The Effects of Reminiscence Group Therapy on Self-esteem, Depression, Loneliness and Life Satisfaction of Elderly People Living Alone
10
0
0
全文
(2) 134. personality is a continuing process. Elderly people, through recalling their experiences, can extend continuity of inner feeling and external behavior so as to achieve integrity [1-2]. RGT can help older people find their lost individual inner resources and merits, establish their confidence, increase their self-esteem, develop positive thinking and resolve most of their mental problems [2-8]. It gives the elderly an opportunity to socialize, and through sharing their experiences, they can exert their deep recall to reduce their loneliness and increase their selfidentity and belonging [3-8]. Many studies have examined the effect of reminiscence therapy on the elderly [3-11]. However, because of the various research designs that have been used to study RGT, there is a lack of consist research findings [1,10]. Chao et al [7] invited 12 elderly nursing home residents to participate in RGT once a week, one hour each for a total of nine sessions. The results indicated that RGT significantly improved self-esteem; however, the effects on alleviating depression and improving life satisfaction were not significant. They concluded that the most beneficial aspect of RGT is that it enhances social interaction in nursing home settings and serves as a support group for participants. Wang et al [3-6] conducted four studies with a quasi-experimental design to examine the effects of RGT on depressive symptoms, self-esteem, and self-health perception among institutionalized adults. They reported that participants who underwent RGT demonstrated fewer depressive symptoms, better mood states, and increased self-esteem; self-health perception also improved slightly. Hsieh and Wang [10] reported that 10 to 12 sessions of RGT resulted in a significant decrease in depression. Most elderly living alone in Taiwan are poor and lack supportive resources. These individuals are often unable to adapt to the aging process, and are susceptible to developing depression, experiencing loneliness and losing their self-confidence and satisfaction with life [12]. RGT may be an effective intervention to improve the adaptability of elderly living alone. However, no studies have examined the effects of. Reminiscence Group Therapy. RGT on elderly living alone who are poor and devalued. Aims and objectives. The purpose of this research was to explore the effects of RGT on self-esteem, depression, loneliness and life satisfaction among poor elderly living alone in Taiwan. Four hypotheses were examined in this study: 1) there are no significant differences in pre-test scales of selfesteem, depression, loneliness and life satisfaction between the experimental and control groups; 2) there are significant differences in pre-post test scales of self-esteem, depression, loneliness and life satisfaction among those in the experimental group; 3) there are no significant differences in pre-post test scales of self-esteem, depression, loneliness and life satisfaction among those in the control group; and 4) there are significant differences in the changing values of the sampled elderly in their pre-post test scales of self-esteem, depression, loneliness and life satisfaction between experimental and control groups. SUBJECTS AND METHODS Design and sample. A pre-post test controlled quasiexperimental design (PPTCQD) was used in this study. Through convenient sampling, a target population of 390 elderly individuals living alone was chosen from a public nursing home for the elderly in northern Taiwan. The criteria for residing in this public community are 1) low income and 2) having no next-of-kin caregivers. Participants were volunteers who had been recruited through posters and interviews. All of the volunteers completed the short portable mental status questionnaire (SPMSQ) test. The inclusion criterion for this study was a score of 8 or more. The final sample population (n = 34) was randomly allocated to either the experimental group or the control group. The elderly in the experimental group participated in 10 RGT sessions. A total of 5 participants in the experimental group withdrew from the study for the following reasons: death (n = 1), went abroad (n = 3), and found a part-time job (n = 1). Therefore, 12 elderly individuals in the experimental group completed the pre- and post-.
(3) Shwu-Jiuan Liu, et al.. test questionnaires. The elderly in the control group participated in 10 sessions of regular group activities. Three participants in the control group withdrew from the study for the following reasons: went abroad (n = 2) and found a parttime job (n = 1). Therefore, 14 elderly in the control group completed the pre- and post-test questionnaires. Protocol of reminiscence group therapy (RGT). RGT was held every Saturday for one hour for a total of ten weeks. RGT activities were semi-structured. The purpose of RGT was to strengthen self-esteem, reduce depression and loneliness, and improve life satisfaction. The main topics of each session were “It is good to know you”, “Singing the old songs together”, “Memorable people”, “Unforgettable events”, “Memorable relatives and friends”, “Past golden years”, “Important life experiences”, “Past and present”, “Memory and expectation”, and “Feeling sad when parting”. The principle investigator was the leader of each RGT session. Three graduate students in nursing and one research assistant assisted in observing, recording and photographing/video taping the RGT process. The principle investigator and the four assistants discussed the RGT process immediately after each session. Instruments. Self-esteem scale. The Rosenberg selfesteem scale (SES) [13] was used to measure individual self-valuation and self-acceptance. The SES is scored using a 4-point Likert-style response format resulting in a scale ranging from 10 to 40, with higher scores representing higher self-esteem. The SES is the most common measure of global self-esteem of adults and has high reliability and validity. The Cronbach’s alpha coefficient of internal consistency of the data scales (n = 34) was 0.87. The significant split-half reliability of this study was 0.89. Depression scale. The Center for Epidemiologic Studies Depression Scale (CES-D) [14] was used to measure the level of depression in this study. The CES-D consists of 20 items and is scored on a 4-point Likert-type response format. 135. from 1 “none” to 4 “most”; total scores ranged from 20 to 80. Higher scores indicated more severe levels of depression . Using 120 elderly in the sampled community as a testing base, the Cronbach’s alpha coefficient of internal consistency was 0.89, and the test-retest reliability between two weeks was 0.85 [15]. The Cronbach’s alpha coefficient of internal consistency of the data scales (n = 34) was 0.81. Loneliness scale. The UCLA Loneliness Scale [16] was used to measure loneliness in this study. There are 20 questions in total. The 4-point Likert scale ranged from 1 “never” to 4 “always”. Total scores ranged from 20 to 80. Higher scores indicated a greater feeling of loneliness. The scale has been shown to have high validity and reliability. In this study, the Cronbach's alpha coefficient was 0.87 and the split-half reliability was significant at 0.85. Life satisfaction scale. Life satisfaction was measured using the LSI-A (Life Satisfaction Index A), a 20-item measure frequently used with the elderly [17]. The 4-point Likert scale ranged from 1 “strongly disagree” to 4 “strongly agree”; total scores ranged from 20 to 80. Higher total scores indicated better life satisfaction. The Cronbach’s alpha coefficient of internal consistency of the data scales (n = 34) was 0.83. Demographic data. Demographic data included age, education, gender, marriage status, religious affiliation, financial resources and disease. Other data gathered included activity of daily living (ADL), degree of social functioning, cognitive function and self-assessment of health scores. ADL was measured by the Barthel Index. Scores range from 0 to 100, with higher scores indicating greater degree of independence. Social functioning was measured by the instrumental activity of daily living (IADL). It comprises 8 items with scores ranging from 8 to 31; the higher the score, the more independent an individual is in performing social functions. Cognitive function was measured with the SPMSQ. There are 10 questions in total with two possible answers: 1 “correct” and 0 “incorrect”. The total scores range from 0 to 10; higher scores indicate higher cognitive function. There were four questions.
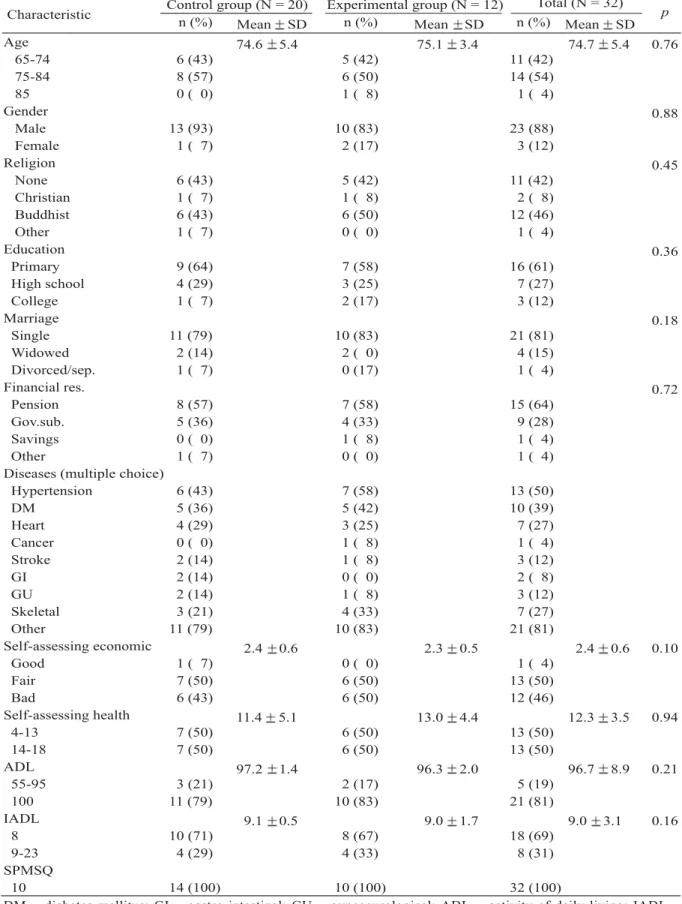
(4) 136. Reminiscence Group Therapy. which allowed individuals to self-assess their health. They were graded using a 5-point Likert scale, ranging from 1 “extremely poor” to 5 “excellent”. Total scores range from 4 to 20; higher scores correlate with better self-reported health status. ADL, IADL, SPMSQ and Selfassessing Health questionnaires are welldeveloped measures frequently used with the elderly and all of them have highly reliability and validity.. deviation of 3.1. The mean SPMSQ score was 10. Self-health assessment ranged from 8 to 20, with a mean of 12.3 and a standard deviation 3.49. There were no significant differences in variance between the experimental and control groups (Mann-Whitey U test; p > 0.05) (Table 1), indicating that the pre-test scores were comparable between groups.. Procedure. The first hypothesis regarding self-esteem was not valid, but the second, third and fourth hypotheses were valid (p < 0.05) (Tables 2-4). There were significant differences in the pre-test scores measuring self-esteem between individuals in the experimental group and those in the control group. There were also significant differences between the pre- and post-test scores in the experimental group, but there were no significant differences between the pre- and post-test scores in the control group. Furthermore, there were significant differences in the changes from pre-to post-test scores in both groups. Therefore, RGT appears to improve the self-esteem of elderly people living alone.. This study was approved by the National Science Council of Taiwan. All participants provided written informed consent. Research study objectives, content, and procedures were discussed with the administrators and assistants of the nursing home before the first session. Interested subjects were instructed to sign a consent form, complete the questionnaire, and return it to the principal investigator. Then, participants were randomly allocated to either the experimental or control group. All participants in both groups completed the self-reported questionnaires within one week after completing the tenth session of either RGT or regular group activities. Data analysis. The research hypotheses were examined statistically by the Mann-Whitney U test, Wilcoxon matched-pairs signed-ranks test, and the Kolmogorov-Smirnov one sample test of nonparameter data. Furthermore, records and audio and video recording produced during the individual interviews and group sessions were added to the database for analysis. RESULTS. Participants ranged in age from 65 to 85 years, with a mean age of 74.7 years. Only 3 of them were female. Twenty-one of the participants were unmarried and four were widowed. Eleven (42.3%) of the participants had no religious belief. Their main financial resources (92.3%) came from pensions and governmental subsidies. ADL ranged from 55 to 100, with a mean of 96.7 and a standard deviation of 8.9. IADL ranged from 7 to 23, with a mean of 9.0 and a standard. RGT significantly enhances the level of self-esteem of elderly living alone. RGT lessens the degree of depression among living-alone elderly. The second hypothesis regarding depression was not valid, but the first, third and fourth hypotheses were valid (p < 0.05) (Tables 24). There were no significant differences in pretest scores measuring depression between the experimental and control groups of elderly living alone. There were also no significant differences between the pre- and post-test scores in the experimental group, and there were no significant differences between the pre- and post-test scores in the control group. However, there were significant differences in the changes from pre- to post-test scores in both groups. Therefore, RGT did not have a significant impact on reducing depression among the participants who lived alone. Yet, when the results from the RGT and control groups were compared, we found that RGT did lessen the degree of depression among the elderly who lived alone..
(5) Shwu-Jiuan Liu, et al.. 137. Table 1. Comparison of demographic data of the sampled elderly before reminiscence group therapy (MannWhitney U test) Total (N = 32) Control group (N = 20) Experimental group (N = 12) p Characteristic n (%) n (%) Mean SD n (%) Mean SD Mean SD. Age 0.76 74.6 5.4 75.1 3.4 74.7 5.4 6 (43) 65-74 5 (42) 11 (42) 8 (57) 75-84 6 (50) 14 (54) 0 ( 0) 85 1 ( 8) 1 ( 4) Gender 0.88 13 (93) Male 10 (83) 23 (88) 1 ( 7) Female 2 (17) 3 (12) Religion 0.45 6 (43) None 5 (42) 11 (42) 1 ( 7) Christian 1 ( 8) 2 ( 8) 6 (43) Buddhist 6 (50) 12 (46) 1 ( 7) Other 0 ( 0) 1 ( 4) Education 0.36 9 (64) Primary 7 (58) 16 (61) 4 (29) High school 3 (25) 7 (27) 1 ( 7) College 2 (17) 3 (12) Marriage 0.18 11 (79) Single 10 (83) 21 (81) 2 (14) Widowed 2 ( 0) 4 (15) 1 ( 7) Divorced/sep. 0 (17) 1 ( 4) Financial res. 0.72 8 (57) Pension 7 (58) 15 (64) 5 (36) Gov.sub. 4 (33) 9 (28) 0 ( 0) Savings 1 ( 8) 1 ( 4) 1 ( 7) Other 0 ( 0) 1 ( 4) Diseases (multiple choice) 6 (43) Hypertension 7 (58) 13 (50) 5 (36) DM 5 (42) 10 (39) 4 (29) Heart 3 (25) 7 (27) 0 ( 0) Cancer 1 ( 8) 1 ( 4) 2 (14) Stroke 1 ( 8) 3 (12) 2 (14) GI 0 ( 0) 2 ( 8) 2 (14) GU 1 ( 8) 3 (12) 3 (21) Skeletal 4 (33) 7 (27) 11 (79) Other 10 (83) 21 (81) Self-assessing economic 0.10 2.4 0.6 2.3 0.5 2.4 0.6 1 ( 7) Good 0 ( 0) 1 ( 4) 7 (50) Fair 6 (50) 13 (50) 6 (43) Bad 6 (50) 12 (46) Self-assessing health 0.94 11.4 5.1 13.0 4.4 12.3 3.5 7 (50) 4-13 6 (50) 13 (50) 7 (50) 14-18 6 (50) 13 (50) ADL 0.21 97.2 1.4 96.3 2.0 96.7 8.9 3 (21) 55-95 2 (17) 5 (19) 11 (79) 100 10 (83) 21 (81) IADL 0.16 9.1 0.5 9.0 1.7 9.0 3.1 10 (71) 8 8 (67) 18 (69) 4 (29) 9-23 4 (33) 8 (31) SPMSQ 14 (100) 10 10 (100) 32 (100) DM = diabetes mellitus; GI = gastro-intestinal; GU = gynecourological; ADL = activity of daily living; IADL = instrumental activity of daily living; SPMSQ = short portable mental status questionnaire..
(6) 138. Reminiscence Group Therapy. Table 2. Comparison of the pre-test scores of self-esteem, depression, loneliness and life satisfaction of the sampled elderly between experimental and control groups (Mann-Whitney U test) Control group (N = 14) Experimental group (N = 12) p Variables Mean SD Mean SD Self-esteem 0.030 22.3 3.0 20.1 5.3 Depression 0.455 42.3 6.3 43.1 6.8 Loneliness 0.481 51.0 8.7 54.3 7.3 Life satisfaction 0.389 56.5 6.1 55.6 6.6. Table 3. Comparison of the pre-post test scores of self-esteem, depression, loneliness and life satisfaction of the sampled elderly for experimental and control groups (Wilcoxon test) Control group (N = 14) Experimental group (N = 12) p p Pre-test Post-test Pre-test Post-test Variables Mean SD Mean SD Mean SD Mean SD 0.018 Self-esteem 0.681 22.3 3.0 21.2 4.2 24.4 3.1 20.1 5.3 0.925 Depression 0.120 42.3 6.3 22.0 3.2 43.1 6.8 22.1 3.4 < 0.001 Loneliness 0.001 51.0 8.7 35.8 7.0 54.2 7.3 35.5 3.4 < 0.001 Life satisfaction 0.013 56.5 6.1 32.7 3.8 55.6 6.6 35.1 3.2. Table 4. Comparison of the change in scores of pre-post test of self-esteem, depression, loneliness and life satisfaction of the sampled elderly between experimental and control groups (Kolmogorov-Smirov Z test) Control group (N = 14) Experimental group (N = 12) p (Change in value between pre-post test) (Change in value between pre-post test) Variables Mean SD Mean SD change scores change scores Self-esteem < 0.001 –2.1 4.0 – 1.1 3.7 Depression 0.047 0.3 4.7 2.0 5.4 Loneliness < 0.001 6.2 12.0 15.8 13.3 Life satisfaction < 0.001 – 4.5 8.8 –14.4 8.6. RGT significantly lessens the level of loneliness of elderly living alone. RGT significantly increases the level of life satisfaction of elderly living alone. The third hypothesis regarding loneliness was not valid, but the first, second and fourth hypotheses were valid (p < 0.05) (Tables 2-4). There were no significant differences in pre-test scores measuring loneliness between the experimental and control groups. There were significant differences in the pre- and post-test scores in the experimental group, and significant differences in the pre- and post-test scores in the control group. Furthermore, there were significant differences in the changes between pre- and posttest scores in both groups; therefore, RGT significantly lessens the feeling of loneliness among elderly living alone.. The third hypothesis regarding life satisfaction was not valid, but the first, second and fourth hypotheses were valid (p < 0.05) (Tables 2-4). There were no significant differences in pre-test scores measuring life satisfaction between the experimental and control groups. However, there were significant differences between the pre- and post-test scores in the experimental group, and significant differences between the pre- and post-test scores in the control group. There were also significant differences in the changes between pre- and posttest scores in both groups, indicating that RGT significantly improves life satisfaction among the elderly living alone..
(7) Shwu-Jiuan Liu, et al.. RGT process and feedback from participants. Group proceeding. The first session included an explanation of RGT by the leader and self-introduction by the elderly. The purpose of this meeting was to acquaint each member with the group objectives, goals and rules. The second session was designed to encourage the participants to sing old songs and describe the background of the songs. The purpose of this meeting aimed to increase the interaction and cohesion of the group. The third session focused on encouraging the participants to show and talk about their photographs. The purpose of this was to get them to talk about themselves and in turn to reminisce. The fourth through seventh sessions were designed to allow the participants to share their proudest events, most unforgettable love affairs, most memorable moments and the most wanted-to-be-shared experiences. The purpose of these four sessions was to allow them to further reminisce about their past experiences so as to continue to improve their self-esteem, lessen their depression and loneliness and promote their life satisfaction. The eighth through tenth sessions were designed to help the participants link their experiences with the present and the expectation of the future. The purpose of these sessions was to ready the participants to accept the ending of the group sessions. Group dynamics. During the first session, participants A and B gave passive selfintroductions and then remained silent. During the second session, three participants were very active, voluntarily participating and speaking eagerly. Occasionally, they did not follow the voicing rules or pay attention to others who were talking. Participant M was irritated by this and voiced his opinion. Many decided to re-initiate the rules. Through the process of re-initiating the rules, the group became more cohesive while the group leader remained in control of the group activities. During the third session, five participants forgot to bring their photos and two of them insisted on going back home for them. They often spoke about past events and all of them were very enthusiastic. There was much laughter, especially when one participant talked about his ex-. 139. girlfriend. The group encouraged each other to go back to fetch more photos. They helped keep seats for the absentees. They also gave verbal support to others. This indicates that the group cohesiveness was strengthening. Although participant A remained silent, he showed that he was paying attention by nodding or raising his head. During the fourth through seventh sessions, the members of the group started to praise the group and voice their expectations. Five people came early and waited for the session to start. Participant W started to actively join during the fourth session. It was said that he had tried to commit suicide; he was also a visibly depressed person. He told the group that he was tired of life because of poor sight and immobility. He believed that the RGT would help him so he came to the group voluntarily. He obeyed the rules and his words were very meaningful. He earned respect from the group. Mr. W participated during the entire fifth session and said that he was eagerly looking forward to the next session. His mood improved markedly. In these sessions, the participants were actively engaged in discussion and the group cohesion was therefore very strong. They started to care for, help and talk to each other. During the sixth session, Mrs. P, an elderly lady recalled her miserable life and started to cry. This inspired the group to discuss the matter ardently. Many of the elders started to compare their past and present situations, such as bad marriages and having children with no filial piety. They encouraged each other and felt blessed and thankful with what they had experienced. Some elders stated that they accepted their past and present situation because they felt that everything was controlled by fate. The participants also mutually suggested how they could adjust and cope with old age, and activities that could improve the quality of their lives. They also provided information as reference to the group. During the eighth through tenth sessions, the participants started to voice their concern about modern society and about the direction that it was developing. They started to compare young people today with young people of their.
(8) 140. Reminiscence Group Therapy. generation. They also advised young people who attended the session to work hard and control their own life. There was more group interaction and the atmosphere was very cordial; a strong group cohesion had developed among them. Evaluation of the group. All of the members stated that they would miss each member of the group when the sessions come to an end. Some of the elderly expressed that they had been forgotten about by the society; however, they felt great comfort and expressed appreciation that the leader and members of the RGT were willing to show concern for them. Mr. F had diabetes, high blood pressure and colon cancer. He indicated that he felt happier and no longer worried about dying suddenly because he had attended the RGT sessions and felt cared for. The researcher also found that some of the participants who were normally loners had begun to interact actively with the group. DISCUSSION. Our findings indicate that RGT significantly improved self-esteem, reduced the feeling of loneliness, and promoted life satisfaction among elderly living alone. The results confirmed the findings reported in several studies [3-7] that RGT helped elderly people adopt a more self-assertive attitude, thereby resolving the feeling of loneliness and promoting life satisfaction. RGT gives the elderly a chance to get acquainted with others who experience psychological problems and life events similar to theirs. Through the process of retelling and sharing life experiences, elderly living alone begin to realize that they are not alone. RGT also provides a chance to support others. Researchers [1,10] have demonstrated that RGT has a positive impact on increasing the adaptability of elderly living alone. For example, RGT helps individuals recall and reconstruct past experiences, achieve a more positive valuation of their lives, expand self-understanding and personality development, increase self-assertiveness, and therefore helps the elderly achieve a feeling of integral satisfaction. RGT can help the elderly living alone find their lost individual inner resources and. merits, establish their confidence and positive thinking, and resolve most of their mental problems [1-2,10]. Although RGT did lessen depression among the elderly in the RGT group in this study, the reduction was not statistically significant, and therefore did not confirm the findings reported by Hsieh and Wang and Wang [3,10]. Those scholars found that 10 to 12 sessions of RGT resulted in a significant decrease in depression, but that shorter or longer periods of reminiscence therapy did not increase its effectiveness on decreasing depression in older adults. They concluded that personal characteristics of the elderly have an impact on the outcome of RGT. Cully et al [19] stated that older adults who reported suffering from depression used reminiscence more frequently than those who did not. RGT was a more comfortable and effective therapy for these elderly. In this study, the performance of participant W seems to support the views of Cully et al. The limitation of the study was that the samples were not randomized; therefore, a further study which includes elderly with a high level of depression is necessary. In this research, the regular group activities seemed to reduce the feeling of loneliness and increase satisfaction with life among individuals in the control group. This finding may be the result of repeated testing. The number of elderly living alone is increasing every year in Taiwan. Dormitories for the elderly have recently been established by governmental agencies and the private sector [12]. Elderly living alone in institutions in Taiwan will become common-place in the future. These individuals tend to have low social economic status, which contributes to their low self-esteem, loneliness, and depression. Depression and life dissatisfaction among these elders have become major problems associated with mortality and suicide. Health care for the elderly living alone should focus not only on the physical dimension, but also on the psychological dimension. Therefore, RGT should be incorporated in the care for these elderly individuals. Further research in the application of RGT for elderly living alone.
(9) Shwu-Jiuan Liu, et al.. 141. using rigorous research designs is needed. This should include a larger sample size and RGT sessions of various durations. This study demonstrates that RGT significantly improves self-esteem, lessens the feeling of loneliness and promotes life satisfaction among elderly living alone. Although RGT did not significantly reduce the level of depression, improvement was noted in the RGT group when the results were compared with those of the control group. The investigators conclude that RGT is an effective alternative intervention with minimal harmful side effects which can help living-alone elderly adapt to the aging process. Future randomized controlled trials are needed to provide better empirical information about the efficacy of RGT on psychosocial adaptation of elderly living alone.. 7. Chao SY, Liu HY, Wu CV, et al. The effects of group. ACKNOWLEDGMENT. 12. Department of Social Affairs, Ministry of the. reminiscence therapy on depression, self esteem, and life satisfaction of elderly nursing home residents. J Nurs Res 2006;14:36-45. 8. Lai CK, Chi I, Kayser-Jones J. A randomized controlled trial of a specific reminiscence approach to promote the well-being of nursing home residents with dementia. Int Psychogeriatr 2004;16:33-49. 9. Jones ED, Beck-Little R.The use of reminiscence therapy for the treatment of depression in ruraldwelling older adults. Issues Ment Health Nurs 2002; 23:279-90. 10.Hsieh HF, Wang JJ. Effect of reminiscence therapy on depression in older adults: a systematic review. [Review] Int J Nurs Stud 2003;40:335-45. 11.Stinson CK, Kirk E. Structured reminiscence: an intervention to decrease depression and increase selftranscendence in older women. J Clin Nurs 2006;15: 208-18.. The author would like to thank the National Science Council (NSC) for financial support and all of the elderly people who participated in the program.. Interior, R. O. C. The welfare for elderly, 2004. http://volnet.moi.gov.tw/sowf/04/new04.asp. 13.Rosenberg M. Society and the adolescent self-image. Princeton NJ: Princeton University Press, 1965. 14. Radloff LS. The CES-D scale: a self-report depression. REFERENCES 1. Lin YC, Dai YT, Hwang SL. The effect of reminiscence on the elderly population: a systematic review. [Review] Public Health Nurs 2003;40:297306. 2. Coleman PG. Uses of reminiscence: functions and benefits. Aging Ment Health 2005;9:291-4. 3. Wang JJ. The effects of reminiscence on depressive symptoms and mood status of older institutionalized adults in Taiwan. Int J Geriatr Psychiatry 2005;1:5762. 4. Wang JJ, Hsu YC, Cheng SF. The effects of reminiscence in promoting mental health of Taiwanese elderly. Int J Nurs Stud 2005;1:31-6. 5. Wang JJ. The comparative effectiveness among institutionalized and non-institutionalized elderly people in Taiwan of reminiscence therapy as a psychological measure. J Nurs Res 2004;12:237-45. 6. Wang JJ. The effects of reminiscence on self-health perception and self-esteem of institutionalized elderly in Taiwan. Int J Psychiatr Nurs Res 2004;9:1092-9.. scale for research in the general population. Applied Psychological Measurement 1977;1:385-401. 15.Chang SH. Research of the relationship of elder’s loneliness to self-assessing health and social support. Nursing Research Institute of Kaohsiung Medical School, Taiwan, 1996. 16.Russell D, Peplau LA, Cutrona CE. The revised UCLA Loneliness Scale: concurrent and discriminant validity evidence. J Pers Soc Psychol 1980;39:472-80. 17. Neugarten BL, Havighurst RJ, Tobin SS. The measurement of life satisfaction. J Gerontol 1961;16: 134-43. 18. Liu SJ. The exploration of life attitudes and life satisfaction for elderly with chronic illness. J Nurs Res 1999;7:294-306. 19. Cully JA, LaVoie D, Gfeller JD. Reminiscence, personality, and psychological functioning in older adults. Gerontologist 2001;41:89-95. 20. Cappeliez P, O’Rourke N, Chaudhury H. Functions of reminiscence and mental health in later life. Aging Ment Health 2005;9:295-301..
(10) 142. 12 14. 2007;12:133-42. 404. 91. 2006. 9. 7. 2007. 5. 16. 2007. 4. 25.
(11)
數據

相關文件
and Kasper, H.D.P., “The impact of Satisfaction on Brand Loyalty: Urging on Classifying Satisfaction and Brand Loyalty,” Journal of Consumer Satisfaction, Dissatisfaction
(2000), “Assessing the Effects of Quality, Value, and Customer Satisfaction on Consumer Behavioral Intentions in Service Environments,” Journal of Retailing, Vol. (2001),
The prevalence of the In-service Education is making the study of In-service student satisfaction very important.. This study aims at developing a theoretical satisfaction
Methodologies used in this study comprise two parts, the first part is questionnaires, which investigate customers’ assessment of the quality and satisfaction of service
Given different levels of homeroom teachers’ transformational leadership, there are significant differences regarding students’ learning satisfaction.. Students have
This study aims to explore whether the service quality and customer satisfaction have a positive impact on the organizational performance of the services and whether the
The purpose of this study was to explore the effects of learning organization culture on teachers’ study and teaching potency in Public Elementary Schools.. The research tool of
2.There are no significant differences in leaning will (including knowledge and skills enrichment, external enhancement and self-development.) among sexuality,
