國立臺灣大學醫學院臨床醫學研究所 碩士論文
Graduate Institute of Clinical Medicine
College of Medicine
National Taiwan University Master Thesis
大腸憩室症與大腸激躁症之相關性研究
The association between colonic diverticulosis and irritable bowel syndrome
劉庭旭 Ting-Hsu Liu
指導教授﹕吳明賢 教授
Advisor: Ming-Shiang Wu, Professor, M.D./Ph.D.
中華民國 106 年 02 月
Febuary 2017
大腸憩室症與大腸激躁症之相關性研究
劉庭旭 / 衛生福利部台北醫院
中文摘要
研究背景:
大腸激躁症(irritable bowel syndrome, IBS)是常見的腸胃道功能性疾病。大腸激 躁症與一些器質性的疾病於臨床表現及病生理機轉有重疊的現象。在近來的研 究發現,大腸憩室症(colonic diverticulosis, CD),特別是左側的大腸憩室症,有 較高的風險會患有大腸激躁症。然而在亞洲人族群的研究中,有相衝突的結果 發現,也缺乏大型前瞻性研究證實。慢性低度發炎及腸道微生物叢的改變在有 症狀的大腸憩室疾病(diverticular disease, DD)的病生理機轉中扮演重要角色。近 來許多研究探討使用 5-ASA,抗生素或益生菌來治療慢性憩室疾病的效果。如 何區分大腸激躁症與慢性有症狀的大腸憩室疾病以給予適當的治療實有其臨床 上的重要性。腹痛持續大於 24 小時的這個臨床症狀曾被指出能鑑別大腸激躁症 與有症狀的大腸憩室疾病,然而其有效性仍需要證實。
目的:
進行前瞻性研究以了解大腸激躁症與大腸憩室症之間的關聯性於台灣人族群中 是否存在。驗證腹痛持續大於 24 小時的這個臨床症狀是否能鑑別大腸激躁症與 有症狀的大腸憩室疾病。
方法:
針對於本院接受全大腸鏡檢查的病人進行收案。以問卷調查方式來診斷大腸激 躁症(根據 Rome III criteria) 並了解病人腹痛的特徵。比較 IBS 及 non-IBS 兩組 病人間大腸憩室症(CD)的盛行率是否有差異。比較 CD 及 non-CD 兩組病人間 IBS 的盛行率是否有差異。比較單純只有 IBS (pure IBS)及單純只有(有症狀)大
腸憩室疾病(pure DD)的兩組病人間,腹痛持續大於 24 小時的這個臨床症狀的 盛行率是否有差異。
結果:
本研究於 2016 年 3 月至 11 月間共收案 1502 人,其中 119 人因符合排除條件而 被排除,最後有 1383 人進入結果分析。病人的平均年齡為 55.8±13.1 歲,男女 比為 1.58:1。收集的個案中 6.6% 符合 Rome III criteria 中大腸激躁症(IBS)定義,
17.1% 有大腸憩室症,以右側憩室症為主,佔所有憩室症中的 69%。IBS 及 non-IBS 兩組間不論是在總體(Diverticulosis, 14.3% vs 17.3%, P=0.455)、右側(RD, 8.8% vs 12.0%, P=0.359)或是左側(LD, 2.2% vs 2.6%, P=0.435)憩室症的盛行率 都未達統計學上顯著差別。在 IBS 組中,有顯著較高的較 BSRS-5 score。年輕 (<65 歲)的 IBS 族群中,有較少的大腸腺瘤(OR:0.43, P=0.012)。大腸憩室症(CD) 及無大腸憩室症(non-CD)兩組間在 IBS 的盛行率上都無顯著差異(5.5% vs 6.8%, P=0.455)。在 CD 組中,年齡大是最主要的危險因子(OR:2.04,P=0.000)。喝酒 (OR:1.48,P=0.037)及較高的 BMI(OR:1.09, P=0.000)亦是大腸憩室症的危險因 子。在所有大腸憩室憩室症(CD)病人中,有 28.3% 是伴有腹痛症狀的大腸憩室 疾病(DD),有顯著較高的 BSRS-5 score。在單純 IBS 及單純有症狀大腸憩室疾 病兩組間疼痛的持續時間、嚴重度及位置均無統計上顯著差異。
結論:
台灣人族群的大腸憩室症好發於右側。我們針對台灣人族群的研究中並未在大 腸憩室症(不論是左側或右側)與大腸激躁症間看到關聯性。使用腹痛超過 24 小 時的臨床症狀來鑑別 IBS 與有症狀的大腸憩室疾病的論述未能得到驗證。在 IBS 病人中有顯著較高的心理社會壓力。在較年輕的 IBS 患者中,大腸腺瘤的盛行 率較低。年齡(大)是大腸憩室症最主要的危險因子。喝酒及肥胖會顯著增加大 腸憩室症的風險。有症狀大腸憩室疾病的族群,須注意因慢性腹痛所造成的心 理影響。
關鍵詞: 大腸激躁症、大腸憩室症、憩室疾病、腹痛、盛行率
The association between colonic diverticulosis and irritable bowel syndrome
Liu, Ting-Hsu / Taipei Hospital, Ministry of Health and Welfare
Abstract
Background:
Irritable bowel syndrome (IBS) is a common functional GI disorder. The clinical presentation and pathophysiologic mechanisms of IBS has overlap with some organic GI disease. Recent researches showed the presence of colonic diverticulosis (CD), especially left-sided diverticulosis, was associated with higher risk of IBS.
However, conflicting findings were observed in the studies conducted in Asian population. Larger prospective studies are needed to confirm the association. Low grade inflammation and alteration in gut microbiota play important role in the pathophysiologic mechanism of symptomatic diverticular disease (DD). Recent studies have focused on the use of 5-ASA, antibiotics and probiotics in treating chronic diverticular disease. It is of clinical importance to distinguish IBS and chronic symptomatic diverticular disease to define the appropriate treatment. The effectiveness of abdominal pain lasting for more than 24 hours could discriminate IBS and DD had been proposed. Further validation is needed.
Objectives:
We conducted prospective study to 1. clarify the association between IBS and CD in Taiwanese population; 2. Validate the effectiveness of abdominal pain lasting for more than 24 hours in differentiating IBS and DD.
Methods:
We enrolled patients undergoing colonoscopy in single hospital. Questionnaire was applied to identify IBS patients (according to Rome III criteria) and to collect the characteristics of abdominal pain. We compared 1. the prevalence of CD in the IBS
and non-IBS groups. 2. The prevalence of the clinical symptom of abdominal pain lasting for more than 24 hours in pure (no overlap) IBS and pure DD groups.
Results:
We initially enrolled 1502 subjects during March 2016 to November 2016 and 119 subjects met the exclusion criteria. A final total of 1383 subjects were enrolled for analysis. The mean age of the patients was 55.8±13.1 and the male to female ratio was 1.58:1. IBS was identified in 6.6% and CD was observed in 17.1% of the patients. Right-sided diverticulosis is predominant (69% of all CD). There was no statistically significant difference between the prevalence of whole CD (14.3% vs 17.3%, P=0.455), right-sided CD(8.8% vs 12.0%, P=0.359) and left-sided CD(2.2%
vs 2.6%, P=0.435) in IBS and non-IBS groups. Significantly higher BSRS-5 score was observed in the IBS group. In younger (age<65) IBS patients, the prevalence of colonic adenoma was lower (OR:0.43, P=0.012). There was no significant difference between the prevalence of IBS in CD and non-CD groups (5.5% vs 6.8%, P=0.455).
Older age was the most important risk factor for CD (OR:2.04,P=0.000). Alcohol consumption (OR:1.48,P=0.037) and higher BMI (OR:1.09, P=0.000) also increased the risk of CD. Within the whole diverticulosis group, abdominal pain was
complained in 28.3% of the patients. Higher BSRS-5 score was observed in this subgroup (symptomatic diverticular disease). The pain duration, severity and location could not differentiate pure IBS and pure symptomatic DD in our study.
Conclusions:
In Taiwaness population, right-sided diverticulosis is predominant. The association between colonic diveticulosis and IBS was not observed in our study. The
effectiveness of abdominal pain lasting for more than 24 hours in differentiating IBS and DD also could not be validated. IBS patients had higher psychosocial stress.
Younger IBS patients had lower adenoma prevalence. Older age is the most
important risk factor of CD. Alcohol consumption and obesity increased the risk of CD. Patients with symptomatic diverticular disease had higher psychosocial stress.
Keywords: irritable bowel syndrome (IBS), colonic diverticulosis, diverticular disease, abdominal pain, prevalence
目 錄
口試委員會審定書……… i
中文摘要……… ii
英文摘要………. iv
第一章 研究背景……….. 1
第二章 研究方法……….. 4
第三章 研究結果……….. 7
第 四 章 討論……… ……….. 10
第五章 未來展望……….. 14
第六章 論文英文簡述………. 15
參考文獻………..………….... 20
圖 1 大腸憩室症之分類及學術名詞義………. 24
圖 2 大腸憩室疾病可能之病生理機轉及其相關治療………. 24
圖 3 收案流程圖………. 25
腸胃道症狀及心理健康問卷……… 26
圖 4 收案流程圖---最終收案結果………. 30
表 1 病人特色………. 31
表 2 有大腸激躁症及無大腸激躁症群之比較………. 32
表 3-1 大腸激躁症危險因子之多變數迴歸分析………...……. 33
表 3-2、表 3-3 大腸激躁症危險因子之多變數迴歸分析---依年齡分層……… 34
表 4 有大腸憩室症及無大腸憩室症群組之比較……….. 35
表 5-1 大腸憩室症危險因子之多變數迴歸分析……… 36
表 5-2、表 5-3 大腸憩室症危險因子之多變數迴歸分析---依年齡分層……….…… 37
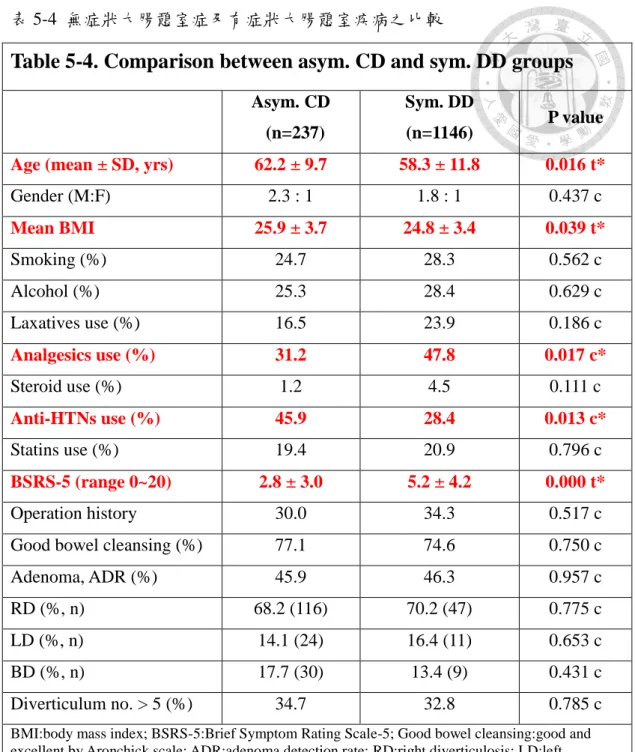
表 5-4 無症狀大腸憩室症及有症狀大腸憩室疾病之比較……….…….…….…….… 38
表 5-5 有症狀大腸憩室疾病危險因子之多變數迴歸分析……….…….…….…….… 39
表 6 大腸激躁症及有症狀大腸憩室疾病兩群組間腹痛特色之比較………... 40
表 7 腹痛特色之迴歸分析………..………. 41 表 8-1 大腸激躁症及有症狀左側/雙側大腸憩室疾病兩群組間腹痛特色之比較… 42 表 8-2 大腸激躁症及有症狀右側大腸憩室疾病兩群組間腹痛特色之比較………. 43
第一章 研究背景:
大腸激躁症(irritable bowel syndrome, IBS)是常見的功能性胃腸障礙。其臨床表 現是反覆性的腹痛不適並伴隨著大便型態及頻率的改變,而腹痛會因排便得到 改善。大腸激躁症的盛行率在西方國家如英國、美國約在 10-15%。在亞洲已開 發國家如日本、新加坡的盛行率也落在 10-15%,而印度則只有 4% (Gwee et al.
2009)。過去認為大腸激躁症是飲食或情緒所引起的單純”功能性”的障礙。然而
有愈來愈多的研究顯示大腸激躁症與許多的大腸器質性疾病有相關。
例如在 Dunlop SP 的研究發現,在感染性大腸炎後的部分患者於恢復後會產生”
感染後大腸激躁症(Post-infectious IBS)”。這種狀況可能和大腸黏膜中
enterochromaffin cells 的增生有關(Dunlop SP et al. 2003)。在 Halpin SJ 的研究發現,
在發炎性腸病(inflammatory bowel disease, IBD) 的患者中,即使在發炎經過治 療緩解後,符合大腸激躁症診斷標準的患者仍顯著高於無 IBD 的族群(Halpin SJ et al. 2012)。
大腸憩室症(colonic diverticulosis)是指大腸有憩室的出現。一般認為大腸憩室的 產生是因腸黏膜隨年齡增長的退化及腸內壓力增加,而造成腸黏膜於弱處的向 外膨出。大腸憩室症的盛行率會隨年齡增長而提升,在 60 歲以下盛行率約 20-30%,而在 80 歲以上則會高達 70% (Everhart et al. 2009)。大腸憩室症的定義涵 蓋無症狀的憩室症(asymptomatic diverticulosis)及有症狀的憩室疾病(diverticular disease, DD),其分類如圖 1 所示(Strate LL 2012)。
憩室疾病(DD)過去認為是一種急性疾病,由一次或數次間斷的急性憩室炎 (diverticulitis)所構成,發作間並無腸胃症狀。然而在之後的研究發現,部分患 者可能有類似典型大腸激躁症的慢性腸胃道症狀,甚至因慢性腹痛而造成憂 鬱、焦慮(Humes DJ et al. 2008),影響到健康相關之生活品質(HRQOL)(Bolster LT et al.
2003; Comparato G et al. 2007)。
近來有一些研究探討大腸憩室症與大腸激躁症之間的關聯性。在 Jung 針對西方 人族群的研究發現,有大腸激躁症,特別是以腹瀉為主的大腸激躁症患者,有 較高的機會有大腸憩室症(diverticulosis)(Jung HK et al. 2010)。
然而大腸憩室症有種族上的差異。西方人族群的大腸憩室多發生在左側大腸,
主要是乙狀結腸(55-95%);而亞洲人族群的大腸憩室則好發在右側(70%)(Hobson
KG et al. 2004)。故西方人族群的發現,在亞洲人族群未必如是。
在 Gu HX 針對中國人族群所做的回溯性研究發現,在有大腸激躁症的族群(IBS, n=3332),大腸憩室症(CD)的盛行率反而較對照組低 (non-IBS, n=1588)(Gu HX et al. 2011)。在 Sirinthornpunya S 針對 150 位 (IBS, n=75 vs. non-IBS, n=75) 泰國人 族群所做的一個較小型前瞻性研究發現,有大腸激躁症患者有較高的機會有大 腸憩室症(CD)( Sirinthornpunya S et al. 2014)。另一個由 Yamada E 針對 1009 位 (IBS, n=76 vs. non-IBS, n=933) 日本人族群所做的研究則更進一步發現,左側及雙側 的大腸憩室症(CD)患者有較高的風險患有大腸激躁症,而右側大腸憩室症則和 大腸激躁症無相關(Yamada E et al. 2014)。由於這些相衝突的發現,以及在後兩個 前瞻性研究中,大腸激躁症患者數目較少,大腸激躁症及大腸憩室症於亞洲人 族群的相關性仍需更多、更大規模的研究。而台灣目前亦無相關研究資料發表。
另外,關於大腸憩室疾病(DD)的病生理機轉,過去認為是由於而糞石或未消化 的食物 (如種子) 落入憩室造成阻塞或局部黏膜的損傷,而引起細菌過度繁 殖、組織發炎、缺血、壞死、甚至穿孔。近來的理論則指出慢性低度的發炎、
腸道內共生的微生物叢改變、臟器對痛覺的高度敏感(visceral hypersensitivity) 及大腸蠕動異常是引發大腸憩室疾病(DD)的原因(Strate LL et al.2012)。而針對慢性 的大腸憩室疾病的治療,已有許多過去的研究指出,可使用膳食纖維來改善大 腸蠕動及腸道微生物叢(Aldoori WH et al. 1994; Crowe FL et al. 2011);使用抗發炎藥物 5-ASA (mesalamine) 來控制大腸低度發炎(正反研究結果均有,仍待大規模研究 證實)(Trepsi E et al. 1999; Di Mario F et al. 2005; Gatta L et al. 2010; Raskin JB et al. 2014);使用 腸道吸收差的廣效性抗生素 Rifaximinx 及益生菌來改變腸道微生物叢(Tursi A et al. 2002; Lamiki P et al. 2010; Bianchi M et al. 2011)。如圖 2 所示(Strate LL et al. 2012)。 所以如何鑑別有症狀的慢性大腸憩室疾病(chronic recurrent diverticulitis and symptomatic uncomplicated diverticular disease, SUDD) 及單純的大腸激躁症,以 給予適當或避免不必要的治療實有其臨床意義。
在 Tursi A 的研究發現,在大部分大腸憩室疾病(DD)患者的大腸切片可發現黏膜 有發炎反應而大腸激躁症則沒有(Tursi A et al. 2008)。在 Tursi A 的另一個研究發
現,糞便中的 calprotectin 可以偵測在大腸憩室疾病(DD)患者的大腸發炎反應,
來和大腸激躁症做鑑別,並可以用來評估治療反應(Tursi A et al. 2009)。而義大利 學者 Cuomo R 所執行的研究發現,腹痛持續超過 24 小時的這個臨床表現可以 區別有症狀的大腸憩室疾病(DD)及大腸激躁症(Cuomo R et al. 2013)。然而這個發現 仍需要進一步的驗證。
研究問題:
1. 大腸激躁症與大腸憩室症(CD)之間的關聯性,是否存在於台灣人族群。
2. 腹痛持續大於 24 小時的這個臨床表現,是否能鑑別有症狀的大腸憩室疾病 (DD)及大腸激躁症。
第二章 研究方法
本研究是於單一醫院所進行之前瞻性研究。
受試者選擇標準:
1. 年滿 20 歲以上的台灣人。
2. 預定接受大腸鏡檢查的門診、住院病患或健康檢查受檢者均可成為收案對 象。
3. 收案前須先取得知情同意書。
4. 排除條件: 如果病患有任何下列任何一項將被排除: (1)腹腔或骨盆腔惡性 腫瘤,(2)大腸檢查後發現有器質性疾病,如發炎性腸病、大腸炎…等, (3) 過去曾接受過腸道切除手術。
資料的蒐集及診斷確立:
1. 符合收案標準之受試者於接受大腸鏡檢查前會接受問卷調查取得相關資 訊。根據問卷上的記錄判定受試者是否有大腸激躁症。
2. 受試者的性別、年齡、身高體重、腹腔或骨盆腔手術史(有或無)、抽菸及 飲酒習慣(有或無)、藥物使用(瀉藥、非固醇類消炎止痛藥、類固醇、降血 壓藥物、降膽固醇藥物) 會加以記錄。
3. 大腸激躁症之診斷標準是依據 Rome III criteria。反覆性腹痛或腹部不適,
至少每個星期有 2 天以上。同時下列三項描述至少需有兩項符合: (1)腹痛 在解便後得到緩解,(2)腹痛的發生和大便頻率改變相關,(3)腹痛的發生和 大便型態(外觀)的改變相關。大便之型態是用 Bristol scale 來評估。大腸激 躁症會再區分為四種亞型: (1)腹瀉型大腸激躁症(D-IBS): 稀水便占排便的 25%以上,且硬便占排便的 25%以下,(2)便秘型大腸激躁症(C-IBS): 硬便 占排便的 25%以上,且稀水便占排便的 25%以下,(3)混合型大腸激躁症 (M-IBS): 符合 D-IBS 及 C-IBS 的標準,(4)無法分類至大腸激躁症(U-IBS):
無法符合上述三亞型分類標準的 IBS。
4. 腹痛的特徵 (嚴重度、頻率、持續時間、位置) 會被量化記錄。(1)腹痛嚴
重度分為五級(從無痛到非常嚴重),(2)腹痛頻率分為五級(從一個月發作小 於一次到每天發作),(3)腹痛持續時間分為三級(小於 1 小時、數小時、大 於 1 天),(4)腹痛位置分為肚臍上、肚臍下、肚臍上下都有、不固定位置或 無法明確定位。
5. 大腸憩室症的診斷是根據大腸鏡的發現。大腸憩室的數量(分為無、五個以 下、五個以上) 及位置(右側大腸、左側大腸、雙側) 將被記載。
6. 大腸鏡檢品質相關指標: 盲腸到達率(cecal intubation rate)、清腸準備乾淨程 度(bowel cleansing, by Aronchick scale)及腺瘤偵查率(adenoma detection rate) 將加以計算。
7. 受試者的精神壓力會以簡式心理健康量表(5-item Brief Symptom Rating Scale, 5-BSRS) 做評估。
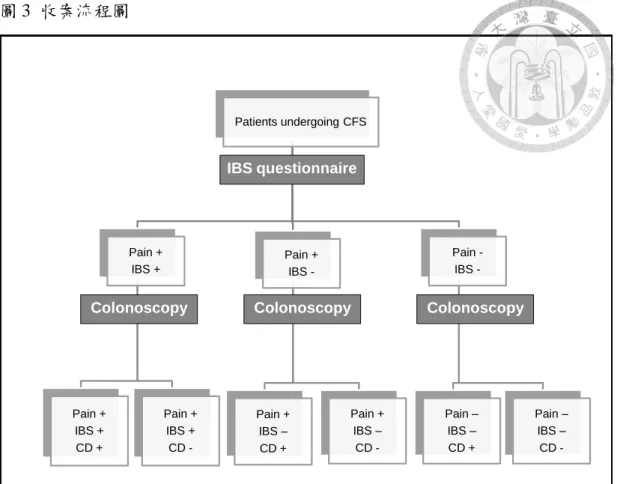
研究收案之流程圖(圖 3)及問卷參見圖表章節。
樣本數估算:
1. 假設大腸激躁症在台灣一般族群中盛行率約 10%。
2. 假設左側或雙側大腸憩室症在 IBS 及 non-IBS 組的盛行率分別為 20%及 10%。
3. 在雙尾檢定,若設定 power 為 90%,而 significance level 為 5%,IBS 及 non-IBS 病人數比為 1 比 9,則估計所需的樣本數分別為 IBS 組 149 人,
non-IBS 組 1341 人。
4. 故預計收案 1500 人。
統計分析:
1. 比較 IBS 及 non-IBS 兩組病人間大腸憩室症(CD)的盛行率是否有差異。
2. 比較 CD 及 non-CD 兩組病人間大腸激躁症的盛行率是否有差異。
3. 比較單純只有 IBS (有腹痛, 符合 IBS 診斷標準, 無大腸憩室症) 及單純只有 大腸憩室疾病 (有腹痛, 不符 IBS 診斷標準, 有大腸憩室症) 的兩組病人 間,腹痛持續大於 24 小時的這個臨床症狀的盛行率是否有差異。
4. 各群組間的類別資料會使用卡方分析來比較,連續性資料會使用 Student t test
來比較。 P 值小於 0.05 為統計顯著。
5. P 值小於 0.05 的變項,會進一步使用多變數迴歸分析,計算 Odds ratio 及 95%
信賴區間,試圖找出 IBS 及大腸憩室症的可能危險因子。
第三章 研究結果:
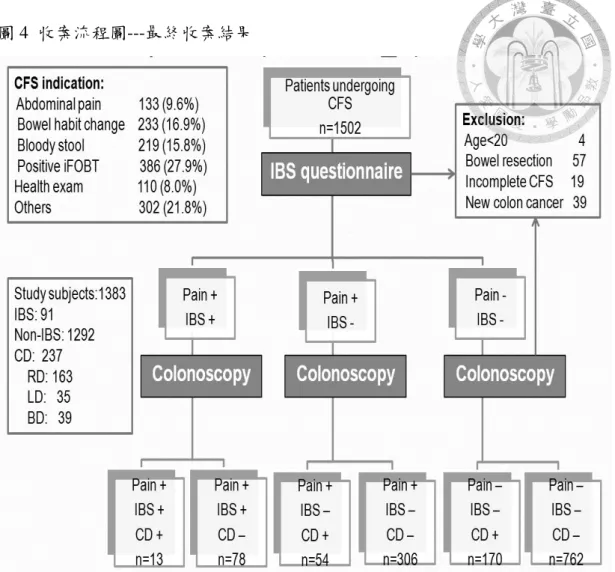
本研究於 2016 年 3 月至 11 月間共收案 1502 人,其中 119 人因符合排除條件而 被排除(年齡小於 20 歲 4 人、腸道切除史 57 人、未完成全大腸鏡檢 19 人、新 診斷大腸癌 39 人),最後有 1383 人進入結果分析(圖 4)。病人接受大腸鏡的適 應症中,以免疫糞便潛血檢查(iFOBT)陽性為最大宗,佔 27.9%。因腹痛、排便 習慣改變、血便等腸胃道症狀而受檢的共佔 42.3%。大腸鏡檢品質相關指標: 於 1502 人次的檢查中,盲腸到達率(cecal intubation rate)為 98.7%;於收案的 1383 人中,清腸準備乾淨程度以 Aronchick scale 評分為優良(excellent)及良(good)兩 個等級的合計占 72.5%;腺瘤偵查率(adenoma detection rate)為 38.4%。
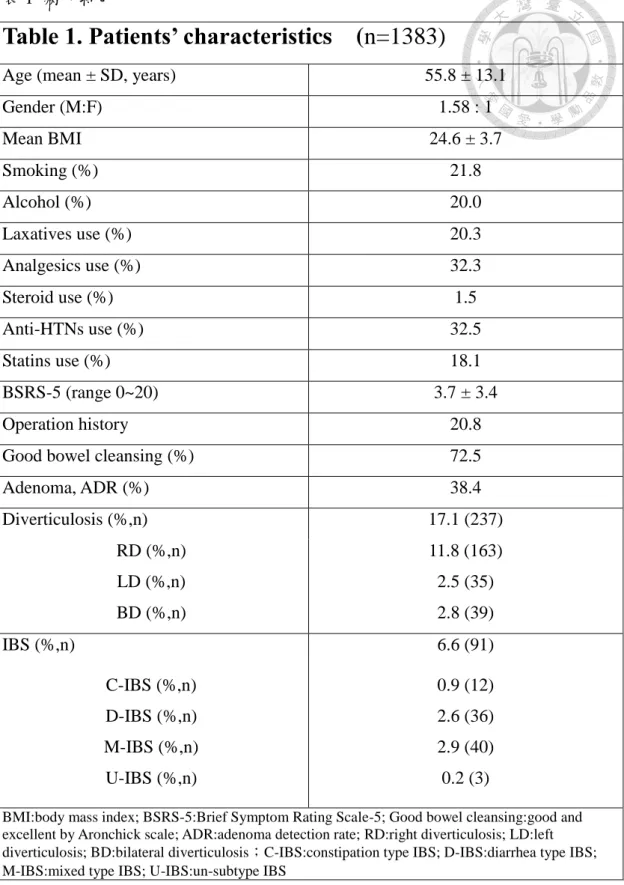
收案的 1383 位病人特色如(表 1)所示: 病人的平均年齡為 55.8±13.1 歲(涵蓋年齡 20 到 91 歲),男女比為 1.58:1。其中 6.6% (n=91)可符合 Rome III criteria 中較嚴 格(腹部不適頻率大於每周 1 天以上)的大腸激躁症(IBS)定義。在 IBS 的次分型 中,以混和型(M-IBS, n=40)及腹瀉型(D-IBS, n=36)為主,各佔所有 IBS 中的 44.0%及 39.6%。病人中 17.1% (n=237)有憩室症,以右側憩室症為主(n=163),
佔所有憩室症中的 69%。而左側大腸憩室症所佔的比率會隨著年齡增加而上 升,在小於 65 歲與大於 65 歲的大腸憩室症群組中所佔比率分別為 10.7% 及 21.6% (p=0.000)。在所有有憩室症的病人中,有 28.3% (n=67) 伴隨有腹痛症狀,
其中的 9.7% (n=23) 受腹痛問題困擾的時間超過 6 個月。
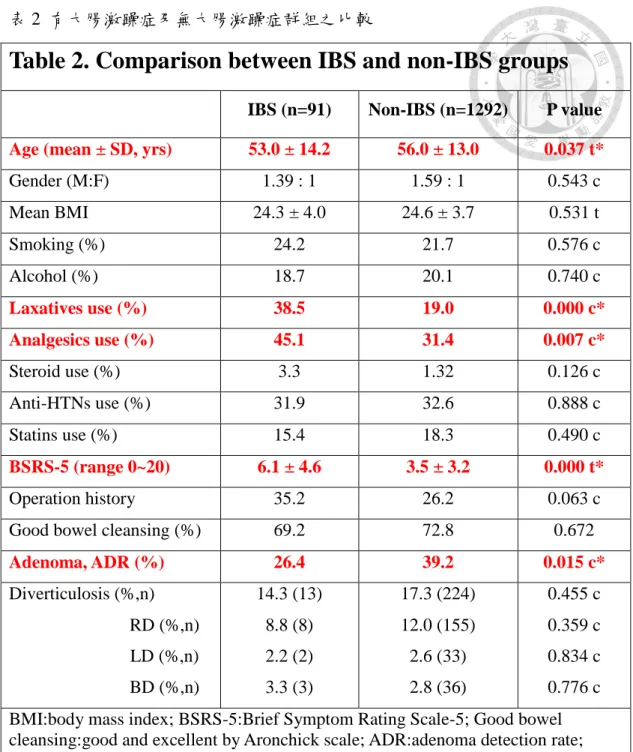
比較 IBS 及 non-IBS 群組間的差異(表 2): 兩組間於性別比率、BMI、手術史方 面無統計顯著差異。IBS 組年齡較輕(53.0. vs 56.0, P=0.037),有顯著較高的比率 使用軟便藥(38.5% vs 19.0%, P=0.000)及止痛藥(45.1% vs 31.4%, P=0.007)。IBS 組 BSRS-5 score 較高,心理壓力較大(6.1 vs 3.5, P=0.000)。兩組間雖腸道清潔度 無差異,但 non-IBS 組較多人有大腸腺瘤(39.2% vs 26.4%)。兩組間不論是在總 體(Diverticulosis, 14.3% vs 17.3%, P=0.455)、右側(RD, 8.8% vs 12.0%, P=0.359) 或是左側(LD, 2.2% vs 2.6%, P=0.435)憩室症的盛行率都未達統計學上顯著差
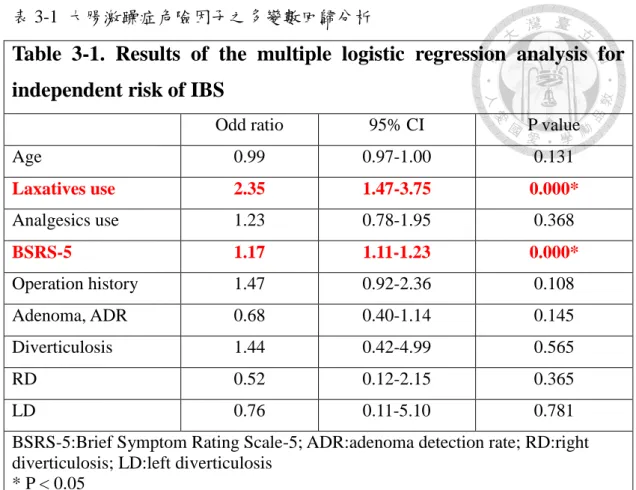
別。將年齡、軟便劑使用、止痛藥使用、BSRS-5 score、手術史、憩室症有無 等變數放入迴歸分析後,軟便劑使用及高的 BSRS-5 分數仍和 IBS 呈顯著相關 (表 3-1)。將病人依年齡大於 65 歲與否分成兩個次群組,分別做分析後發現: 在 較年輕(age<65)的 IBS 次群組中,有較多的軟便劑使用、較高的 BSRS-5 score 及較少的大腸腺瘤(表 3-2);而在較年長(age≧65) 的 IBS 次群組中,只有 BSRS-5 score 較高呈現顯著差異(表 3-3)。CD 不論是在大於 65 歲或小於 65 歲的次群組 中,和 IBS 都無關連。
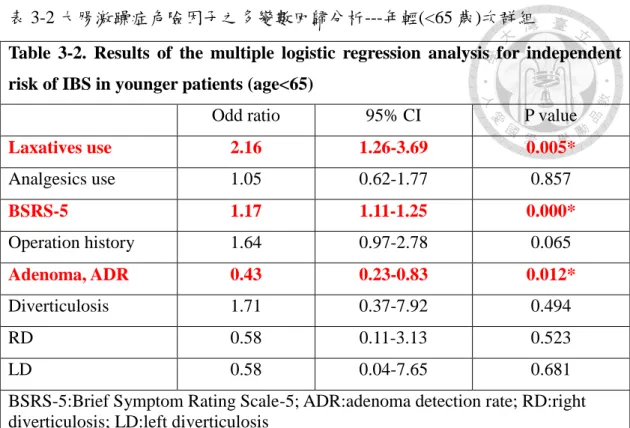
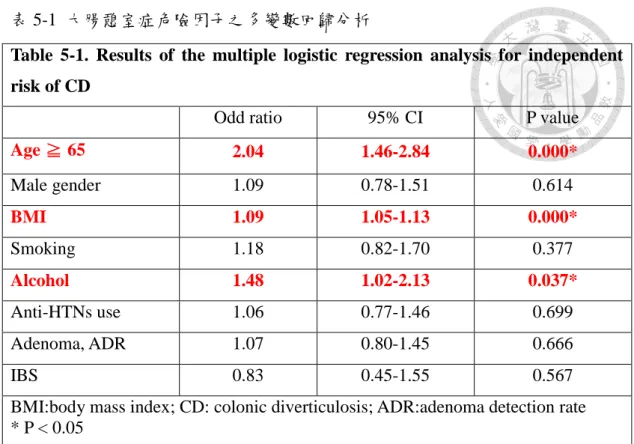
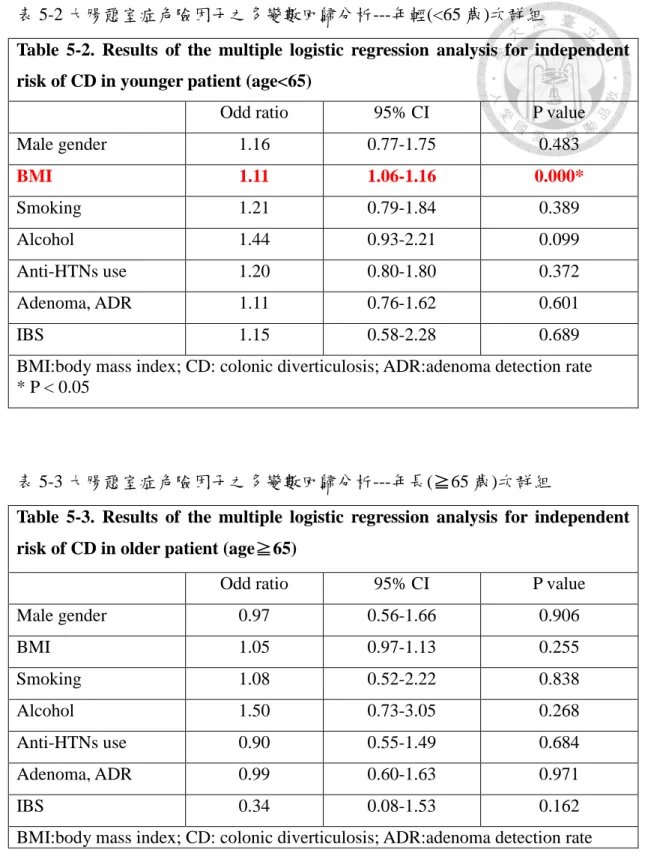
比較有大腸憩室症(CD)及無大腸憩室症(non-CD)族群間的差異(表 4): 兩組在年 齡(61.1 vs 54.7, P=0.000)、性別比率(P=0.020)、BMI(25.6 vs 24.3, P=0.000)、酒 精使用(26.2% vs 18.8%, P=0.010)及降血壓藥物使用(40.9% vs 30.8%, P=0.002) 等變數呈顯著差異。兩組間雖腸道清潔度無差異,但 CD 組較多人有大腸腺瘤 (46.0% vs 36.8%, P=0.008)。而在 IBS 的盛行率上,兩組間無統計學上顯著差異 (5.5% vs 6.8%, P=0.455)。將年齡、性別、BMI、抽菸、酒精使用、降血壓藥物 使用、大腸腺瘤有無及 IBS 有無等變數放入迴歸分析後,年齡較大、BMI 較高 及酒精使用仍和 CD 呈現顯著相關(表 5-1)。將病人依年齡大於 65 歲與否分成 兩個次群組,分別做分析後發現: 在較年輕(age<65)的 CD 次群組中,BMI 顯著 較高(表 5-2);而在較年長(age≧65) 的 CD 次群組中,在各變項間都沒有顯著 差異(表 5-3)。IBS 不論是在年長或年輕的次群組分析中,和 CD 都沒有關連。
比較無症狀大腸憩室症(asymptomatic CD)及有症狀大腸憩室疾病(symptomatic DD)兩群組間的差異(表 5-4): 兩組在年齡(62.2 vs 58.3, P=0.016)、BMI(25.9 vs 24.8, P=0.039)、止痛藥使用(31.2% vs 47.8%, P=0.017)、降血壓藥物使用(45.9% vs 28.4%, P=0.013)及 BSRS-5 score (2.8 vs 5.2, P=0.000)等變數呈顯著差異。將年 齡、性別、BMI、抽菸、酒精使用、止痛藥使用、類固醇使用、降血壓藥物使 用、降血脂藥物使及 BSRS-5 等變數放入多變數迴歸分析後,僅剩(較高的) BSRS-5 score 和有症狀的大腸憩室疾病成顯著相關(表 5-5)。
比較單純大腸激躁症 (pure IBS) 及單純有症狀憩室疾病 (pure DD) 兩群組間 疼痛的特色(表 6): pure IBS 組年齡顯著低於 pure DD 組,但兩群組間不論是疼 痛的持續時間、嚴重度及位置都無統計上顯著差異(表 6、7)。將 pure DD 再依 憩室的位置分成右側(pure RD)及左側/雙側(pure LD/BD)兩個次群組後,分別和 pure IBS 做比較後發現,不論是左側或是右側的大腸憩室疾病,其腹痛表現都 無法與大腸激躁症區分 (表 8-1、8-2)。
第四章 討論:
在我們的研究台灣人族群中,大腸激躁症(IBS)的盛行率為 6.6%,以混和型 (M-IBS)及腹瀉型(D-IBS)為主,各佔所有 IBS 中的 44.0%及 39.6%。而大腸憩室 症(CD)的盛行率為 17.1% ,以右側憩室症為主,佔所有憩室症中的 69%。此發 現符合過去研究中,亞洲人種以右側憩室症為主的特色。然而,我們並未在大 腸憩室症(不論是左側或右側)與大腸激躁症間看到關聯性。可能原因論述如下:
1. 本研究族群的平均年齡較低:
在 Yamada E 所研究的日本人族群,平均年齡為 64.2 歲,大腸憩室症的盛行 率為高達 40.2% (Yamada E et al. 2014)。而本研究族群的平均年齡為僅有 55.8 歲。年齡的差別可一部分解釋為何在本研究中大腸憩室症的盛行率僅有 17.1%。我們嘗試針對年齡做分層分析,但仍無法於年輕(age<65)或年長 (age≧65)的次群組中,看到 IBS 與大腸憩室症間的關聯。
2. 研究族群經過不同程度的篩選:
在 Yamada E 於日本人族群的研究中,IBS 的盛行率為 7.5%,病人接受大腸 鏡的原因都為大腸癌篩檢,文中未提及其研究族群中有腹痛或腸胃道症狀的
比率 (Yamada E et al. 2014)。本研究族群 IBS 的盛行率為 6.6%,病人接受大腸
鏡的適應症中,以免疫糞便潛血檢查(iFOBT)陽性為最大宗,佔 27.9%,因 腹痛、排便習慣改變、血便等腸胃道症狀而受檢的共佔 42.3%。兩個研究族 群經過不同程度的篩選,均可能與 general population 有差異,研究結果亦可 能不同。
3. 大腸憩室症的盛行率於本研究中可能被低估:
除年齡因素外,造成本研究中大腸憩室盛行率偏低的原因可能在於大腸鏡對 於大腸憩室偵測率偏低。大腸鏡對於小型病灶或憩室的偵測會因腸道清潔程 度而受影響。一般高品質的大腸鏡檢其盲腸到達率(cecal intubation rate)應在 95%以上,腸道準備乾淨程度以 Aronchick scale 評分為 excellent 及 good 兩 個等級合計應在 85-90%以上,而腺瘤偵查率(adenoma detection rate)應在
率(adenoma detection rate)為良好的 38.4%,但腸道準備乾淨程度僅有
72.5%,可能會影響到憩室的偵測率。Yamada E 於其發表中並未提及其研究 中大腸鏡檢的品質指標,但其研究使用了附加於大腸鏡鏡頭前的透明遮罩,
可能因此改善了憩室偵測率。過去即有研究指出使用透明遮罩可以提升小型 病灶的偵測率 (Kondo S et al. 2007),此一方法或許能供後續的研究者借鏡。再 者,過去有研究認為大腸鏡對於左側大腸憩室的偵測率低於大腸鋇劑灌注攝
影 (Niikura R et al. 2013)。然而由於大腸鏡檢在台灣取得的方便性與可同時進行
內視鏡治療的優點,大腸鏡檢已取代大多數大腸鋇劑灌注攝影的角色,如果 要以鋇劑攝影做為大腸憩室有無的確診標準,可能需要長時間或多中心的收 案才可行。
關於 IBS 與 non-IBS 族群的比較:
過去的研究發現心理社會的因素和大腸激躁症的產生有關 (Drossman DA et al.
1988)。本研究使用簡式心理健康量表(BSRS-5)也看到在 IBS 族群中,不論年齡
長幼,都有顯著較高的 BSRS-5 score,確實有較大的心理壓力存在。
在我們的研究中,較年輕(age<65) 的 IBS 族群,有顯著較低的大腸腺瘤盛行率。
此一發現過去亦曾在 Gu HX 於年輕中國人族群的研究中提及 (Gu HX et al.
2011),然而其間的因果關係仍未明。
關於 CD 與 non-CD 族群的比較:
本研究中,年齡是大腸憩室症最主要的危險因子,年齡在 65 歲以上的 odds ratio 是 2.04 (P=0.000)。在 Hjern F 和 Strate LL 過去的研究中發現肥胖及身體缺乏活 動,會增加憩室炎和憩室出血的風險 (Hjern F et al. 2012; Strate LL et al. 2009)。我們 的研究亦發現在較年輕的(age<65) 大腸憩室症族群中,BMI 顯著高於無大腸憩 室症的族群。推測可能與不正常的大腸活動(abnormal colon motility)有關。酒精 使用在我們的研究中發現是大腸憩室症的危險因子。在過去的幾個研究亦有相 同發現 (Song JH et al. 2010; Nagata N et al. 2013; Sharara AI at al. 2013)。其原因雖未明,
但有大鼠研究顯示,酒精會經由活化 NF-kB、iNOS 的 up-regulation 而增加腸壁 神經叢 NO 的釋放,最後會抑制大腸活動 (Wang C et al. 2010)。
關於無症狀大腸憩室症及有症狀大腸憩室疾病族群的比較:
本研究 237 有大腸憩室憩室症(CD)的病人中,有 28.3% (n=67) 是伴有腹痛症狀 的大腸憩室疾病(DD),其中的 9.7% (n=23) 受腹痛問題困擾的時間超過 6 個月。
這些群患者經多變數分析後仍有顯著較高的 BSRS-5 score,承受較高的心理壓 力。在治療此病人族群時應注意慢性腹痛所造成的心理影響。
關於腹痛症狀在 IBS 與有症狀的憩室疾病(DD)間的差異:
在過去兩位義大利研究者 Cuomo R 及 Tursi A 前後發表的研究中指出:中重度、
持久(超過 24 小時)下腹痛的這個臨床症狀可以區別有症狀的大腸憩室疾病及大
腸激躁症(Cuomo R et al. 2013; Tursi A et al. 2015)。此一發現並未於我們的研究中得到
驗證。可能原因為西方及亞洲人種憩室症好發位置不同所造成的影響。西方人 種的憩室症好發於左側而亞洲人種以右側為主。本研究所分析的 54 個單純有症 狀大腸憩室疾病(pure DD)的病人中,39 位的大腸憩室是位於右側。我們雖試圖 將右側及左側/雙側的憩室疾病分開分析,但可能因樣本數過少,無法看到統計 上的顯著差異。
本研究的限制如下:
本研究是屬於 hospital-based study,病人經過已經某種程度篩選,所得到的結果 可能無法代表一般族群。大腸鏡對於左側大腸憩室症的偵測有所不足,可能影 響研究結果。大腸激躁症的診斷是使用問卷,需要受試者回憶過去 3 到 6 個月 腹痛及排便的狀況,難以避免有 recall bias,可能會影響結果。本研究中 IBS 及 左側大腸憩室症的樣本數仍太少,鑒於在台灣族群中 IBS 及左側大腸憩室症的 盛行率偏低(IBS:6.6%、LD:2.5%),可能須多中心、長時間收案才能解決。
總結:
台灣人族群的大腸憩室症好發於右側。我們針對台灣人族群的研究中並未在大 腸憩室症(不論是左側或右側)與大腸激躁症間看到關聯性。使用腹痛超過 24 小 時的臨床症狀來鑑別 IBS 與有症狀的大腸憩室疾病未能得到驗證。在 IBS 病人
中有顯著較高的心理社會壓力。在較年輕的 IBS 患者中,大腸腺瘤的盛行率較 低。年齡(大)是大腸憩室症最主要的危險因子。喝酒及肥胖會顯著增加大腸憩 室症的風險。有症狀大腸憩室疾病的族群,須注意因慢性腹痛所造成的心理影 響。
第五章 未來展望:
在台灣人族群中,大腸憩室症與大腸激躁症間的關聯性仍需要更多大型、多中 心的研究或 meta-analysis 來證實或推翻。鑒於左側大腸憩室的盛行率在台灣人 族群中偏低,使用腹痛症狀來區分 IBS 和有症狀的憩室疾病(DD)並不實用。Fecal calprotectin 在西方人的研究中可區別 IBS 與 DD,但在亞洲人種的有效性仍需 證實。
第六章 論文英文簡述:
Background:
Irritable bowel syndrome (IBS) is a common functional GI disorder. The clinical presentation and pathophysiologic mechanisms of IBS has overlap with some organic GI disease. Recent researches showed the presence of colonic diverticulosis (CD), especially left-sided diverticulosis, was associated with higher risk of IBS.
However, conflicting findings were observed in the studies conducted in Asian population. Larger prospective studies are needed to confirm the association. Low grade inflammation and alteration in gut microbiota play important role in the pathophysiologic mechanism of symptomatic diverticular disease (DD). Recent studies have focused on the use of 5-ASA, antibiotics and probiotics in treating chronic diverticular disease. It is of clinical importance to distinguish IBS and chronic symptomatic diverticular disease to define the appropriate treatment. The effectiveness of abdominal pain lasting for more than 24 hours could discriminate IBS and DD had been proposed. Further validation is needed.
Objectives:
We conducted prospective study to 1. clarify the association between IBS and CD in Taiwanese population; 2. Validate the effectiveness of abdominal pain lasting for more than 24 hours in differentiating IBS and DD.
Methods:
We enrolled patients undergoing colonoscopy in single hospital. Questionnaire was applied to identify IBS patients (according to Rome III criteria) and to collect the characteristics of abdominal pain. We compared 1. the prevalence of CD in the IBS and non-IBS groups. 2. The prevalence of the clinical symptom of abdominal pain lasting for more than 24 hours in pure (no overlap) IBS and pure DD groups.
Results:
We initially enrolled 1502 subjects during March 2016 to November 2016 and 119 subjects met the exclusion criteria. A final total of 1383 subjects were enrolled for
was 1.58:1. IBS was identified in 6.6% and CD was observed in 17.1% of the patients. Right-sided diverticulosis is predominant (69% of all CD). There was no statistically significant difference between the prevalence of whole CD (14.3% vs 17.3%, P=0.455), right-sided CD(8.8% vs 12.0%, P=0.359) and left-sided CD(2.2%
vs 2.6%, P=0.435) in IBS and non-IBS groups. Significantly higher BSRS-5 score was observed in the IBS group. In younger (age<65) IBS patients, the prevalence of colonic adenoma was lower (OR:0.43, P=0.012). There was no significant difference between the prevalence of IBS in CD and non-CD groups (5.5% vs 6.8%, P=0.455).
Older age was the most important risk factor for CD (OR:2.04,P=0.000). Alcohol consumption (OR:1.48,P=0.037) and higher BMI (OR:1.09, P=0.000) also increased the risk of CD. Within the whole diverticulosis group, abdominal pain was
complained in 28.3% of the patients. Higher BSRS-5 score was observed in this subgroup (symptomatic diverticular disease). The pain duration, severity and location could not differentiate pure IBS and pure symptomatic DD in our study.
Discussion:
In our Taiwanese population, the prevalence of IBS was 6.6%, predominantly mixed and diarrhea subtypes, accounting for 44.0% and 39.6% respectively. The prevalence of colonic diverticulosis (CD) was 17.1%, predominantly right-sided diverticulosis, accounting for 69% of all colonic diverticulosis. This finding is consistent with past studies in Asian population. However, we do not see any association between CD (either left or right) and IBS. Possible reasons are as follows:
1. The mean age of our study population is lower: In Yamada E’s study, the mean age was 64.2 years and the prevalence of CD was as high as 40.2% (Yamada E et al.
2014). The mean age of our study population was only 55.8 years. The age difference may partially explained the lower prevalence of CD in our study (17.1%). Despite the attempt of age-stratified analysis, we were not able to see associations between IBS and CD in younger (age <65) or older (age ≥ 65) subgroups.
2. The studies were hospital-based. Studied population was screened by certain probably different criteria: The prevalence of IBS was 7.5% in Yamada E's study, and all patients received colonoscopy for colorectal cancer screening. The
mentioned in their study (Yamada E et al. 2014). The prevalence of IBS in our study was 6.6%. About 27.9% of patients received colonoscpy for positive iFOBT. A total of 42.3% of patients had abdominal pain, changes in bowel habits, bloody stool or other GI symptoms. The two studied populations were screened by different criteria and this may partly explained the differenct results.
3. The prevalence of CD in our study may be underestimated: In addition to age factor, the lower diverticulum detection ability of colonocscopy may also contribute to the low CD prevalence in our study. The detection ability of
colonoscopy for small lesions or diverticula largely depended on the adequacy of bowel cleaning. For high-quality colonoscopy, the cecal intubation rate should be more than 95%, the adequacy of bowel cleaning (excellent or good by Aronchick scale) should be 85-90% or more, and the adenoma detection rate (ADR) should be 20% -25% or more. In our study, the ADR was quite good (38.4%) but the adequacy of bowel cleaning was suboptimal (72.5%). This may hinder the detection of diverticulum. Yamada E did not mentioned the quality index of their colonoscopy. They used a transparent hood attached to the tip of the colonoscope during examination. Previous studies had shown the use of a transparent hood can fascilitate small lesions detection (Kondo S et al. 2007). Furthermore, it has been proposed that colonoscopy may have a lower rate of detection of colonicl
diverticula than barium enema (Niikura R et al. 2013). In Taiwan, due to the easy accessibility and therapeutic potential, colonoscopy has replaced most of the role of barium enema. If we use barium enema as the final confirmative study for colonic diverticulosis, we may require a much longer time for case enrollment or a multi-center study design.
Comparison of IBS and non-IBS groups:
Past studies have found that psychosocial stress are associated with the development of IBS (Drossman DA et al. 1988). In our study, significantly higher BSRS-5 score was found in the IBS group, regardless of age strata. In our study, the younger (age <65) IBS subgroup had a lower adenoma prevalence. This finding had been mentioned in Gu HX’s study of the young Chinese population (Gu HX et al. 2011), but the causal relationship is still unknown.
Comparison of CD and non-CD groups:
In our study, age was the most important risk factor for colonic diverticulosis, with an odds ratio of 2.04 (P = 0.000) for age more than 65 years. Previous studies in Hjern F and Strate LL shown that obesity and physical inactivity increased the risk of diverticulitis and diverticular bleeding (Hjern F et al. 2012; Strate LL et al. 2009). Our study also found that BMI was significantly higher in the younger (age < 65) CD subgroup. This may be associated with abnormal colon motility. Alcohol use was found to be a risk factor for colonic diverticulosis. The finding was consistent with several previous studies (Song JH et al. 2010; Nagata N et al. 2013; Sharara AI at al. 2013). The reason is still unclear, but rat studies have shown that alcohol consumption may activate NF-κB, up-regulate iNOS, increase NO release in myenteric plexus and finally inhibit colon motility (Wang et al. 2010).
Comparison of asymptomatic colonic diverticulosis and symptomatic diverticular disease:
Within the whole colonic diverticulosis group (n=237), 28.3% (n=67) of the patients were symptomatic. They suffered from abdominal pain and the chronicity (>
6months) was noted in 9.7% (n=23) of the patients. After multivariate analysis, significantly higher BSRS-5 score was observed in this subgroup (symptomatic diverticular disease). While treating these patients, increased psychosocial stress due to chronic pain should be concerned.
Comparison of the characteristics of abdominal pain between pure IBS and pure symptomatic diverticular disease (DD):
In Cuomo R and Tursi A’s studies pointed out the clinical symptom of severe and persistent (more than 24 hours) abdominal pain can differentiate symptomatic diverticular disease and IBS (Cuomo R et al. 2013; Tursi A et al. 2015). This finding could not be validated in our study. Western and Asian ethnic difference of the colonic diverticulosis may contribute to the result. Right-sided diverticulosis are predominant in Asian population. Of the 54 patients with pure symptomatic
diverticular disease, 39 patients has the right-sided diverticulosis. Although we tried to analyze right and left/bilateral diverticular disease separately, we could not see
The limitations of our study are as follows: This study is a hospital-based study, the generalizability of the results should be concerned. The suboptimal bowel cleansing and probably lower colonoscopic detection ability for left side diverticulum may have influence on the results. The diagnosis of IBS is by
questionnaires. The enrolled subjects have to recall their characteristics of abdominal pain and bowel habit in the past 3 to 6 months. Recall bias is inevitable. Furthermore, the case numbers of IBS and left-sided diverticulosis were still too small. Due to the low prevalence of IBS and left-sided diverticulosis (IBS: 6.6%, LD: 2.5%) in the Taiwanese population, a multi-center study design and longer time for case enrollment may be needed.
Conclusions:
In Taiwaness population, right-sided diverticulosis is predominant. The association between colonic diveticulosis and IBS was not observed in our study. The
effectiveness of abdominal pain lasting for more than 24 hours in differentiating IBS and DD also could not be validated. IBS patients had higher psychosocial stress.
Younger IBS patients had lower adenoma prevalence. Older age is the most
important risk factor of CD. Alcohol consumption and obesity increased the risk of CD. Patients with symptomatic diverticular disease had higher psychosocial stress.
參考文獻:
1. Aldoori WH , Giovannucci EL , Rimm EB et al. A prospective study of diet and the risk of symptomatic diverticular disease in men . Am J Clin Nutr 1994 ; 60 : 757–64.
2. Bolster LT , Papagrigoriadis S . Diverticular disease has an impact on quality of life— results of a preliminary study . Colorectal Dis 2003; 5 : 320–3.
3. Bianchi M , Festa V , Moretti A et al. Meta-analysis: long-term therapy with rifaximin in the management of uncomplicated diverticular disease . Aliment Pharmacol Th er 2011 ; 33 : 902–10.
4. Clemens CH , Samsom M , Roelofs J et al. Colorectal visceral perception in diverticular disease . Gut 2004 ; 53 : 717–22.
5. Chang HY , Kelly EC , Lembo AJ . Current gut-directed therapies for irritable bowel syndrome. Curr Treat Options Gastroenterol 2006 ; 9 : 314–23.
6. Comparato G , Fanigliulo L , Aragona G et al. Quality of life in uncomplicated symptomatic diverticular disease: is it another good reason for treatment? Dig Dis 2007 ; 25 : 252–9.
7. Crowe FL et al. Diet and risk of diverticular disease in Oxford cohort of European Prospective Investigation into Cancer and Nutrition (EPIC): prospective study of British vegetarians and nonvegetarians. BMJ 2011 ; 343 : d4131.
8. Cuomo R et al. Symptom patterns can distinguish diverticular disease from irritable bowel syndrome. Eur J Clin Invest. 2013 Nov;43(11) : 1147-55.
9. Dunlop SP , Jenkins D , Neal KR et al. Relative importance of enterochromaffin cell hyperplasia, anxiety, and depression in postinfectious IBS . Gastroenterology 2003 ; 125 : 1651–9.
10. Di Mario F , Aragona G , Leandro G et al. Effi cacy of mesalazine in the treatment of symptomatic diverticular disease . Dig Dis Sci 2005 ; 50 :581–6.
11. Drossman DA , McKee DC , Sandler RS et al. Psychosocial factors in the irritable bowel syndrome. A multivariate study of patients and nonpatients with irritable bowel syndrome . Gastroenterology 1988;95:701–8
12. Everhart et al. Burden of digestive disease in the United States part II: lower GI disease. Gastroenterology 2009; 136:741-54
13. Gatta L et al. Efficacy of 5-ASA in the treatment of colonic diverticular disease.
J Clin Gastroenterol 2010;44: 113–9.
14. Gu HX et al. Organic colonic lesions in 3,332 patients with suspected irritable bowel syndrome and lacking warning signs, a retrospective case–control study.
Int J Colorectal Dis 2011 ; 26 : 935–940
15. Gwee KA, Lu CL et al. Epidemiology of irritable bowel syndrome in Asia:
Something old, something new, something borrowed. Journal of gastroenterology and hepatology. 2009; 24:1601-1607
16. Hjern F , Wolk A , Hakansson N . Obesity, physical inactivity, and colonic diverticular disease requiring hospitalization in women: a prospective cohort study . Am J Gastroenterol 2012 ; 107 : 296 – 302 .
17. Huizinga JD , Waterfall WE , Stern HS . Abnormal response to cholinergic stimulation in the circular muscle layer of the human colon in diverticular disease. Scand J Gastroenterol 1999 ; 34 : 683–8.
18. Hobson KG et al. Etiology and Pathophysiology of Diverticular Disease. Clin Colon Rectal Surg. 2004 August; 17(3) : 147–153.
19. Humes DJ , Simpson J , Neal KR et al. Psychological and colonic factors in painful diverticulosis . Br J Surg 2008 ; 95 : 195–8.
20. Halpin SJ , Ford AC . Prevalence of symptoms meeting criteria for irritablebowel syndrome in infl ammatory bowel disease: systematic review and meta-analysis . Am J Gastroenterol 2012 ; 107 : 1474–82.
21. Jung HK , Choung RS , Locke GR III et al. Diarrhea-predominant irritable bowel syndrome is associated with diverticular disease: a populationbased study. Am J Gastroenterol 2010 ; 105 : 652–61.
22. Kondo S , Yamaji Y , Watabe H et al. A randomized controlled trial evaluating the usefulness of a transparent hood attached to the tip of the colonoscope. Am J Gastroenterol 2007 ; 102 : 75 – 81.
23. Lamiki P , Tsuchiya J , Pathak S et al. Probiotics in diverticular disease of the colon: an open label study . J Gastrointestin Liver Dis 2010 ; 19 : 31–6.
24. Nagata N et al. Alcohol and smoking affect risk of uncomplicated colonic diverticulosis in Japan. PLoS One. 2013 Dec 10;8(12):e81137.
25. Niikura R , Nagata N , Shimbo T et al. Colonoscopy can miss diverticula of the left colon identifi ed by barium enema. World J Gastroenterol 2013;19:2362 – 7 . 26. Painter NS , Truelove SC , Ardran GM et al. Segmentation and the localization
of intraluminal pressures in the human colon, with special reference to the pathogenesis of colonic diverticula Gastroenterology 1965 ; 49 : 169–77.
27. Parks TG . Natural history of diverticular disease of the colon . Clin Gastroenterol 1975 ; 4 : 53–69.
28. Raskin JB . Mesalamine did not prevent recurrent diverticulitis in phase 3 controlled trials. Gastroenterology 2014 Oct;147(4):793-802
29. Spiller RC. Role of infection in irritable bowel syndrome . J Gastroenterol 2007 ; 42 (Suppl 17) : S41–7.
30. Strate LL , Liu YL , Aldoori WH et al. Obesity increases the risks of
diverticulitis and diverticular bleeding . Gastroenterology 2009 ; 136 : 115 – 22 31. Song JH, Kim YS, Lee JH, Ok KS, Ryu SH, et al. Clinical characteristics of
colonic diverticulosis in korea: A prospective study. Korean J Intern Med 2010;
25: 140–146.
32. Strate LL et al. Diverticular disease as a chronic illness: evolving epidemiologic and clinical insights. Am J Gastroenterol. 2012 Oct ; 107(10) : 1486-93.
33. Sharara AI, El-Halabi MM, Mansour NM, Malli A, Ghaith OA, et al. Alcohol consumption is a risk factor for colonic diverticulosis. J Clin Gastroenterol.
2013 ; 47(5): 420-5
34. Sirinthornpunya S; Rungjiratananon S. Association of colonic diverticular disease and irritable bowel syndrome in Thai patients. Journal of the Medical Association of Thailand. 2014 Nov 97; Suppl 11 : S18-24,.
35. Talley NJ , Phillips SF , Wiltgen CM et al. Assessment of functional
gastrointestinal disease: the bowel disease questionnaire . Mayo Clin Proc 1990 ; 65 : 1456–79.
36. Trepsi E , Colla C , Panizza P et al. Th erapeutic and prophylactic role of
mesalazine (5-ASA) in symptomatic diverticular disease of the large intestine. 4 year follow-up results . Minerva Gastroenterol Dietol 1999 ; 45 : 245–52.
37. Tursi A , Brandimarte G , Daffi na R . Long-term treatment with mesalazine and rifaximin vs. rifaximin alone for patients with recurrent attacks of acute
diverticulitis of colon . Dig Liver Dis 2002 ; 34 : 510–5.
38. Talley NJ Irritable bowel syndrome . Intern Med J 2006 ; 36 : 724–8.
39. Tursi A et al. Assessment and grading of mucosal inflammation in colonic diverticular disease. J Clin Gatroenterol.2008; 42 : 699-703.
40. Tursi A et al. Faecal calprotectin in colonic diverticular disease: a case-control study. Int J Colorectal Dis. 2009 Jan ; 24(1) : 49-55.
41. Tursi A , Papagrigoriadis S . Review article: the current and evolving treatment of colonic diverticular disease . Aliment Pharmacol Ther 2009 ; 30 : 532–46.
42. Tursi A et al. Moderate to severe and prolonged left lower-abdominal pain is the best symptom characterizing symptomatic uncomplicated diverticular disease of the colon: a comparison with fecal calprotectin in clinical setting. J Clin
Gastroenterol. 2015 Mar;49(3):218-21.
43. Wang LH , Fang XC , Pan GZ . Bacillary dysentery as a causative factor of irritable bowel syndrome and its pathogenesis.Gut 2004;53: 1096–101.
44. Wang C, Wang S, Qin J, Lv Y, Ma X, et al. Ethanol upregulates iNOS expression in colon through activation of nuclear factor-kappa B in rats. Alcohol Clin Exp Res 2010; 34: 57–63.
45. Yamada E et al. Association between the location of diverticular disease and the irritable bowel syndrome: a multicenter study in Japan. American Journal of Gastroenterology. 2014; 109(12):1900-5.
圖表:
圖 1 大腸憩室症之分類及學術名詞定義
(13. Am J Gastroenterol. 2012 Oct;107(10):1486-93.)
圖 2 大腸憩室疾病可能之病生理機轉及其相關治療 (13. Am J Gastroenterol. 2012 Oct;107(10):1486-93.)
(Symptomatic uncomplicated diverticular disease)
(Segmental colitis associated with diverticulitis)
圖 3 收案流程圖
Patients undergoing CFS
Pain + IBS +
Pain + IBS + CD +
Pain + IBS +
CD -
Pain + IBS -
Pain + IBS – CD +
Pain + IBS – CD -
Pain - IBS -
Pain – IBS – CD +
Pain – IBS – CD -
IBS questionnaire
Colonoscopy Colonoscopy Colonoscopy
腸胃道症狀及心理健康問卷
(版本/日期: Version 1.0/2015-12-25)
1. 請問您的性別為 男 女 ,年齡_________
身高: ________ 公分 體重: ________ 公斤 2.請問您是否有抽菸? 有 ____ 包/天 ____ 年
無 3.請問您是否有飲酒習慣 有 無
4.請問您在過去三個月是否有使用下列藥物:
軟便藥/瀉藥 有 無 消炎止痛藥 有 無
類固醇 有 無 降血壓藥 有 無
降膽固醇藥物 有 無
5.請問過去是否曾接受過腹部或骨盆腔手術 有 ,何手術?______________
無
請您仔細回想,在最近三個月中,下面五個問題使您感到困擾或苦惱的程度:
06. 睡眠困難,譬如難以入睡、易醒來或早醒來
完全沒有 輕微 中等程度 厲害 非常厲害 07. 感覺緊張不安
完全沒有 輕微 中等程度 厲害 非常厲害 08. 覺得容易苦惱或動怒
完全沒有 輕微 中等程度 厲害 非常厲害 09. 感覺憂鬱、心情低落
完全沒有 輕微 中等程度 厲害 非常厲害 10. 覺得比不上別人
完全沒有 輕微 中等程度 厲害 非常厲害
11.請問您接受大腸鏡檢查的原因為何?
腹痛 大便習慣改變(便秘或腹瀉) 血便 糞便潛血檢查呈陽性 單純接受健檢 其他
12.請問您在過去三個月內是否有腹部不舒服或疼痛的情況? 有 無 (若回答無,則結束作答,無須再填寫以下問題。)
--- 13.請問您腹部不舒服或疼痛的嚴重度為何?
非常輕微 輕微 中度 嚴重 非常嚴重 14.請問您腹痛的位置是在?
肚臍上 肚臍下 肚臍上下都有 不固定位置或無法確切描述
15.請問您每次腹痛發作大約會持續多久?
幾分鐘而已 (小於 1 小時) 好幾個小時
持續一天以上
16.請問您腹部不舒服或腹痛發生的頻率為何?
一個月中有一天或更少 一個月中有一天
一個月中有二到三天 一個星期中有一天 一個星期中有一天以上 每天都會痛
17.若您為女性,請問您的腹部不舒服或腹痛,是否只發生在生理期時?
是 否 不適用。受訪者為男性或已停經 18.腹部不舒服或腹痛是否已經困擾您有六個月以上的時間?
是 否
19.請問您解完大便後,腹部不舒服或疼痛的狀況是否會有改善?
腹痛 從未 因排便而改善 腹痛 有時候 會因排便而改善 腹痛 經常 會因排便而改善 腹痛 大部分 會因排便而改善 腹痛 總是 會因排便而改善
20.當腹部不舒服或腹痛發生時,解大便的頻率、次數是否有比平常增加?
解大便的次數 從未 比平常時增加 解大便的次數 有時候 會比平常時增加 解大便的次數 常常 會比平常時增加 解大便的次數從 大部分 會比平常時增加 解大便的次數從 總是 會平常時增加
21.當腹部不舒服或腹痛發生時,解大便的頻率、次數是否有比平常減少?
解大便的次數 從未 比平常時減少 解大便的次數 有時候 會比平常時減少 解大便的次數 常常 會比平常時減少 解大便的次數從 大部分 會比平常時減少 解大便的次數從 總是 會平常時減少
大便的外觀分類 正常 (如圖 4)
堅硬成塊 (如圖 1、2、3) 鬆散不成條 (如圖 5、6、7)
22.當腹部不舒服或腹痛發生時,解出的大便是否較為鬆散不成條?
大便 從未 比平常鬆散不成條
大便 有時候 比平常鬆散不成條 (25%以上的時候) 大便 常常 比平常鬆散不成條 (50%以上的時候) 大便 大部分 比平常鬆散不成條 (75%以上的時候) 大便 總是 比平常鬆散不成條
23.當腹部不舒服或腹痛發生時,解出的大便是否較為堅硬成塊?
大便 從未 比平常堅硬成塊
大便 有時候 比平常堅硬成塊 (25%以上的時候) 大便 常常 比平常堅硬成塊 (50%以上的時候) 大便 大部分 比平常堅硬成塊(75%以上的時候) 大便 總是 比平常堅硬成塊
圖 1 圖 2 圖 3 圖 4 圖 5 圖 6 圖 7
24.在過去的三個月,解出的大便是否堅硬成塊?
大便 從未 堅硬成塊
大便 有時候 堅硬成塊 (25%以上的時候) 大便 常常 堅硬成塊 (50%以上的時候) 大便 大部分 堅硬成塊 (75%以上的時候) 大便 總是 堅硬成塊
25.在過去的三個月,解出的大便是否鬆散不成條?
大便 從未 鬆散不成條
大便 有時候 鬆散不成條 (25%以上的時候) 大便 常常 鬆散不成條 (50%以上的時候) 大便 大部 分鬆散不成條 (75%以上的時候) 大便 總是 鬆散不成條
---
大腸鏡檢查日期:
檢查是否到達盲腸: 是 / 否 是否發現息肉: 是 / 否
清腸程度: Excellent / Good / Fair / Poor
是否發現大腸憩室: 是 / 否
大腸憩室位置: 右側 / 左側 / 雙側
大腸憩室數量: 小於 5 / 大於等於 5
圖 4 收案流程圖---最終收案結果
表 1 病人特色
Table 1. Patients’ characteristics (n=1383)
Age (mean ± SD, years) 55.8 ± 13.1
Gender (M:F) 1.58 : 1
Mean BMI 24.6 ± 3.7
Smoking (%) 21.8
Alcohol (%) 20.0
Laxatives use (%) 20.3
Analgesics use (%) 32.3
Steroid use (%) 1.5
Anti-HTNs use (%) 32.5
Statins use (%) 18.1
BSRS-5 (range 0~20) 3.7 ± 3.4
Operation history 20.8
Good bowel cleansing (%) 72.5
Adenoma, ADR (%) 38.4
Diverticulosis (%,n) 17.1 (237)
RD (%,n) LD (%,n) BD (%,n)
11.8 (163) 2.5 (35) 2.8 (39)
IBS (%,n) 6.6 (91)
C-IBS (%,n) D-IBS (%,n) M-IBS (%,n) U-IBS (%,n)
0.9 (12) 2.6 (36) 2.9 (40) 0.2 (3)
BMI:body mass index; BSRS-5:Brief Symptom Rating Scale-5; Good bowel cleansing:good and excellent by Aronchick scale; ADR:adenoma detection rate; RD:right diverticulosis; LD:left diverticulosis; BD:bilateral diverticulosis;C-IBS:constipation type IBS; D-IBS:diarrhea type IBS;
M-IBS:mixed type IBS; U-IBS:un-subtype IBS
表 2 有大腸激躁症及無大腸激躁症群組之比較
Table 2. Comparison between IBS and non-IBS groups
IBS (n=91) Non-IBS (n=1292) P value Age (mean ± SD, yrs) 53.0 ± 14.2 56.0 ± 13.0 0.037 t*
Gender (M:F) 1.39 : 1 1.59 : 1 0.543 c Mean BMI 24.3 ± 4.0 24.6 ± 3.7 0.531 t
Smoking (%) 24.2 21.7 0.576 c
Alcohol (%) 18.7 20.1 0.740 c
Laxatives use (%) 38.5 19.0 0.000 c*
Analgesics use (%) 45.1 31.4 0.007 c*
Steroid use (%) 3.3 1.32 0.126 c
Anti-HTNs use (%) 31.9 32.6 0.888 c
Statins use (%) 15.4 18.3 0.490 c
BSRS-5 (range 0~20) 6.1 ± 4.6 3.5 ± 3.2 0.000 t*
Operation history 35.2 26.2 0.063 c Good bowel cleansing (%) 69.2 72.8 0.672
Adenoma, ADR (%) 26.4 39.2 0.015 c*
Diverticulosis (%,n) 14.3 (13) 17.3 (224) 0.455 c RD (%,n)
LD (%,n) BD (%,n)
8.8 (8) 2.2 (2) 3.3 (3)
12.0 (155) 2.6 (33) 2.8 (36)
0.359 c 0.834 c 0.776 c BMI:body mass index; BSRS-5:Brief Symptom Rating Scale-5; Good bowel cleansing:good and excellent by Aronchick scale; ADR:adenoma detection rate;
RD:right diverticulosis; LD:left diverticulosis; BD:bilateral diverticulosis c Chi-square test
t Student’s t test
* P < 0.05
表 3-1 大腸激躁症危險因子之多變數回歸分析
Table 3-1. Results of the multiple logistic regression analysis for independent risk of IBS
Odd ratio 95% CI P value
Age 0.99 0.97-1.00 0.131
Laxatives use 2.35 1.47-3.75 0.000*
Analgesics use 1.23 0.78-1.95 0.368
BSRS-5 1.17 1.11-1.23 0.000*
Operation history 1.47 0.92-2.36 0.108
Adenoma, ADR 0.68 0.40-1.14 0.145
Diverticulosis 1.44 0.42-4.99 0.565
RD 0.52 0.12-2.15 0.365
LD 0.76 0.11-5.10 0.781
BSRS-5:Brief Symptom Rating Scale-5; ADR:adenoma detection rate; RD:right diverticulosis; LD:left diverticulosis
* P < 0.05
表 3-2 大腸激躁症危險因子之多變數回歸分析---年輕(<65 歲)次群組
Table 3-2. Results of the multiple logistic regression analysis for independent risk of IBS in younger patients (age<65)
Odd ratio 95% CI P value
Laxatives use 2.16 1.26-3.69 0.005*
Analgesics use 1.05 0.62-1.77 0.857
BSRS-5 1.17 1.11-1.25 0.000*
Operation history 1.64 0.97-2.78 0.065
Adenoma, ADR 0.43 0.23-0.83 0.012*
Diverticulosis 1.71 0.37-7.92 0.494
RD 0.58 0.11-3.13 0.523
LD 0.58 0.04-7.65 0.681
BSRS-5:Brief Symptom Rating Scale-5; ADR:adenoma detection rate; RD:right diverticulosis; LD:left diverticulosis
* P < 0.05
表 3-3 大腸激躁症危險因子之多變數回歸分析---年長(≧65 歲)次群組
Table 3-3. Results of the multiple logistic regression analysis for independent risk of IBS in older patients (age≧65)
Odd ratio 95% CI P value Laxatives use 2.43 0.90-6.54 0.080 Analgesics use 2.31 0.82-6.51 0.112
BSRS-5 1.16 1.02-1.32 0.023*
Operation history 0.75 0.27-2.13 0.592
Adenoma, ADR 1.71 0.62-4.75 0.299
Diverticulosis 1.42 0.17-12.14 0.751
LD 0.58 0.03-11.08 0.717
BSRS-5:Brief Symptom Rating Scale-5; ADR:adenoma detection rate; RD:right diverticulosis; LD:left diverticulosis
* P < 0.05
表 4 有大腸憩室症及無大腸憩室症群組之比較
Table 4. Comparison between CD and non-CD groups
CD (n=237) Non-CD (n=1146) P value Age (mean ± SD, yrs) 61.1 ± 10.5 54.7 ± 13.3 0.000 t*
Age ≧ 65 (%) 37.1 23.3 0.000 c*
Gender (M:F) 2.1 : 1 1.5 : 1 0.02 c*
Mean BMI 25.6 ± 3.7 24.3 ± 3.6 0.000 t*
Smoking (%) 25.7 21.0 0.110 c
Alcohol (%) 26.2 18.8 0.010 c*
Laxatives use (%) 18.6 20.7 0.461 c Analgesics use (%) 35.9 31.5 0.191 c
Steroid use (%) 2.1 1.3 0.347 c
Anti-HTNs use (%) 40.9 30.8 0.002 c*
Statins use (%) 19.8 17.7 0.441 c
BSRS-5 (range 0~20) 3.5 ± 3.5 3.7 ± 3.4 0.351 t Operation history 31.2 25.9 0.093 c Good bowel cleansing (%) 76.1 71.7 0.216 c
Adenoma, ADR (%) 46.0 36.8 0.008 c*
Patients with pain (%,n) 28.3 (67) 33.5 (384) 0.117 c IBS (%,n)
C-IBS (%,n) D-IBS (%,n) M-IBS (%,n) U-IBS (%,n)
5.5 (13) 0.4 (1) 3.4 (8) 1.7 (4) 0 (0)
6.8 (78) 1.0 (11) 2.4 (28) 3.1 (36) 0.3 (3)
0.455 c
0.493 c
CD:colonic diverticulosis; BMI:body mass index; BSRS-5:Brief Symptom Rating Scale-5; Good bowel cleansing:good and excellent by Aronchick scale; ADR:adenoma detection rate;
C-IBS:constipation type IBS; D-IBS:diarrhea type IBS; M-IBS:mixed type IBS; U-IBS:un-subtype IBS; c Chi-square test; t Student’s t test; * P < 0.05
表 5-1 大腸憩室症危險因子之多變數回歸分析
Table 5-1. Results of the multiple logistic regression analysis for independent risk of CD
Odd ratio 95% CI P value
Age ≧ 65 2.04 1.46-2.84 0.000*
Male gender 1.09 0.78-1.51 0.614
BMI 1.09 1.05-1.13 0.000*
Smoking 1.18 0.82-1.70 0.377
Alcohol 1.48 1.02-2.13 0.037*
Anti-HTNs use 1.06 0.77-1.46 0.699
Adenoma, ADR 1.07 0.80-1.45 0.666
IBS 0.83 0.45-1.55 0.567
BMI:body mass index; CD: colonic diverticulosis; ADR:adenoma detection rate
* P < 0.05
表 5-2 大腸憩室症危險因子之多變數回歸分析---年輕(<65 歲)次群組
Table 5-2. Results of the multiple logistic regression analysis for independent risk of CD in younger patient (age<65)
Odd ratio 95% CI P value
Male gender 1.16 0.77-1.75 0.483
BMI 1.11 1.06-1.16 0.000*
Smoking 1.21 0.79-1.84 0.389
Alcohol 1.44 0.93-2.21 0.099
Anti-HTNs use 1.20 0.80-1.80 0.372
Adenoma, ADR 1.11 0.76-1.62 0.601
IBS 1.15 0.58-2.28 0.689
BMI:body mass index; CD: colonic diverticulosis; ADR:adenoma detection rate
* P < 0.05
表 5-3 大腸憩室症危險因子之多變數回歸分析---年長(≧65 歲)次群組
Table 5-3. Results of the multiple logistic regression analysis for independent risk of CD in older patient (age≧65)
Odd ratio 95% CI P value
Male gender 0.97 0.56-1.66 0.906
BMI 1.05 0.97-1.13 0.255
Smoking 1.08 0.52-2.22 0.838
Alcohol 1.50 0.73-3.05 0.268
Anti-HTNs use 0.90 0.55-1.49 0.684
Adenoma, ADR 0.99 0.60-1.63 0.971
IBS 0.34 0.08-1.53 0.162
BMI:body mass index; CD: colonic diverticulosis; ADR:adenoma detection rate
表 5-4 無症狀大腸憩室症及有症狀大腸憩室疾病之比較
Table 5-4. Comparison between asym. CD and sym. DD groups
Asym. CD (n=237)
Sym. DD
(n=1146) P value
Age (mean ± SD, yrs) 62.2 ± 9.7 58.3 ± 11.8 0.016 t*
Gender (M:F) 2.3 : 1 1.8 : 1 0.437 c
Mean BMI 25.9 ± 3.7 24.8 ± 3.4 0.039 t*
Smoking (%) 24.7 28.3 0.562 c
Alcohol (%) 25.3 28.4 0.629 c
Laxatives use (%) 16.5 23.9 0.186 c
Analgesics use (%) 31.2 47.8 0.017 c*
Steroid use (%) 1.2 4.5 0.111 c
Anti-HTNs use (%) 45.9 28.4 0.013 c*
Statins use (%) 19.4 20.9 0.796 c
BSRS-5 (range 0~20) 2.8 ± 3.0 5.2 ± 4.2 0.000 t*
Operation history 30.0 34.3 0.517 c Good bowel cleansing (%) 77.1 74.6 0.750 c
Adenoma, ADR (%) 45.9 46.3 0.957 c
RD (%, n) 68.2 (116) 70.2 (47) 0.775 c LD (%, n) 14.1 (24) 16.4 (11) 0.653 c BD (%, n) 17.7 (30) 13.4 (9) 0.431 c Diverticulum no. > 5 (%) 34.7 32.8 0.785 c
BMI:body mass index; BSRS-5:Brief Symptom Rating Scale-5; Good bowel cleansing:good and excellent by Aronchick scale; ADR:adenoma detection rate; RD:right diverticulosis; LD:left diverticulosis; BD:bilateral diverticulosis
c Chi-square test t Student’s t test
* P < 0.05
表 5-5 有症狀大腸憩室疾病危險因子之多變數回歸分析
Table 5-5. Results of the multiple logistic regression analysis for independent risk of symptomatic DD
Odd ratio 95% CI P value
Age 0.98 0.95-1.01 0.145
Male gender 0.76 0.36-1.60 0.464
BMI 0.93 0.85-1.02 0.142
Smoking 1.18 0.52-2.70 0.694
Alcohol 1.08 0.47-2.49 0.864
Analgesics use 1.59 0.84-3.01 0.155 Steroids use 4.45 0.59-33.61 0.148 Anti-HTNs use 0.54 0.26-1.13 0.104
Statin use 1.16 0.52-2.60 0.716
BSRS-5 1.21 1.10-1.33 0.000*
BMI:body mass index; BSRS-5:Brief Symptom Rating Scale-5
* P < 0.05
表 6 大腸激躁症及有症狀大腸憩室疾病兩群組間腹痛特色之比較
Table 6. Pain characteristics between pure IBS and pure DD
Pure IBS (Pain+,IBS+,CD-)
(n=78)
Pure DD (Pain+,IBS-,CD+)
(n=54)
P value
Age 52.4 ± 14.6 58.6 ± 12.1 0.011 t*
Pain duration Pain < 1hr (%,n) Pain 1hr~24Hrs (%,n) Pain > 24hrs (%,n)
57.7(45) 24.4(19) 18.0(14)
59.3(32) 25.9(14) 14.8(8)
0.858 c 0.838 c 0.635 c
Pain score(range 1-5) 2.6 ± 0.8 2.7 ± 1.1 0.720 t
Pain location
Upper abdomen (%,n) 18.0(14) 24.1(13) 0.391 c Lower abdomen (%,n) 25.6(20) 35.2(19) 0.237 c Upper & lower (%,n) 29.5(23) 18.5(10) 0.152 c Un-clarified (%,n) 26.9(21) 22.2(12) 0.540 c c Chi-square test
t Student’s t test
* P < 0.05