Obstet Gynecol, 161, 381-2.
Lee, A., Christenson, L.K., Patton, P.E., Burry, K.A. & Stouffer, R.L. (1997). Vascular endothelial growth factor production by human luteinized granulosa cells in vitro.
Hum Reprod, 12, 2756-61.
Man, A., Schwarz, Y. & Greif, J. (1997). Pleural effusion as a presenting symptom of ovarian hyperstimulation syndrome. Eur Respir J, 10, 2425-6.
McClure, N., Healy, D.L., Rogers, P.A., Sullivan, J., Beaton, L., Haning, R.V., Jr., Connolly, D.T. & Robertson, D.M. (1994). Vascular endothelial growth factor as capillary permeability agent in ovarian hyperstimulation syndrome. Lancet, 344, 235-6.
Millauer, B., Shawver, L.K., Plate, K.H., Risau, W. & Ullrich, A. (1994).
Glioblastoma growth inhibited in vivo by a dominant-negative Flk-1 mutant.
Nature, 367, 576-9.
Milton, S.G. & Knutson, V.P. (1990). Comparison of the function of the tight junctions of endothelial cells and epithelial cells in regulating the movement of electrolytes and macromolecules across the cell monolayer. J Cell Physiol, 144, 498-504. Neulen, J., Yan, Z., Raczek, S., Weindel, K., Keck, C., Weich, H.A., Marme, D. &
Breckwoldt, M. (1995). Human chorionic gonadotropin-dependent expression of vascular endothelial growth factor/vascular permeability factor in human
granulosa cells: importance in ovarian hyperstimulation syndrome. J Clin
Endocrinol Metab, 80, 1967-71.
Olson, T.A., Mohanraj, D., Carson, L.F. & Ramakrishnan, S. (1994). Vascular permeability factor gene expression in normal and neoplastic human ovaries.
Cancer Res, 54, 276-80.
Polishuk, W.Z. & Schenker, J.G. (1969). Ovarian overstimulation syndrome. Fertil
Steril, 20, 443-50.
Rizk, B., Aboulghar, M., Smitz, J. & Ron-El, R. (1997). The role of vascular
endothelial growth factor and interleukins in the pathogenesis of severe ovarian hyperstimulation syndrome. Hum Reprod Update, 3, 255-66.
Senger, D.R., Galli, S.J., Dvorak, A.M., Perruzzi, C.A., Harvey, V.S. & Dvorak, H.F. (1983). Tumor cells secrete a vascular permeability factor that promotes
accumulation of ascites fluid. Science, 219, 983-5.
Sheid, B. (1992). Angiogenic effects of macrophages isolated from ascitic fluid aspirated from women with advanced ovarian cancer. Cancer Lett, 62, 153-8. Shen, H., Clauss, M., Ryan, J., Schmidt, A.M., Tijburg, P., Borden, L., Connolly, D.,
Stern, D. & Kao, J. (1993). Characterization of vascular permeability
factor/vascular endothelial growth factor receptors on mononuclear phagocytes.
Blood, 81, 2767-73.
Terman, B.I., Dougher-Vermazen, M., Carrion, M.E., Dimitrov, D., Armellino, D.C., Gospodarowicz, D. & Bohlen, P. (1992). Identification of the KDR tyrosine kinase as a receptor for vascular endothelial cell growth factor. Biochem Biophys
Res Commun, 187, 1579-86.
Topley, N., Mackenzie, R.K. & Williams, J.D. (1996). Macrophages and mesothelial cells in bacterial peritonitis. Immunobiology, 195, 563-73.
Wood, N., Edozien, L. & Lieberman, B. (1998). Symptomatic unilateral pleural effusion as a presentation of ovarian hyperstimulation syndrome [see comments].
Hum Reprod, 13, 571-2.
Yan, Z., Neulen, J., Raczek, S., Weich, H.A., Keck, C., Grunwald, K. & Breckwoldt, M. (1998). Vascular endothelial growth factor (VEGF)/vascular permeability factor (VPF) production by luteinized human granulosa cells in vitro; a paracrine signal in corpus luteum formation. Gynecol Endocrinol, 12, 149-53.
Yan, Z., Weich, H.A., Bernart, W., Breckwoldt, M. & Neulen, J. (1993). Vascular endothelial growth factor (VEGF) messenger ribonucleic acid (mRNA)
expression in luteinized human granulosa cells in vitro. J Clin Endocrinol Metab, 77, 1723-5.
計畫成果自評
研究內容除了荷爾蒙和hCG 對微血管壁上 VEGF receptor (KDR and flt-1) mRNA 表現的影響需要再研究外已經達成原始計畫擬達成目標。本研究發現腹
水中的 VEGF 隨著病程的改善而逐漸下降,但是腹水細胞 VEGF mRNA 則無明顯變 化,顯示卵巢黃體化的顆粒細胞是腹水中 VEGF 的重要來源,並與預後有關。排 卵前後至胚胎植入前血清內 VEGF 無法預測卵巢過度刺激症候群的發生,但是來 自高危險群的卵巢顆粒細胞受到動情素與人類絨毛膜促性腺激素刺激後 VEGF mRNA 的反應高於對照組,其VEGF 訊息核糖核酸表現呈現劑量相關與時間相關, 顯示動情素與人類絨毛膜促性腺激素為引發卵巢過度刺激症候群的重要物質,所 產生的反應可能經由VEGF 媒介。 卵巢過度刺激症候群為從事人工生殖科技常見的併發症之一。研究可能致病 機轉,提供預防卵巢過度刺激症候群的臨床數據,可進一步提供臨床醫師對該病 的認識,有助於預防及治療卵巢過度刺激症候群,減少人工生殖科技的併發症, 避免醫療源費。降低對卵巢的剌激並且設法阻斷卵巢顆粒細胞產生大量 VEGF 是 未來預防及治療卵巢過度刺激症候群需要努力的方向。部份研究成果已在學術期 刊發表如附錄。
附錄
Fertil Steril 2003; 80:86-90 (July, 2003)Comparison of coasting and intravenous albumin in the prevention
of ovarian hyperstimulation syndrome
Chin-Der Chen, M.D., Kuang-Han Chao, M.D., Jehn-Hsiahn Yang, M.D., Shee-Uan Chen, M.D., Hong-Nerng Ho, M.D., Yu-Shih Yang, MD, Ph.D.
Department of Obstetrics and Gynecology, National Taiwan University Hospital and National Taiwan University College of Medicine, Taipei, Taiwan
Financial support * Supported by grant NSC89-2314-B002-293
from the National Science Council of the Republic of China Reprint requests † Reprint requests: Yu-Shih Yang, M.D., Ph.D.
Department of Obstetrics and Gynecology, National Taiwan University Hospital, 7, Chung-Shan South Road, Taipei, Taiwan (FAX: + 886-2-2341-8557; e-mail: [email protected])
ABSTRACT
Objectives: To compare the efficacy of coasting to prevent ovarian
hyperstimulation syndrome (OHSS) with intravenous albumin and to determine if different timing of gonadotropin coasting would affect the IVF outcomes.
Design: Retrospective study.
Setting: University hospital-based IVF program.
Patients: 162 women undergoing IVF treatment cycles who were considered to be at high risk of developing OHSS.
Intervention: Gonadotropin administration was withheld in 60 patients, either coasting occurred before follicular maturation (early coasting subset, n = 28), or follicular maturity was attained before coasting (late coasting subset, n = 32). Outcomes were compared with 102 patients in risk of OHSS received intravenous albumin on the day of oocyte retrieval.
Main outcome measures: Incidence of OHSS and outcome parameters.
Results: Although the fertilization rates and the incidence of OHSS did not differ significantly between the coasting and intravenous albumin groups, the mean number of oocytes retrieved, the pregnancy rates, and implantation rates were significantly lower in the coasting group. There is no statistical difference in the entire outcome examined and the incidence of OHSS between the early and late coasting subsets. Conclusion: Coasting is as effective as intravenous albumin in preventing OHSS in high-risk patients but yields inferior pregnancy rates. Early coasting is as successful as late coasting in preventing OHSS with similar IVF outcome. (Fertil Steril
2003;80:86 –90. ©2003 by American Society for Reproductive Medicine.)
Key words: Albumin, coasting, IVF outcome, ovarian hyperstimulation syndrome
INTRODUCTION
Different strategies have been proposed for the prevention of OHSS in the high-risk patients, but these approaches do not offer complete protection against the development of OHSS. Among the selected preventive methods, discontinuing (coasting) gonadotropin therapy and intravenous albumin were by far the most
popular choices (1).
Coasting has been shown to reduce the risk for OHSS in high-risk conditions, such as rapidly increasing E2 levels or massive follicular recruitment (2).
Preovulatory oocytes appear to tolerate a deliberate reduction in markedly elevated E2 concentrations. However, little information exists regarding cycle management and outcome in coasting with immature follicles. In addition, the optimal coast timing and duration has yet to be determined.
Our previous work has shown that prophylactic intravenous albumin proved to be an effective strategy for preventing OHSS in high-risk patients. The use of prophylactic albumin, however, does not completely eliminate the risk of severe OHSS, especially when patients had high-order pregnancies (3).
Because of the substantial theoretic risk of OHSS among high responders, it may be difficult to continue generating control groups who receive no other interventions to minimize the development of severe OHSS. However, it would appear to be logical to initiate a comparison of coasting with other techniques designed to reduce the risk of OHSS. Benadiva et al. (4) retrospectively compared coasting with cryopreservation of all embryos whereas Tortoriello et al. (5) compared a group of highly responsive patients who chose between coasting and standard IVF-ET. To our knowledge, there is no study compared the efficacy of coasting with Intravenous albumin for the
prevention of OHSS.
The first objective of this study was to compare two methods of preventing OHSS: coasting and intravenous albumin administration at the time of oocyte retrieval, in an IVF program. The second objective was to determine if different timing of gonadotropin coasting would affect the IVF performances and outcomes.
MATERIALS AND METHODS
This is a retrospective study performed at the National Taiwan University Hospital from November 1997 through July 2001. Before June 1999, we used prophylactic intravenous albumin treatment as the main method to prevent OHSS in high-risk patients. Coasting was offered as an alternate method for the prevention of both cycle cancellation and OHSS since June 1999. The choice of preventive methods was based on physicians’ preference and patients’ willing. During this time frame, we did not have any changes in the clinical protocols.
All patients in this study underwent the long protocol of gonadotropin stimulation beginning with pituitary desensitization with intranasal buserelin (Supremon; Hoechst Laboratory, Frankfurt, Germany) (3). The luteal phase of the treatment cycles was supported with progesterone IM at a dosage of 50mg daily. We did not use hCG for luteal-phase support in patients at high risk of development of OHSS.
Coasting group (group 1)
Group 1 consisted of 60 women who underwent IVF or IVF with intracytoplasmic sperm injection (ICSI) cycles. In all cases, a rapid rise in E2 secretion was followed a deliberate reduction in the hMG dose to the prevention of OHSS. In order to define the optimal timing of coasting in patients at risk of developing OHSS, they were allocated into two subsets on the basis of follicular size and serum E2 levels at the time of initiation of coasting.
Early coasting subset (Group 1A)
Early coasting (n = 28) were defined as: (1) the presence of > 10 follicles per ovary with a leading follicle of < 14 mm; (2) gonadotropin administration was reduced/withhold before the cycle day 9 and (3) serum E2 level between 1,000 and
2,000 pg/mL. In group 1A, E2 concentrations rose rapidly in the presence of numerous intermediate-sized follicles. In anticipation of overstimulation, the hMG dosage was reduced for one to two day followed by withdraw for a total of 2 to 4 days. Gonadotropin treatment then was reinstituted to restimulate follicular growth (6). Once two or more follicles were ≥ 18 mm in mean diameter and the E2 level was ≥ 150 pg/mL per follicle, the ovulatory dose of hCG (10,000 IU) was administered and oocyte retrieval occurred 34 to 36 hours later. ICSI was used in patients with severe male factors, when indicated. Three to six embryos were replaced to maximize the pregnancy rates. There are three women who had no embryo transfer (elective cryopreservation of all embryos). Two women with fertilization failure (non-male factor) were excluded from statistic analysis.
Late coasting subset (Group 1B)
Late coasting (n = 32) were defined as: (1) the presence of > 10 follicles per ovary with a leading follicle of ≥ 15 mm; (2) gonadotropin administration was withhold after the cycle day 9 and (3) at this time, serum E2 level generally exceeded 3,000 pg/mL. Exogenous gonadotropins were withheld to allow E2 to decrease. Once two or more follicles were ≥ 18 mm in mean diameter, the ovulatory dose of hCG administration and oocyte retrieval were the same as described for group 1A. There are three women who had no embryo transfer (elective cryopreservation of all embryos).
One cycle was canceled in group 1B (3.1%) because of a significant drop in serum E2 level and was excluded from analysis. In this particular case, the serum E2 rapidly declines from 5,262 pg/ml to 1,722 pg/ml after discontinuing hMG for one day, and the serum E2 subsequently drops to 164 pg/mL, regardless of the restimulation with additional gonadotropins in the following two days.
Intravenous albumin group (Group 2)
Group 2 consisted of 102 infertile women who had serum E2 levels ≥ 3,600 pg/mL on the day of hCG administration and/or ≥ 20 oocytes retrieved. They were
considered at high risk for severe OHSS and were selected for Intravenous albumin treatment (3). The details of the ovarian stimulation protocol (long protocol) and the dosage of albumin given have been previously reported (3,7). There are five women who had no embryo transfer (elective cryopreservation of all embryos). All patients were seen 7 days after embryo transfer to determine if there was early clinical or ultrasound evidence of OHSS. OHSS was classified according to the classification proposed by Golan et al. (8).
Statistical Analysis
The data were analyzed with Student’s t-test, χ2 test, and Fisher’s exact test, as appropriate by using the Statistical Package for the Social Science (version 9.0; SPSS Inc., Chicago, Illinois). Statistical significance was defined as a value of P < .05.
Institutional review board approval was not obtained for this retrospective study because coasting and intravenous albumin administration have been the standard methods for managing overstimulated cycles in our center.
RESULTS
Table 1 details the data on IVF performances and outcomes between the coasting group (group 1) and the intravenous albumin group (group 2). The mean age (31.8 versus 32.2 years) and etiology of infertility did not differ between the coasting and the intravenous albumin groups. Although the mean number of oocytes retrieved was significantly higher in group 2 (21.3 ± 8.7 versus 24.6 ± 6.7; P = .009), fertilization rates (60.1% versus 57.1%, respectively) did not differ significantly between the two groups.
The mean number of embryos transferred was 5.0 ± 1.1 and 5.4 ± 0.9 in the coasting group and the intravenous albumin group, respectively. The pregnancy rates per transfer was 35.5% in the coasting group versus 60.8% in the intravenous albumin group (P = .003). The implantation rate also was significantly lower in the coasting group (10.8% versus 16.6%, P = .047).
Five (9.8%) patients in the coasting group developed severe OHSS, where as 9 (9.3%) patients in the intravenous albumin group developed severe OHSS. Four (80%) of five patients with severe OHSS in the coasting group carried multiple pregnancies. Two required thoracocentesis and another two required repeated abdominal paracentesis. The remaining non-pregnant woman with early-onset OHSS also required abdominal paracentesis. Eight (88.9%) of 9 patients with severe OHSS in the intravenous albumin group conceived. Five (62.5%) of these eight pregnant patients carried multiple pregnancies. All patients with severe OHSS in the intravenous albumin group required repeated abdominal paracentesis. There was no significant difference in the rates of moderate OHSS between the two groups (19.6% in coasting group versus 15.5% in the intravenous albumin group).
The cycle characteristics between the early and late coasting subsets are shown in Table 2. The mean age (31.8 versus 31.8 years) and etiology of infertility did not differ between this two subsets. The days of coasting was significantly longer in the early coasting subset compared with the late coasting subset. The mean E2 level at start of coasting and the mean peak E2 values were significantly lower in the early coasting subset compared with the late coasting subset. However, there were no significant differences between the two subsets in E2 on the day of hCG administration, total ampules of gonadotropin used, number of oocyte retrieved, fertilization rate, pregnancy and implantation rates. The incidence of moderate and severe OHSS did not differ statistically between the two subsets.
DISCUSSION
When coasting was compared with intravenous albumin administration, no difference was found in the incidence of moderate and severe OHSS between the two groups, despite the fact that the pregnancy and implantation rates were significantly lower in the coasting group. Both coasting and intravenous albumin decrease the expected incidence of severe OHSS in these high-risk patients (3). Nevertheless, they do not completely prevent the development of OHSS.
It is of interest that significantly more oocytes were obtained among women in the intravenous albumin group, suggesting that some oocytes may be sacrificed during the coasting process. In addition, although the fertilization rates were not significantly different, the pregnancy and implantation rates were significantly lower in the
coasting group compared with the intravenous albumin group. These findings suggest that the oocytes quantity and embryo quality have been affected during the coasting process.
In the clinical situation of assisted reproduction, the three most important criteria are numbers of oocytes obtained after a course of ovarian stimulation, their
developmental competence, and the ability of implanted embryos to sustain viable fetal development (9).
The proposed mechanism by which coasting may prevent OHSS emphasizes that granulose cells and smaller follicles are more susceptible to gonadotropin withdrawal and atresia than are the developing oocytes, thereby reducing the risk of OHSS in this high-risk population (10-12). In a cow model, study has shown that the decreasing gonadotropin regimen allowed some follicles to enter atresia earlier, producing some
oocytes and follicles at a more advanced stage of degeneration (13).
It has been assumed that only actively growing follicles would or could contain oocytes capable of supporting embryonic development following fertilization. Studies have shown that oocytes from follicles in early stage atresia is not necessarily
detrimental to oocytes and that early atretic follicles are more competent to support embryonic development in vitro than those from actively growing follicles (14,15). In one experiment designed to induce a form of early follicular atresia in vivo, animals were treated with exogenous gonadotropins followed by an abrupt cessation of treatment to reduce the follicle growth rate by gonadotropin starvation (coasting). Animals were coasted for 1, 2, or 3 days. Optimal oocyte developmental competence was achieved after 2 days of gonadotropin-free coasting (16).
The second objective of this study was to determine if different timing of
gonadotropin coasting would affect the IVF performances and outcomes. The present study shows that the mean E2 levels at initiation of coasting in early coasting and late coasting subsets were 2,010 and 3,753 pg/dL respectively (P < .001). As reported in most of the published data (6,17-21), the levels of serum E2 at onset of coasting varying from 3,000 to 6,000 pg/mL and the duration has ranged from 1 to 11 days.
Excessively high serum E2 levels prolong the duration of coasting to allow the serum E2 levels to fall. Although high estrogen levels are associated with OHSS, it is unlikely that they are causally involved in its development. Hence, reduction of E2 levels in itself is not the main goal of coasting (22).
Recent clinical evidence suggests that cycle outcome may be impaired with more prolonged coasting periods. Ulug et al. (23) reported that patients in whom coasting lasted ≥4 days had significantly reduced implantation (10.5%) and pregnancy (26.7%) rates compared with patients with a shorter coasting interval (range 18.4-27.9 and 41-55.7% respectively, P <.05), whilst oocyte and embryo qualities do not appear to be affected. Tortoriello et al. (24) also suggested that the coasting interval may affect IVF outcome. In their subset of patients with a mean interval of 2.6 coasting days they found a 19% implantation rate, while in those with 3.5 coasting days it was only 6.7%.
The mean leading follicular diameters at initiation of coasting in early and late coasting subsets were 12.8 mm and 17.0 mm respectively (P <.001). As reported previously, the size of leading follicle at onset of coasting varying from 16 to 18 mm (6,25-29). It had been suggested that follicular diameter of 15 mm was probably the critical follicular size prerequisite for LH surge in spontaneous ovulatory cycles (30). Previous study has shown that quick, dramatic reductions in medications or coasting before follicle development of approximately 14 mm in diameter portends very poor oocyte retrieval results (31).
It is likely that when follicles reach a threshold size (approximately 15 mm), they can continue to grow for an interval without gonadotropin support. Nevertheless, the lower number of oocytes obtained in early coasting subset when compared with late coasting subset suggests that smaller follicles may undergo maturation arrest and/or atresia following gonadotropin withdrawal. The fertilization rates, however, appears not to be affected, as indicated by similar fertilization rates in both groups. It is of note that both fertilization failures (non-male factor) are within the early coasting subset. This may be a reflection of oocyte problems associated with coasting.
Egbase et al. (32) reports that withheld early at leading follicle of 15 mm and serum E2 levels of >1,500 rather than >3,000 pg/mL with leading follicle ≥18 mm is consistent with good embryological and clinical outcome in IVF cycles. Our report shows that early coasting at leading follicle of 14 mm and serum E2 levels between
1,000 and 2,000 pg/mL did not adversely affect cycle outcome parameters or the incidence of OHSS.
The main concern of early coasting is that immature follicles may lack sufficient time and gonadotropin receptors to reach maturity during the coasting period (6). Reduction of gonadotropin dose before coasting (33) and prevent ‘prolonged coasting’ (34) may be the keys to success in performing early coasting in patients with
excessive ovarian follicular response. The efficacy of early coasting in preventing OHSS still awaits evaluation in a well designed prospective trial.
In conclusion, coasting is as effective as intravenous albumin in preventing OHSS in high-risk patients but yields inferior pregnancy rates. When compared with late coasting, start coasting before follicular maturation can be achieved successfully in reducing the incidence of OHSS with similar IVF outcome.
REFERENCES
1. Delvigne A, Rozenberg S. Preventive attitude of physicians to avoid OHSS in IVF patients. Hum Reprod 2001;16:2491-5.
2. Urman B, Pride SM, Yuen BH. Management of overstimulated gonadotrophin cycles with a controlled drift period. Hum Reprod 1992;7:213-7.
3. Chen CD, Wu MY, Yang JH, Chen SU, Ho HN, Yang YS. Intravenous albumin does not prevent the development of severe ovarian hyperstimulation
syndrome. Fertil Steril 1997;68:287-91.
4. Benadiva CA, Davis O, Kligman I, Moomjy M, Liu HC, Rosenwaks Z. Withholding gonadotropin administration is an effective alternative for the prevention of ovarian hyperstimulation syndrome. Fertil Steril 1997;67:724-7. 5. Tortoriello DV, McGovern PG, Colon JM, Skurnick JH, Lipetz K, Santoro N.
"Coasting" does not adversely affect cycle outcome in a subset of highly responsive in vitro fertilization patients. Fertil Steril 1998;69:454-60.
6. Fluker MR, Hooper WM, Yuzpe AA. Withholding gonadotropins ("coasting") to minimize the risk of ovarian hyperstimulation during superovulation and in vitro fertilization-embryo transfer cycles. Fertil Steril 1999;71:294-301. 7. Chen CD, Wu MY, Chen HF, Chen SU, Ho HN, Yang YS. Prognostic
importance of serial cytokine changes in ascites and pleural effusion in women with severe ovarian hyperstimulation syndrome. Fertil Steril 1999;72:286-92. 8. Golan A, Ron-el R, Herman A, Soffer Y, Weinraub Z, Caspi E. Ovarian
hyperstimulation syndrome: an update review. Obstet Gynecol Surv 1989;44:430-40.
9. Fleming R, Rehka P, Deshpande N, Jamieson ME, Yates RW, Lyall H. Suppression of LH during ovarian stimulation: effects differ in cycles stimulated with purified urinary FSH and recombinant FSH. Hum Reprod 2000;15:1440-5.
10. Fluker MR, Marshall LA, Monroe SE, Jaffe RB. Variable ovarian response to gonadotropin-releasing hormone antagonist-induced gonadotropin deprivation during different phases of the menstrual cycle. J Clin Endocrinol Metab 1991;72:912-9.
11. Sher G, Zouves C, Feinman M, Maassarani G. 'Prolonged coasting': an
effective method for preventing severe ovarian hyperstimulation syndrome in patients undergoing in-vitro fertilization. Hum Reprod 1995;10:3107-9. 12. Sirard MA, Picard L, Dery M, Coenen K, Blondin P. The time interval
between FSH administration and ovarian aspiration influences the development of cattle oocytes. Theriogenology 1999;51:699-708.
13. Blondin P, Sirard MA. Oocyte and follicular morphology as determining characteristics for developmental competence in bovine oocytes. Mol Reprod Dev 1995;41:54-62.
14. Salamone DF, Adams GP, Mapletoft RJ. Changes in the cumulus-oocyte complex of subordinate follicles relative to follicular wave status in cattle. Theriogenology 1999;52:549-61.
15. Blondin P, Guilbault LA, Sirard M-A. The time interval between FSH-P administration and slaughter can influence the developmental competence of beef heifer oocytes. Theriogenology 1997;48:803-13.
16. Lee C, Tummon I, Martin J, Nisker J, Power S, Tekpetey F. Does withholding gonadotrophin administration prevent severe ovarian hyperstimulation
syndrome? Hum Reprod 1998;13:1157-8.
17. Sher G, Salem R, Feinman M, Dodge S, Zouves C, Knutzen V. Eliminating the risk of life-endangering complications following overstimulation with
menotropin fertility agents: a report on women undergoing in vitro fertilization and embryo transfer. Obstet Gynecol 1993;81:1009-11.
18. Dhont M, Van der SF, De Sutter P. Prevention of severe ovarian hyperstimulation by coasting. Fertil Steril 1998;70:847-50.
19. Ulug U, Bahceci M, Erden HF, Shalev E, Ben-Shlomo I. The significance of coasting duration during ovarian stimulation for conception in assisted fertilization cycles. Hum Reprod 2002;17:310-3.
20. Cahill DJ, Wardle PG, Harlow CR, Hull MG. Onset of the preovulatory luteinizing hormone surge: diurnal timing and critical follicular prerequisites. Fertil Steril 1998;70:56-9.
21. Whelan JG, III, Vlahos NF. The ovarian hyperstimulation syndrome. Fertil Steril 2000;73:883-96.
22. Egbase PE, Al Sharhan M, Grudzinskas JG. 'Early coasting' in patients with polycystic ovarian syndrome is consistent with good clinical outcome. Hum Reprod 2002;17:1212-6.
23. Aboulghar MA, Mansour RT, Serour GI, Rhodes CA, Amin YM. Reduction of human menopausal gonadotropin dose before coasting prevents severe ovarian hyperstimulation syndrome with minimal cycle cancellation. J Assist Reprod Genet 2000;17:298-301.
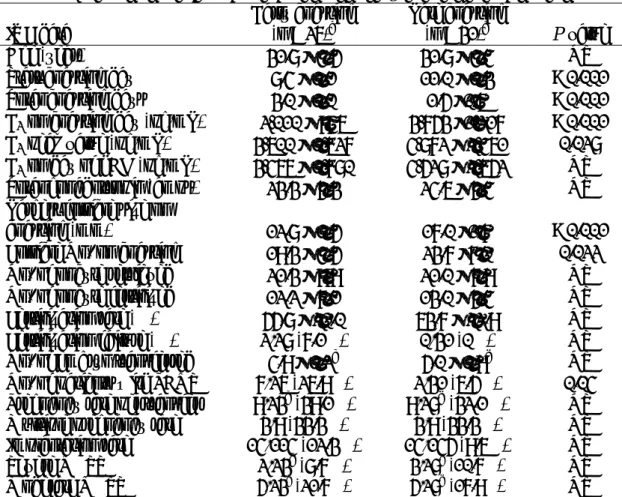
Talbe 1 IVF performances and outcomes between coasting and intravenous albumin groups.
IVF data Coasting group (n = 57)a Albumin group (n = 102) value P
Age (year) 31.8 ± 4.3 32.2 ± 4.0 NS
Total gonadotropin (amps) 23.9 ± 5.3 28.9 ± 7.0 < 0.001 E2 on day of hCG (pg/mL) 4,054 ± 2,345 3,831 ± 1,364 NS No. of oocyte retrieved 21.3 ± 8.7 24.6 ± 6.7 0.009 No. of oocyte fertilized 12.6 ± 6.2 13.8 ± 4.6 NS Fertilization rate (%) 60.1 ± 21.9 57.1 ± 14.3 NS Fertilization failure (%) 2/59 (3.4%) 0/102 (0%) NS No. of embryo transferred 5.0 ± 1.1b 5.4 ± 0.9c 0.007 No. of patients with PCOS 9/57 (15.8%) 23/102 (22.5%) NS Pregnancy rate per transfer 18/51b (35.3%) 59/97c (60.8%) 0.003 Pregnancy rate per retrieval 18/53b (34.0%) 59/97c (60.8%) 0.002 Multiple pregnancy rate 6/18 (33.3%) 23/59 (39.0%) NS Implantation rate 28/259 (10.8%) 86/535 (16.1%) 0.047
Severe OHSS 5/51b (9.8%) 9/97c (9.3%) NS
Moderate OHSS 10/51b (19.6%) 15/97c(15.5%) NS
Note: Values are means ± SD or the number (percentage) of patients. NS = not significant; OHSS = ovarian hyperstimulation syndrome; PCOS = polycystic ovary syndrome.
a One woman is omitted secondary to precipitous drop in estradiol with no retrieval and two additional women are omitted for fertilization failure.
b Six women who had no embryo transfer (cryopreservation of all embryos) are omitted.
c Five women who had no embryo transfer (cryopreservation of all embryos) are omitted.
Table 2 Outcome of ovarian stimulation between early and late coasting subsets. IVF data Early coasting (n = 26)a Late coasting (n = 31)b P value
Age (year) 31.8 ± 4.5 31.8 ± 4.4 NS
Start coasting day 8.4 ± 1.1 11.0 ± 1.3 < 0.001 Total coasting days 3.0 ± 1.0 1.5 ±0.6 < 0.001 E2 on coasting day (pg/mL) 2,010 ± 946 3,753 ±1,217 < 0.001 E2 peak value (pg/mL) 3,600 ± 1,627 4,872 ± 2,461 0.028 E2 on day of hCG (pg/mL) 3,466 ± 1,780 4,528 ± 2,652 NS Total gonadotropin (amps) 23.3 ± 5.3 24.6 ± 5.4 NS Largest follicle size on
coasting (mm) 12.8 ± 1.5 17.0 ±1.7 < 0.001
Follicle No. on coasting 19.3 ± 4.5 23.7 ±7.0 0.022 No. of oocyte retrieved 21.3 ± 9.9 21.0 ± 7.9 NS No. of oocyte fertilized 12.2 ± 7.1 13.0 ± 5.4 NS Fertilization rate (%) 55.8 ± 20.0 63.7 ± 22.9 NS Fertilization failure (%) 2/28 (7.1%) 0/31 (0%) NS No. of embryo transferred 4.9 ± 1.2c 5.0 ± 0.9d NS No. of patients with PCOS 7/26 (26.9%) 2/31 (6.5%) 0.04 Pregnancy rate per transfer 9/23c (39.1%) 9/28d (32.1%) NS Multiple pregnancy rate 3/9 (33.3%) 3/9 (33.3%) NS Implantation rate 14/114 (12.3%) 14/145 (9.6%) NS
Severe OHSS 2/23c (8.7%) 3/28d (10.7%) NS
Moderate OHSS 5/23c (21.7%) 5/28d(17.9%) NS
Note: Values are means ± SD or the number (percentage) of patients. NS = not significant; OHSS = ovarian hyperstimulation syndrome; PCOS = polycystic ovary syndrome.
a Two women are omitted for fertilization failure.
b One woman is omitted secondary to precipitous drop in estradiol with no retrieval. c Three women who had no embryo transfer (cryopreservation of all embryos) are omitted.
d Three women who had no embryo transfer (cryopreservation of all embryos) are omitted