ࠉȁȁِ
住院醫師訓練階段對個人的成長及專業的發 展而言,畢業後的第一年(first postgraduate year,
PGY1),是個有明顯改變的嶄新的一年。許多議 題考驗著 PGY1 的醫師的能力與適應力,包括承擔 照顧病患的責任、病患照顧的各種需求、睡眠剝 奪、減少與家人相處的時間、支持系統的變動等等 [1,2] 。80 年代起,國外許多的研究[3-8] 顯示 PGY1 承
呂碧鴻
1,2、高美英
3、陳秀蓉
4、王長偉
1目的:畢業後第一年住院醫師(First postgraduate year, PGY1)訓練是最有壓力的一 年,本研究調查 PGY1 醫師的壓力源與內容以及探討其工作滿意度與相關影響因素。研究 方法:以 2006 年度 PGY1 醫師為研究對象,調查期間為 2007 年 1 月至 6 月。利用問卷 調查方式進行工作壓力與滿意度的測量與資料收集。以因素分析檢測工作壓力來源。利 用迴歸分析探索工作滿意度之預測因子。結果:共有 555 位醫師(回收率 90.0%)參與研 究。工作壓力源有工作情境壓力、情緒/病患需求壓力,醫學臨床技能壓力、親友生病與 臨床病患處置壓力及個人因素壓力五種因素(解釋工作壓力變異量 55.7%)。有 38.0% 之 PGY1 醫師經常感受到壓力。工作情境壓力與情緒/病患需求壓力為主要壓力源。將近七 成之醫師感受到睡眠不足或值班時要常常保持警覺之壓力,六成左右的醫師有文書行政作 業或工作過量之沉重壓力;55.0 % 的醫師感受害怕做錯事或發生訴訟事件之壓力。工作滿 意度之最主要預測因子為工作情境壓力(解釋變異量為 19.9%),其次為情緒支持(解釋 變異量為 9.7%)。結論:PGY1 住院醫師主要壓力源是工作情境壓力與情緒/病患需求壓 力,工作情境壓力影響工作滿意度。因為工作壓力將威脅身心健康與臨床表現,本研究建 議建構諮商輔導機制與確實運作,以降低因住院醫師壓力影響所及之身心健康問題與提升 醫療照護品質。 關鍵詞:工作壓力、工作滿意度、畢業後第一年住院醫師 (醫學教育2009;13:113 ~ 121) 1 國立臺灣大學醫學院家庭醫學科、2社會醫學科;3臺北醫學大學醫學人文研究所;4國立臺灣師範大學 教育心理與輔導學 受理日期:2009 年 4 月 22 日;接受日期:2009 年 6 月 30 日 通信作者:陳秀蓉,106 台北市大安區和平東路一段 162 號 國立臺灣師範大學教育心理與輔導學系 電子信箱:[email protected]
受許多的壓力以及與壓力密切相關的情緒、精神 的困擾。根據美國內科訓練計畫主持人協會(the Association of Program Directors in Internal Medicine) 的調查,住院醫師常見的壓力源可被歸類為情境壓 力(例如睡眠剝奪,沉重的工作負擔);專業壓力 (例如病患照顧的責任,生涯規劃,健康照護型態 的變遷);個人壓力(例如經濟議題,因應策略技 巧不足,家庭問題)[3] 。 為因應新世紀疾病型態改變的挑戰,與避免醫 師過度專科化及失去一般性病患照護的能力,美國 醫療研究院(Institute of Medicine)於 2003 年發表 的醫療專業教育,指出要實現優質、安全的醫療, 必須進行醫療專業教育的改變,使醫療專業人員具 備五項核心能力:以病人為中心的醫療;跨領域的 團隊工作;基於實證的專業執行;醫療品質促進及 資訊技術利用[9] 。國內衛生署為培育住院醫師的核 心能力與落實全人醫療訓練,2006 年 8 月起國內 實施一年期之 PGY1 一般醫學訓練。依規劃的訓練 內容將包括一個月的一般醫學實務訓練、一個月社 區醫學基本課程、一個月社區醫學相關選修、3 個 月之專科相關選修及 6 個月之專科全人醫療訓練 [10] ,因此 PGY1 醫師一年內將會面臨至少 5 種不同 科別之訓練,人、事、學習環境與學習內容的更迭 對 PGY1 醫師而言將是嚴格的考驗。是否因而造成 壓力以及其學習成效如何等議題都值得探討。因此 本研究的目的為:1. 瞭解 PGY1 醫師的壓力源與內 容。2. 評估 PGY1 醫師之工作滿意程度及探討其影 響因素。
ਟᇄПݲ
研究對象 本研究以 2006 年度全台灣之 PGY1 醫師為研 究對象。但考量讓 PGY1 初起對承擔醫療事務需 要些許時間來適應,本研究調查以 2007 年 1 月~6 月底所有參與 PGY1 訓練者為主要施測之對象。 研究工具與程序 本研究以問卷調查法進行。為提高回收率,選 取 PGY1 醫師醫療業務負荷較不沈重(不須值班) 之時段,即利用其前往接受社區醫學訓練之時段進 行問卷調查。由社區醫學訓練計畫主持人說明調查 目的與內容,邀請 PGY1 醫師參與調查。研究對象 完成問卷之填答後,直接以隨附之回郵信封將問卷 密封郵寄回研究人員。 本研究分析涵蓋之問卷內容如下: 一、壓力測量量表 Cooper等學者為探索英國全科醫師的精神健 康狀態與壓力之相關性,透過訪談全科醫師之資 料,分析出 31 項全科醫師面臨的工作壓力而建構 了工作壓力量表(Job Stress Questionnaire,JSQ) [11] 。Tyssen 等學者則因應挪威醫師訓練情境的差異 性,進行 Cooper’s JSQ 之修正[12] ,該量表共有 32 題項,因素分析結果得到 3 個因素:情緒壓力/ 病患需求、工作中斷(interruptions)/時間壓力 及社交生活影響。本研究參考 Cooper’s Job Stress Questionnaire(JSQ)及 Tyssen 修正後的版本建構 本土化之工作壓力量表。量表共有 38 題項,感受 到的壓力程度,以五點量尺計分(1= 從不覺得; 5=總是覺得),分數越高表示壓力越大,Tyssen 的量表 Cronbach’s α 值為 0.90。本研究樣本在此 量表之 Cronbach’s α 值為 0.931。此外,並詢問 PGY1醫師就整體而言他們感受到的工作壓力程度 (1= 從不覺得;5= 總是覺得)。 二、工作滿意度量表 Cooper等學者由 Warr 等人發展之工作態度與 心理健康測量量表選取十個題項建構工作滿意度量 表[11,13] 。本研究採用 Cooper 之量表進行工作滿意 度之測量。量表共有 10 個題項,內容涵蓋對職務 上賦予之責任、職務之活潑多樣性、工作情境、同 事相處、自由選擇工作方式、工作時間、達成工作目標可以得到認可、能充分發揮能力等。量表計分 採 7 點量尺,分數越高表示越滿意。本研究樣本在 此量表之 Cronbach’s α 值為 0.910。 三、基本資料 另蒐集人口學資料、其原屬科別及每週工作時 數等基本資料。並且徵詢 PGY1 醫師就整體而言在 工作中從家人、師長、學長姐與朋友感受到適切之 情緒支持度,以五點量表來評量(1= 從來沒有; 2=很少;3= 有時;4= 常常;5= 一直都是)。 統計分析 本研究使用 SPSS 16.0 for windows 套裝軟體進 行資料建檔及統計分析。以描述性統計方法檢視研 究變項,以 Student’s t-test 比較獨立樣本之連續變 項之差異,並以因素分析探索工作壓力因素結構與 驗證其建構效度。各量表信度分析以 Cronbach’s α 係數評估。另採用逐步複迴歸分析進行工作滿意度 預測變項之探討。本研究設定 p 值 0.05 以下為統 計學上有顯著差異。
๖ȁȁݎ
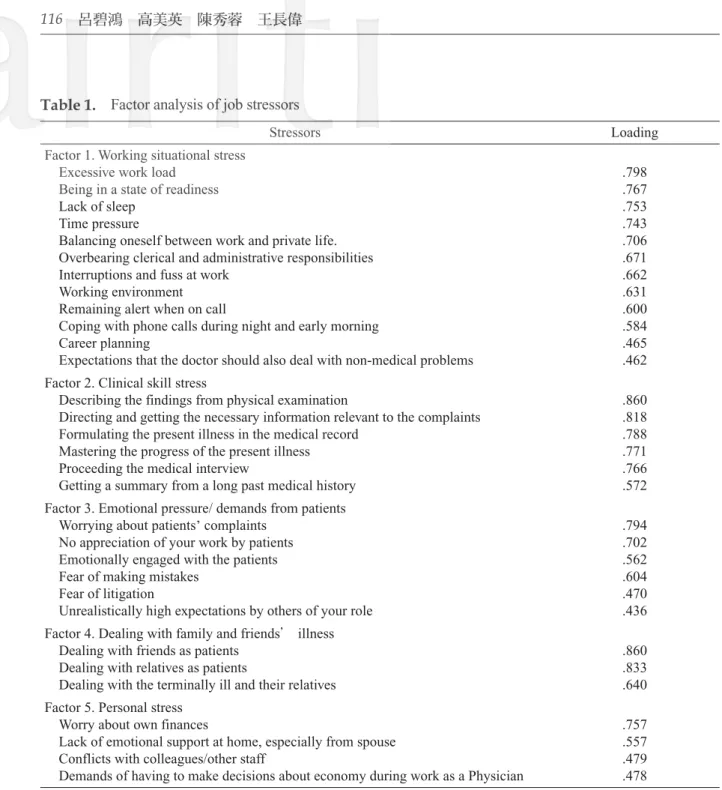
基本資料 共有 617 位 PGY1 醫師接受問卷調查,回收 555份(90.0%)有效問卷可資分析。 男 性 3 5 4 人 ( 6 7 . 7 % ) , 女 性 1 6 9 人 (32.3%)。男女性別分佈與當年度 1221 位 PGY1 醫師之性別分佈無顯著差異。平均年齡為 29.35± 2.58歲。依所屬原科別分成內、外科系兩大類,內 科系(包括內科、家醫科、皮膚科、精神科、神 經科、復健科、急診醫學科、職業醫學科、病理 科、影醫/放射線科)399 人(72.8%),外科系 149人(27.2%)。平均每週工作天數為 5.56±0.54 天,每日工作時數為 10.03±2.48 小時,每週工作 時數為 56.48±17.96 小時。 壓力源及內容 本研究建構之壓力測量量表所得之資料,經 主成分分析法萃取因素及直交轉軸法之最大變異 法進行轉軸,刪除因素負荷量過於接近及低於 0.45 之 7 個題項,最後以 31 題項進行因素分析並強迫 萃取 5 個因素,分別命名為工作情境壓力、醫學臨 床技能壓力、情緒/病患需求壓力、親友生病與 臨終病患處置壓力及個人因素壓力(表 1)。解釋 變異量分別為 19.97%、13.18%、8.79%、7.52% 及 6.24%,累積解釋變異量為 55.70%。本量表 31 題 項之 Cronbach’s α 值為 0.920。 整體而言,有 211 位(38.0%)醫師經常感 受(常常覺得及總是覺得)到工作壓力,302 位 (54.8%)有時感覺到工作壓力。PGY1 醫師感受 到之工作壓力程度其平均得分依大小排序為工作 情境壓力(3.63±0.64)、情緒/病患需求壓力 (3.27±0.60)、醫學臨床技能(2.88±0.65)、親 友生病與臨終病患處置(2.81±0.76)、個人因素 壓力(2.67±0.62)。工作壓力整體得分比較無性 別之差異性。但男性在個人因素壓力之分數較女性 高(2.71±0.60 vs. 2.57±0.63)。(表 2) 依照 PGY1 醫師深刻感受壓力之程度(常常覺 得與總是覺得)的比例來排序,在工作情境壓力內 容中分別為睡眠不足(69.7%)、值班時要常常保 持警覺(67.4%)、負擔過多之文書雜務及行政責 任(63.4%)、工作時被瑣碎雜事打斷(62.0%)、 工作過量(61.6%)、隨時在備戰狀態(58.6%)、 工作上的付出影響到家庭生活(52.1%)、在 夜間或清晨接到電話(51.0%)及工作時限的壓 力(50.0%)。情緒/病患需求壓力方面,依序 則為害怕做錯事(55.1%)、害怕引起訴訟事件 (55.0%)、自己的角色被別人不切實際的過高期 待(34.6%)。醫學臨床技能方面之壓力則為摘要 病人冗長之過去疾病史(28.3%)與掌握病人目前 疾病的進展狀況(22.5%)。親友生病與臨終病患 處置之壓力源中,以處理臨終病人及其家屬問題較多人感受較深(28.1%)。個人因素壓力內容中則 以要求醫師在工作上也需做最經濟合算的決定為主 要的壓力源(42.0%),其次為擔心自己的財務問 題(21.2%)。 工作滿意度與情緒支持 工作滿意度平均得分為 4.12±0.84,男女並無 顯著差異。綜合所有因素,對自己的工作感覺滿意 的有 187 位(33.7%),而相當滿意與非常滿意者 僅 52 位(9.4%),普通者 226 位(40.8%),相當 不滿意與非常不滿意者 50 位(12.2%)。
Table 1. Factor analysis of job stressors
Stressors Loading Factor 1. Working situational stress
Excessive work load Being in a state of readiness Lack of sleep
Time pressure
Balancing oneself between work and private life. Overbearing clerical and administrative responsibilities Interruptions and fuss at work
Working environment Remaining alert when on call
Coping with phone calls during night and early morning Career planning
Expectations that the doctor should also deal with non-medical problems
.798 .767 .753 .743 .706 .671 .662 .631 .600 .584 .465 .462 Factor 2. Clinical skill stress
Describing the findings from physical examination
Directing and getting the necessary information relevant to the complaints Formulating the present illness in the medical record
Mastering the progress of the present illness Proceeding the medical interview
Getting a summary from a long past medical history
.860 .818 .788 .771 .766 .572 Factor 3. Emotional pressure/ demands from patients
Worrying about patients’ complaints No appreciation of your work by patients Emotionally engaged with the patients Fear of making mistakes
Fear of litigation
Unrealistically high expectations by others of your role
.794 .702 .562 .604 .470 .436 Factor 4. Dealing with family and friends' illness
Dealing with friends as patients Dealing with relatives as patients
Dealing with the terminally ill and their relatives
.860 .833 .640 Factor 5. Personal stress
Worry about own finances
Lack of emotional support at home, especially from spouse Conflicts with colleagues/other staff
Demands of having to make decisions about economy during work as a Physician
.757 .557 .479 .478
整體而言,感受到適切之情緒支持度,平均 得分為 3.64±0.74,女性比男性得分高,有顯著差 異。而常常覺得與一直都覺得有獲得適切之情緒支 持者佔 59.2%,很少與從來沒有者佔 5.3%。(表 2) 影響工作滿意度之迴歸分析結果(表 3)顯示 最終模式(F=60.52,df=4,525,p<0.001)內工作 情境壓力、情緒支持、工作時數與個人壓力因素 為顯著之預測變項,共可解釋 31.0% 之變異量。 其中工作情境壓力為最主要之預測變項(解釋 19.9 %之變異量),其次為情緒支持(解釋變異量為 9.7%)。
ଆȁȁ፣
本研究發現近四成(38%)的 PGY1 醫師經常 感受到工作壓力,稍高於 Cohen 與 Toews 等學者 在加拿大的研究[14,15] ,報告約有 34% 的住院醫師 自覺大部分的日子都是很有壓力。許多研究已顯示 醫師的壓力導致情緒變化包括生氣與憂鬱,影響個 人的身心健康,進而妨礙醫療照顧品質,甚至發生 醫療疏失[5,16-19] 。因此,如此高比率的 PGY1 醫師 承受高度的工作壓力是必須重視的。 探討之壓力源中,工作情境壓力與情緒/病患Table 2. Gender difference of job stressors, job satisfaction and emotional support
All mean±SD Male mean±SD Female mean±SD p value Job stress
Working situational stress 3.63±0.64 3.61±0.64 3.66±0.63 p = 0.451 Clinical skill stress 2.88±0.65 2.88±0.64 2.89±0.69 p = 0.792 Emotional pressure/ demands from patients 3.27±0.60 3.26±0.63 3.30±0.56 p = 0.488 Dealing with family and friends’ illness 2.81±0.76 2.80±0.77 2.86±0.74 p = 0.392 Personal stress 2.67±0.62 2.71±0.60 2.57±0.63 p = 0.011 Total 3.21±0.48 3.21±0.50 3.22±0.45 p = 0.718 Job satisfaction 4.12±0.84 4.11±0.88 4.16±0.77 p = 0.559 Emotional support 3.64±0.74 3.54±0.74 3.84±0.70 p < 0.001
Table 3. Stepwise multiple regression analysis of job satisfaction
Predict variables Model 1 Model 2 Model 3 Model 4 Standardized coefficients beta and significances
Working situational stress -.448*** -.401*** -.383*** -.349*** Emotional support .317*** .303*** .291*** Working hour -.101** -.104** Personal stress -.092* Adjusted R square .199 .296 .304 .310 R square change .199 .097 .008 .006 F 132.599*** 112.280*** 78.179*** 60.518***
Dependent Variable: Job satisfaction Note.* p < .05, ** p < .01, *** p < .001
需求壓力是最主要的來源。過去國外的許多研究亦 分別顯示情緒壓力/病患之需求壓力、睡眠不足、 時間壓力、家庭生活與工作之衝突、行政作業、工 作上或生活上受到干擾(例如緊急照會)[5,12,14,16,20] 是最主要的壓力來源。在十二項工作情境壓力中, 就有九項讓五成以上的醫師經常感受到壓力。其中 七成左右醫師覺得睡眠不足。研究文獻指出缺乏 充足之睡眠導致思維障礙、不適切的情感表達、焦 躁、抑鬱、近程記憶缺損等問題,間接影響到臨床 技能表現[5,16] 。目前 PGY1 之訓練,已依相關規定 值班以平均不超過三天一班為原則,但本研究也 發現 PGY1 醫師自填之工作時數,每週工作時數平 均為 56.48±17.96 小時,已低於美國立法規定之每 週 80 小時[21] 。而每日平均工作時數則為 10.03± 2.48小時,超過之工作時數可能意謂著涵蓋住院醫 師必須負責任的工作,額外付出的時間。另外為醫 療專業的成長所付出的時間應該也是睡眠不足的可 能原因。至於六成的醫師感受到過多文書雜務及行 政業務之負擔及工作時被瑣碎雜務打斷的壓力,這 議題也出現在國外的研究結果[20,22] 。但其並非針對 PGY1醫師的調查,所以無從比較。不過,如此高 比例之醫師感受此壓力,則教育訓練單位確實應給 予關注,以便減少對訓練成效的影響。至於值班時 需保持警覺、隨時在備戰狀態或接到電話應診等之 壓力感受,顯示仍有五成以上的 PGY1 醫師有待其 適應能力與臨床技能信心之提升。 在情緒/病患需求壓力的感受方面,Tyssen 等 學者研究[12] 指出此種壓力感受是住院醫師有精神 健康問題的顯著預測因子。理論上,發生情緒或精 神問題可以是多重因素影響,包括個人性格傾向, 例如神經質,與不適切之因應策略,例如傾向逃離 因應,個人對壓力的承受閾值較低,或者支持系統 的匱乏,或工作的負擔確實沉重[23] 。因此建構諮 商輔導的機制與醫療團隊的支持系統是協助住院醫 師身心健康與專業成長的重要策略。本研究發現五 成以上的醫師害怕做錯事或害怕引起訴訟事件。因 此密切監控指導與回饋住院醫師之醫療措施,將可 增加他們的臨床處置技能,降低醫療錯誤的發生, 以及提升他們照顧病患之信心。另外,提供法律訴 訟案件的討論與相關知識的講授也是教育訓練中的 重要一環。 醫學臨床技能與臨終病人處置之壓力面向,則 約有二至三成醫師經常感受到壓力。這方面相關的 訓練在 PGY1 應是加強與延伸實習時段的訓練,因 此大多數 PGY1 醫師較能勝任與承受壓力。個人因 素壓力中,有四成以上的醫師以醫療決策中須考量 經濟因素覺得壓力很大。可能是在訓練過程中,經 常接收到來自醫院或老師提及目前全民健保制度下 的各種規範與限制有關。 整體而言,本研究結果顯示 PGY1 醫師對工作 滿意程度尚可。相當不滿意與非常不滿意者及相當 滿意與非常滿意者均佔一成。工作壓力與工作滿意 度具有高度相關性,在 Cooper 等學者的研究[20] , 指出工作的沉重要求與病人的期待,工作衝擊到家 庭生活與社交生活,工作或家庭生活受到干擾(例 如應診)及行政文書作業是工作滿意度的負面預測 因子,其解釋變異量共佔 18%。本研究的迴歸分析 結果顯示五種工作壓力面向中,工作情境壓力最能 預測工作的不滿意(其解釋變異量為 19.9%)。而 本研究的工作情境壓力內容涵蓋了 Cooper 的四種 預測變項。 另外,本研究變項尚包括情緒支持與工作時 數,且呈現出顯著的影響力。在情緒支持方面,常 常或一直都感受到適切的情緒支持者佔六成,從來 沒有或很少者佔 5.3%。如果能夠增加醫療團隊成 員互動的機會,營造支持團體以及落實導師與單 位臨床教師的角色,深入了解 PGY1 醫師與及早發 覺 PGY1 醫師的處境與困境,給予及時的支持,將 有助於他們在工作上的愉悅與成就感。工作時數對 工作滿意度的影響亦不容忽視,顯然如前所述每週 工作時數已低於歐美國家的要求,但超時的每日工 作時數意謂著 PGY1 醫師的額外付出。究其原因,
此時間是花費在行政作業或學習照護等文書工作上 或者個人在專業的努力上,有待進一步的研究來釐 清。 住院醫師因工作的壓力影響臨床技能的運作 與表現,進而威脅到病人安全是近年來備受關注的 焦點[18,19] ,國外醫學教育學家呼籲大家重視住院醫 師的壓力預防與介入策略[24-26] 。美國畢業後醫學教 育評鑑委員會(the Accreditation Council for Graduate Medical Education)目前也要求所有教學醫院必須 有住院醫師之輔助計畫(assistance program)[27] 。 為了降低壓力與提供優質的病患照護,Levey[3] 與 Firth-Cozens[16]均建議預防或介入措施應從組織 (organization)與個人兩層面著手。例如在組織層 面上,提供溫馨的學習環境;增進資深住院醫師與 指導老師的指導技巧;減少不必要的夜間任務,提 供諮商服務機制。在個人層面上,不同訓練階段的 專業諮詢;透過講授、工作坊,支持團體或個人諮 商服務學習壓力調適與正向因應技巧等。目前導師 制度是監督與指導 PGY1 醫師的唯一策略,病患醫 療照護的臨床技能與決策之指導應無庸置疑,但是 否能兼顧到住院醫師承受的壓力與情緒變化,是值 得去探索的課題。本研究的結果顯示,除了在組織 機構上對住院醫師的壓力須檢討與努力去減少壓力 源以外,訓練與強化導師的諮詢輔導能力,以便及 早發掘有困擾的住院醫師,及給予及時的介入處置 可能是現階段最重要的課題。有效的諮商輔導機制 須考量其方便性,可近性與隱私性。所以如能落實 導師制度的運作,則 PGY1 住院醫師的工作滿意程 度與身心健康是可預期的。 本研究是台灣第一個深入探討住院醫師壓力源 的研究。研究對象的問卷調查回收率高,亦具代表 性。研究的限制是調查時間相當長,個人壓力感受 的測量可能會隨著適應能力的增強而受到影響。 總結,PGY1 住院醫師主要壓力源是工作情境 壓力與情緒/病患需求壓力,工作情境壓力影響工 作滿意度。諮商輔導機制的建構與確實運作是降低 因住院醫師壓力影響所及之醫療照護品質的主要策 略。
ᇬȁȁᗂ
本研究承蒙行政院國家科學委員會之經費補 助(NSC-95-2516-S-002-010)。感謝研究過程中 所有 PGYI 訓練計畫主持人的支持與協助,及所有 PGY1住院醫師的竭誠參與,使本研究得以順利完 成,僅此誌謝。ՃМᝦ
1. Alexander D, Monk JS, Jonas AP: Occupational stress, personal strain, and coping among residents and faculty members. J Med Educ 1985; 60: 830-9. 2. Hsu K, Marshall V: Prevalence of depression and
distress in a large sample of Canadian residents, interns, and fellows. Am J Psychiatry 1987; 144: 1561-6.
3. Levey RE: Sources of stress for residents and recommendations for programs to assist them. Acad Med 2001; 76: 142-50.
4. Firth-Cozens J: Emotional distress in junior house officers. Br Med J (Clin Res Ed) 1987; 295: 533-6. 5. Butterfield PS: The stress of residency: a review of
the literature. Arch Intern Med 1988; 148: 1428-35. 6. Collier VU, McCue JD, Markus A, et al: Stress
in medical residency: status quo after a decade of reform? Ann Intern Med 2002; 136: 384-90.
7. Tyssen R, Vaglum P, Gronvold NT, et al: Suicidal ideation among medical students and young physicians: a nationwide and prospective study of prevalence and predictors. J Affect Disord 2001; 64: 69-79.
8. Hainer BL, Palesch Y: Symptoms of depression in residents: a South Carolina Family Practice Research Consortium study. Acad Med 1998; 73: 1305-10. 9. Institute of Medicine. Health Professions Education:
A Bridge to Quality. Washington DC: The National Academies Press, 2003.
10. Chu Tzong-Shinn (Eds): Six core competencies in residency training. Taipei: Taiwan Association of Medical Education, 2009. (In Chinese)
11. Sutherland VJ, Cooper CL: Job stress, satisfaction, and mental health among general practitioners before and after introduction of new contract. BMJ 1992; 304: 1545-8.
12. Tyssen R, Vaglum P, Gronvold NT, et al: The impact of job stress and working conditions on mental health problems among junior house officers. A nationwide Norwegian prospective cohort study. Med Educ 2000; 34: 374-84.
13. Warr P, Cook J, Wall T: Scales for the measurement of some work attitudes and aspects of psychological well-being. J Occup Psychol 1979; 52: 129-48. 14. Cohen JS, Patten S: Well-being in residency training:
a survey examining resident physician satisfaction both within and outside of residency training and mental health in Alberta. BMC Med Educ 2005; 5: 21.
15. Toews JA, Lockyer JM, Dobson DJ, et al: Analysis of stress levels among medical students, residents, and graduate students at four Canadian schools of medicine. Acad Med 1997; 72: 997-1002.
16. Firth-Cozens J: Interventions to improve physicians' well-being and patient care. Soc Sci Med 2001; 52: 215-22.
17. Weinger MB, Ancoli-Israel S: Sleep deprivation and clinical performance. JAMA 2002; 287: 955-7. 18. Shanafelt TD, Bradley KA, Wipf JE, et al: Burnout
and self-reported patient care in an internal medicine residency program. Ann Intern Med 2002; 136: 358-67.
19. Williams ES, Manwell LB, Konrad TR, et al: The relationship of organizational culture, stress, satisfaction, and burnout with physician-reported error and suboptimal patient care: results from the MEMO study. Health Care Manage Rev 2007; 32: 203-12.
20. Cooper CL, Rout U, Faragher B: Mental health, job satisfaction, and job stress among general practitioners. BMJ 1989; 298: 366-70.
21. Patient and physician safety and protection act of 2001, HR 3236, 107th Cong (2001).
22. Colford JM, Jr., McPhee SJ: The ravelled sleeve of care. Managing the stresses of residency training. JAMA 1989; 261: 889-93.
23. Lazarus RS, Folkman S: Stress appraisal and coping. New York: Springer; 1984.
24. Pitt E, Rosenthal MM, Gay TL, et al: Mental health services for residents: more important than ever. Acad Med 2004; 79: 840-4.
25. Shapiro SL, Shapiro DE, Schwartz GE: Stress management in medical education: a review of the literature. Acad Med 2000; 75: 748-59.
26. Dabrow S, Russell S, Ackley K, et al: Combating the stress of residency: one school's approach. Acad Med 2006; 81: 436-9.
27. Graduate medical education directory 2002-2003. Chicago: American Medical Association; 2003.
Purpose: The first year of postgraduate
residency (PGY1) is the most stressful year. The aim of this study was to investigate the job stressors among PGY1 residents, to measure their job satisfaction and to explore any influencing factors. Methods: PGY1 residents in the academic
year 2006 were the study subjects. The study was conducted from January to June 2007. The job stress and satisfaction data were collected via a questionnaire survey. The job stressors were examined by factor analysis. Stepwise multivariate regression analysis was used to explore the predictors related to job satisfaction. Results: A
total of 555 PGY1 residents (response rate 90.0%) completed the survey. Five stressors were identifi ed including working situational stress, clinical skill stress, emotional pressure/demands from patients, dealing with family and friends’ illness, and personal stress; these explained 55.7% of the total variance. Overall, 38.0 % of the residents frequently or always perceived the presence of job stress. Working situational stress and the emotional pressure/demands from patients were the main
stressors. Close to 70% of the residents felt they had insufficient sleep or that the need to be constantly alert on duty was very stressful. Furthermore, more than 60% of the residents perceived that there was excess pressure due to the clerical/administrative activities or an excessive workload. Finally, 55.0% of the residents felt threatened by the possibility of making a mistake or perceived the threat of litigation. The important signifi cant predictors of job satisfaction were working situational stress, which explained 19.9% of the variance and emotional support, which explained 9.7% of variance.
Conclusion: PGY1 residents perceived that most
of their stress came from their working situation and the emotion pressure/demands of patients. The presence of working situational stress affected their job satisfaction. Developing assistance services for these residents or reinforcing the functioning of the current mentoring system are recommended in order to promote the well-being of these residents, which, in turn, would improve the quality of medical care provided. (Full text in Chinese)
A Nationwide Survey in Taiwan
Bee-Horng Lue, M.D.
1,2, Meei-Ying Kao, Ph.D.
3,
Hsiu-Jung Chen, Ph.D.
4, Chang-Wei Wang, B.S.
1Key words: job stress, job satisfaction, first postgraduate year residents. ( J Med Education 2009; 13: 113~121 )
1
Department of Family Medicine; 2 Department of Social Medicine, National Taiwan University College of Medicine; 3 Graduate Institute of Humanities in Medicine, Taipei Medical University; 4 Department of Educational Psychology and Counseling, National Taiwan Normal University.
Received: 22 April 2009; Accepted: 30 June 2009.
Correspondence to: Hsiu-Jung Chen, Department of Educational Psychology and Counseling, National Taiwan Normal University. No.162, Sec. 1, Heping E. Rd., Da-an District, Taipei City 10610, Taiwan.